Handbook of
Neurosurgery
Mark S. Greenberg
Sixth Edition
~Thieme
:~iBOivSi l l l
56
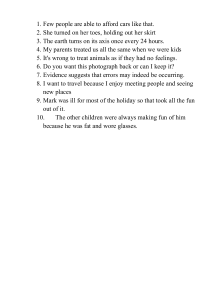
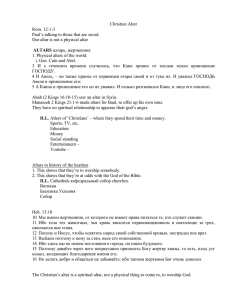
HEAD CIRCUMFERENCE
54
52
: tttt~tt~~
..
.6
"
"
38
36
"
32
30
... 0
eM
2
4
6
8
456;891012 14 16 18
10 12 14 16 18 20 22
YEARS
MONTHS
t
AG E
6O: ~~_
GIRLS
HEAD CIRCUMFERENCE
"
52 ~~~~~+-+-+-j .
: :f=I:=I+:~~
46 +-H,~
.. ~~-t
42 ~-h'-li
40
38
36
34
32
30
o
2
4
6
8
3 4 5678910 12141616
10 12 14 16 18 20 22
M ONTHS
I
YEARS
Reproduced by Pel/russian at Pediatrics, Vol. 41 , pages 101 & 108, ©1968
AG E
Theutlulive dinributo. in the Americal and Canada ;1
Thieme New York
333 Seventb Avtnue
New York. NY 1000l
United States or America
(BOO) 782-30188
The "clUllV' d,.tribul.or QIIt.11ida tha Americas 18
Thieme inl<emlOtionai
Rudigentraase I~
Stuttgart. Germany
+49 (0) 711-8931-126
Wbrary orCongress C"t.logins-;n-PubliClltion Data fa ayaiiable from the publi.h@r
HANDBOOK OF NEUROSURGERY
MatI< S. Greeobere:
ISBN 1-58890-.57_1
(ThIeme Ne ... Yorl.)
ISBN 3-13-U0886-X
(Geare: Thiem. VerlaS Stutts.rLJ
Capyrillht C 2006
Marl< S. Greenbe'll. All nghl.l
re~e",e-d.
Third ed.itiun, 199<1
Fourth edition. 1997
Fint e-ditiun, 1990
Secvnd edition. 1991
Fifth !!dition. 2001
GTHnberJ Graphk •. Inc,
Lakeland, n .
•. mail: edil.o~apbic:a.Cllm
_w.IP'ITaphiea.cum
Cop)'tiant C2006 b)' Gl'Mnbets G.a phla. lnc. This book, i rw:ludinlaU pllU thereor,
II itgaUy J)I'Otected by ClDp)'tighl. My UN. aploitltlQII o. eommerda!ltatioll oubide the
IIDnow limita _ t byropJriiht legialation, without the publi.her'. conaent." ilIl'galand
Ii.ble to ~tioll. 1'biI'PJ)lie. in part!cul.r to p~t.at reproduc:tion. copying. mim·
eD(l'Iphilll or duplication of .ny kind, tranalatins, pnparatill!l Dr mkrofiimll, and elecIronic data Proceainl and 'tor.,a.
....
Loo.port."t " """ Medieal ~ledp ~ ~"';nl' All ...... TMeatcl! and clinical Mpe'n...... broUot.o our ~J"'" npt,III 1n.1Jpen1 and d"'llhenopy may ba requinld . Th. au_
\lion and ""iton oHM ..... t.atlat <DntaIned hoe",dn b... con.uJt.ed lIOu .... ' believed til be reU.ble
jll !he.. eftiltU to PI'O"ide inl'om.alion thIot is «I"'p~ and III aeeo>rd ""til the .tandlll"d8 _pt.ed
.L the ti ..... ~p"liI;e"tiorI. H_eoer, in vi.w e(th, popihiHty of hum .... error by th, aulh p.... M_
iton. or publWwr of
work hueirJ, "" chana. ,n roedical ilnowlod, e, neithftf th, .uUwm. «1_
;1On. pubu.h«, ..... al\1 otMr party who hall r-n in~oI~od In the preparation oflhla work.
wlJT&II,-!ha1 1hIIi:rt."""-tiIIn <OIItruncd ~ b ill £Yery TUlpoel OUU",II:OI' <Dmplctc.1LDd
lMy an ....t ...."....mbLa for ... y .......... or omiPionl or for the _ulta obtainM from u"" of RUch
infon:nalOoll. RHcItnI .... _raced toCG<lfitn> the infonn.tioo conl&in«l tM!rein with othtr
110"",*, Per eumploa, .... derr .... odviMd IOdIeck the produet informati.:m lbMt 1nd0Jde.d In the
~ oC~drvr lheypjan ta,dnlillisteftoba_1n lM,t lheinforttlltion contained In this
publicatiOll 'ncelln"" and that than.i:es haye !lOt ~ ""...:Ie in the .-""nded dC*O or in the
coot ... iodX:.liona for adDIiniuntion. "This recoommendalioo ;. of poorticular ImpOrtonC4 ;n eoo·
nection orith DeW or in£reqUolntiy uoed d",1PSomeoflhe FOdud. IWDD, .,.IaIIa, .nd ....... lem delipo refer'tt'CI to in this book.re in
f.d; ~Iter'ed tr.demarkl .... p",.,.;.tary na .....
lboup lpecitic referenoe.lO thll flet J. not
at ....,. made In !.he Ia!. n.enr....., !he IpperonM1l of. name wllhoul dH;pIIJlOOI •• prop .... t.ary
WIlOI. to be<llloDltlued ... repreocnlation to,. the publiober th.t il II In Lht public: domlin,
u..
tv'"
eo-. iIluatno..... br!boo .~Iho< ~ 1M onteruIo\.e<1ll braiotlom...d II.......1&1"... _10II'" ..HI! pono;- Ir_: '-II sa. Chaq 0.1. p...,. 0 .... I.o6nL. PJ, /)o1A1.. DinIlL pelion""
... r..ior """'Iar &rWty _ _ _ <hll_1
ad .......-..1- J Nou""u,* 2002, ~1 [4 ~
1~e6, r ... l.abelod mUW- <A u.. lJ:Ia~, _ _ 80 bo..t ...
_1..1_
Prinl.ed ill Onta.ricl, CanIda.
Prinlinjr: 6 • 3 2. 1
•
Printer: Web<:om, Umlted.
NEUROSURGERY
DeDI CATION
The lixth edition ofthe Handbook ofNcurGllurgery book i. dedicated 1.4 the mC'mory of
my mother, MAry, t.II the tOntinued giflor my rather, Lou;', to thc pre"n! ormy dlltlil1l
wife. Debbie, and 1.0 the (uture of my child ... n. Shaina, Aleu, Laah and Mich.~1.
CONVENTIONS
PRACTICE PARAMETER OH'N'T'O"S
Standanl5 Pncl ice Sklnd4rd~ indicDI.c I high degTft of clinical OIIrtllinty
and are lIenerally balled on CII5S I ",video c", ( _ or more wel!..!~ill1ed. ran·
domiled controllP.d au>diell) or atrooll ClISS U "",idl!flctl eal)fti.Uy wh,,,, dn:um.
II.Mce:I pnoelucl", r.ndomized clinical trials
SUlde line s Practice G.. ;~l~ rell«t • lII.rll le! d~ of clinleal oertDinIy and are I1!OOUIro.:ndeclwhen Ihe revie~ fell th!rt! "'N il\8ll fficN!.nl inform. _
tion to CrftaUlI SklNJc;rd, and are " l llall,y '-d OG C lu .• l1 e .. ide nc .. lone or
more weU-duigned tOmplirati.. e dinic, l l tudiu 01" Ie.. well-do-.igned randomiaed ltudiea) Or . PTi!PQnderao.:e ofChw III evidu.u
Options T'racticeOpiiOll4 of IlnclelircUnic.l ""rtainly and .... r1I<!'IIDmendft(!
when the ...... iew~ra fOllt thetf) ",as ;ll$llffitk!nl lnlormal.ion to create I SIU~dlJrd
or C"i~/iIM. and arfl generally based on CI..I IU l viden~ (C¥lIe r;eriu , hi.\() ...
ie, 1c:ontroll , cue repOrtii and erperlopUlion)
Retommendallon s Some refe~1II:ft use Ihil WmI IftMnully ,oil th~
q>eci1Y the Ilrength ofth. dlta. For th_. the natu .. of the d:lu ",ill 1M gi-..en.
A CKNOWLEDGMENTS
I would like 10 ockno .... ledge.U the 1OIlt'CU .. Hod ror tile malQrialln thit book.. 'J'hia
lnelud<ll tha mnny ~II iovolved;~ m.y mt!dkll and OIIiTOlutJicllll"lliniog. Spi!rial II'"
preciaUool. upfftll4!d UI J ohn M. T_ , Jr.. M.D., undoer ",n.-ruidllf>Cf! Il'Klli....d my
neu,..".u rgie.allra inlng. II I I... lncludell thou who pnuously rntitOO penninion ~ uM
nrurea and \JObiN pr...iOlllly publUl hed .
ABBREVIATIONS
AbbreviltiON \l.I<!d only locally Ire denn..-:! ill thlt sectlOrl using bold&.oe type..
\\'boere appropriate, pap numbers Cor tho Durin "'-"lion rele .. ant to chll topic i.given •
"~cy:sl.~
...t ..... ~ ..
~""""""' 1 :1
anI..-"", _ _
--
.~MIocIInIII
• 31 Q
--... - HO
_
y
t
I
P
.
.
.
.
.
c
.
.
.
.
.
.
MIl~cIr\toI - 2'68
,
....~
~"Iar c.rv\C;tI di$«IoclOlny & fusion
~..:c<I ...t\in9enl'f1'111O
N~UROSURGERY
'- 1
....._Iicoo''' *'toI)'ft)DnII
· ruwv
asympt<>m1llC: CO<OIicI ~ stenosis · m
II! AsympIQmaIlC:Carolld
SIUd~ · 813
"'*Y
-.tDr~-.y
"
"""
..,.,-1-·. .
"
''''
~'"
_~ ""'U\l'llCylorno -41:1
~
M
o
-." •.
__
101 ,.. U. S. P\lGkHaa!l'l s.Mce)
'"
."""" _...
.,
....
.,
·~
MI<I.;o.IIIt"'OOI'c.... I>8II"'_f'I
.CQUn<lltn<nunodflldft>(:y sr~
~
.
alM>"'-"n as
-
'"
.00
.".G
"......
~
...n
"",fO!roPt'k IIIWai Qr<):IIS • :.2
....""""""
."',badln
~IIC>,"."'"
,~
..,.,.at""
0.'
GO,
GO,
GO,
,GO
~
_ " ' " ,,..-.,_ 151
biol /la( At\&r;
EBA T
Mul~
W"
tlolfI.I 'I'ii'l.... "'~.,Iy . 74g
DoN """Pf'o9_1lc pml .." • rn
,~
_PI·. .,'.a.c:w",
·-
~o_,""",,·511
-,
IIe<I , ../II (OIdo"ry ,..IIICUIrI)
DoI. .1$1o.uII
665
tnl"''''''' q4iDma _ '20
~"".".~. -!It'
car&aI~"'¥<'P<III'IY-
<X),Ot""Y Il1*Y ~ gr.~
COO'..... 'Y l&I'IOr(<IIlloas.
_et>raJ _
no.. - 76J
'"
"""_tlOIOod.....e........aDPI...
_~ n
c.I"'m-clut1lOftl _
. a.~
00IIgIIniIa! ~ ic r.u~ ~
~..,, 1 1gen-501
"""""I """""'...
~1.ar'Y (lcOy . I rlld)
IXIfl\!n.... -...IIIiIu ...
cI>r ...... ll'l1\ammoI1ay QefI1yeilrwMlng 1IOIyr. '
diailon..""""hy - 5'
Cro;JlZI","'..JDi<Ob dI...... - 227
""_""". "",1_,.,.,· a.1
CMFI01 c:e<ebral ...., _ ",'" 01 DXYII"" 0010·
!IIImop\lOI't ·163
,OM'
awoot·"'....T;xoUt·&54
<GO
"""HI'!..,...
cardl", <IIAj)01
,~
'0
'"
'"
'"C, N.
'"
""'"
""W
""
m
'"
C'"
~
'"
,~
,~
GO"
'";.
~u.
ceI11f" 11'MI<"OOUI" 'y$I~
~.,dIac ""II'<'I
te.-rlOr>O<llirl<> ""!lie
celli,,, p)I1'lnot ~ - 12
"""'~PI_"'_·~7~
tertbllll pertllalOn ",fIS5<lta - !i-l7
r:taniII
nosrv&/.,
DlfVleaI~rlemy""" lhy·331
C-rIIlClIVO pr<ll,"n
~\"\l1 ~ syndrome· J!f6
c
I08I.0 - 911
,,/fIg.
ce<ebtOi Yli. .....
14
c:I'I.ro<'Jc lnIumallc efl..IQ/lIUopolI')' • G83
CIIfp.l1
'''mer..,....,'''... · 565
ce<eIIroYosculo, ..x:kIeOl. Woke -
~
Cef\lfal VIfICI\I5 prao ... ,.
t41leboo...,..,"" _ . l f lromllPJiol-1IIIIl
oe/~" reoIII..-.ot - 763
C8\et>rat ""'001IIII:111\ - 79 1
-
j~
....
~
..IBI""I_:IO<y""...
(MI'lI I_ 136
e>t_I~ ...... ftf\)1
""om" btll/1'l ra<lial00n 'NoIlIUI'
O<}'1h4om' ch!onIcuM
234
mig,..,., -
l!Ilidu.., """"'1oIna· 669
.~t ....... 1IaI"<u11orlgu1
"'~_"'8d Irnm~
'"
.0,
'"
".
"""
''''''.
....'"'W "
OIeCltQnySlllogn-og'aplly - 0132
Hr, ~ *"Il ll'lroal l'*""'lOQOIO\J)')
~
'"
"'"
""'.
GO.
'N
{l.8Iin:
~ll\roI'ItmI! · ~
<lil'fl,$IM"'eIgn1&/1
~.
~
'00
""""'" ....o.r..fOdOff"/ - B1'''''
..
""
"'"
<OM
_<lor· R4
'H
CIDP
OW.
II1et'lO';enous nlAlloonatJOl'l • 835
<:arol!d-<;a<;811"10<16 I _ I I\$llIla
•
'"'"
'"'
'"
d1og""'* peritQn6a!IlI• •
dogit .. ~trlldoon angioQf8rT\
~afNe ",me _32:l
dur.1 ....." 1I'IrO!r>~ - &88
etMI-.k Marl cbotue
GO'
CCHD
or
a,;p(01 (l.,.r,toaiICYIic 1<><1)
u""",,"poMIl>IfI
DtrtIl~~,
(at DNET) <l;58fI'b)'opIa.uc """~
""'laI fOOl anll)' .OM ......, • l!15
~1'.&IIOfataryd~f~
~
'M
'000
dl.bel.. melI~ ...
anlllI"'UoDomorI/II o.mirIoOtyt:oa.c»
_M1InOpI'I" • 28
p.t!lalll'lt«nC>opl.SlIn lime (0-
bIOC<I~1n
0.
0.
dj_,O:k.,."..".",$O'
OOC
• ,,,mO ·OCCrN'" dlSIO<:atio<1· 717
~,
'"''M"
M'
""
""
''''
""
~
acou511c: ",..,,""'" • 129
_nSoclery"'A.n ..
""" ""
.~
~
. ....-
.....,..~,,,..IIg_1
~'"
--..
dIs!lll atl'erioo' ~retw1ll .~
00
dJl""nlial
.1IIJ2
*Ilel.. ~~-'6
<'e/.llyed -...rcNuroiDllicoe(C! · 791
d""'""~tIie~""'81h~ .
""..rIoI llIn'Ilir "'tert>o<!y ,.. &/001
....
CAe ...
..,
dilI..01!u'Y ·uz
"leu""",,,
""
'0
"W ,
""
, a..a....
'"' hI,"""",- 409
'"
'"U
'"
""
'"
'"
'"
""
a.ma-ocuw rI'IUICIn
•• I.m.I_OI~
t')'thn>CY\l' ~ .....
aIoohoI (~~)
elJdQl"'I:IIetiIUo.
' ' 1'1
.o\er...... nIr.,.,..,<II""'I_~1
F""""'nall~" """"..,. . ... - 901
,--
~,hhn....,.1IId """"slon
'''''''"'''Y (oe
'lbrorrlUX~1at ~ -
53
"'R'I· 135
~-.
1
....'OI..,_<>rIQIro
p""",,·.mInotio\ynC aclcI
gliotliulOlNO mt.II!i!ctme - 412
G.s
Go.
Gu,'oIn-aarrt ~ - 53
'"
=
"
,."
~"
,,..
'"'
W.
'"
"'"
""
,,,
""
Glasgow<X)ma oc ..... - IS-C
G/""" .. d"" ....
.
00
"-
..... y
~I""~(mlc'_y)
gianl eel anertlis - sa
GI>{I!ie!mI ""'aeIIlb'" .",;1$ - 803
glillll,btJltary -.;leI", "''''.''' • 500
g""""\I"'amyI~
germ""" maW """"",,,",ga- 861
gram~'ods
\IV-~
lIt"""'iUO f<)n~ (...il:Ule)
M""'"*,,, . ~.
,"",nl _ _ (SAH 11'_1 - 180
"_,I.. B....
~_
Inl'll'ln
"GO
t-o.miIled CQfYleaI <be: - 31 B
IIydn.teflllllul • , 80
hyperdyNmo: ~6rl'/ - n7
l"IemIIngjaO\HIa - '59
.,
human 1mtT!\l..--.cy viru •
I\ImIt$ed iIwn!>e' ","".!102
Hgb-"'C~"IC
1>U!"n... ~OWI/l r>oI"""'"
HHT
nor"""",), .... ",o,,1I.1gic reIq;,cru!a _
i'OH
"~
"~
~,
...
Iv:nan Nl<lkocy\II ",,1910
~_9<1
_ . purpoo ... (",,",la'lt(!
"""'
d.scl -302
"o.
"'""oIbI!CI
HNPP
1lut0t!il1ll'{ I\Il>ropll!l>y wirII "-1lo1il)l1O
.",. DIlliN - S54
pt"'-
NEUROSURGERY
'"
'"
""
'"
""SO ..
""'
0'
"''"
<"
""
''''
,~
IPOM
."
_s
~~rI,O!·""'-POI",lIIl)'·.j,eovoI.a.o."
o/rnpIIlo _
h"'M· 22:5
n~_1on
Inl1iIrt\AlaullllO'I'U","'
1nI"",.. .,.,\I ~"I'>e<nIlOmiI . 67~
In!e'"," ""'''tid
an""
'nI'~_"'"!I'I-8<lU
I"uacr_ ~\'QefI ,,","'" (Incle_1CPJ
p'_,.. · {;41
inlrect....
In'~ ... ~8'.
urO/
~dIabelel m.lIitu~
1nQ<II5cIi . .... 0Ihe!rN11"-'1P)' - 307
I........... oIeeItOllI1OInIS
lnsu!If>.i~o growlh IaclOf'1 ("1(.l5Of!lalO~
""'C)·4041
kI10palhic InIr~ - ~V"""1Mk>rI
(pseL.<lDiumor "",1IbrI) . 093
IItiWOP \<IkIpalNe itlI<lIC1ar>\ll ~e<>slcn wllno'"
'"
we
'"
'"
15"T
~Mf!mI' ~95
. . - , ap/IT,,"imoplegle. . 565
inI,matkll>Aj """""Il<fd '''UO - 2.l
l6Q:Ialllic parJIy~IIg1!""" (P- - . , ' "
dlMne) - .,
I nlern~lOnaI
SUbaredlnoi<l " efll(U"'asI'>
" " - " T riol_ 803
"""a~tallleler
P"SII (mediellllol'l ro\ll4),or
'"""
ln~,,,,,,,,," ~'.m (H"'~)
CO,
low Datlc pain
1rO"_
'"
"
,,~,
~G
~
U"
''''
U'
"'"
""
""
.,"
MAOI
"'"
"' AST~
....
.,"0"'"
~
~
""
N"
"O~
N"
-""
MMP'
MPTP
."'"'"'".
~,
foIrll pof;~"", ",,'lSI!
lOW", moIO''''"""
_.!l'IOIe«J ...... IIIg ~1 ('_1/_....,.rin3)
lola O' coJltC\ou'nU$II_P,-"",,,"" - ~li
rnotIO<I ..... o>klaa. inhibit",
fOIl"" . ~ m~1 p'~S<J'e
""""
0"'
_IHma",,"""""'.
pl1et...." •• 4
'::r.:::!PwIl
8
...1' asciculw
"'" m)'lee ..
-IMV~
"'I"'Qflenlfl9ClClrie' " ~; '"
muU!JI4elll'/elotM - 5 , '
Pe/"""iII'/ ""'_
1-I1'1'1II")'I-4. ",....,,-1 .2,3. 6"'W.~1'd'0Il1'"
· 41
MR'~y " ' 37
I!IOIII'IICI1Jn,e~ISJ""'.I'~"''''''
fI'I<I'~pll1 KIefQN • 49
m1c,O'.sculir 1Ieeomr>re"*'" "385
IIIQlectllar WBlg~'
Na 0< NI! "$CXIiUm
nitrou. nxid. " I
NM
N·acelyl.SPa<!aNl " 137
..... SCET NoI!!l Ame"'." Sympt<ol'll411e CIo,Cdl<! Eft.
... rtrlreclO"'y TriaI - 81.
"P
11.O.~" . nal~ ~ no40"'~
38
.'' ' fO..... 361
norI°'l<!<okIaI .n'~amma""" Or"ll • 28
nM1fll/III <:411 eatr;e, ot !he 1ut>iI- "&Ii
...
''''''''....,.·3
_"ItId...,milinU
.....rca!O>n ~ u.. RIII9tIo! 1o<!Q<1UdIf>aI1lrl'"
menI' :148
0I0g0C_ tNt"<lS
I" CSF/_ 51
OCGIpdoillOl'l<l'l"'" Itaclut8 ·121
~;II-lfOl1l"''lelld) drcumle'...,.
OfI'I""m." Jln """"""" «:'511"'- X"1fo/ ."...,
~ PI'''-'.(01'1 LP)
(II;lltar~~raphy·811
o~""~m"l1.<~tlof,
(I.. witl\OUl pre&c<'c)\iOI1)
<>... ' ""
pall·af1e!i\llesi. c-.e .".., (AKA r~
PM)
(<>t~)
arl.rn.s'lOdoY · 61
~""" .... b,aCl>/al J»a>rus PIIlsy • .562
.'7 Dr
~,
~''''cc:y101'M -
~,
P"e>u""'''''' _,,"ion _
~,0I/lI0Inbjn complu """"""tt:olJo • 24
..
'"
""
,-
'"'0'
~,
( ~II'l!\.
~~I
IIIOfph"eSllll'"
moIOI vaMlde acclde,u
<>t~Ia<~ ",$<1"
normlllll'''''''''''' i>yd"..,.~ •• 1l1li
neurOplllI1oc ~n
ossifles!ion 011"" posle<ior lDnglIuOItooi ~
on
myo<:IItIIlol "'Ia!CIIon
~
--
RUOIl""'' ' lube
ocuklrnoIo. ~hird
~' 1
opHr: _1I>e .tIIl~I''''''''· 4911
-.....
-~
m~.m
..... nCIII _ _ ' .
-~ InhltWlofy OOI>CO<1tr.,lon
enltroooli!iof
","",oJib.roma\olIS· 50\!
_I
""
ON"
""'
""
"'"
""
- -'"«'Un,"
OR"
'"''''" '110,..,
i>D'r
' CO
"'"
,.,-
"*'utIoIJ<asl_ ~ 413
1IIiadIlIl;4lret>ta! 811ery
NEUROSURGERY
~
~
So""'" 1nde. - IlOO
nIISIl cannl/l.
"
"'"
"""
NSAtO
NSClC
~,
miIIl!Il}I. n ti"'_,~
N"
NW
""
'''''
~,
~$aClltlorf>c.5il
_
,~
_"""""" OIsordel, , 5Ol!
_~1on~ 'I'
fItI<101lring
pG$ln, ,,-,lII>'aI ~
WO\9"'
.....
"
NO lube
~"
10<*'11'_ gIioml' 4G6
_ mcltct>la,
IIotxltan
MiMoI!I01a ~un'I>N&ic;
.....
,~
,~
."'If ,.womlty
_r~""1!
modlfiIKI
'"
'"
'"
PLED.
PLr ~
'"'
'"'
'N'
"'M
''''''
''''
,~
,~,
•
"'m
orr
"'"
""
"',
•
'"
""
P!riOiliioI
PM\AryCNS Iymp~a · '61
PM'_ CIlmmunlc.11ng ""0<)'
~bu.I"'. CCNU. l """,",,1M (cr.tmOItwnpy)
~.",
U>JIIIa...,. wedgl
~\en' ~u •• ~.rl<> ....
pa/nlul diabellc""""", ... n,
~.O.MIn!
• JIe
Physlc:io:ns De •• F!1!1~
~iaUni (inlillll$ &
dnat'N
pCsllruo emlssioro ~ (SCIII»
.,..,."'"
",,1mOn.>ry luocIion ~
poxlr...,..,.,ic ...."'90 . 367
p/>ertyioIn (tliI.lnIin8j- 27 1
pn1<!Il'" Inl...... ctlet>ellllr 111161'/
I!QOieptIIorm CiIc!IatlIOs
In\efDocly fusion
poHioaoc "'.'~i
.....
pos"""
P1C\1"''''''"'""'"
",u~k>cIllI!uII.08nc;epNIoI>a.
1I'tJ ~ 23'
.,-
pctymy.lgla ' ...... maIlca · 61
~iIc"" ..
P1im_""
__ """ 1_ - ' 12
~~~
PG"",'h1i<> , . .SIaM ~ynllI8!1c PCN
JIIO!I.... _s~"'~-I'IUOI8at ~" o B
petC\llMl(M)U' SIfi~ rniloI<Irny flo!
~_f.IOiA)·
36C
plllionl
~)'$i<:1III!\efapy ; ",ptOll>follll)ln I,"'"
pmgjIOfleOUJ IrigemlniOl IIIUo!Omy
IIIn>mboIA$lln IIrN (0< APTT)
p.o~1IIi
pepllC uke! oi3e_
_......,.," .. ~tlHopLI.1V • 7~
l>I~uok>n-welg!>l.o irTwIgIng (MAl) "
AA
(L.'I1!; ~""""f
meuflllllOlcl
rills
,I'V1 1e
,""" ~ ttrroI
_ _ """,encr "';'Dlomy
,~ lec~\ia l .o) LacIo, ¥II
136
•
....
'"
',.,G
""
~·PA
.n
'"
""
'"
""
""
"'-,
""
.,""
"'"
""
"",.
,~
,~
'"'''~
,=
"-'"
~
~
'"
"'''
'"
,,,,.
""
"'"
""
'"
"""
".
,., ,
~
S1 1R
..
,~
~
TlWI
'"""
""
"""
"'''
_ _ ...... CIIIIgIc .....IciI.!I6t
,.
-~ n..t;opy ~ G""'II
RMooIion
I'~"
_WltlYOI_
r._
........
~
(AJY, ......
__
~
...1
~_~
(or XRT)
~ i'ltomotrl'llge '
111
m
/ug6I<) • 889
IiMuI pla""'"""'ll"" IOCINalOl
P.~ ("" WlI)' 1300
rm.!O
II>V"I'
"' ' ' _"'II toDI""""':
O\.KA TS,HIIi
_-......·5().IDI
w......... oeJ1tt14
II>ytOIcI ·MlIIO .....1itIg I'l0l.,,....,
I«A l/Iv!OIrOPt"
~~~
"" ......
'"
""
lI.nclala o..JalOn
SIJb<I\IraI ......,.,..",. • 223
"""
'baC_~r03l<I
~
superior - - , . . . . , . ,
stMM .... """' ....... ~ae
NO
CO!.
optIal
inIu<\' • 8i8
SIOI"""'~1OIcI (1IlUIC1e)
h .
..-...alhemI\Oma · 612
""'lUI ep/leplicul (/oI .... ...n) • 26<1)
II"rW opId.,,-, ab ....11 • 2~O
1000SSEI') _ _ I'ISOIl~~
apea/Ic QlMy
sy(ld_OI~ •
..,.idiult!lo:ilo>r.
"""'" (AOH) seaelkln· 13
tud<I.n " faflt de"'"
syncI'_
""Ilb'1aMf
""""II <II~
Iysltmie ~ e"l'h_POUI
... ~ i!)i ~_~r~
'"
WI!ut-1!OI1
'Mom",,,, ...
_~
.
__
,.,bo\ItIne_1r<jee!Jon
1!etw*1ic: r.<!Ica.IJ9I<)' - 537
(or 8Ep) _--.v ewI<eCI~
-tOIIno ~Ii!i$.
lOW'''''
Mltc\lo._~.~
",,*;0.
'.5
_!"-' .....
~
1....PDlIII.ne.y
Su~ T nllltl""'l'OIIebr"' I1
__
·M.
_
· ............ .....-tUlllirnlop)
~\UIio:_I"
___
::,t._1cuIe!
IK",..,...
_ . ",
T1~~ !CI<1 "'I'Ij).,3oI
It ~ IINOe ~ IoIAIJ• 1:15
- ...
"_bl*'itojo.ry
1\1CyCIIC..,~
"8RIC'_~
-~-- . ~,
1ilN1O_(""1oCFI~ . ,
10*--,_,.,......
11_ _ _111(81_--""
Ir-...
"'0"'
"n
""
'"'
"w
"""_ ......
l!Ir<ImOO!k"r~_.
----.
~..,.....
' " - otI<ICI.O',ICIn$ ' ~
~"_'
~ DlIOI1I oc,tc:Wo (..... MAl)
..-y1r"",W.*-
- ---
upptoI ""tlOty ".ocl~
~
..wy.,,~
...
..nMIIII_""'"
.....W""'"''" ==
....
~
lGN
1riC _ _JulQIoo. 371
T·H Iw1eoo l~ . .....,kIo\_ - 1O
flA
iIcfII<IoIc 1IIIad< . 1159
• _ _ (.a-w)~., ' t
"~
.,..,110<-..1 ~ InIOlObocly "'....
nso
'"'
""
"
1Mf:lpy
.,;gr..-~
__
... acw.1Dr
I'f'I'IPlI*membrQ".
b _ 1 momcuIat 111;,,0...... (1OITIaUj!>SIo;
\IffIt!I! •
_~u...:.... (_)
.•S9
........
111..., ____
~
- --bng,, ......
, ..,,-
'"
_
.. 0rgI0nIt ......
~-....,. v.._
tat RT)(, _ _
-
Rz
- ""..,,;-
-..10
-•
causes Of
"*"'"
~
-~~)
--.
~ (~$OMI
In 0n<:ribtIg ",""",Of Iefri.
-J
.~oIlNlII~_
*
•
1:
,.
0
!II*.""_ ....
........,
~'~~' "
_ .."",,_\JRI.~
medical pearl.
~_orIIIOIiI
NEUROSURGERY
I.
Ctnfral c.an~ I
1.1 .
~aIol
J .5.
l a l ...... ''''' ...... e Il
3.6'. MiKdllo ...... 84
l.1. "'""'I'b)'Sioloo 84
37.1
8_-Ini~botY\n8'
] 1.2
RcJ:i<mal bniJo J)ndIann U
J .1.3
Jwptar ra.-. I)""""" It>
) 1.4
Poriolallcll:& .ylOdroonoo 17
)U .
801>iftU<i .. '" at
I.l. C r ~c""- l
1.1 1
H~l
1.1.1.
Hl'I'I*_ t>hock16
• .1.3
Nnrop""''''''''-''odom.1
I .J.~I
I.!U.
IA.
1.'.1.
Sit"'" •
n..w.""" £10<:1.01,.... II
Ele<tIOI,.. abooornW,j, ... 12
1.5. H...... 1GIoo I'
1.l.1.
8IoodCCNlOpOflClWihc'''Pl'19
I.l.l.
CooaulolJorl2'
l.l.'.
E>~U"'l' _OIOf'QidI, 1'1
1.6. "" armKO!oc1 l7
1-'.1.
A.......... 21
1.6.2.
Aftuspumod"'oImuock ,.. ....... J<I
1.6.3.
IlallOd.atq»_U
1.6.-1 .
1 1 .6.
" .... h oMl.y ... 9oI
... ,.. hnoiotcyou.\nI..., ....... C).I
4.1 ,1
"'..I\tIoIcI~)'StI.I.u....pl... ~
4. 1.
~.I . t
~ .l.
1.1.
Scd.o,,,... &.pu&lyl"" J6
DtmrfttJ . ....
Iindoch.....
1>11".,..
2.2 .1.
41
I'0Il U'(onyd<>c ...n) Il!/I 46
2..l.1 .
U.
Pa""...o~t<m
U .
M~II!pI ..<..raolo
U.
_)'OI. opllk
4'
49
2 • .l.
J.
Nfl&~ "ri<<) .u98
no
,-,trII' .....' OSIO 51
1.6. C ~IIl"""8""".)'a_ 5J
2.7. M,.lillf!5
U . \'Hto......s.o.r<eIdlISb: 5'
2.' . V-..litb: ......""",lapIlb] 58
2.9.1 .
O.... ,COO _riliJ (CCAJ sa
U.1
I'oly..,yal"" ,""""'-" "
1.9.1 .
0. .....~~,~ ... 61
19A
F"--.onblrd)'opIawl>l
Hlp01llol"",1t ha"",r1omas '"
~A,
4 ~1 .
C'rWI~OO>l""" 99
4.lJ.
Enocph.lo«l<: 102
4.1>.
Chl.r1 """ fo.",.l loo 10J
4.1 . O.nd)'·Wolk... ..,rJfo, ,,," rio<lllO
U . A'Iu.duClaI Ik_1t 11 0
4.,.
N<w,MI I.. t...Jd'", .. 11I
4.91 .
A.~"OI'IM...,....nlJcm.m II.
4.9.2.
Spin ~ 1 dylToplima (spina blf\6a) 11 4
4.1 0. Klippf! .FdI oyadnI_ I"
(.II . T~II .."'eonI J)nd .....
4.12. SpJiI <O«I _Ihonnl ll!>n III
4.U. MiKdI _
_ . 1""......111 ..........
lief I II
1. N.... rotogy 44
1 .1,
1.1.
s..
• •" . Ref.... _
12.1
NtW"Of"Ydlology lUi
V-..J ... d ) "," ~1OI)'
lKCp .........1.b)' 64
1,11.
Rof• ......nt 66
Nturo. n~tom)'
Ynd ph)'siolO&)' 68
l .l . SII.l'l cu,,,,,,,,,,, 6S
3.1.1 .
COt1iu1 ...
1nJoIOIII161
) 1.2.
Soor!..,.~ ., IIIa ••_lum69
ll.l
S.rr...,.l>ndmarUOI...mcolk.eb
rrl<C
"
1"" ., '1I00I. """1.0, 11
J.1. C. , alal ""....
7J
J .3. SpI .... .... d .., . ..... y 7)
J.3 .L .
SpinaicordltXlI 71
3.3.2.
Qe, ....,orntJ.vod .eo.o.), ......... 1.
3.3.3.
Sr lslal cord •• J<u,.,.... 11
J.4 . C.,ebn......-ut., . nlIOIny "
3.4. 1.
Ce .. lxal 'OUO\II ..
l~
H 2.
C.r$'ol _ria, "MlOIf1)" TI
JA.3.
Cc .. blal "UOno" "OftI)' 11
,.ni,Otic-.
CONTENTS
CMtrasl-cnIS'" ... rtneIioIoc1
5.1.
5.l.
SJ .
SA.
l~
kId~ ",,,Il'"
H I
S.11.
Mbcdl _ _. _ 6 4
1.11.
1..1............ llipoom .. 96
U .
4.5.
C .. nlol"o<ial .... fI<>tI"' .... 98
4 .51
Nonnal<k"'iop"",nl9B
/I.iII ;ahihl'or. 010
Itd.... n..' 41
1 6.l.
8tar1c1n ........ Y'icIIo&)'l9
U. R _ n
4. De"dopmt ntal anomaliu 94
oIlaty pep III
R....,hO... lOinn~_u .. <>IIfttm.I
_"Ill
CAT .... " 1]1
""""",""",{ ... ,-m.. lj 1]0
M~ .""""""lmIJi"l(.'tI.1)
,~
Wonna,_ tlol
).01.1 .
Gnoo....
1,4.2.
D;ffIrticM\·Miaf\lCd ,....,,.,. IDWI)
SAJ .
""" per("'''''''i ..... 'ftl{l'W l) ' "
M'IIInelicrcsonMa!-sp«~
(MRS) 1J7
Plala nl .... 138
5.5 .
B. I
SUI! fi lmllJ1
S.U..
Lumbof.oorai (Uhp''' 1010
5.5.3 .
C-S~I"" 1<10
5..6.
Mytlogropby 141
5.1.
80 ... SIjaJI 14J
! ,j.
R. I• ..., ...... 'O
6, EI""lrodtagnosli(:5" 145
6.1 .
Elulrooncep/laiCll'".m ( EEC) lotS
,"
u.
6..l.
r., ....td ""woUah 145
F.Wtt.....'OVOp!oyl'L\.G) .U
'A. IUftr'UlCU'"
"7 . Ntl>rolo~kologJr 149
1.1. Elhuoll.,
U. Opkll&; 151
U . C"""", III
lA . "'",ph.tamlna IS)
1.5. Rd.....,..... ISJ
Il.!I.1.
ocpll.)~i.12?
,10", 1M
. 54
AIIP ...... h 111.11< _ _ "".ifftl 1S6
'3.
U. IIttn"' ..... .,. ....._
119
1.1.1 .
C..-I ............. 100
U.1.
U... "' ......""iooII61
.... IIYpOdr<oml . 61
1 .5.
Rdtt.... a IU
9.1.
'.3.
t.l.
1~
arlin .... th In odul .. 1601
B.. ln .... thln~blld'Ml"
0rJu aod u..... do~ltlon I"
411
CnlcrilrOtqyoJir"'OIICH\I«orpn
...... ,,,,,,161
Orpn...,...;o"", . . .I1 ...;u,1no<o
iIIlJIOIl 16\1
M....Jm>mlIr.. . .'n-u, I<Ir<lr.
931
qJ..l
.ondDtlol1Ofl16\l
U .
IItI,",,~a
170
10. CufbrMpl .. al n uld 171
10.1.
Iu.
IOJ.
10...
10.5.
C. .. r "l~romn.LlQn 17 1
('Sf c"'.. d •....",. 171
Artlr..1oJ c...r 17.
CSf fbi ....
17~
Spon~_
,n
10.0. 11..,.... _
In.......... nlll ~ypOloooioo
11.1. T, .......... ol h yd~h.I'" I n
1111
S""" .. 117
11.2. S hMn.p,o ble""' I~J
11.1. Norm .. p..-.-. hyd ...... pblluI 19Il
I IA. 8Undroao ' rom hyd~ph.I ~.lOl
11.5. Hyd ...."1' .... us.., d p'tplnq ZOJ
11-'. IItlo'*"<a2O-l
Il . l nftttlarn: "208
n .l . Cn>enlial.......... a t18
I U.l
Spoo;ir...... ,booIt<.208
Aotllboota ror ~'r.. lIr&""i...u
'"
11.:1. ,. ... plly .... riunUbiolks21l
1l.J. M."llJi!lio2U
12.:1.l. POSH''''l'OI u''lk-a! procedu",..,.·
in,ilis'lll
U.J.l. ra...mUo.-p.nl ,.. u...........1'...
11.)..1.
IU...
(pO...... _ ;., _ .."",~lI)1 1 1
1I<c~ .. _nl,.lli.lI1
A""biotin lOt
<>rJIfIISfI'"
.pe."''
1.~.21)
11 .... Sb .... IIlfHlIon 1 1(
12.5. WOol .... lnlttlLon:o 1 1'
11.5.1. L..rwnr<' OOIy"OIInd I.....KliooIll6
Ilob. OtteomrcUIliol lh,oj,.ull117
fl .7. C....bnI..b&<:<$I1 I'
11.7.1 . .s...... ""..-1 ........1."" fl<'>dll<; .....
.111
U .ll. Paral.k 1,nfr<1ioolt ft"l1< e NS 2J6
11.14. FIMIpI ;."'dlom .r .... eNS 09
11.15. SpIDf ..rift ...... wt
1115.1 s,.wI.~_a. lotU
11 15.2 . v. ndonl.-.....,....'I.' !4l
Il.!D. 0;"'1;0 1('
11.16. ll.or......... 151
I3.Sdzurl'S !56
..
IJ .I. StlruH ota..II1<aMon 15'
tl.l I
fOCIOnIll .. Io..-cr''''"''U>ftI~~
,,~
1J.l. SpecW '111t'> 01 $tI.~ra zg
Ill. l. /<4"CIMd>e«om:sl5S
III J. 1'uwno.l'-"l<lDRn 160
t).l.J
"I<ohoi witMrlw.~ ..I,-.}Iol
I) 1.... Noarpikp..: $Oit"", WZ
I}
l .s
Fcbrilcu;.~ l(IoI
IJ J . Sc.o"... piltpI1 .... lM
1)".1. o. ..",llJU lmcm ""'""'lIlT.' 10< w·
In
L
11I1<."kpo ino> lU
.... ""..".,"".. for I"nrrlli1C4C011",I .
."•• """" .pilop'iwo UI6
Miwcllaroeotn _ ....... l<1!l1Cll1 :!68
1l.J.I.
"alMpikptk ..... p 161
IlA .1. C1W,r_ofAEDll"
IJ....
IH 2 .
119
II . HydriKfphaJus 180
11.1 I
M ~I~loeal ~1rl«1"'_.Inol<.... •
12.10. C., u i:I.~IdI.JI.oI>d"'_ U1
12.1I. NOll rol"lk" ml nn.. ~ll ..... at "' 1I1..~ %J(I
11.11 . ..ymc diHloe· ... ....oIo&I< ",..,IIttt.·
8. Com.1S4
U. (; .....-01
9. Brai .. duO.
....... m
SuW"""~"'P~"" UJ
IU. \1taI oacqo ..... i' b US
n ' I
He<po> ..""",,~ mcc"".liIk 1tl
n.l.
Ooat""oI"'I~leprc"",,7M
IlA.J. A.I..........u.fIl~r')111'l
IJ.!. Sd.~" ... '"Ift")' 181
13.6. 1I. '.rrnra U6"
14.Splne and spl ...l ronl 189
I ~. I .
..., ... b... k ""In IIDd rld •.'uJ<>polhy 189
lal<r • • rt<bMr1 d isc .........1I0 .. :lG I
1~ .l. 1
Lumlwdisc IocrllJltiorrlOl
1 ~ 2.l .
Otmut di ... h<mi_ 111
, _rc .."" ........ ,;..,,)7.1
1• .1.
,.1.)
1• .3. ~yt.iwllpl.rtlloeMtJlJ
IU .I . St>i>rol)l<""o,,,ns
I.... . C n~lcaIjlrfl<lIo., .... uWOl' ......
,~ .ptno .IoMruIIJUIN JJ6
IU . 1IbNa>I.oId.rtbriU.n1
1 ~ .5 I.
UPiJtf«f"41.,....... -ol ..c....ru
'"
1406 . P. ,eI·.dioe_:l4O
14 ' .1. p~·.<Ii_orlll<lf'!""141
1• .1 . .......)~ •• .,......ylllilJ4l
" ... ()Mifln,1DtI 0( tile pOIl.rlor ,""Iadl.
001 IJpmcm (OPU) :145
1'-'.
o.IIIau...llf cho ..'ttIork>a$il"" .....
lip_I (O,-\t.t.1J46
I ~. ". OIIT_Id "p'''IIk_'''h~lOIIb
,..
lUI. SpinrolA\lM.J41
1(.11. Spll>1II m ... lrlgHl <ysl$).IS
I~ . IJ. S yrl ~o",y.n.
14 U .I
J.t9
NO/H."" ..... i<
"l'""'....'~I,. J50
CONTENTS
I ~ . U.l.
PosI"""","IIC .y';"JlOITI~U. 3S I
Syringob<llbillSa
14. 14. Splul.pldll." h . ....1O.... 3SJ
17.1..21. Mooilo,...;,u,prinwyt>l\ll.,U/lIUf>
1 ~ . I).l .
14. 11. S",,,,,I'ubdu u " hot""' ....... m
14.1'. CO<C'Jdynl. JSl
14.11. IId~ •• I>«S.l5S
I S. Functional
n~uf"1)5urgtr)'
36S
15. 1. IIr.l~ ",. ppla ~ 3M
15.2. S""IkaL IrulGltn, of ... . kl _ ' . cU!..
I S~.
- '"
UA.
Tor1ItoIlb 376
Spa>tl<h)' lii7
15.5. N.......~IK"Ia. «Impnss lon .)1Id .........
'"
15.5 .1 H~ml fl<i.I_", 3 1 1
15.6. KYp'rbldn>d<51 J7J
15.1. T ••..-J1J
IS..I!L. Sympa,hec'OfI!J'J7J
IS.... Rortu _ J74
16.PBln 376
16.1. N..... _IhlO' ... u.5Jadrorncs 376
16.2 . C r . ~ i "rori .1 poUD .y ndro"," 317
16.l.I . "l'ri,• .m,..ll>Oural,1a 373
16.2..2. (a">$"pbAl)'n~ ...>nl!io 186
16.2.1. Genicula .. I>OlIrol,11 386
16.3.
Po<~Ir ""IU"~. J8'7
16,.1 . ..... po-ond ...,.." J90
16.' .1.
16.4':'
16 A3
16.4.4.
16.U .
C.. do!GmJ 391
Corn",\.",rol myelOlQtI>y m
"""".... midll ... m)'1!kI<Qmy391
CNS nar'~ ic od"'in; , u","",)9)
Spin. 1'Old Jl;",u~ioq (SCSl195
16.U.
o..p bt10iD "'",ul."oo lOX
16.4.7. Onnlllt>Ol~"'1}' <OI'e(OIlEZ) ~
rion. J9S
11>.'.1. no.l" IIOlomy J%
16.5. Complex ~ poln S)'lIdrom.
(CJU>SJ J'Ui
16.6.
'"
17.3. ..edl. llk bn ie ''' '''''" "-80
17.4. S/.;uIIwm..... "-80
17".1.
o._Ut
17 .~2.
tI.mon!iotnl4BI
Epl""""",d ... dlknnoi.llUln<nol'
...... ,~uIl481
Eo.'nop/Iifo< iranllk",,. 482
No.·n«>pI ... ,1c . kullie<io!>. 4S]
17,01.1.
11.' .4.
17 .• .!i.
17.5. C.n-b<. l m. l.o5laon ~
17.6. C.n:illO<MlOW _nln~tJ . 4 9 t
17.7. Fo,amtn mlinu", '"m0l"1 4,2
17.l1. Idl"""lhk "" ' Knul" ~y ..."rnMlln
'"
17.9. Empt)' H ll.o . ynd, ...... 499
11. IG. Tu",,,.. "",.k... 500
11.11.
dJ .......n501
N."•..."......,....
17.11 . 1. t-kurofob",maIOI;S 50!
17.11.2. TIIbon)U<tck ....
,.5OoI
11.11.3. Snav--Wd.."yndt""",SOl
J7.12. Sp;... and Of'ln~1 _d IUIJIOI"l Sll6
17.12. 1. In\Iamt<I<JIlIU)'
1COld I.""""
Il .IU . BontI",,,,".oI' liKSpII>OSII
17.12.J. Spino! rpidll ..1 OI"O>!.U<:' Sl 6
11.11. Rd' nna& 511
18. Rlldllitipn thnapy 5J4
...
Ie.! . Con.rn, IoQal
IS.II .
1&.1.2.
Rer.,me.. Ml8
11 .2. SIt'tolloC6c ndiOSUrtltry 5J7
Iiol. IDltnlltial ~ """lIy u.."pr SoIl
18.4. Rer. , mmo Soll
19.5ttrtlllactk surgny 545
L9 ."
Itd....M ... ~
20.1 . BrKhil.1 plt"lIus 55 1
...,lphtroL IItIlFOJ>I'lht.. 553
1Il:2..1
MI..,lelftjuJiduil"'rip/l<r.Il"" .....
l eU.
17.1. Gmt nol l nro ",, ~ , IoA oiOl
11.1.1. Bnti....
,.ldinlcal ....
"""$· '....
pK"~
1O:2l.
17 .2. 1'rInI.'y bt.iDlu"' ..... o!O&
n .2.1 . IAwil"",,!llom •• 4Oe
11.1,1..
AJIIQC)1Of1l1 4O\l
172.3_
OIlg<Jd< n dtv~ l l _
11.2,1 .
En""P'I"'nl """opol/llu 563
XI.5. lI er......, ... 517
4D
21. Neurophlha lmoklgy 580
Ct"""II>O"""'Ylom ~ 4:!5
lU .
1 1.~.5
M .~lngiOHl"
A~"'lku"'ml419
11~
11 2,7.
Pi,."'lr)'adtIlOmU08
Cr.taiql/llr)'ni'orn.4}(i
4M
Ihl/lu· l ct.n~~$I4H
CoUOId~~"451
tlr","nSiot>l"'omI4S1l
CNS Iympll<l"" 461
Cltor-cloml ~ 64
112 .14, alngt""liomI466
17.2 u. l'.... i.,,'~om. <I61
112.16. EpondY""'mI~7(l
172 .11 . Plinll!l"" l>Ouf"llCClOCkmMl "'''''''
tPN€l)47l
'"
W .3. T ha,ati< 01111., $)nd""". 516
2004 . Misc.II."..,.... pc-tipbo ..1n.... 577
11:Z1l
.""d,,,,,,,,id
11.2.18 . fpldmnoid
ru""", 474
17.1..19. PInul •• 'io!>rurnon .... 7b
17..2.lO. Cltoroid pl.~~II~""""$ 479
CONTENTS
tx'.......1bn m , .,II", lon
Cllnillllll •• " ... SJS
SpiOlI rad ,.tlQn SlG
ZO.Pulpl'lfrll l nerve:!i 548
11.Tumur 4(11
11:2.1.
11 .2.9.
11,;UQ.
11.2.11
11.2 .11.
t7:2.11.
'1',...
~.
NyotaplUl 5SO
I'rIpUltdtma sao
21.l. l"u"'Il.ory dJ~Q""" sa l
"21 J .t . A~ ••• """. In pupillory iii. ..... ' • • Sal
...
.j'l,....
1l A. E~' ... ocu l. r .... tor
S84
1U . Ml$«llIInrous /ltliropbt/lII""""ci.
lUi.
",
RoI"....,.. S89
22.Nt urpjol0l0' 590
n.l . OiQiDUUJHhffl IJo5'"
11 .2. Mm"",'lr dt._ S91
Uol . !'odol ,.. ..... pWy 5n
21 .... H" rtnc tos< 5t7
11.5. Rdu. n<.. S ~
D .Ope.r:al loru; and proctdUR$ 599
U .I. 1""lOpr",.h. d,.. 599
U.2 . Opo ralinS room .... "lpmeM S99
"
2.1.1. S.... t;I<.1 h.mn<UIW IiOO
23... "'n,erlor I pp',,",ch... 10 ,II. opine 600
23.s. c..""lolf.mln 601
13",.1. POI'.rlOt 10011 (~boo:fp'tlil
tf1II,e<tomy 6O-l
n',l P\cnOnaJ c""'~O/II) 6011
lJ ..'D . T.~\P<'r~ '''"''''amy 60S
U.5.4
FIOIU" c..niolomy ro9
lLU. Skull ba>e "or&",), 60\1
13.5.6
Pwol.1 tI. . ~omy 610
"21-'.1.
"'ppnw-bo. 10 tho '''....1 ~I<
'"
n.s,l, "'Pfl'_b<~ . o ,lie l ~inI """trick 610
23-'9, l .ttJIIo:m"~k'_'h611
1U. 10. 00<1", ..1cruidomy 612
:U .6.
nklp!uly6Il
23 .7. "~~rIo<lpp ..... chalo ll>o . pI ... 61l
Il.l.l
T .... .;or.1 0pJ>IO"'h <0 anttllo. c..... _
10(1"\'0001 )""",;0" ~1 J
D .12
... omior ",CC$S 10 ll>o.Uf'o 0«>-1110...,ltjl.nlo,lonIuppe, ,ikn<ic "P'"
e...
1] .7.l .
."
n.? ~
"';';'1'1",,613
"'ntt"'" OCC .... IO Ihorat:oI\Kr\lw
U .1",.
"'n"""" .«nolO mid"
J-<'_6 1~
... ....i.QO "'«MIO ,)&kMt>bAt.pine
."
13.8. 1'm:tt.."""... _
1) 1.1.
"lU.2.
lUJ.
~1tIo·
".
VOlllm."" _ . "'100 621
""'<t:I ......
2).9 ",
rinrloolOn[y6U
1).9 5
LI' ..... IIl 621
ll.lO. s..flIl ....... bIopoy 521
13.11. Suf"Jkal ' lISf"" of Ui. ~lcahpIJN W
lUI I Upper "",ylc;." .... bl..l
un. 8_ .... ft 6U
1l.U . N_ bloo:b U7
B.IJ.I . Sl<JWe pnJIiorIl>Io<\ 621
2).132. Lumbar" Iymp.doclle bll>cl 617
HoI).J
In_",,*, """e IrIoc:k 621
!l,III . lI de...
....,.n.
24. lit .d Inurn. 632
M.1. Traasrtf"(>I'1.." .... ,..tiottll7
Mol. ~bn ., .......( In EIR 6J7
14.1..1.
Nar ........ ocaI ... """~ .......... lIl1
24.1 .2. It~ .. no _ _ 6010
!H.3. EIIt .......' _ ......r... 64 1
20'1.... &pIonooryllou .......... 64S
14.3. 11'1_ ...... JIfUAInt-'1
M.31
GftIeral"'f....... _ _ lCPfIol1
14J.l
ICP _ ....1... 1\019
2A.J..I
Icp ""..",... _ 1 I »
2A.3A
Hilh-drcrK bartIo_ dIcnpr 1161
:.... Sk .... f f1l<ta<a 1064
14)1 1 PtpmKd"'ull fr..... oes~
20''' 1. a.. ..."u (nco ......
us
•
c•.....,r...;.! ,....."" 661
...
S ~ "\I
'rllC ... ,~ .I" podllln< poIlefttl
14.5. H_
.... "lcCO)ftI.oIo« 6119..
!-l.6. Epitluro.l b..... _
669 - "
lA .7. Subd uflI' lIo",ol<lfll.l,n '
241.1.
........ ..-""""-671
Z4.1.1.
2'-13 .
~oubd ....l
14.7.• •
",l,oll-'
o.""",,"-rW""InOIOf1t1I17<t
_
'"
T......"..io-..lllyt_li71
E/; ...... ioI n.. od <"OI1<rcUo<to ,0<hOl·
dofn 678
14.... Nuu;.1on In 011< .....-1,y..'"" ,..11...
.~
o..'-.efrom"""'ln_'"
...,.,681
14'.
1H.1.
"N.9.l
1"9.3 .
.,
OU!CCOD<~6I1
~"""",Ii<_tr_""",,,'II"'Y
2otJ I. G ..... IIot ............ to'~r_ 6801
20'. 11. Noa....u.llr ,.-rodflllho& .......... ci86
24.I!. HIp ........ _
....... 681
:.&.13. l'edlIlrk....., '-Jury ""'
14.U I Cq:rItIItt&matamI6&I
7~.IJ':'!
Ch,lcl_ 619
101 •••. Rd..-- ' "
lS.Spine ill.luriu 698
IoI .... c.."'"/Io"S6 ' .
1'1:","",,_ ....tlicul.. pun<"".
Su!>Ou' ''Uopbl.
lIIml>Arptoct~ ... 61~
a ..... CI.2""nc:,vrcmdc,wrmalIlop6 11
D.9. t;SFdI"'nMlul"]' plD<K"tft ' "
2).9 I
VC'llnO;ular clll\l!tonufloa 619
23.92. V~n.n.ulol.lOmyIlC P tMAi ..... 6;tO
13 9J . \1... 01< ...... ,.... 1120
D.9.4.
•J
! • .~...
~4
2:5.1. W •• pWb-'-'",~,"
U.1. p.o;',u"" spIoo
U.J. l.iIIIl ....... _ . of .pIn&/CO)'" "V....
I.j_""" '"
o ,to
15.... N......-.p:.I_I liO
U.5. SpIJOIIl.-I\-.Iu ..... , "
IS", .I CornpItIO.,...m ...... iaJlUlO 713
US.:.! IIICCII!lI'ictelJ'ifl4lcoodirojufics714
IU.
koII'p;,. rntt .... 717
1.5.5.1 . Ad"'''HICCipioaldllloCllloo 711
e.....
e
IH,l.
OcdpitaJ"lltrNC~721
1.5.6.3
lJ.6...
U .6",
U.6.6.
"" ........ ldi\lotlrl IOll7l1
....111 (el) fnrc"''''' nl
A~ .. (01 r.... ~"'. nA .
C_"... . CI .lirtJ"!'Cf7)1
SubUiol(O lItmu,hC7) ,njlr.rlerlf..,,,,_7U
Tn:OlopeO. 01' ... bal<oal ttn ...1Mil"
' . ........ 7)9
Spom ",11lIItI o;e ... ",,1 opi ...njuric.
2!i 61
"B.6.1.
U .6.9.
'"
"2S 6.10. Ptb)"td . .... jcaI i<QllIbiluy 7'J
l!i61 1 91,,", «:ntlnI.....,. in"n ... 7,u
l!i.7. n." - - o p l n c ' '''''lIrti1.w
U.I. ~fr .......... 7H
15.... c..10$1!61 ,"011_ 10 ,'''' 'PIIM\ 753
!S.IO. hntirilloo ....." ....... ,'''' DIdo; 7!-6
:5 J
C"IIn!nk
fJI ' plnll """' la,JuM$lSS
!Soil. ltd, ....... 757
I.
......,...."1
l6. Ctnbro....51\:ulllI accidents 163
;6.1. Slra..1r! .......176.1
2U.I .
16.I.l.
16.1..)
M.I A.
,I!."
Modif"..tIk
fx",," lor wake 764
e • .oIuOlol)ft760
M....,........ 'ofll li'ED.n .... orC ......
".
Card....",," \IonoiuIDboll$m 71J
CONT~NTS
16.1 . eVA In ,o"~. 011" ' 1$ 174
l.Kunor Mr...... 176
lAOA. MooU._ .... CVA 178
!'.5. Ih·r...... no .. 17.
16,).
ICH In ~_..rn:ru
101..-.....
~emoN"'~ In 1M !!.Ill!:.
19.1.
:!9.l.
......,/1'"
19.1.
Md~ ........ 8&!
_...
3U .0cC:Iu'i"~C\'I"dJro· ... sc:u l. r dl5ease 869
..MI.I. Albor_k.or.bo-•• _ r di...
11.SAII .. nd .Innu·Y5ms 7111
n .l . 1• •• DClotctI .... O$A II 7. ,
ll.J . C ..... I•• SA H 7115
n.).
InlIl.I .... ~ 1 ..,5A " 1M
Vuoopum 1tl
l H 1 Oo:r""d_741
nU
~tritrjq: nl «I't\II.J ... _
1U.
n .t.).
-".
Carocid IIIU)' WI
lI).I.2. V..,<bo</booil. i _ff",ICIO')'"
.!oIl.l. Cotnb.. l ..vn.t dbHnMm 8Il
)0
1.1 .
lO':"l
JOU.
C-Id <lll,.,..;...,n,
V~I .. . ~ ... ......,.~
,,,,,,,!86
......
...
P.. boct...·191
le'). £ u no:roalol-ln.rKl'UlaI (ECIlC) by·
17A.l
~.. oI< ...bnoI..-,.."' 191
Tru,,,,,,
.. lor
7904
~1JI.6
V-.pMIII .............. '"pI-.oI"
JeA. Crrrlo, D•
'"
30.5. MoJUDD)'_ d._an
11,4-"
. _~
H.!I . C* ....."'., In.II')._799
11.$.1.
CoIodnlou iHlQ<l _ ," ,' h oncu-
ryn>101
11.6. 'ttftl ....... ~IonJ for l a ... ry.wa.101
11.7. nftllnt or ... M.., ...........1'). I&l
27 ". Cr ...... 1.. /lnk.1 <onlld.noll..... .., .n·
."r1,,",,"~,,1105
21 •• I
In' ~';'·"o","'Y'''' """ . .. 101
17.'. A"" .. ry ... ruur.-e~ oftf,r Ino ''''''''
."
J7 .1 0. "'n,,,,")",,", ,ypo b, loco" ..., ' 10
17.111.1 Anocnorm''''''untull''S _ ry . ... u.
')'Im,I IO
17.10.2 O,llOl ""toe""" <" ri>ral lfICry ........
ry_1 11
27. 10.J . I'<lIotoerior
_I)' In·
• "O' " ml ll
27 .10.4 C_id ~,mll\11:1(bif"r<:...
'"",m"",,"''''
I)'IJIU
III
"""I_...
17 111.5
M I6d~
27 .10.6
1)'.",, 811
S. P""III'o••h"""'l' .....l~ I II
"-no.cirtu'lIlorI"",,,,>_")
n 107
2710..
n .ll .
,. ".!oI ."ff"J' (MCAI . "' . ·
a.lilorl>oflllClllo. ~ 115
U".lIpt"'.......".,......II'
n .ll. M.,'I...........'~ ....."
17.Il. r ....IH .....*...)...... ' 9
_"')_.:0
n . I~ .
Tr'M...1It
17.U . M.to;(llk ..."t'fS..... , l
Clon. .....".."..U
SAI l Dl lllk ...... ..
17. 1'. NOOIaot • .."..... SAil I II
!7. 1, . I"rqMIIQ'IIt 1.. ~I"'_"".e
n .•,n.n.
1aoI'"*'·.n
on
17.lf. Rtf..
_ .lAO
28. Vll§Cull r mll rlWml liOl'V8.\5
"''''''_allo"135
ztI .l. Art ..... _ _
:II.l. v....'"
ZlU. ARc\ovo""lrall, 1M'nI I,
.",I_1l'I
"'''"'or ",11f_a,""" $>10
~I.J . ' .
C..ettIOII. mol (armauon lol t
111.1 . l)u •• t AVMUl
1lI.5. v.1n IJI C.I.., ",.lforma''''" 144
111.6. C ...... kI .... . er nou. n.'~I. 845
1A.7. k.rtr .....,S46
19. hl l ra~rebrlll h( ",urrh~KI' 849
29. 1. In,,,.,,,,ebr " M ..... ' ~1t" In I ~
'"
CONTENTS
Je.6.
...,Illo, _
II............
tI.r.... ...,.. 195
J I. Oulcomr 156tSSmrnl 899
11.1. Kde...-901
32. DilTrrr ntial dlagnt>51l; J02
31.1 .
Dil'f.~
.. j;" d!.ogn"",,, tOO_)
by oi~ . nd .y"""1" .... M
J2 L.I
Myebplollly'102
32.1 2. SclOl ic.a ~
1.1
Loo.o bo<;k pain 901
12.1 4
1'ooI1I"'l'909
12.1.5. We oX"",,I"up/Iy ar ,he h.l.nliolUEr
n
'"
HIlli<:ulap:llhy.uWCI." .. m,.y{CCf'
'1CI1)9 11
Jl. 1.7. N.d po;o (.,.",.,,1 poi .l fl !
ll_I"
1J\tmlJ' ..
911
nJ9
8 ....".S ......wrecl9 11
J2J .•O. MlIKlep:oWlo ........ 911
n.'.'I . ...<..... pcwplqlo .. ql'ldnpio1Jt. 9 1)
12. ' .12. 11.~.is ... "" IIIipI.".' I ~
32.l1J Syocnpo _ _I..
3!.1.6
·.'i,.
) 9 1~
'IS
31 J 14
lU.lj
1!nccpIuIopo1ll)'913
T' .........lII'OIask60r",,,
J2 1.1 6. Diptop..916
:12.' 17_ A....,.,;a 916
12.1.... M....1pIo <nai.tl ......, ~lliQ
(ctarloll ... """""'OUC')917
'32.1.19. 8 ;no<IIl.. bI~9 11
32.' .20. Monactolar bliOldoow. 919
32.1.21. ~91 9
n. '.21. hllI.;lIaslo lid ~ hon9 t'
12.LU. Mac .... .".,..I)"19
ll.I.loI. T;",,;,... 'Y.! I
1l.US. FIO'IOI.......,.,.tlw.rlctS92 1
». 1.26 Looo_ e dislout>An<c 92 1
12.121. S... III> ..,", diff'ICIIKon 921
J 1.2. OiIT./'tfII'1oi d~ ( D()~1 by Ion ·
....,,921
11.1 .1.
Ct.rtb<j!won'i~"," (CPA1""
.ion; 922
:.I21.l.
ll.2.1.
l l .l ....
PO>ltf.... rl)O~ IotOM 9D
Fnrom<n
i<1i<JII1924
".,..'110..101 JubIU.., k., 9:!-i
.... .. (C 2) • • ,.".bf. 10>...... 924
MUlliplc l/IIIac ,.,,'O' lu ...... on CT
Jl.! .!1
ll.2 .6.
mq.o"'''
", MRI9n
.1
31.2.7.
Rfn&~"h_ln,
32:18.
'"
31,1.9.
n.2 .11l.
322. 11
IU ,I"L
32.2.13
32.2.1 4
12.1J!i
lesion.- <HI CTIMIU
U"~ ot""'rIo'"","lhy 926
C<wpon nllOl"m 1Il1
Soli .. ,oil _I(..-I..ion, 9li
IntnIC"'n,>.I <y,u 9'23
0'1o<1Ol !eJloO$ 929
CIWmoI!' jjn<" blQ",929
S~ull "'~iOM 9J()
Comblhtd ,nU-=rlni.lle.o".. ranb.l
",.;o.u.9n
12.2.16 InlfXnI","1 c-okirrcaH""i 9)]
12.2.17, In''''vtn<r\cul.. 1<';011$ 9J4
~i
J1.2.IS. f\>ri .... nlticlll ... l..i""-, 936
31.2.19. M,","Il"'" ,,,kkenlna/cM:oooomtnl
".
JVLM. Ep<n<!) ....1 oind lubop<n<!ym.l,n.
""""'In,,,. 931
32.1.21. I~"""'nlrl<"' .. r.:mom..Jc 9'8
)2.2,12.
32.2.21.
H22-i
J2.2.1.5 ,
)2-1.
M.d ...1!<",~Ilcbt ",1<,",,938
lnlrll\UlllmtrlrC,"",oJ I.. io", 93$
S",""I 'p>duril '"_
9J9
De'ln":".~ Inio .. o! lbe
9]9
R,r.~ce.
!NO
'pI""
'll.lnde,r 944
CONTENTS
- .
~
1.1.
'
Neuroanesthesia
INHALATIONAL AGENTS
MOit reduce ce rebr al metaboli~m (e.'<cept nitroull CIlride, .~e bf,low) by luppre>llling
oeurona illctivity. Thel:W! agenla distu rb cerebrailiutoregulatign and causetlrebral va·
sodilatation which inC""~8es cerebral blood volume (CBy) Bnd ~an increase ICP, With
administ.ratiGll» 2 hMl mey intre""" CSF volume which ~nn alllll potenti nily contribute
to i.ocrea~ ICP, Most agents increa ..... the Co. reactivity of cerebral blood _ t b, All of
these agenla off""t intro-operative EP monitoring (au "bo~),
~
halothane (Fluothnne®)
\
I
ORUQ INFO
\
,
In<reus"" CBF al~ CBV, and decreases CSf' ab&orption, all of which can increase
[CP, AlitoreguJntion i~ disrupted . Affect.. EEG and EP c.u obow), and produees i.oeleotric EEG lit conceutl1lt b ll of ~ 4.5%. Produces cerebrotol<ic effub at lower level. (~ 2~1.
~
enflurllne (Ethrane®)
\
I
IlfIUO~Fg
\
,
A pDQr agent fOT neuroo ne.thellio. III Lower. $ebu~ threihold at thera,P"utic levels
(further exace rbated hy hypocapnia ). CS f' production increases and abi;orpllon decre.a~el
both or which oontribute to increased ;ntncralllol volume a n d thus increased ICP.
~
nitroc.s oxide (N20)
\
/
DI\UG!NFO
\
,
A poLt>ut vasodilator that markedly increases CB r 8nd minimally inCTI':IlU&e<>:rebral
rnetabolisn;I.
Nitrous o ><ide co ncern. w ith pn culno.;:e ph al u Jl and 11.;" em bo li!fm: · The solubili·
ty of nitrou& Oltide (N~O) is ~ 34 times thatofnitrogen' •. When N~Ocomeaoutorsolution
in an airtight space it C3n increllse the pressure wh ith roay ro.,vm pnellillocephalu& to
· w.n~ion pneumoeephaJus", It may also aWDvate airembolisr.."I. Thus cau\.ion must be
used /!!:Ipeci aUy in th~ &ittiRg" position whe r~ signilkant post·op p'>eumo<:I!phalus and lIir
embolism areCOD'imon , The ri sk oFtension pnewnOCt!phalua may be reduced by filling the.
e8vi ty with fluid in col\i u nct.ion with turning offN.O about 10 minute. prior to compl e·
tion of dUTllI closure . Su: PNJllmoctphaiwI en pag" 667,
Hal ogenated agents that m ay provide cere bral protec tion
AU ohhese agenb suppress EEG activity.
~
i.!ioftllrene (Forane®}
\
/
OfIOOl>lFO
\
,
Can produce 1£OI!lectric EEG withou t metabolic toXicity. ImproVe<! neurologic out·
come in CIOBes of incom plete global is<hemia (although in uperim eota l studi... On rala.
the amount of tiS&ue inJury was greater than with thiope ntal").
/
~
desflurane (Suprane®)
\
/
OfIUG INFO
\
~'----''--"
A cerebrnJ v8Godi istor , ;nCfIIO"ei CBF and Jep. Decrl!&llet> CMR01 which tends to
tluBe II competlli8 toty Wlsoetlnst riction.
GENERAL CARE
1. 1. Neuroaneslhetia
~
sevoftu rane (Ultaoe®l
\
I
DRIIGIUFO
\
,
Mildly incre.uu CBP nnd [CP, find reduoe5CMRD,. MUd negat;ve inotrope. Cll.rdiac
w;t.h isoflura.n e or deIlflun.ne .
putpll l not fill ....·1'11 ,mllou.inP.Ol . fill
INTRAVENOUS AGEtffS
BARBITURATES IN AtjESTHESIA
Produce flignifiClln~ redu~tion il\ CMROa and scavenge free radical l llJUongl.>ther e ffed.• (mo pC.8' son Produce dose-depr:nd<mt EEG BUpp'Usion which U n be u.ken all the
way to illOC!le.:tric. MiuimaUy affect EP, MOlit a re anticonvulsant, bul methohellita l
(B . .. vitol®) ~an IOWf' the ""ZllTIl th .... shold (u( pase ,36), MyocaniialluPPreniofl and p"ripher/l. l vllfiOdillltation from harbi turatea may cauu hypoten sion and compro mio;e CPP ,
e$pe.:ially in hypovolem ic plltienta .
NARconcs IN ANESTHESIA
increa..e CSF nbso'l'tion ""d minimoU)' reduce ce rebral metabolism . TIley Blow r.he
EEG but wilillCll. produ~ ao Iaoelect rlc tracing. II All nlln:otks «IU6E' dOOle-dependent
respiratory depression which tan re/iu lt in hypercarbra and concomitan t increased IC?
in non -ventilated pali~nt.ll .
MOl"p h.lne: d~lnot sign irlcantly CI'(IIIS the BSB.
• Oisadvantagt'll in neuro pali\mI8'
I. ca uRS hi stam ine release which
A . "'",y pro<iu<" bypote=i<N,
8 . 1Il4y cauHocerebrovII.!ICul 4r vlUOdi lBtion - inere/lsl!1l ICPO'-'''''
C. !he IIbMe lOgelh~ r ma,y C(lmpromi~ cpp
2. in renAL or hepatic insufficiency, the meUibolite rnorphine·6·glucW'o nide can aecumu late whkh may Cllu8eeonfuaion
Meverirlille {Demeroi®:, has nevt.ive illQl.rOpic .. £feeLS, IlJ)d il!I uellroexc;tatory
metahohte nor-rnependine ca" cause hyperactivity Or sei~W'I!5 (s •• (ooll.ol., f"l8~ 32).
Al so cau.es hl,tamln" relealll! .
Syn thetic narcotics
*
Th~
do.QQL cause histamine rele:ue, WJlike morphone and ITIt!pendine.
Fentanyl: crOSiie5!.he 8BB. Re<\ul;@sCMRO" CaVand ICP.
S ufenl"n il: "IO~ polenllheu fentnnyl. Dc>6 nOI increase CBP' hut . ra;SftS ICP
and Is thus o~n not appropriate for neurOll urlPca l casel.
Alre n tllni l: the mo. t mpid on""l and the &h 0rte8t duration oftt.e oarcotil:!i. • NB:
also raise. ICP.
BENZODtAZEPINES IN ANESTHESIA
1"es .. dn.>gs are GABA aguoisUi nod decreasecerebllli metabolism. Tbey a lso pr0vide IInticonv"I, .nt /lctio o Hnd produce amnesiH. See fXlII. 35 for o,!lonUi lind r"ver..ai,
M ISCELUNEOUS DRUGS IN ANESTl-tES!A
i1:tornlda Ul! "sed priuuIJily for induction. AliO deacnbed far urebral protection
d"riog a neurys m s urgery (Aee pagIIH08). A cerebrova""""ru;trictor , It reduces CBF and
ICP. DoeI not a uppress brainstelTl .cth'ily. Suppressf!I cortisol production with pn>
longed /uiministrJ!l tion, tl.nd rntI)' induce aeiI W'e5.
proporol: a , edative hyPnotic. Reduces ce rebro! metabol i9 m. CBP and ICP. Has
been d~bed for~erebral protection lI« pog~ 8QS)and for sedlttion (_ ptJ/le37). Useful
ror cort iea! mapping where rllpid reco~ery from anesthes ia i! ne.eded (recovery is not as
rapid ... with melhohexital ) Not analgesic.
,
1.1 . Neuroane!lthesia
GENERAL CARE
Lidocai ne . IuppreMU laryntul renex~ wInd. m.,. hf:l~ blunllCP..ue, lhat normally follow endotracheal intubation OT luctioning. Anticonyulunlal]ow doIN, rn.-.y
provoke leitu,"" a~ high I:Oneentr~l;on • .
REVERSAL OF COMPETITIVE MU SCL E BLOC KADE
Ite.n ult. up 10 ~ 20 mlnullII for full rey..-..I ofpancuronium (P.... uJo-o«J}(de pm<i-
;ns on the 1I1'\10Ufll of tim~ .i nee the J.SI dou). Ray.,...! ;, ul ually not .~mpt.ed until
paUln! hi.ll al lUll 1 twitch ta.ll Irain of 4 ~limu1Ui, olh, .....i •• reye .... ] may be intomi{patient ill protowldly blocked aDd blockade UlHf reoccur u the revenalwN.l1Iof[
t
nt!oUlrmint (P,oU.iiDli.c.~l: 2.5 mil" (minimum ) l(I 5 mK (mlUtimwnl IV
(Ua n low , no efficae! /'rem:> Ii m8 aud can prod\l"" M!Vet"e """a~ espi'cially if
the mllXlmum dose II ueeI!ded in Ih e abMnoe ofneuramul!t:ulaf hlocltade)
PLUS ( to preven t brad~rdj •...). EITHER
• 0.5 1011" atropine for each "'II: of IIfiMIlilllnin.
p~1.e
OR
0.2 mg glyeopyrrolat. (Robinu\®) tor each mil otneo!ligmint
E VOKED POTENTIAL MONITORING
An~lhaia
requu-etnenlJi tOlf intra-operati ... e monitoring of evoked patenl.lal, (EPa):
ifinhalatiou.l Mestlletie ag.nl.8 h8'" to b6uHd
A. a ... oid halotllan", isonu rane (both reduce the IUJIplil\lde and intnaH th.la·
te""'y of EPa InGllow Ihe EEGl.nd Elhranelll
B. IlJlWltIF slt.:luld be u.!-ed .. I c:onc:entration l < 0.25'"
C. Nrommend: e.l. FOTllna®.t e I 1>tAC (ide.lly < 0.5 MAC)
nilt"O...m'~lic techruqutl prefelTad
IIIUIIC1e reI .... n ... are pem,jaaible
a>lOid benzo<iiueptnttl
minimlu pento:h.1 .~ induo:tion. Of uK et.(>mldllU: (upec~ _ 30 mini-ltd of l uj)pnRJon orEPs after ;nducUOtI du e to lfIedicotiolll
conlinuO\d infU3ion off~ntanyl is preIem!d oll@rintennitlentinjectionl
1.
2
3.
4.
5.
6..
1.2.
Critical care
1.2.1.
Hypertension
PA.RENTERAL AGENTS
Table l-l show. fOme
parellUtralagent.J for acute rontrol
of hJJ>trtenalon rrouped ba$ed on
their efJect. on lCP'o·.
-:...-/
nicardipine(Cardcne®}
\~L/~--:-~----,~~
::-__\-,-~,
rv.
Calcium channel I:lockl!:f(CCB) !.hatlllay be,;yen
UnUkeNTP, does not require
Irt.erialline., dOl'!! nDt ' ,iR Ice .nd noe,.nide toxi-cily. Doea not ~\lce heart r1\te, but
may be used in tol\iutKlion with e.g. labetalol 01" _101 iflhlt ill desired . 81D1:~
WA I S\\o. nBU5U~, ~iGo S'IO. ~fIO tachycardia 3.S" .
R:£ obln It Ii IJIgfU IV (off Ioobl!l: 10 mr/hr fOlly be used in . iluatiOlll where u r~nl
reduct iotl. is needed). Ilicreue b, 2.5 mgn-,r 1tYfJ)' 5-15 minutflll up W. muimwn of IS
mgihr.
1.2. Crill.,.1 care
,
~ nitroprusside (NTP) (Nipride®) \
I
DRIOINFO
\
,
Re.lktl rep in patients ...!th InlrB~rl\nLaJ ma.,lt!II;on,' due ta dlrec~ va5O\lil,talion,
arUrial» ",nOIlI (111\1111 eo",n ..'; • • :> large) Msy p~ferent.i.lI)' dilate periphlr1lJ .-enel'
b\>Jore eerebrnl vene1,. ltlU' pf'Oduciug. "Ct!tllbl'lll,t.ell" pheoomt!non. At\a in MCOIldt,
dura!.lon 3·6 min ,
11101: U't'R(;1'9;
thiocyonD~
and "Yanidl wxicily (may u .....
lUl'ul1>logie~tilWl'
ifuaed:> Z4 hre, at II. .aloe ~ 10 ~mtn, 01' in
renal failure: DIC ifth.iOl'Ylinat.e La".I, ,. 10 nlll"l>1, tuhyqrdia, Ulldu'PhJtluil, hypo\.en·
.ion which ~an extend II" Ml "coronary l \.eal", "'""id in p~ancy.
& rv drip O.:u.·8 l.I&fl<ctmin (ave. '"' 3). To reduee riik of cyanide toxicity. ltan al
very law .au ofO,lll&l'kdmin, lind do lIot rive maximWfll'1lte of 10 l'Wk&lmin for mONO
than 10 min"t" . To prepllra: put tiO ml in 500 m! D5W (can GIlly btl mixed in O.5W; 10lunon ean be dmlble con(!tntnted to reduct nuid or ,l....aee ]lIIId ) .. 100 I'&lml, C:OVl!r bottle. with roil (I igb~ sensitive ),
or hypotenaion)(follow thlooyamlte
~
nitroglycerin
l~veJ!
(N'I'G)
\
I
0AlI(I;
INfO
\
.
Ralse81CP (leMlMa with nitropronided"e to prefuentiaJ ¥<!nol'! &<:bOn' l. Vasodilator, venD"." arterial lIaree I'Oronari-e!J" $mall). Rel"lt: d~ LV liUin, p,"""ure
(pr. ·loodl. Does not cao!MI 'C(>rona~ stN.l" (cfn;troprusside).
Rs 10·'11) I'efrnin IV dri~ lincrea!lfl by 5· IO)l"0.in II ~- 1 0 min). For angina """'ton.;
0.4 mg SL q II min )( S dotel, check BP before each dose.
/
,..---/
labet9.lol
\
/
OFIUGorfll
\
(Nurmooyne®, Trandllte®)
8101'1(11 III seleelivi. B norHlelective (potency < propranolol). ICP nduc:u Or DO
chance'. Pol.. rite: deeresses Or no chang • . Cardiac output does notchao~. Does not
nM~erbDte 0;:0.0011")' ilO;.lu!mia. May be uM(! in eonLroUed CHP. but not in oYen CHF.
C!>nl ra.indl~ted;n ,.. tbml. Renal failore: urne do... Sm~ ~rn:cra: raligue. din.iIl<!R.
orth~l.atie hypou!n!ion .
Inlravenou. (IV)
Ol"ll<'lt II wil"l', peak 10 mini, durAtion 3-6 htl.
Rx 1Y: pat",nl . up;na; c.'Ieek 8P II & min ; jfive each ckIIa . Iow IVP(oYar 2 min)q 10
minute, until duiN!d 8P adtieved; doae .eque~ 20, 40. 80. SO, lheo 80 wg (900 mlf total). OnQl controll~, UM .. umetotal dOM IVPq 8 b ...
1U .IY...dJ:Ul (allemllive) add 40 ml (200 mgl to 160 rol of IVF (nolull: I mglmU; NO
At 2 mUmin (2 Olcfmin) until d"ired 8P (0 ....1df«tive d_ . $O,~OO m,l Or until aoo
mg "nn; then titrate rate(bn.d~.rdi.l;m;tJI dOH. lncruM.lowly);nno eD"M'1 tall" 10
20 minu,"").
Orlli (PO)
UodereOl!S nrll pMlllivet" degnodal loD. therefore l"fiJuire. higher dOlet PO. PO on-
2 hrs. peo.k.:. hn.
Rz £0: 10 ""nvert IV - PO •• tart with 200 mg PO 810. To ,tart wllh PO."ve 100
ITIIl BID.1UId incnll8& 100 mjJ/do..;e q 2 day: IIIU. "' 2400 mdday,
let:
~
enaloprilat iVasot.ec®)
\
I
DIIUEIINI'O
\
1
An angiotensin"«Klvertina: e~ym!' !ACE ) Inhibitor. The active n1l'.t.abolile oftbe
orally admini5l.ered dn.oe enalapril (Kf btlowl. Acta wltlUn . 15 miNI or "droinilltrat!oll
Sloe EfTICTII: h)'pl!rkaJeOlia <>(:C"re in _ 1*.00 not ""'" durine pregnlUl(,)'.
Rz TV: ltan with 1.211 mg ,low IV over 5 mJIUI, may iDcrease up t.o5 IIIg q 6 hrll P RN
~
esmolol <Breviblod'il)
\
/
DI!OO
INFO
\
I
C<'IrdioHlective short-Kting bela blOC"ker'·, Being investigated for hyperteM i~e
""ff1rtn~ia. Metaboliloo by RBCette".... Elimination half·life: 9 miN. Therapeut.ic . .
• ponl!' (.> 20.. d«r@al!'in heart rail', HR < 100, or eonverslOO t.o ainus rhythm) in 72'ot.
5If* uncn: dote relalA!<! hypOte". ion (in 20~), gener ally re$Olvel within 30 min5 IIf
•
1.2. Critielll care
GENERAL CARE
DIC Bronchospllsm 1.,. likely th"n othllr beta bloc:klll"ll . Avoid in CHF.
Rx 500 llgi'kg loading dOH over I min. folio,", .... itb. mill infUllion atamng .... ilh 60
~glttnn. Repeal loading dPS'! and increment infullion rllte by 60 ).Ig/kglmin 115 mins.
Rarely", 100 1Ig/k&lmin requJr.. d. l)o;g~s ",:200 IIsfkg1min add li llll•.
fenoldopam (Corlopam®)
\ I
\
VII"oollftlOr, Onse: "rllction < 5 minutes. duroLion 30 mil\$.
Rx tv infullion (no bolus dOMJ1: IIUln .... ith 0.1·0.8 mcglkpmin. tilAla by 0.1
mcglkefm.in q 15 min up to II maximum of 1.6 mrg/'k&lmin .
.---I
prop ranolol (Inderal®)
\
I
00I.0C31N1'O
\
\
Main use tv is tQ Q)un terflcl LIIchycardia with yasodilatoTII (Ullually d~en'l lower BP
a<:UOlly when used alous) .
Rx tv: load with 1-10 mg slow !VP, rollow with 3 n'glhr. PO: 80·640 rng q d in divideddOS6.
ORAL AGENTS
F"r 1e!14 urgent control of HTN (excepUon: sublingual
.---I
donidine (CetapreS®)
\
nifP.dipine(rl~
I
belown.
OROClINFO
\
\
Ad.son oardlov!Oo;cular control reoo:~pt(lrJ ill m«IuUaoblongllla. inhibit,a symplitheUf
l>U.tnow. t...o;s confusion lhllll A1domal. but still aedaUna. Tath}'tardia rara. Onse~ < 30
mm .
1iI"'~ E...,.,."., fluid ret<lnllon (",hiob may .... d""" eWecliv...,..., oount<lr wilh diuntic),
dry mouth. &edItion (minimi z., by slo .... dou incr"men~J. CQn.tipation, decreased CO &
iI.R (by illcreaHd vllgalloOll ..), rebound "TN ifwit.hdrawn rap,dly (caution m un reliable
pat.K!nts; treatment for ",boWld HTN ; donidine and lobl!talol, 11ft! paIJ~ 4). Rebound i.
less lik~Jy and leSll lcvere with cloQldine patches (Catapret iTS®). applied onee per
w!'(!k.
Rx Rapid control: 0.2 mg PO. tben 0,1 mg PO III hr. 8top atO.S mg total or ifaltbo·
IIWtiC. Mainwnllnce d<.>ae,O ,1 mg PO BrD or TID, in.,.eaH~lowly to m~. 2.4 mgldl\)'
(usual 0.2-O.K mglday) ,
.---I
propranolol (lnderal®)
\
I
DAUOfII'O
\
Beta hlocker. Use in HTN: blunts reDell tachycardia from ~alodi liltora.
SmE Im'WtWI CHF, symploOlIlati~ bradycardia. bronehoep,um (avoid in ll.5t.hmatics),
rapid withdraw! - rell"" tachyc .. rdia - ua~rbat ... myocardl .. J i""hl)l1lill io CAD.
Jb: 40 mg PO BIC (usually .... ith diuretic), titrote up to 6~ 0 mglday in 2-3 divided
donn. Or, !nd~r .. I.LA, 80 mg POq d. lJtn"Puw; 10, 2040, 60 &80 rug 1II'OTt'!<i t,a1>o. lnden.al LA (lao, acting) 60, 80, 120 & 160 mg clpsul0!8 ,
.---InifediPine(Procardia®.Adlllat®} \
/
ORWINFO
\
\
Short-acling calcium channr! blocker (CCB). Deereaaes il)'lItemic va6CUlar reiislanae.ln.,.ease, cardiac indu, CBF lby 10-20'1'), GFR, and Na eXCl'lltio". ReoIponselome.
What variable, Onlll!t: .-16 mini . Duratlo,,: 3·5 hn.
SmIlEfFf:C1"& lIushiog HiA. palpitation, edema; reflex tlIdl,ycardia. t&ution with belli
blocker u negative ino tropy IIllly be additiv • . May taUH 1IIIV0!ft hypotensiun i1l vol ume
deplet.ed patiellta (thu, uM with clution with mannitol or futoo;emide). May increase serum phenytQln (Oila"tin®) levels. Ule oraho n-acti"g
mil,)' be asaocial.ed with car·
diac risk, thusloni·llcti0i agents sbould be uS@odunleuspecific bo!nefit outw~iib. the
risk.
&- 10-20 mg po. raster onset with sublingua l or buccal admlnistratiou i punclUrt!
~aJ»lule). or ifchewed (pali"llt ~pe!. caJ»lule ~fter che .... ing). Note: the bo!neficial err""ts
orlbedrug results rrom swallowing the capaule contents, the medicltion is Il9l ab!iOrbed
through the m""""" . ifno reSpOnSB after 20,30 mm. give additionBI 10 mg.
cca.
GENERAL CARE
1.2. Critical Cln!
,
labetalol
(Normodyne®, TTandate®)
\ /
\
See page 4 . Chrome administration rna)' have higher incldonce of orthO!ltatic h)'·
po\@n.ion, fe~er , leltUa] d)'llmnttlon., lind hepatk toKicity than othl!r beta blocKer.! .
.--/
metoprolol (Lopressor®)
\~--:,/~_='~_._ro
__\-,-~
Beta b~ker that is nlll.uvel), cllrdioseledive (It doses < 200 m!l:.
Rx 50·200 mg il\ I 01" 2 doo;ell .
.--/
enol:lpril (\'asoteC®)
Angiot.l!~in
\
I
DRU<i.tII'O
\
I
convertingenzymll lACE ) inhibi tor. 00 OQt Ul!8during pl1!gn8n~. Mol'
be le.s effective in !>IIICK pat;etll$. See,"r.loprilr.1 a bove ror IV use.
Rx Initial dose 2 .5·5 mg in onl! doee: maintenance 5 ·40 mil in lor 2 desr.s.
1.2.2.
Hypotension (shock)
Classification:
L hypOVolemic: fir~1 .ign usually tachycardio. :> 2IJ..40% 0(111000 vol luna 10&11 mUllt
OCCUr berore perfUlio n orvital orgon5 is impairl!d . Includu:
A. hemorrhage (exte rnol or internal )
B. bowel Dbstructic.n (w; th third .pacing)
2. septic: lAostonen due to gram negative sepsia
;I. COrdJogeOlC! ,ncJlldes ,'1l, Clrd'omyopllthy, dytirhythm las ('ndndlr'lg .... fib)
4. neurtlgunic: e.g. pual:; s" due to spinal cord inju.ry. Blood pools in venolla capacItance vessels
5. miscellaneoll.
A. anaphylBll.ia
B. Insulin reaction
C ARD IOV ASC ULAR AGENTS FOR SHOCK
Pla.rna expanders. Indudo;s:
l . ",rysl.alloids: normal saline hos less tendency to promote cerebral edama than others (&ee tv fluids , page 657 unducontrol of elevated !CP)
2. a:>l1njds; e.g. het.astarch lHespan~) . • CA1J'l'ION: repeated administl"lltlon(lYt!Ta
pariQd orda)'. mtlY prolong PTIP'rT and dotting UrofS and may ine:.reoee \.be ri~k
of rebleeding in oneurysmal SAH" ($« pG//! 7871
3. blood pradu~t.I; upensive . Risk nrtra.ns m;ssible (liseBllU \lr tnIlLBFu~iw:> reaction
PReSSORS
phenylep hrin e
(Neo--Syneph ri ne@)
\ !
\
Pure alpha sym pathomimetic. Useful il"l hypotension ilSl.o ci8ted with tachycardia
(a triol tachyarrhythmiaa). EIe"Oh!8 BP b)' we .... uing SVR via VASOCOnStriction, cause,
rt'1I"" in<Teueln parllll}'Tllpathetic. tone i with resu ltant . lowing of pulse). Lack or 0 action
means non-inotropk. no earoiae o«('leration, and no n-lslUItion ofb nmehial l mooU, mUll'
de. Cardiac output and TIlna.l blood II"", may d""r" .8<I. A,·oid in spir,al cord illj urit'~ (""e
page 703J.
Rx pn!Sllor range: l()()..I~O I'Wmin; maintenance: 4()"60 I'Wlllin. To pT1lpare: pu~ 4()
mg r4a mps) in 500 ml D5W 1.0 )'ield SO I'g/ml; e rate ors mVhr _ to JIg/min.
,
1.2_ Critical car"
GENERAl; CARE
~
\ !
dopamine
S ..... Tobie /.2 for II &urnm~·
/)' of the effects ofdopllmine
(OA) at "8"0\1.9 dll6ag<!6. DA il
primarily a vB.HlCQnatriclor(6,
elfi'C1Ii uaually overridd~n by,,·
activity), 25%of dopamine giveo
;8 rllpidly converted to I1OrepinepbriDe (NE L Atdo&el > 10
I'g/kg/min one is e/;Ientilll!y giving NE. May .aulle signi li cant
hypergJytf!ml. at high d<>!le8.
\
nble 1·2 Popamlne dotage
Ooy
......'..
Result
Ellecl
!~glmln)
0.5-2.0 (S<ITlII'
1ime$1.IP kl5)
(anal, mL'Se1lIeril:. COlO-
ne~' &j~'
2·10
,,,
<'I,
0 8. 00p8ll1irler!lic:
Rx Start wi th 2·5
llllioo\ (0)
positNe frto1ropll
raeasas nor-epi (vascr
..-.,
I'glkglmin Dnd titrate.
~
dobutamine (DobutreX®)
\
I
IlFIUGItlFO
\
I
Va~odilal.eJ
by 0, (primary) lind by increa~ CO from [+ )\notropy C~); result: little
or no fall in ap.l~ tad\ycardln than DA. No alphe relea~ nor vS9DConiitricuon , May be
uged synergistlca.lIy with nitropl"IIssidl\. Tachyphylaxis after _ 12 It.... PuI'1\! increllJl<'ll >
H)% mllY ... acerbate myocardial ischemia. more cornmon at dC~1 > 20 "glkg/min. Optima! ~ requires hemodynantic monitoring, PIlssibl" pLal.elet f'~nctiOfl inhibition.
Rx usua l range 2.5 - 10 I'gr\g/min ; rilrelydOfie5 up to 40 ",sed (t.o prepere: put SO mg
in 250 IIlL DtiW to yield.200 I'g/ml).
/
amrinone (Inocor®)
,-----/Nonadrene.rgic cmiotoni.:.
\
/
DfIUO",O
\
':c"L,------=-----:-:----'~,
Pho~phQdie8t1!ra!1e inhibitor. eITecl.ll l ilDilftr to dobIIt amine (i ncluding exacerbation or mYDC8n!ial ischemia). 2'10. incldeuce ofthrombo<;ylopenia.
Rx 0.7ti mglkg initially over 2-3 min. then drip 6-10 I'gIlt:Imin.
/
/
DIUlINFO
\
~-'-----:--------:-,-'>--"
Primarily vnSocoDl trietor (7 co.unl.erp.oouctiv,., on oerebral vasospasm, 7 deere9I H
CBl't B_agon i5t at I(>W dO'le!l . lncruJlea puJmonlu)I voscula. ,..,.i~ laMe.
,-----/
nore pin e ph rine
\
epinephri ne
\
~
I
~IIfFO
\
,
& 0.5-1.0 rug of I: 10,000 ~lutfon [VP: may repeat q 5 minu tes(may boJua p.!' ET
lube). Drip: llartat 1.0 J.lglmin, titl'\lle up to 8 J.lglmin (1.0 prep:ire: put I 109 in tOO 101 NS
or05W).
~
isoproter enol (Is up rel®}
\
/
0RUa 1M'{)
\
I
Positive chronotropic and inotropic, - iucreased caminc 0 1 consumption. arrhythrni ... vasodilatatioo (b)' BI action) ~ kelet81 muscle " eerebra! ~essel&.
~
p,,~
levophed
\~.L/_-:-;-~_~_~
__\-'---,
DirectB l timulatlon (jIQ.'!it;ive iuolNpic.and ohrDnot",pi~ )
Rx If tart drip at IH2 J.lglmio ; maintenance 2· 4 I'gfmin (0.1>-1.0 mVminl (to prepare:
2 lOgin SOD rnl NS ~r D5W to yield 4 Ilgfcc).
1.2.3.
Neurogenic pulmonary edema
A rRra ""mi ition
GENERAL CARE
a~"""i"t.!<I
with A v .. ,-; .. ty Ori nl .... cnoni"l
1.2. Critical
cs.re
,,'Hh nl~ ....
induoiing:-
,
• ... barachnoid hemorrhage , lIene ... lhed
" i1~',
.nd head injury_
Pat hophyfliology
Two pon ibly Iynergi, tic mKhan;, m•. Sudden inc~ ... ed lep or hypothalamic ''\i\lmil,. produce II ••1vo of,ympathetic di.charge cauling l'fl!iuribut1Oll of blood to lh.
pulmonary circulMion, resulting in ,l,v,tlnn ofpulmon.ry e/IIplltary wedge PI"I!Qur"e'
(PC WP ) .lId in<: rellsed permubility. 5«ondly. th, ...oc:iated . urge ol c.tec:hoIamina
directly di,rupu the capillary endothelium which incl"I!'_ alveolar permeability.
f}'
Treatment
Supportive, using m eUUTeI .uc h al positive pl"l".ure ~ntil.tiO!l with 19~ I_l,of
PEEl> (su pagt. 659) and trelltment to norma liu lep. A PA·eatnete. il u."ally helpful.
'I'h",re may be lOme effIcacy in using II dobu .... mine infusion" . upplemented with fu·
rosemide as neflled . The theoretical adv1nt.aaeof'dobutemine OVer ~iolUly attempted
alpha. and beta-block.... i. that dOOulamine does 1l2t reduce DerebrailH'rfusion. Niuopros.o;ide may help dilate lhe pulmonary vasculature.
1.3.
Endocrinology
1.3.1.
Steroids
1.3.1 .1.
Replacement therapy
Under normal ,
basal eouditions. the
adrenal cortex .e·
crete. 1.s.25 mgldayof
bydJ'oeortiao ne
(AKA cortilO1), and
1..s.40lgid ayorco rli.
costeron e. COr1.iJol
hili a halr·life of _ 90
minute..
[0 priDlary
adrenoc:ortieal ;nlulTt.
ciency (Add;lOn', di,.
use), both
glucocorticoid. and
miDeralocorticoid.
mud be replaced. In
secondary adrenal in.
sufficiency eaused by
deficient corticotropin (ACTlil release
by lhe pituitary. min·
eralocorti«lid . ecretion i. usually normal
and only glucocorti.
coids need to be reo
placed.
T(lbie ' ·3 sho .....
equivalent daily corti,
CO$teroid d<o.el for re'
placemenllherapy.
Tabl.'·3 equivalenl eor1leoSl~oId dotes"
_.
_g;.., .-.1IIiW_.~ 1_ ... ....., prImatiIy u\JIUCOCDI'
..........lltItgho<J>C'A1imicl po", IV _ I , gMln; 1M .......,dlll...
~ lor _110_' - . . IV IOCUI C.wIO! t..
'1PdY otoIainod
SIenoI:w«l tJrri.PaII8<li1<l<WoO 21 ....,. '" 5 mgo 1 " _ and , - ' <I00I.
~. 1ronI3O 10 5 mgs ...... 611oys; "OS' ~ 10 mg Iab& .,.,
Itorr> 60 mg 10 10mg ...... '<\aYS; "DS 12.000y" COO'Uins~8 10 mg ,.", and
' - I fromSQ rng 1021:1 mg_ 12diol"l
-.,. ~c:oonIIoins 21""" "'. "'lIS .... ttr<1I"_~....,
~ doage from 2. 10 • mgs"""" 6 <»ys
_
"" """. , ..... ,., ... _
,ape"
f
Physiolo,;c replacement (in the absence of stress) can be accomplished with either:
I. hydrooorti.one: 20 rng POq AM and 10 rng PO q PM
2. or p1"flinilOne: 5 mg PO q oUl and 2.5 mg PO q PM
Cortitol and corti_ ~ uH r,,1 for chronic: primary adrenocorttcal ill5uffidency or
•
1.3. Endocrinol"lO'
GENERAL CARE
1M AddisonJan cruJs. Bee... """ or mineralocorticoid IIctivi~y, ""6 for chronk th .... apy or
other conditionl (e.g. hypopituitnrismJ may ruult in saJ~ and nuld reW!otion , hypertens ioll and hypokalf.mia.
HYPOTHALAMIC-PITUiTARY-ADRENAL AXIS SUPPRESSION
Ch.ranic 6wro[d adr.linJstratJon suppresses thll! tlypoLhalomie-pituil.:!",,·Rdre"1I1
l HPA) axis, and eventu~lIy CHUseS adr~nlll atl"Qphy.lf5teraid~ are ~bruptly ,t(Jpped or
if aculli iIIne" develops. &ymptl)ms ofadrenoc:ortkal inBulf.c:iency (Al) may ensue (_
Tobit I ..#), which ifsevere may proVi!8I t(J Addisonian cri~i! (_ post II ). RecCWBry of
.adrenal oortelt IOg$ beh':1d the pituit.:J.ry. so baul ACTH levels increase before cortilol
1""1'18 do .
HI-'A 8UpPNWiJOn depElnds on the specific
glueocortiooid used, Lhe routo! , fnquency, tllne,
Tobie 1-4 Symptom, of adrenal
and duration IIf treat ment. SUppre""ion i$ IInlih·
I".ufflclency
ly with < 40 Ing predni60nf (or ~quivalent) giveo
fallgue
in the mllming for leJl$ than. 1 daY~.lIrwith "".
~)'POglyeefl"lI
ery-othu-day therapy of <. 40 mg for . 5 Wltek.o".
~.­
aJlhrillgla
Some Idren.l s tropI\)' lIUlyOtcUr after 3-.4 day. of
AddisfIIlian CliSIII (~
aoor~xia
high dOt>esteroidili, und wme IIxis suppreesioll will
severei ..ll/T !lsk 01
aimon certainly neeur aner 2 weeks of <10-60 mil"
dealh. sae page 11)
hydrocortisone (or equi"",lent ) daily. Mer a
month Or more ofltEroids, th~ HPA lIXil may be
dep~ for ~.long Bli one YEll r.
Mft3iuring morning plnma hydrocortisone CIIn evaluate the degree of J"1!<"<Jvery of
basal adrenoeorti~al funetion, butdoos ~ useSi' IIdeq uacy ttress r lli5pon6e.
-.......
STEROID WITHDRAWAL"
In ao;lditi!J1l to the above daJJgenof"llypooortisolism in the preYence IIf HPA dUpp>,",!8s ion. too rllllid II taper m.yalUS8 aDore-up of the underiyi nf C(l ndilioll for whleh ! teroldA
weTi' presmbed.
wnell the risk of H?A suppression illow (as is the ease w.th ahort (OUnles of.le·
raids for lelia than - 5·1 :laya" ~ne .... lly Pl'KCribed fot most neurosurgical imiiaotionai
ebruptdiscont'n ualion uauallyconie, alow risk of AI. For up t~ 2 weeksofus<>,s teroids
ore Wlually 6afely witlldrawn by tapering over 1·2 weeks. For longer treatment. or when
withdnwlI! problem. develoll. lise the following woaervatjvr..tanu:
1, makeamall d~ .... menta (equiva lent to 2.5-5 mg prednis~ne) every 3-1 d. Patient
may experience mild wlthdrowBI symplOJT1S 01" ;
A. fatigue
B. anoreKia
C. n8U~U
O. orthostatic diuine&&
2. "backtrack" (i.e. increase the dose and ",Kurue]l. moregrsdUlli taparl ir allY ofthe
(oUawing pa:ur;
A. l!)(acerbAtion of thl! Wlderlyinll: condition for which steroid.s were used
B. evidu.ce of swroid withdrawal symptoltl$ (P<t TabI~ 1·4)
C. intercurrent infection or nei!<! for ~lIrll"e.r:y 'Be-!; Slreu ~I below)
3. OnOO -ph)'@JQlogic~ dOllu ofgJucorortJcotd ba"e b<!en reached labuut20 mg hydrocorti60owday or equivll lent (see Tab/I. 103)1:A. the patient i.$ 5wil.l:hed Ii) 20 mg hydrocortiKOne PO q AM (do !lOt UGe long
acUng preparations)
B. af\er _ 2-~ """eb, II morning corti&ollevei Is d>echd (prior to th ~ AM hy·
dromrtj,uoedose), a.nd the hydrorortisone is tapered by2,5 mg W"'lkJy un!.ii
10 mgtd is n!ached (Ia wer lirnit.s of physiologic)
C. then, every 2-4 WHM, theAM cord. ol level i. dre .. n (prior to AM dose) until the 8 AIlI cortisol is > 10 1'81100 ml, indica t ing retum ofbll5elineadrenal
I'uncLion
O. when this return of baseline adreu.1 function DOCU" :
1. daily steroid..!l a~ stopped, but strMS dosu must stili be given whn
needed (u. below)
2, monthly cosyntro]lin Klimulatioo leaL!! (_ pogt 444) Nre JH'rfnrmoo
....ntll oonnll1. The need for stress doaes ofsteroid~ ceases when a PQ5'
itive lut is obt ained. The riak for adrenal illl!Ufficie.ncy perl;latii-..2..
)'jlJI.[5, sf\erce$atlon of chronic neroids (upecially thlO first year)
GENERAL CARE
1.3. Endocrinology
,
STFIESS DOSES
Duri.rl, ph)'lliologic ".l.rHl" ill , nonnal .dr, nal
",nd proc!uott. .. 250-300 ml bydroooortilOnoid l Y.
With cilronie,llucorortiroid therapy leither It pr~lnt,
or in lut ].2 yB), fLlppr ulion oftha tIOrmal ".t,ess·r&,pon..- ntoeHeitat. lIupplenHlnt.1 d OIft.
In
Table 1·5 s.erokl alt, u dol·
u 10' "IItcUve . urgery
pIIt~" ....!tll
.. l uppreued IIPA axi.:
for mild mn.-.l • •, . un, co mmon cold), linal.
dental eJrtracuon: double t he dally do .e (if off
I l.;lroidl, stvII 40 IlII1 hydroo:o/'1ilOn e OlD)
fa, modera\e . tl1!ll' (e.,. nU l, minor I W"jIwry lUId e . iIlalllneathe.11I (endO&tOpy, multiple den.
tal utraction. ...): giVII 50 InlI hydrocortison •
• '0
for m-,j or Illne.1 lpnllumon;a, l )'tle." ic ln fectione, high fever), I16Yi!~ trauma. or llmergenC)'
I Ulpry under il8oe rlllllOe.lith l'llll : giVI tOO mg
hydnl<;ortil"n.. IV q 6.8 h... far 3.t day .. until
the &t re.. l, resolved
for .. lec tiYi> urger)" _ rable J·5 for gWdellne-
POSSl8LE DELETERIOUS SlOE efFECTS OF STEROIOS
Although t.helle aide d l'e cla anI moll! common with prolOll,ed admini$trltion'", lome
elln Dec u. liven with . hort. u e a tment cou ....... Po.sibl" Pie "lferts indude''''':
aordiovllKU la. and renal
• hype...u.nlion
• . odium and water retention
•
hypokalemic alkalosis
e NS
• progreuive OluJliroalleukoenupl-oalopalhy (pML) (IN P<lGf231)
• mental sgitat.ioo 0. -Iterold pilycbOlli.·
• I pinal oo,d compreuiO<l from spllUll epidu,allipomalolli.: rare (_ pclIt 903)
• pseudOlumor <8rebri (.ee. ldiopalh ~ .n'",r ,..,,,iol AJ'fHr~fUit)n, P"le 493)
endocrine
• Cll UliOll! bI,a,,,w ot growth lUwresunl effect in children, daily r'ueoron.icold
da.ing O~ r proLonged p!!riod.!I should be ,"""Ned ror tbe mJlI l "'lI:ent indiauonl
• ~ndary araenOlThea
• su ppreaaion ofhypothlJ llrnic-pituitaJy.. dre.IllJ am: mUCH r ndoPnow lteroid
ptodu.ctioo - risk of adrenal in3ufficiency wit b steroid withdraw&! (sH .. 60<.01)
Cuabillgoid fel hue!! with prolonged USllse (i'\.rogenic Cushins'II!Ild/"OllH!): obe,i ty, bypel1.elllion, hinutilm . ..
Gi: .uk inereued only with . terold th~ rapy > 3 weeD dUnlti(lll aru:l ~ of
pncdniflOne > 400-1000 mdd 0. deumethuOfIa > 40 mgld"
• gUl nt', .Qd .teroid "~I1I; incidence I_red wi\h the twleof flntacict. andto. Ii,
antaroni,ta (e.i . Dmelidine, ..ru\.idine_.. )
•
•
•
•
PIInc.'f'U!ilil
in tel\.i n"J or . i""oid diverticul ... perforatiOll": incidenOo! _ 0.1910. Sine;! steroids
may mull. alp orpentonitill, t.hillhou]d be(oll$idereo;l Ln ""tlenlll on steroid.
witb Ibdomi nal dWcomfort. especially in th •• ldetly aod thoe. wilb a bisr.:Irr of
ru-1Je. Abdominal ..·ray ""'Illy ihOW5 ftft intr!lperitoneal air
mh..ibi lion orflb.-oOlouu
• imPflirod woWld beeling Of \IIIOWId b...,.kdown
• lubcutaneout I!q utt atrophy
roet.abol.ie
• ~intoler __ (~be~ ) Ind & turbance or ni~1I metaboli, m
•
molar nonket¢ic !;Oma
• ~.l.Ipidlmi"
divertlcvJ..
ophthalmologic
•
poIIl.lrior l "bcllPlwa r aou.-.cu
• I J·ucoroll
musculotkeletaJ
• aVNCUlar necl"OlMl (A' 'N) arthe hip or other hone.: ...oolly with p.ol<mge<l admilus ,",!ion - o:\IlhiTl(oid habillR and incl"1lBled marnlw fat"';thin thl bone"'
"
GENBRAL CARE
•
•
OfittlopoTOli,; 111a.!' preodillpOSfl to veruhral coropreBllion fractures wtllch occur in
30-51)!jl, ofpatientll em prolo"8ed gluCOCl.>l'ticoid..(8ff pag~ U81, Steroid induced
boae 1068 may be reveTUd with cydical administration of etldrona!.e>' in <I cyclu
0(400 roWd .. 14 oiaY" followed by 76day8ofo. a] calciumaupplementaoffiOO mgld
(not proven to reduced rate of VB fruCl-uns, KI/ fI<l&e 7411)
• muscle wulmeN (I~roid myopathy): often wonlt! in prmcimal muscles
infectious
• mununosuppreasicm: with possible supllrinfect.ion, eapedally fungal, parasitic
• pOIIBible reactivation o(TB, chkkenpox
hematologic
• hypercoagulopalhy from inhii'>ition oHLsaue pJuo::tinogen activator
• stcroid~ UU5e demarginat lon of white blood cellJl, which mllY artifactually elevate
t.he wac count even in th e aboleou of infection
mi.y""llaneoua
hlc~uJlll: may r9/1pond to chlorpromatine {ThoNlzimm) 26-50 mil' PO 11D.QlD II 2·
3 daY" (if l ymptoms persill!, giv.. 25·50 rog 1M)
~tc roid. readily 0'0&& the pI8""01.ll. anel {~tailldrenal h.)'poplasia InQy occur wilh
the " dministration oflQrge dOll811 during p~gnaDl:y
•
•
1.3.1 .2.
Addisonian crisis
An ad ..... n,,1 inlufficlellCY emergency ,
Symptom.: ment.'lllllatUfl change! (confusion, lel.hargy, or agit.fltion), muscle
WGUnI!tS.
S igD ~:
poetural bypotenaion or shock, hyponat~a. hyperkalemia . hypogiyCflmia.
lu1>erthenni" (811 hIgh n lOS' Fl.
TREATMENT OF ADOISONIAN CRISIS
Ifpoasible. draw ",,",m for cort;'o! det<lrmill£ltlon (dow ",,&.it for the$e resulu to
iI1l5titute thertlpy ). Give fluid. auffici""t for dehydration and shock.
FOT ~B lu cocurticoid e m ergency"
hydroeortilOna 5~um 8u~in"t.a (Solu·Cortel®) 100 mg IV STAT and then .50 mil
rvq61\r.
AND co'till.me ac<!taI<l75·100 mg 1M STAl'. aM then ,5().705 n'g 1M q 6ltn!
}-' o r "'miner alocorticoid e merge ll oy"
U&u.Uy not naCBfUliI.<Y it aecondlltY adtenul io."fficiency (e.g. panhypopituitarism )
dll8oltycorticOfii.erone lleetaU!- (D(JC.!l.®): 5 rug 1M BID
OR nudroevrti60ne !Florinel@):0.06-0.2mgPOqd
NOT re~ mm end ed fo r e m ergenc y trea tm e nt
• methylprednisolDne
1.4.
Fluids and Electrolytes
SERUM OSMOLAUTY
Clin ical 8lgnjfi~ ofvariau. aerum osmolarity .,a)ue$ i, shown in To~ }·6.
Appro:<inu.l.evaluernay oocalculated usiog
,,,illS Eq I· J.
Tllble 1-8 Clln1cal cllrrelallil IIf11 ..
rllm o, motallty
,,
GENERAL CVlE
1.4. Auid, and Electrolytes
u
05mol.licy (m05nVLJ "'- 2, (rNa'J' [I<' J) .. [B1USNI .. lllh;c:se J
1.4.1.
Electrolyte abnormalities
1.4 .1.1.
Sodium
Eq1 ·1
Anti d iure ti c h orm o ne
The major SOW"Cfl ofthe cnnopeptide arginine "'as<lpnl'sain. AKA antidiuretic ho ...
mon~ (ADI1) is tbe rn&gnO<'elh. lar portion of the s~pr&optic nucleus ofthe hypotho.lamu5.
II is "fIn ... eyed alons: Ul!WI. in the supraoptie·hypophyaal tract to the po8to!riorpiluilliry
gland (ne urobypopb)'llia) where it is releuo.d inID!.he s)'IItem.ic cirt:ulation. All actions or
ADH rUlilt from binding mUle hormone to lIPfl"ifIC membrone bound rffepton on the
aurface of target geUs". One of the major eff...,u; of ADH i. to incre~ the p~rme$bility
of the distal renal l ubulea resulting in incn!Ased reall!orption of water, dilliling 'he dr·
cllitting blood and producing" alncentralA!d urine, The mOllI pOwerf.•d physiologic stirn·
111115 fot ADH release il an in<rease in serum osmolality, e less pOl<lct stimulus is a
reduel.;oa ofintravll5<:ular"'olume. AD~I if al.o released io glueoo>nicoid deficiency, and
i, inhibited by f!J<ogenousllluoororti"flidlllnd adrenerJic drug., ADH is 9190e potl>nt ... u ••
oeonslrietor.
H VPONATf'lEMIA
.,
bit/om)'
Usually
iI
po&toperati... e hyponatremia: a rare condition usually ducribed in YOWlg. otllerwise IIB11II.hy womlln undergoing ele.;ti ... e $\lrgery;'
Oue to 510w compa[).llatory me..:hanisml in the bmin, II gradual de<;linll in 8\!1'W:II ~o-­
diwn i. better tolernte-d thMII ropid drop. SympIDms or wild orgrodual hyponatremia
include More>d$, headache . irritability, snd muac!e we~knl'1lll. SeV<!re hypOnat~mia
« 120 mmol/L)or a rllpid drop (> 0.5 mmoVlIJ') un cause neuromu8cular ucitability, cerebral edrffill, muscle 'wil.ching and erampll. nau!ieR/vomiting, ",nru~ion, !leizu .... s. rtipl'
ralory arrest and poI;sibly permanent neurologic iQjury. (Offill!jr deaLb .
Cen tral po nti ne myeli nolys is
Wbcrtu eMCfl ...;vely .to.... correction of hyponllt ...."". fa .... <K;.~d ",jth Inaecoacd
morbidity and mortality• . Inordinately rapid t",Dlment bft~ been associated wjth cenU1l1
pontine myelino!y$i.tI (CPM ), AKA osmotic demyelination syndrome, II taredi!lorder of
pon t ine white mattl>r- as wen 11$ olher area~ of~rebral white metier , fint deatribed in
al"flholiC!)"', producing iMidioo.lS Oeccid qUlOdriplegia, mentalsiatuedlangu, and cl"lInie]
n~e ebDorm.litl~ with a ~udobuJbllT palsy appelltMOl'.ln one re.... iew ... , no patient
developed CPM whl\O treated 310wly S/I outlined below. And yet, the rat@ofeorTe..:tionco ...
.... Iau.!! poorly with CPM; It may bI! that , .... ~is t llecriti"",j '·lIriabl e>-. F .... tu,..,.
comUlOn to patients who develop CPM a"""
deloy in the diagnoeisofhyponatremla with .... sultant respiratory BrTi'8t or MlI~ure with probsble hypoxemic "enl
rapid ron-eetiOlI to normo· or hYP"I'-nlltremia (> l S5 mEqIt. ) .. llhln 48 houtll of
initiation ofthenpy
increase oflJ(lt\lm fOdlum by , 25 IUEqIL within 48 hours or;nitiation of therapy
O'Ier-ronecting5l1rum ~UID in patil!l1ta with hepatic encephalopathy
.NS, many patienta de,".,IDping CPM wen! victims of chn"'icdebilitat.lng disellse.
"
VI.. Fluid$ and Ele-etrolyt ...
GENRRAL CARE
malnourishment, or alcoholism and neve r had hyponatr-tmi • • Ma ny had an episode of hypox,ialanoxia'"
p1"QO!IlCII ofhyponatremi. > 2~ hlll prior to treatment"
TR£ATMENTOF HYPON",TREMIA
PUientl with hypon. tremi. of unknown durMKln probably h.ve chronic hyponatre.
mia ifminimally . ympto .... tie. and ehould be trealed _lowly, preferably with flu id re·
striction. Thoee .. lUI acute Iymptomatic hypon.tremia (convull ionl, Itupor or coma)
. hould be treated promptly _inee the! pr_n«o of eNS . ymptoros h.. been _hown to be
auocilted with brain edema lrad)ographica Uy and I t necrop.y) and m.y henold impendh" hern.illiOtl and cardio...... prralOry
Symptomatic r.:lientl with hyponatremia ofunknown duration InI t heOtle, a t ril k
of neurologic HqUl .e.lnd one . boukl,lartoft" .. ith. I"col"l"fttion, followed by. more
cradulltrutment u outlined below". TIM followina method for con-ec:ting hyponatremia UNa') < 12S mEqfL) iSll&Ocilled with low riB of deveKlping CPM (although it may
not be poMible to define. note of co~tion th.t I, conai. tently free of m k):
1. • CAUTION: avoid oormo- 01" hyper.n.tremia during con-e<:t ion, check frequent
....... m INa" levela and lrIOdul.te therapy ,.. fDllowa::
, top if ..fUn! IN.') " 126 mEqlL over 1 po:riod of. 17 :t I hoU ri
stop if the dla.D.p In .......m IN, ' IIe :ll 10 mEqIl. in U hoU ri"'
do not e~ a ute of correctioo of. UI :r 0.2 mEqIlJh.
2. , lowlyadmini,te. S'Io(S lS mEq/L)o. S"(856 m£4'L) NaCI toadhere totheabove
criteria (Uart with 2S-50 eclhr of the S'" solution and foll ow INa'] closely)
3. aim ultaneou.Jy administer furoaemMle (~l"' to p......... nt volume overload
with . ubeequent incn_ in atrial n.triuretic factor and f'IIullJLn t urinal)' dumping Drthe uu. Na' being adm ini.tend
4 . m.....,.. l(' IOIIt in urine .nd repl.ce -rungly
."'"t.
SYNDR OME OF INAPPROPRIATE ANllD1URET1C HORMONE SECRETION
1 Key futu ......
0 rele... of ADH u. the abo5ence 0t,h:faiologic (osmotic) stimul i
o f'lluitl in hyponltrem.i. with hi Ilrine OIIlDOlality
o \laually 1l(e01D~.IIied by hypervo emiD (OttUionaliy with I!\IlIo!emia)
o may be KI n with cert.ein malignanciea.nd many intratrani.l.bnonnalitte.
o critical to di&t ingulgh from cerebral Alt wasting which produces ~Iemi.
1
SlADH , AKA Sch "" arh·Bartter ayndrome, w... lintdestribed with broo.c~nic
It il Ule releue ofantidiuretic hDrmone (ADm in the al»eDceofpbyaiologic (_
motic) l timuli. nul produc"" elevated urine OIImolality. and upansion oftheeKtraoellu_
liTfl uid vDlume leading to. dilutionsl hypon,uemia, which c.n produce fluid overl.,.d
(hypervolemia) butSlAD H may also occur with ",",volemia. For ....1M>n1 thoot ..... undeaT.
edema doe. nOt ooc:ur.
can~r.
E ti o logies o f SlAD H
The hyponatremia ofSlADH must be differentiated from that due to «Tebral A lt
wast ing (CSW) (u, ~Iow). SLADH may be KIn in the fDllowin6 ... ttin", (KI refe",noel'
for more utensive list):
L malignant tumD": especially bronchogenic
2. numerous intnerani. 1 prooeISN including:
A. men.ingiti.: ... pecially in pediatric patientl•• tao .. ith TB mf'~ti.
B. tr.uma: seen in 4.6'1r of head trauma patientl
C. increaaed lep
D. tumDn
E. post cnoniotomy
F. SAM (NB: ..... Ie-out CSW, whidl ~ui r.. dilfenl!nt tre.tment. _lH!low)
3. numerous pulmonary dillarden
A. malignancy
B. pulmonary TB
4.
5.
6.
7.
C. aspergillOiIl
m.y lO.IIleti mH occur . ecooda.ry to enemia
with !tren, ..vere pain. nau ... Dr hypotension (all can st imulate ADH rele...)
ooc:uion' Uy _ ... with acute i nterrnjt ~nt porphyrilo (AlP )
d..... gl:
A. ehlorpropramide(Oi.binese¢l): mayeauSflI "n1.lIve" SLADIi byincr...ing
GENERAL CARE
1.4. Fluid. and Elactrolyt.ea
"
the renal ... n,it;";ty to endogenOUi ADH
8 . OJIytoci ..... hal""'6 ·croo activity" with Al) ~I , and UlII.)' al., bI contarninllt.
eel with ADH
C. thiuide diurr.tiet: h.Ydt«hlorothluide . 00 po~ 18)
D. arbamaupine ' 1'egretola)
DIAGNOSIS OF SIADH
In
gl!lItnt,
3 diagnostic ail.erilllrl: hyponot.reuua, in'PfH'Op';lllfly conCMt r/l1ed
uri"", and DO ."idenc- of ren, 1 or Idrlllnlli dY'f\metion. 10'1 more detai l:
1. Iow ... rum lOdium lhyponatreOl.iI): u.ulllly < 1$4 m£qll..
2 . low I61,Im o.mollliity. < 2110 mOnnIL
3. hl,h Urilllll')' lIOdiumA :... It wutin,,): 01 le ... l ,. 18 mEqIL. often S()'160
-4 . high rltio o(Urlnl:M n;lm Q8tnOUolil),: onen 1.5-2.5:1, but may be 1:1
$ . norttlllll'f:na\lUndion (ebec:1r. BUN &. ~.Ihlille): BUN eommon ly < 10
6 . normal.d .. n.aol function (no hypoiAnaioD, flO hype rlu lemia)
7 no hypothyroidi.m
8. no .1.". ofdoth)'dl'lltion or _ r hydra t lon (in many pat>enUi with lieull! b rain d,.ea... there i. signLiiaont hypO"Olemia often due to CSW (ou /H!/Qw ) Ind II thi '!&
I atimulu. for AOH lIr."ellC)n , the ADH relulM IM.lI be "appmpriQIa"")
\(further \.eStin, ito required, thl wate ... load Iell Wcmlidered to bl the defini t ive.
Ielt-. The pati.nt Ia ulud to con.ume a wal.er load 0(20 m.tIq up to 1:100 mi. In the lib·
tenet or,.drenal or ren&! inlu n-'dwty, the fQi\ure to I!;(~rete 65'110 of the ",. lH load in 4
mor ~ in.5 lin indkall's StAnH. . CAUTION : lhito te!lt i. danll~roWl if tile at.arting
IM!rllm !NII'I iI ~ 12-6 mEqIL o~ iftbe patient h .. I)'lIIpUlIIlII ofhypormtremil,
Ah.emll~ively, OM! may n:e .... u"' IM!ruJD <lr urinary I....ela or AllH "'hid> do nOrn1aUy
uodet.ectabl<! In hyponatremia of other uuses. In SlAOH , il IJ ollen detecl.3ble IUld , in
the ~tut of the low .... rum ~Jum, UCeII$ivt1e
Sym pto ms
ot S lADR
Symptom. ofStAnH art' lh_ ofbyponatrel1lia ioonfUli<lD, lethargy. NN, ClDmlI, W'
lure) Ilnd ponibly /'Iuid DY1!rkNtd. Ifmild , Dr if d ....... n~ of IN.'! i. gra:iul l, it mlly be tQI_ted . INa') < 1.2().12S I1IEqfL i. all1lost&!WlYla)'ZRptomatie. Theaep.atientaoften hlva
a pllTadol<ir:a1 (inIPJl"Opri~tlhhint.
_mEN>"
BellUre that hyponatremia IS notdu .. to CSW 1_
Mloui ) bef<l ... ..,.tsicting nulda.
'I'rola lQl e nt ot a lOlili: SlAD"
by anernill: usulllly ....pOll.h 10 trensfusion
;rmild and IS)'tnptomltic: nuid rIIItrittion < 1 Llday lpedr.l Uml/day)(eaulil)n
inSAfI; see /lJ'pt>rWJt"",", (olI4wing SAIl, p&ge188
ife~uud
i( sevel'll Dr . yroptomllt ie: UM hypertonic .. Un.. and , i(MCeU.ry, fu.-mKla(IH
pose 13). CAUTION: CPM IIl.Y botMHcillted wilh uteMiY1!l:,' r.pld cornelion
(..~pagt 12)
Treatme nt ot ~ SlADU
lo"l!·te= nufd n!!Itriniom. 1200-1800 OlIId
demeelOG)'cl ioe: 150-300 mg PO q 6 hni, I tetruyelinl antibiotk £OWId to PaTtioJly antliOniH the effeell or ADH on the renal tu~
(uro.emid .. Il..a.ixe): _ -40 mg PO q d (Dna! dlily) aIong"';th hiilh d1eury aodiulll
int.ke Ind monitoring for hypochtQremic . lhlDei,"
ph e nytoin IDiI.ntinG)): mRJI inhibit ADH ~I~IIII!
IIlblulII: not very ,,!fICtive and mloy lide effKla
Ce REBRAL SAl.T WASTING
Cer ebral ...It w a.tinl rcsW): reJ\llll_ oI~lum .. e ...,ull orintrRC'Mlniel dt.hyponatr\lm;" and. d('Je1'f,ll1l in ulI'lf;ellu\ar nuid YGlUDle'l. CAl1MON:
with anwl')'llma\ SAlI may have. CSW with hyponatremia .. hich mlmlet
SlAOH, ho~ ... r thtre \$ u.ually l ito hYJlO'l'ull!lIli1 in CSW In 1h1t IeltiDa;, ntlid ..,.vic·
tion mey eKaeerlNlUl ~a_pAsm Induced itcheoma-- ~u.e, produ~ing
pllti.n~
"
1.4.
~1uid •• ndEI..,trtll)'teI
GENERAL CltRE
The mechanism whel'flby the kidneys fail to conserve sodium in CSW is not known,
and may beeither a I'flsult ofan as yet unidenti fied na t riun!tic fBctor ordireo:t neural control mechanisms ($ell Hyponnlremill (oJ.Jcwing SAR, page 788).
Laboratory Uleta (seTUm and urinary
electrolytes snd osmola!itiea) may be idenTable 1-7 C$W va. $IAOH 30
tical with SIADH and CSW". Fw1.hermore, hypovolemia in CSW may stimulate
ADH release. To differentiate: CVP.
PCWP, lind plasma volume(a nuclea r med·
icine study) are low in hypovolemia (i,e.
CSW). Table /·7 compa res IIOllle features of
CSW and SIADH. the two rtlOIIt important
differences being extracellular volume and
saIl ballUlce. An elevated SeTUm [K-1 with
hyponatremia is inoompatible with the diagnOl iaofSIADH.
0
•
Treatment or csw
•
Goals: volume replacement and positive sa lt balance. Hyd rate patient with
0.9% NS Or sometimes hypertonic 3%
NaC!. Salt may al!!o be replaced oraUy .
Blood prOOuct.l may be needed ifanemia iii
pruent. Rapid COlTtCticn of hyponatremia
haa been 8JlSOCiated with CPM and care
should be taken toavoidovercorrection (su
page 13).
Fludrocortisone acetate acts direetly
on the renal tubule to incl'flaJle sodium ab.bbre""'!Ions: j • dset..ued. t • _..ed. t t·
sorption. Benefits of giving 0.2 mg IV or PO
slg nllican'l~ Jnc',,"sed. WNL • _~ no, ..... !Wl>q d inCSW have been reported", but signif·
lls. no A • no cIIIngo , U• """"",,1'0Ii0n, + •
p,esenl, • • Ina)' Of may no! t>e pouenl
icant complications of pulmonary edema,
hypoulemia and HTN may occu r.
An alternative tre&tment using urea may be applicable to the hyponatremia of either SIADH or CSW. and therefore may be used before the cause haa been ascertai ned:
urea (Ureaphi J®l 0.1) gramslkg (dissolve 40 gn' in 100- 1$0 ml NS) IV over 30-60 mi1lI< q
8 hr&". U~e NS + 20 mEq KCVL at 2 mVkglhr as the main IV until the hypOnatremia i5
corrected (unlike mannitol, urea does oot increase ADH secretion).
H VPERNATREMIA
Definition: se rum sodium> 11)0 mEq/L. [n neurosurgical jXltien\JI, m08~ often se<ln
in the setting of diabetes insipidUl! ( Dl) (.ee below ).
S in<.:e nonnal total body wat..'r (TBW) i, . 6O% ofthe patient', normal body weight,
the patient's current TaW may be estimated by Eq J·2 .
TBW.-.... '"
( N.· l-....~ TBW_,
[Na 'l:"""..
140 mEgIL. 0.6. usual body WI
{~s>
(N~·.k-ou
Eq 1-2
The free water deficit to be replaced il given by Eq 1·3. Correction m .... t be made
slowly to avoid exace rboting cerebral edema. QnUaIl the water deficit is replaced over
24 houfll, aud the remainder iY given over 1_2 additional days. Judicious replacemen~of
deficient ADH in cases of true DI must also be made (see beloUl).
fttt watt, d.ficil • 0.6 . usual body wi (kg)_ TBW","""
'"
[Na'l~;;;'~~::" mEqil" 0.6" usual body wl (kg)
GENERAL CARE
1,4. Fluids and Electrolytes
Eq 1·3
"
D IABETE S INSIPIDUS
TKey
~tu _
° due to low leve11 of ADH (or, nIT..,i)'. renal in'''Mit;vlt)' to ADH)
hi, h output of dilute ur;ns « 200 mo.mol/LQr SO < 1.003) with normll! or ht"h
~""'1Il (llmol",ty
• of\en aceompanie<! by (rtI"jng ror water, elp«ial1y ice-waler
• danger of HVere dehydntion i f not managed carefully
Diabetes in. ipid .... (Oil i. due to ifUluffieient ADH, and resu l ~ in the excell$ivI NO·
nalloa ofwat.er and elec1.rolyteL Dl mllJl be produced by two different etiologiel:
• ce ntral or Murogenie 01 : a .. bllOTolat lev el. or ADH t outed by hypothalam.ie_pltu _
ita,.,. axil dysfu ~;on. Thi. ia the type mo.! often Hen by neu,..,. .. "¥eonl
"De phrore n ie DI", dIM to relative THi,tance of the kidney to normal or upranorm.II...."I. 0( AOH . SHn with IIOms drup t- bcolow)
•
1
EtiolQ(iH orOI";
1. (neur<lt!enkJ diabetH ill8ipid"l
2.
A. r~ili.l (a.,t.o.oml! l dolmiMnt)
8 . idiopathic
C. poIttraumatic (andudintllurgeryJ
D . tUOlor: cran iopha.ryngiolfUl, mlta,ta, il, lyrgphoma ...
E. gran .. lom.: neuresarooid ...i•. hit.tiocyto&i.
F. inff(:tia.." mlni"';t", enc.ph'litit.
G• • utoimmune
H .....cul.r: .neurytm. Sheehan', ayndreme (n rely c.us" 01)
nephropnk di'betes in,ipid ul
A. r, mmal (X-linked recessi ..e)
B. hypok.lemia
C. hypercalcemi.
O. SjilgN:n'lIyndrome
E. d .... p: lithium. demeclocydlne. colchicine...
F. cbren ~ ren.1 diMue: PYtionephritis, .myloidosis. s ick le ceU disesse, poly_
ey. tic kidney distflse, u n:oidosi.
CENTRAL DI
~of ADH ","cretorycapacily mUllt be lost bef...... din~al 01 ens ...... Cha racteri$lic
high urine O\Ilput (polyuri.) with low urine ""molality, and (in the conscious patient)
cr.ving ror w.ter {polydipsi.). especi.lIy ife-water.
Different ial diagnosil of 01:
1. (Detlf"O«!ftic) di.betea iosipidus
2. nephrogenic diabetes insipid ",
3. psychogenic
A. idiopathic: from resetting of the osmOila1
B. psychoglenic: polydipsil
4. osmotic diures"' : e.g. following mannitol. or ",ith renal glu<:OM .pilling
5. diuretic use: furosemide, hydroch lorothiuide ...
Cen tra l 01 may be ~n in Ih.. foll ..... ing ,itu.lioruo:
I. foU ...... ing tr.nssphenoidalsurgery or remoul o(cr.niopharyncioma: (u ....lly
Imnsien!, therefore ...oid long •• cting agent. IUltil ite.n t.. detennined if long·
term repl.cement i. required ). lJUury to the post.erior piluitary or .talk uluslly
causes one of Ihree pal\.ern. ofOlIf:
A. Ir.n.ienl 01: . upra·norm.l urin .. oUlpul (UO).nd polydipsi. wh~h norm.li%1'lI _ 12·36 hni .,...I.op
S. ·prolonged" 01: UO ItaYllupr.·nono.1 for prolooged period (may be
montlu)or eve n permaDf'ntly: only aboul one third oflheu !MItientl will nOI
ret urn to new-nonn.l.t one year ~t-op
C. · triph ..ic . ... poD ...·: I<o..t eommon
ph ... I : injllTY t() piluitary redUQtf AOH I. .... t. for 4-5 d.y' - 01
{polyurialpo:ilydiJlll;.l
phase 2: cell de.th liberB," ADH for the ne~t 4·5 d.y. - tralll;enl
nonnaJiution or even S lAOH·lilo.e w.t.er retenlion (HB; the ... i. a
dan""r of ill advertently eoDtinuin, .. aaopreuin therapy beyond the
initi.IOl ph... into this ph ... c....in. l ignificanl hemodilu\i01)l
phllSe3: reduced or .~nt AOH teCrelioa - either t r.n.;"nl 01 (•• in
"A" ,bov,l cr. · prolonaed" 01 (•• in "S" ahavel
"
1.4. Fluid. and Electroly,"
GeNeRAL CARE
2. following brain deoth (hypo!.halamic production of ADH "",as"51
3. wi th certa in turr.or& (e.g. craniopharyng'iomo. oft.!n pOlItopet~tively): rare. sInce
damage 1.0 pituitary Or low" r stalk don oot prevent produetion and relew;e of
ADH by hypothalamic nudei
-l. . wi!.h o!.her mallll luloflS prt'lOSing on bypo!.ho.lamUli ; e.g. a·comm aneurysm
S. following !lead inj urY: pr>"ulfily with ba sal (clive!) . kuU fr3Cture& !&N! P<lI1l! 666)
6. wi!.h encephalitis or meningitis
7. dtug induced:
A. ethanol and pllellytoio ean inhibit ADH rele a6e
B. "xogenou,et.<>.roidiIT\8Y6fi>m to "bol\(out" DI be\:a.use t.heymayeorTfflad.... nal inBullidency (Bel) Diogmni, bel/lw) and !.hey lnhlbit ADH relea ...
8. Wegener's granulomnto!Jla; 0 YO!lClllitla (He p"gt 61)
9. innamllUll.OrY: lYmphocytic hypophysltia<' (U'l posr 928) or lymph«,ytic
infundihuloneur:lhypophYSitilr" (d iatind oonditiollll)
DIAGNOSIS
The following are u"ually adequ9le 1.0 make the diagnosis (>fDl , /;lIpe<:i~l1y io!.he op-proprillle clilli«ll !etting:
I. dilu~ urine:
A. urine o l"l>ololit)' < 200 mo.mIL ( u~ uaUy 50-150)'" or s pe<:illol>'Tllvity {SG)
< 1.003 (/JIlIY be 1.00 1 to 1.005)
B, or theinability toconcentrate unne to:>o 300 mOsmIL in the p ..... enOllordin·
ica.l dehydration
C. NB: largi! d08e8 ofmannilol fill may he !,lied in hell(\ mumn elIn m>l$k thili
by producins p more COMentrllted urine
2, urine OUlplll {UOl:>o 250 cdhr {peds:" 3 eelkgfhrJ
3, norma! D. aoo..e_nonnpl seturn .sodium
4 . normal adrenAl function: OJ cannot oc<:u' in prUnary adremd insufficiency beCl\usea minimum ofmineralOOlrticoid a<:tivity 15 needed for the kidney to make
free waler, thus st.eroids may "bring ou t" underlying O! by correcting adrenaJ InBufficien~
In Wlcertaio CIISelI, plot simulta·
neoulurine and serum o~molality
on the b'Tllph io Fie'''" !.J
1. low ~etum osmolality; tile
patient hn polYdipsi~
2, if the point fall, in the
"normol" .... nge, IIlJ.U1tt:
!iH!1 WSl<'r depriv9!ion
latis neede<l tod.~rmine
if the patient can co;>ocenlra~ their !,Irine with dehydration {caution: IU
/Hilow}
~
POL Y?IPSIA
3. high setum OIImo[al;ty: d; ·
agnosia of 01 i! "I!It 81>- 600
lished, and further leating
NORMAL
is not needed (exrept to
differential<' central from
nephrog,mie 01. if desired )
t.o differentiate cen·
DIABETES
; 200
!.ral from t.ephrogenINSIPIDUS
ie 01, give aqueous
Pil.rWlinlll5 U SQ:
in central D! the
!elUIl1 osmolality (mC:>!mo1.)
!,Irine osmolality
should double within
Figure 1-1 Interpretation 01 s lmultall.eou, serum
1·2 ho ul'!l
vs. uri"" asmolallty
01. plotting more than one
(FIIIVide<I tl'f NnoId M. MOMs. MO .• ""'" will> p,,,..-oe)
ds\tl point may help as
son,e Plltients te1ld to "v"c_
ilJat.<>." around the border 1.0,,93"
"oor-"--I
,ooef-t--t--t-,!
'boo
t
I
r-;-- r-i;/
~ "'"
tt::::::l='
O\2J.706=O~2~SO:=~2!"~~20'~'~-:29~2~C29~6
OeNERALCARE
1.4 . Fl!,lids aod Electrolytes
"
Wa te r d e p ri vati o n teet
If JIilI \lPelear. the diagn(llliliorO I i. QIlnfirmed by a WB1.er deprivation \olin! . CAU.
TlON: perform only unde, clOle .upem..ion ,. rapid and p!I~nlially fa tto l d~ hydniliM
maye".ue in 01), 'nI.. Wt .. t'BJ'ely neceu.ry ifllef\lm namnl.lrlY> 2911 mOsmILA Stop
rv. and make th e patie nt NPO: ch eck urine OIImolal;ly q II • .
L a mtinue the ~t until \)ne orth" foll.owing OeruJ'lll:
A. normal response occu ..: urine output del:"'~lu. and urine na'nollllily..ue.
t.o 600-850 lfIe>.ntIL
B. 6-8 lIounlllPIi4!
o uri...., (ll molelily pie lnul (i.e. clUlIlge. '" 30 m(fflm In 3 ~on~("live hou ..'
O. peli~t to.H 3'1& ofbod)' weiJht
2. If patient rai,. 10 demoost.tllte the norm.l ,up!lnH. then:
A, FYI emsel\()UI AllH {5 U Ioqu~~ Pil .....,inSSQI, which nnnnllUy lhere • • •
.. uri ne o.t .noltli ey to > 300 mO.o::v'L
B. chedc urine ".molallty 30 and
60 IBinutu late r
C. tampa ... highelt urin~ OIImol,·
lily .Iler P,I.reUinG'J to the 0&.
mola lity jUlit ber," pic..-in®
B«<lniinll to Tobia J.lJ
TREATMENTOFDI
J.g .nd 1'abk 1·10 rOl'doII,",
rOrml . nd duration of ection (J/ ",.,.,... _
~1'obl.
pressln p re/N-I'1II;M • .
Teble 1-9
A,,~IJble
" eaOprtlllln
I
"
I
A.
B.
OR
2 . ADH enhanan, ....h .... lions (worka primanly in chmnk pertilll ADH deficiency.
W,lI nol work in total /obaence of ADH)
A. dofob, al.e (Almmid SIS) 600 ... , PO QLD
B. .hlnrpropramide: increelel...-mol HIlI,tlv; ly 10 ADH
C. hydrochlo..,thinid. ; thi."id. d i",.tiQlIO"" act by depklit.l, Nt.' which In.
ere_ rn.t-rpt ion in proximal tub"l. . .nd .b1ftin, flu:d aw..,. {fOIl] ru.t.al
t ubul" which it when! ADn won.... Rr. ~.I Oyaxidc$1 PO q d (m.y IncrellH up to 2 per d .)' PRN)
I.n
~Qll.I
ambu.l.a tory pat ie r'll wi th Im painld th irst ole eb ll.Qla m.
Ifthint mechllli.ml .... lIIlI. in Ulct in CODKious emb"hl1.ory pIItl~nt, lMy run \.hI
risk or dehydlll tioo II, fluid .... e, l... d . For th.,.. p&tienU:
L have r-tw,nt rou... ", UO and daily "'li,M" balat10Ce fl"id IDUIU and ... utpul ...in«
A
"
in ~"""ID .......oI,1,Y It -..lllwly 10 bt. ....."woo ....,t.p ..,II>.........,...
1.4. Pluidu...:i Electrolytes
GENERAL CARE
an~idiun~ic rut'dication u needed to keep UO reaS(Onable
2. check serial laba (approxi·
mately <t wHkJ.y) includin(
Ta ble 1-10 Meantime
H nun .odium. BUN
,
III n o n ·arob uJ a to.-y, co ma·
toaeJat u pon>u 8, or braln ·d ead
p at ie n t
(also leo! MonQjJrnunt o{ftr brain
dUJlh {or organ doILotion, page 169)
I . follow 1'1 &. O's <t 1 hr, wIth
urine ,pedro. iTavity (SG) <t
4 hr. and whenever urine
output (UO):> 250 mlth.
2 . lab" Hl'\lm alf<:trolytel with
OImolality <t 6 II ..
3. IV fluid management.:
~05112NS.2:0
mEq KCUL at appropriate
rate (75.100 mlthr)
FLUS: repla« UO above
Mile IV rate ml for ml with
' " NS
~OyAMolclM . M:IMI. M. O~ _..;u. .......
......
aI.,.,..~aI""
.. _ ...... »45
minuI" 1oIoMrIg ............ (e-.,. piI<Noy PIJIO'dIr
NS, for post.op pat.ienl-s. if
llloiI~_2-.rwslO . .n~)
the patient rece ived .iilliIi·
. ....., .a'V!tam poUeoot 10 ~ tIt.oI ... ......,
cant intraoperative fluid.,
\lOrIIIi8Itnlin"'~~
then they may have an Ik
_
, lliQ 810 01 dHmop...... .. at ,,*,,,,,, at 4 1iQ Q
~p<>IIklpdi\U'""is.in t
lI.tIt.oI-*I-.sIyoe_.--...
this caae use 1fl NS to replace only ~ 213 ofUO that
exceeds the basal IV rate
4. ifuneble to keep up with nuid lou with IV(o. NG )replacement {ulually with UO
> 300 mllht), then EITHER
:; U arginine vasopressin (aqueous Pitresain®) IVPIIMISQ q 4-6 h ... (avoid
tannate oilnt'pension due to erratic. absorption and variable duration)
OR
OR
vasopreni.n IV drip: aLan at 0.2 U/mi.n & l.ilnlt.e (mu: 0.9 Uimin)
desmopn'Sllin i.rl,iection SQJIV titrated to UO. usual adultdoee: 0.5·1 ml (2·
4 1'1) daily in 2: divided dose.s
1.5.
Hematology
1.5.1.
Blood component therapy
PLATELET'S
Nonnal platelet count (PC) ia 150R-400K"'. Bleeding (lponLaneOUS 0' with invasive
pl"O«dures) wrarely I problem with PC:> SOK. SpontaneoWl h~morrhap i, very likely
with PC < ~K. I unit conUlitll 5.5 II: tOI' (minimum) to 10 X 10" plateleta. The volume or
6 W\ita'" 250-300 ml. Plal4!leta mIIy be .tored up to 5 dlY • •
Recommended tl'1l1ll i'u,ion crittri. o.:
I. thrombo<:yto~ni. due to I production (with or without increased destruction)
(the molt common cauletl Ire IplUlio: a.o<!:mi. and leuumia)
It. PC < 10K IVln if no bleed.ina: ( prophyl~ t ... n.r... ion to prevent bleed ins:)
B. PC < ZOK and blee<iinr
C. PC < 30K and PfltMnt at ritk ror bleeding: complainta orHlA, hal connuent
GENERAL CARE
1.5. HematowIY
"
(d. scllt~red) pete<::hill/!, continuo ... bleed;"1 from II wound,llIer..
;nal heOlorrhage
,;n,
~t­
D. PC<SOKAND
I. m~ lu rrery planned within 12 haul'll
2. PC rapidly f"llinl
3. pata nt < 48 bou r . pcMIl.-op
4. patient require. l.. mW . punctu~
~.
acute blood 10111 of > I blood volume in < 24 houn
2. platelet tran, f\lliol'll have limited utef"lnttll wilen thrombocytopenia I, due to
pia Ie let dfttruction (e.g. by antibodie ••• in fT1'P) or co",umption (ifproduetkm
1.ltIIequate or Incte.ued, platelet traosfu.;on usually will not be useful)
3. dO(umen~ plaUletdyaru.netion in II p' t len t "h~u led forlurgery or in .. patient
with advanced hepatic andfor renal iNuflidency (con,ide r pharmacologic l'lInancemea\ o( platelet fUnction, I.g. desmopreasin f ')
Other inOic:ation. for platelet t ..n.r.... ion,
1. ptltiente
have betn on Plavilc®or upiri n who nee u'llenl , urgery U, IILclln not
be poatpone<! for _ $ daYI to allow new plateletll to be synthesized
wno
"""'"
Approximately 25'10 ofplateleUl are losljU.t with transfusion.
Peel., I Ull'I)l rsi_ PC by ~ 10K. UlusUy give 4 Ulm·.
Adult: 1 U raise. platelet count by ~ 5-IOK. Typical dose for thrombocyklpenic
bleeding adu lt: 6-10 U (UIUa! order: '8-paek"). Alternatively. I U of plleresed pl ateletll
may be given (ob~ined from a lingle donor by apheretlH!, equivalent to 8·10 U of pooled
donor plateleta).
Cheek PC 1.2 h .. after transfusion. The inc ..... ue in PC will be leu in DlC, ""pllis,
splenomegaly, with platelet ant' bodie., or if the pIItient is on elwmotherapy. In the abIfmtf! of intreau-d cons\lfllption, platelets will be needed q 3·5 dsys.
P LASMA PROTEINS
FFP {FRESH FROZEN PUSMA}
1 bag. 200-250 ml lUlually ..... ferred to 110 'unW, oot 10 be confused with ivnit of
{odiN ,,"'ivily which isdelined II I mll FFP is pllllll1ll separated from RBCs and platelets, and contains aU coagulation factoMl and natural inhibito... FFP hu an Dut-<late period of 12IllOnth•. The risk of AlDS and bepatitis for each unit of FFP is equal to that of
a whole Wlitofblood.
Recommended trans fusion criteia (modi fied"'):
I. history or c1ini(al course s,,""li ve of eoquiopathy due to tongenit.al or aequired
coagulation factor der~iem:y wilh active bleeding Or pre-op, wilh PI' '" 18 sec or
AP'n' '" 1.S II upper limit ofoonna l (usually'" 55 sec). fibrinOCel!. functioning normalLyand l"el '" 1 gIL. and «III(Ulation factor aMaY < 25'10 activ ity
2. provenooagutatiol!. factordeliciency willi active bleeding or lCheduled forlurgery
or other invuive pt(l(:lt(iure
A. QOo&enial deficiency off..,tor II, V, VII. X. Xl or XU
B. deficiency offactor VIII Or [X ifufe replacement faclOn unavlil.bl,
C. ¥On Willtbraocrs di!leue unreapOnliv~ to OOAVP
D. multiple «III(Ulation factor deficiency as in hepatic dysfunction. vitamin K
depletion 01'" Dl C
3. /"tve,...1 of war1arin (Cou.madin®)efred (PT > 18 He, or INR '" 1.6) in pati.n~ ac'
tively bleedioa-or requiring emefJrency surgery Or prooedure with insufficient
time for vitam in K to COrTect (which u.ually requi .... '" 6-12 h.no) (Nt fXJl' 24)
-t. delicier'K'y of antithrombin Ill, heparin cofactor II, or protein C or S
6. mauive blood tnnsfution; replao;emtnt or> I blood volume (~ S L in 70 kg adu lt)
within leveral hou ... with evidence ofcoaguJat ion defK'ien~y II in (1) and with
continued bleedin&
6. treatment of IhrombotJc thrombo<::yt.Optnic p!.Lrpura, hemolyt ic uremic ~ ndrome
7. • beclUMofauociat.ed haurd. and suitable al!.ernalives, the UI8 of FFP a.a vol.
u~e O!OI:pander iI retatJvIly QOntraimlic.ated
Do.age: Ulual.t.artina dose il2 bop orFFP(400-600 mI). IfPI' ill8-22 aeca or AP'n'
i, $ .70 aeca, 1 ha, may suffiOI. 0-. as hi,b a. 10-16 ml/kt may be needed for lOme
patienUl. Monitor PI'IP'IT (or specific factor ....y ) and clinical bleed in,. Sinoe fatlllr VI [
ha. a shorter half.life (~ 6 hn) than the othe r facto .... P'l' may become prolonpd before
10
I.S. HematolOfl)'
GENERAL CARE
APIT.
R&mernbtr: IfpaOent I•• t.o re.x>lvlll( pl.tel.II, thaI for every 5.6 IInl1.1 of plal. leu
the JMltl.nt I•• Iao reallvi ng coagul,tion r8~tONl equivalent I.(l ~ 1 bag of FFP.
ALBUMIN AND PlASMA PROTEIN FRACTION (PPF, AKA Pv.sMANA TE®)
U.ualiy fro,n outdated blOC)(!, I ...led to inllttivau hQpatitia 0 vim • . Ratio of .IbuTII1n:,lobulin P4'1'Drnt.ll,! In ".Jburuin" illl6\1U~. in PPF it .. 63'11:17Ilo, Av,ilabJ" iu 5'"
(OO(Oliul!, ..nd otmotlcalb O!quiVilellt to p18ll"'8J aud 25'i11> (contraindiut<!od in dehydrat.ed poIti.!nt..,. 25'" albumiu n..,11 lot diluted to Mil by mUting 1 volu me of25'il. albumin to 4
VOhllDH of rx,W o r O.9'l NS (_ caution: mixing with I teri l. water will result In a hypotonk 8OI ution that can ( II""- hemol)", , and poai bl a ,-..nQ] fallllJ"eJ.
E:cpeMive for UH .imply u . volu me "~paud,,r (- $6Q.&O per uuitl, lndica\.ed only
"'Mn IOlaI pr()W:i n <: 5.2 1PlI'Ilo(otlw!rwISl!, uncrylt3 l1 01d which i •• quall)' effective). Rap·
id influiOli (;> 10 celmin) has \)Mil ~pGrtcd to UI\1141 hypot.>na;o:l, ld ...... to Na 'ac~late and
lielemBn r~Ot r'~ ilMn""). Ute in AROO iI controvenial. In "euros .... g;cal patieQI.S,
may be <:QNlid ... red .. an adjunct I'or vol ... n>e expan sion \a101lg wilb crystalloids) ror hy.
pem)'llllmic th,rapy CH.1IfI.P 197) wllm the hem atocrit Is < 40'lI0 fQUO'Wlng SAH wh~
tMllI I. cOIKIIm about irlen!..;ng th. ri.il of rebleedi.JIr e,g. wilh the U5l! ofh.etl1llt.~r~1I
pagt 781).
c.m
CRyOPRECIPITATE
lrIInsfu!liGn mteri e;
I heonophiJia A
Rfoeom~nded
2.
vOn Willebrand d isea ....
3. documented fibrinog~nfr.dor VIII deficienc,y
4 docwnen~ di55eminated inl.rll~allCUla r t'OIIgulation tDI C~ alonl with oLber
m.odeoI oftberapy
1.5.2.
Coagulation
1.5.2.1.
Anticoagulation
AN~GLt.ANT CON51OERATIONS IN NEUROSURGERY
Contralndication l to beparin tberapy
Many U'adilional contraJndkation.aalll bein, r~nlIidered and challenced. M"';Vf
PE producinghemodynun itO)mprom iH should bI! treated witlli nticoogulalion in mOll~
dupite in traut.nial rUb. ContrRindiCl tillnt to h,~rin include;
.-..cent !leVeR hud injury
te«nt uarllolomy: ..e IMI"",
palj..,ta wi th roIIplopa thia
hemorrhagic infarct ion
bleed.inlulcer or otbu ,nllcc85.bl ... blH.hng si te
'Hitolllrollto bl" hypertan5jon
Vvelll hepat ic 0. renal dr_v
immedia tely before inv..ive procedu .. (au ~ for ar.riocnphy 0. my~IOI"T"
phy)
b... in tu mor;,"~
cue.I
10
pati~lltllwltb
unM.lphu'-ed (l ocide otal) ce rebra l ane u rylIm ,
Nllioo.l\IlMion 111&, no!. ilKrN'" the rillil of he,""rrba~(i .e. r upturtl. hO'Wevt'r,
. hould nrplu .... occur, 8111ticotJUJItion would most likely inl!l'fue volumeorhlmotTh.~e.
'lid
o,u. ;nCff'a. morb'di\,)' and mortallt,.
In plltieou wic.b braJn tumllr
Sonw au thora are .... Iuclanl \0 adminil ter heparin l(I any p!!Iti~nt with a brain
lum~. , Itl\ouih a numbr!:ror.tudJ. found no hi~u ri.k in th .... patientawhm treal'
f:tiwi\h her-rin til' DrIII.nt~ lat;"" •..·(PT.hould be follO'We<l yery tlo..el),,_utwiy
r«:Oll\IMnded m.i nUinin , f"I' _ 1.2:5 • ""ntm!").
POfIt«JpertltiveJ y rollowill' cra niotomy
ReQuil'8S individualiu.tion baaed nn the ruaon fOr et'lltIiotDmr (I.L luruur . AVM , an·
eurya-m, e~ ). Howe ...... , most n. uro .... rgeon. wou ld prob. bl, not fulb' antioo.gul8t.e pa-
GENeRAL CARE
l.~.
HematQJogy
"
tients <.3·$ (laya followingCl'lUlictomy", and soma t~:omroeJld at lean 2 We6s (one
itud]' found no lncfea8udlncidence "rhll!f!ding when 81Iu"'8g1.1latiol1 W8$ rellun,ed 3 day.
POIIt craniotomy"').
S afe le ve lll of PTIINR to pe rform o e urosurgicaJ p l'Of,:edures
Patienb on warfarin who mUllt be anticoagulated .... !,,"g·u po!<!IihlB (e.g. roedl/m i.
cel hllllrt Yalv~a) nred \.Q be admiU"d to tlul h0i5pit.allll\d converted to h~parin , Moet eIIn
stop warfarin at home, ~lId theD be admittotd 2-3 d ..~ later and ~t.arted on heparin lUI PT
begina to normalila. Pat;enlJl with 1"811 critical nee,h for antio:o.gu lation (a ,g. chronit."
lib) can usuAlly ~ takM offofthe ""arfann at ]Il""t 4·5 daY" before the procedure, and ..
Pl'IlNR is (nlln mecked on admission to the hoapilal. Pntienta ~ to be aware thatdlJr·
in,s the time that they are not antit<)agu lated, that they are at risk ofposslble romplica"
lion8 from !.he lvndition for which they life !'eC<'iving the ",ana ~ rlo k for
meehaniclll nlve iA . 6%, for .·fib it i. ~ 1.5,*,).
In p a Ue n l.ol n eed ing IlDgi o gra ph y or myelo grap b y. In 1111 pllti.. ntB,
hn pnor ro
~tudy.
mil
~top
h"pllrin 4
For non·em.e rgcn L n e urosurgical proced ur.llr. For procedUnlB where posl.-Op maSli
effect !Tom bleedIng would po6e ... rious ri~k (whioh ;ndudes llIost neuroourgi~1I1 o~ ... •
tiona ). it ia recommended tlllll. the PT . h u uld be _ .. 13.5 sec (i.e . .. uppe r limiUl ornarmill ) Dr the JNR sb o ul d hOl - '" 1.<4 (e.g. fur n!fe","CII, thlB INR ',s ~"Onl.id"rN ~af.. rDr
performing II percut.llneou. needle li ... er biopBY). To r .. v"rs .. antieoagulllllUl.1U JXl8f 24 .
F or em erle nt ne urOHur]i(ical p roced u ..... For eme'JencYlitulltiolUl, giye Ff'P (Bl.lln
with 2 urnta)lInd vito",in K (10-20 tug N Ilt" 1 mg/miD) II !lOOn s5 poe.8,bl" (u:e ~e U
far fIl ..... rsal ofantiCOllgUIBtianl, The timing of . urg.. ry;8 th .. n ba~o~ the urgency of the
.itUlltion Ill1d the nature of the ptoCl!dure (e_g the decision might be til evacU8~. spinal
"pidurol h.. matomll in sn acutely »3r11lyzed ""tient befo", anliC08gullltiDn is fully reY~rsed).
ADtipla tele t drugs a nd Deuro!lurgical procedures
Plov\x®(clopidogrel)($tt pagt fJ72) and 8.IIpirin cause p....mAnent lnllibition ofplatelet function tn.t pel"lliats - :;, days al'le!: diloontinUlltlon oftbe drug and CDlI ;~""Ul!- the
risk of bleeding_ Fl>r elective callOlll. 5·7 dl\Y1l offthesa drug5 il1"8<'Ol1IUlended. For e,oer·
galley Burge,.,. platelets may be given (art ~ 20), howeyer. with Plavix the drug ~r'
,ist5 in the lytLem for up to a couple deya lifter the last do:oe. and can actually Inhibit
platelets given o{t.r the drug is dificontinued rthe half·1ifeoraaplrin ia lower IIIld ahould
not be an iuI,I« after I day). [n cas... wilh contioued ooling in the fj"t day or !to afUlr
w;,,",ontinuiog PlaYi~. use tb.e following regim~n:
I . retOmbinanlactiyo!ed coagulation factor VII (rFV1h,J: even thnugh the defect ;s
in the plateiett. rFVlb ...·Iltluo:. via a rnechllnlsm not mtdlated by protein clotting
factor.. Very exPl'IUI ..... (_ $10.000 per dose). but Uti, mU5t be billanced againBL
the..u.o\ Ilfrepeatcraniotomy, increased leu Slay and additional morbidity
A. initial do"': 90-120 m<.'g/kg
B. Bamedole 2hra11lter
C. 3rd dOle 6 hra lIf1.er initial dos8
2. platelo;lS every 8 bouN! for 24 hour8. ~
A. 6 U Ilfregular platel,ta
B. 1 unit ofphe"'"",d platelets (ifpt. ill on nuid or volume ~atrictiOD )
or
ANT~GULANTS
~
heparin
\
I
OROO Iff0
\,
ilJt: Administered a. TV drip or luh ·Q bolua. To antil"OlIgulat<! "'erage waight pa·
tient. giy~ 5000 U bolu" TV . follow with 1000 UIhr N drip. Titrate to therape-utic entitaBgulatioo of APn" ~ 2· 2.5. control (for OVl'. Stlme recommend 1.5·2. conLTQI"' ).
SID'~ (""eA"lkoog~lclllj consuumfWIU tn lIeW'O$urgery aboye ): hemor.
rh ag~. thrombolii611O (he]>llrin activates ."tl·lhrombin lJIand can CUU$e plateletaggrega·
tion ) which caQ rEDult in 10111. CVAs, OVl'$. PEa. etc. Thrombocytopenia: tranSient mild
thromboo;ytop.tnill i& (airly common in the 61'11t few days "fter initiating heparin therapy.
however se>'1'rE thrombocytopenia IK:CUr8 in L-~ of Piltients l'eCf!iYlng hepQrin " 4 dil)'ll
(usually has a delayed Dn5l!tof6·12 dilY~. ilDd is due 10 CDlUlumpt;on in heparin·induced
thrombas" or toantibodill!l rottlloo. ~g3il1fit~ hep$rin·plllteletpTOu,in ooltlplllX I. Conijider
LIM-of l~pjrudin (",~ tHlow) iD thrombocyr.openic patients. Chrollk th4!rIlPY may cRUle OIl·
teopOrlI6~ .
II
1.5 Hematology
GENERAL CARE
Low mo lee ular w e ight be pa ri n IJ""
Low tnQlec:ular wei,hl hepl.rinJI (LMWH) (.v~llIge mol~ lar weight .. 3QOO.OOOO
daltorwlare derived rrom Wlrractionllted hepllr in (IVlrIlPMW", 12,OOO· 15,OOOr:\altoM).
LMWH. dllr•• from UnrtllCI;onnted Ileparin becaute th ey h.v • • higher ... 1;0 of IInli·flll<..
tor X. 10 11I\t!·flIc!or n . (antithrombin) aetlYily whleh theurelicnUy . ho\lld producor .,, \iIhrombie 'fTKI.I with fawer heODorrhaljlc complicatioN, aealiutlon
orth~
bene6t tI..
been ..... .,. minor In clinical trialt;, LMWH MV11I.ellt&t bioIIIvailahflily .ner aub-Q inJec·
lion luding to more p."dlcillbl. pl .. l.ma l,,,.1II wh k h eliminatq Ihe need to roonitor blo-
lo';'c artivit)' (au ell •• Af"M'1. LMW U have .. lonller hllif-lif. and
t1011U pt. rl~y.
thl!fffo~
require few!!\'"
Oruglo'inctude:
da1teparin (Fhopinl»); Rx 2600 ~ntJ·Xa U SQ q II
eno~.pllri.n (1.A.o .....nodl): & doSll,~ eslllbli.hed foll"wini bip replacement u- 30
mg SQ BID JI 7-14 day•. A1tetnatlve: 100 Ulltg SQ BID
ard~parin fNQnnlflt4): Rx 00 1ll>1!.x. UiKc SQ q 12 hn
•
dllnllparoid
(O~tHrlOn®):.
i'w!paring,d.
E~n
hither IOnli·X,a:/lnu .lla MIllo than
LMWB •. Doe. n6l require lal.,u111O')' moniloDnna. 1U 750 antl.Xa U SQ BID
tinnpario lLoaiJlOrinS. lnnohep®); notav.iJ.blt in U.s. ~ 176 antJ ·Xa U r-erk(
SQII"ced~ily
S pina l ., p idurlO! b~ .wma.: 'l'Mrr have lIMn. num~r of aiR repgrW of,plllal ep'·
dural hlln'atllmIUI oecurring in p"'lien ~ on LMWH (primarily tno.apatial ... ho 111110 U"'derwent spinaLlepidurnl .. ...,.lhpi. Or lumbar puncture , primArily in rlderly "'.,/flal
undergoing urthopedic lurgef)'. Some h.ve bad signiflc.nl naW'OlO¥ic Hql.lelae. includ·
ing permantM par,IYlilI". The risk .. further incrta5ed by Ihe Wie orNSAID., pl.telet
inhibitoR, orothe•• nt;ooaguhUl~.lIl1d ... il h Il'8umll'(I or rePfated@piduralor . pina.!
puncture.
Fondapal"iow: (Ari ll:t ra®)""
(ncrealle!l ractor x.a inhibition ",ithouta(fectint: racto.r Iia (throlQbiD). UnCraetiunllt·
eli &. l.MW heparin. bind plalellOl fac:tor 4 and caO UIWI ;mmUllftomediat..d heparin.,n.
dueed lhrombaeytoP"!'ia (HIT) . FondaparlnllJ' don not bind plal4!let ractor 4 , and h ...
not caUlled HIT. May be. mo.... effective than enoxaparin (r.o-.·e~) for pn.·lI!nlinc pilat ·
op OVlil. S IIICD'f1«:'1'S: BI@ed;ngillhemO;!llcommon!lidedfl!Ct lm..,.boJincreauo;tbyCOfl·
current NSAlO u",1.
Rx: 2.6 '"i SQ injection q d. lWPl'Um: 2.5 mg Ilnglwose.ayringes.
Lepirudin
( Renud ~)-"
A direc:llhrombin inhibitor which blocks the thrombogenic .... tivUyofthrombin.
and, IInlih heparin. lleo "'1-11 on dot-bound thrombin . II is rnA IPJll'O'I'ed for a nticoe.f'
walion in puJenu wi th heparin-induced thromboc:ytoopenia.
IU: loItding d ...... of 0 .4 t:IJIk, (up 10 44 mg) rv, followed by «)nllnUOlJl; inr.... ion nf
0.16 mifM;Wh r fer 2·10 days. 'llIedoae i.e tilrated to sl.3rgl!t aP'M' rlItio of1.5-2..5. __
''LIW' I lilT .. iall eont.lllnlnt: 60 mi.
/
,---J
warfarin(Coumadin®)
\
/
OIIUQN'O
\
~L_ _-----'''--"
1'0 Int;eo.,rulate 'YI!rajle wejpt pati~nt. rive 10 mt: PO q d.2-4 day., lben . 6..,.q d. Follow ~gu"lion 1OI.ume., ti\t1lte to PT. 1.2·1 _5 ' -cunlrol (or lNR . 2-3) for most
«lndil ion. (••,. OVT •• incle TlA). Hillier PT r.tiOi of 1.5-2 I control (lNR . 3-4) may be
IIHded fot m:unenl.,.,temk tmbGiirm, lIIethsnieal Wart utves ... (th, recommended
rlln._ for th, Inte .... ation.l Nonn atl i_~ Ra ti o (INR) lte.b.own io T"b/e l · /J~
NB: Warfarin lhould nO! be started
until /I tl\,,,'lp;!utic: PTTb.. been achieved
nbte 1-11 Recommended INR , '"
on he~rin to reduce the risk oC"Coumadin
I\II('l'(IIi • • " Ourin, l he li nt _ 3 da,.. of ......
filrin therspy, I*tiellla .. re I>t.tua lly hmu:
colII!ulable ( _ d i l l ' to rl!<iul.'l.ion of
v;lamin· K dependent anl.icc.oqul.,ion r.otoR protein C .. nd pt"O~ "S). tMrefore,
ODntlnue he.,.rin durint: the lI ..u few da,...
8UPI>I.WI: K'OJ'ed UlbI orl , 2. 2.5, 6, 7.5
lind 10"", TV form: 5ml!ilMal
GENI!:RAL CARE
1.6. H""lIto1"1l'
1.5.2.2.
Coagulopathies
CORRECTION OF COAGULOPArHlES OR REVERSAl. OF ANTICOAGULANTS
For recommended norma! yal"u (or coagulot,on a tudil!!l in IM!lJrO$urKary."" Me 22.
Platelets
S.t J>08' 19 (or 'ndicatior,e alld administration
guide!;ne~ ,
Fres b froze n plasma
To revetH wlllfari n an t itOll/{llIBtion. u lW!- the (ollowillg 91 II sta rtin!: point a nd tt!che<;k PTIP'M' IIft.erwBMS'
wh~1\ pat,ent is 'th&tlI!)eut;C/l Uyanticoagulated· s tart .... ,tn 2-3 unit. ITP rapproximatf!ly 15 mUleg i, usually nlll!ded )
for ~verely pro\o"ged PTIPTT, start with 6 uojts FFP
Prothrilrubin complex cancentra.te
Warfarin indu.~ u.r,jeollgulaeilln may be revt rsed up to ~ Or 5 iimo mono qui.kly
wi th prothrombi" com plex con ... ntTat~ (P CC) (conr.ains COHg raclonl ]1. IX. and X) thon
wit.h FFP". P"tient may become hyperthrombotiewith th is.
,--/
vitamin K (Aquamephyton®)
\~--,-I--::c~"""-,--~.~ro,----:c\
,;--c
To reveTae elevated Pr fr:llJ) l\'ru1arirL give. "'1U ....U8 eo!Joid al lolulion orvitumin K,
(phytonadione. A'IuarTU!phyto~). Dc.sea", 10 o.ng
produc.!- warf,tr:;n r~5isUo n~ for up
to I week . FFP Ill.y be adminls!.I>1'I!d oonc urrently for n,ono .opit\ 'orredion (see obo~).
FOT noeammended levels of PT. see page 22.
Jtx adult : start with 1().-)5 rug 1M; the err"" takes 6-12 hl"lliin abAell«l Qf l ive~ dia·
ease). Repea t d0&8 if needed. 'I'iuo llY1! re~ tot..] dOH needed to reverse theraPj!utlc enti ·
c:oaguler,jon i. 25-35 mg.
rv admini,tration hal been assc>ciated wlm &evete . eaction. (possibly 8nephy lae-tic). including hypotel\ll;on lind eVi!n fataliti" (even wiOl proper precaution.l to diluteand e dmi n;. ter slowly). therefore rv route i. reserved only (0 • • 'tua tloll$ where other
routes are !lOt fell.9ible and the ~riOU5 risk isjustifi\!d , R.l: rv (when lM route not feal;'
ble): 10·20 mg IVat a rate ofinjeetion nollo """,,«I 1 mglmin (e.g. put 10 mg in 50 ml of
D5W and give ove r 30 minuteal.
""'Y
,--/
protamine su lfate
\
/
OflUGlNFO
\.
1 mg revenell apPl'Ol[imlltely 100 U ~ (gi've slowly, not to exceed 50 mg in any
10 min period). Therapy I hould be guided by coagulati on studIes. ~tam,ne can 11180 r eversE! _ 6lJ1i, afLQven ox.
,--/
desmopressi n (DDAVP®)
\
/
DROOIHI'O
\
.
Cau&etl lin inerllase in fsetar lIT coaguleut activity and vo n WiUebrand fact.o. which
help$' OOODgu)ation and platelelaClivity in hemophilia A and in VQll Wi1l~brand·. di&eDfIeTyptIJ (where th e factonl are normal In makeup but low in oonoentration • • but may
c.u.~ thromboo:yloOpc"l1i. i,. ....", Wlll~ brand'a d'.t a.>e Type liD wheT" faclOT$ may be ab·
normlll 0. miMing).
R.o; 0.3 OJg/kg (u8fl 50 ml nfdiluentfor dovl ~ 3 OJg. usot 10 Ill] for :loses> 3 11K) given
over 15·30 minute.o 30 minu\.(,s prior 1.0 a s urSica l procedlJ,te,
ELEVATED PRE-oP PIT
In a palient with no h'i tory ofOOllgulopathy. a $,gnlfiCB otly eJevatc(\ pre-op P'IT,5
eommon]y d ..... to I!ither a foetor deficieney o r to lupus ant,eollgulan~ Worku p:
I. milting study
2. lupus coagulont
If the mixins s tudy cor,..., .... !he el"v8U!d P'l'T, th"'n there- ia probably B factor defi.
ciency. CoNU! t II hemalologi8l.
Lupus anticoagulant: I flh~ test for lupUJ pn t ieuagula n t ;5 ~ilive.lhen tM major
risk to tM pa tient wi th surgery i. o.ol blllEdin" rath~r it i. thromboombolism . ManD!:ement reNlmm~ndBtions:
"
1.5. Hllmlltology
GENERAL CARE
as soon as feasible post-op.SLart patient On heparin (Met page 22 ) or LMW heparin
(_ page 23), e.g. Love nox
2. at the ume time SLart warfarin, and maiotain therapeutic antiooagulation for S·
4 weeks (the risk of DVTIPE is attuaUy highest in the fint few weeks !X'et-op)
3. mobilize ft8 soon as p08.!lible post-op
4. ronalder vena-tava intelTUption filter in patients for whom anticoagulation is
contraindicated
1.
THROMBOEMBOLISM IN NEU ROSURGERV
Deep-veiD Ih ro m ~i 6 (DVT) is of ooncem primarily because of the potential for
material (dot. platelet dumps ... ) to dislodge aod form emboli (i ncluding pulmonary ern·
boli. (PE» which may cause pulmonary infarction, sudden death (from cardinc arrest),
orce rebral infarction(from a 8()o.called paradoxical embolus. which mayoa;ur in tbe pres.
ence ofa pateot forameo ovale. see Cal"diOllfllic brai" ~mbolirm. page 773). The reported
mortality from OVT in the LEs ranges from 9-50%"". OVT limited to the calf has a low
threat « 1%) of embolization. however. these dots later extend into the proximal deep
veins in 3Q..5O% ofca5es", from where emboliutioo may OCCur lin 40·50%). or they may
produce postphlebitic syndrome.
Neurosurgical patients are pa rticularly prone to developiog DVTa (estimated risk:
19-50%) due at least in pa rt to the ..... lative frequency of the following:
1. long operating tillles of some procedures
2. prolonged bed rest
3. paralyzed limbs (e.g. in spinal oord injuries or stroke pa!ienLl)
4. alterations in COlIgUlation status
A. in patients ..... ith brain tumors (_ below) or head injury'"
I . n)'lated to the eondition itself
2. due t<:l releaM orbrain thromboplast ins during brain s urgery
B. increased blood viscosity with concomitant ~sludgi ng"
1. from dehyd ration the rapy sometimes used t<:l reduce ce ..... bral edema
2. from volume 10M following SAH (cerebral salt wasting)
C. use of high -<lose glucocorticoids
Specific "neurological" risk factonl for OV'r and PE indud ....:
I. spinal cord in,jUl"J' \SU page 705)
2 . brain tumor: autopsy prevolenceofOVT ., 28%, ofPE., 8.4%. Incidence using 1261_
fibrinogen" : men in ..'ioms 72%, malignontgliomo 60%. metastasis 20%. Risk may
I>!! reduced by pre·op use of aspi rin"
3, suba rachnoid hemorrhage
4. head trauma
5. stroke: incidence of PE = 1-19.8%. with mortality of25·1{)()%
6. patients undergoing neurosurgical operation
PROPHYLAXIS AGAINST DVT
OptiON includa:
I. general measures
A. passive range of motion
B. ","~u1at.o ~"ptup riat~ pati~" ts as ~'... Iy .... pob.ibl~
2. mechanica l te<:hniques (min imal risk of eomplications):
A. pneumatic compression boots" (PCBs) or oequential compression devices
(SCDs): reducea the incidence of DVT. and probably PEs. 00 not use if
DVT. already pn)'sent. Continue use until pat ient able to walk 3·4 hrs per
d.,
3.
B. TED Stockin~ : (TEOS) ap plies graduated pressure, higher di8tally. As
effective as PCB. No evidence that the benefit is odditive". Care should be
taken to avoid a tourniquet effect At the proximal end
C. electrical stimu lation of calf mu.s<:les
D. rotating beds
anticoagulation B
A. full anticoagulation ;! associated with penoperative complications"
"- TE~ JI' ",g;,,~~ t,..d.",o.rk. "TEO" .\.O nd. f... th"''''boomboli<di . ....
B. for.Olllrl;ndkations ond ton.id."lIionl ofull_gulltion in Dl!ut'OIurge'Y. ___ 21
GENERAL CARE
1.5. Hematology
B. "low-dose" an ti_gutalion" ("mini-dose" heparin): 5000 IU SQ q 8 or 12
!In, .tarting Z hr$ pre-op or on admi..ion 10 i>olpital. Potential for hazardoua helllOJThagt ...[OIin braiD or . pinal canal hll! lilllited ;1.1 "10
C. low molflCU lar weight heplll'in. and heparinoida (He pogr 23), not a homoCt~u. group. Err~cy in ~u"""urFcal prophylaxis has not bHn dete.mined
D. upirin: role in OVT prophylw. illimited becaUIM! ASA illhibl!8 platelet aggregation, and platelet.. play only. minor role in OVT
4. combination of PCB. and "mini...:!..." he~ri n awtinlll on the mornmg of poat-op
day I {with no evident<! oraipificant comp\icatioosJ"
Reeo mm enda tion.
RecomD>eod«l
prophyluia ".rie,
with the risk ofdevel·
oping DVT. a • •Uu.-
Table 1. 12 Rl,k & p. ophylaxl a of OVT In neu rosurgical pa118nl'"
trated in Tobk J·12
-. AJIJoO I « pogr 105
fot det.aig orprophylaxil in cervical . pI.
nal cord injuria.
DIAGNOSIS OF OVT
The clinical di agt>O$i. of OV'l' ill
very unreliable. A patient with tha"d,uie
liJ'lI" of. hot. awol·
leo. nnd \.ende. enlf,
ora poII itlyt Homaou'
. lgn (calfpll;n on dor •
• inexlon ofthe a nkJe)
will hpva. OVT only
2().50% of til." tim .....
00·60% o'f patienLl
with OVT will not
hav" thesa f,ndiop.
Laboratory testa
abOrn.tU. : Ovr.LIMI'_~PC8 _ -,,*_
tion~. TEOS . T"EO \~ _
...)SIad<irIgse.ICH ......
Ir_M"'''l'Ionl\age. SAH _ ~~
_ " . 70510< speciIies '19l''*'!I OVT ~ .. CWWQI SCI
ri".
oontra8t venography: the -gold ILtandard", howeY1l r it is invasive and earri""
ofiod,ne reaction. occasionally produces phlebitis, not readi ly repeated
Doppler ullrasound with B'mode imaging: 95% ",nsitiYe and 99'Jlo _"""ilic fot"
proxi ma l OVT. LesseffectiY<! forealfOvrn. May be used io immobilized orea.sted
LE (unlike IPG). Widely accepted a5 the non·inyasiY1l test of choice (or OVT"
impedance plethysmogra phy ( IPe): 1000 for reduced electrical impedlnc<l! produced by blood now from the calrfoHowing relaxation ora pneumatic lOunIiquet.
Good in detecting proximal DVT, not &elll itive forcal f DVT. A po4itive Itudy in.
dicates OVT tha t should be t reated, a negM;Y1l5tudycan o«urwith non-oeclLllive
OVT or with good 00llate ral5, aod should be repeated OYer a 2 week period
'''I·fibrinogen: radiolabe led fibrinagen il iooorporated into the developinll thram·
bus. Bet te r for calfDVTtban proximal DVT. EKpeol ive, IlIId cnany false poIIitiyes.
Risk ofHIV tralllmiuioo has resulted in with d rawal ofUM
O-dime r (a . pecific fibri n degradation product): high levels are uaociated with
DVT and PEn
TREATMENT OF DVT
I . bed rest. with elevatir:m. of involved 1eg(1)
2 . unleu..,tiroagulation ilcontraindiea ted (_ pog~ 21),ltal1 heparin (as outlined
in AfIlit:oogulaJ.ion On page 21, aim for API'T . U.·2 I oontrol) or fuLed. dOH of
t...MW heparinoidl (e.g. tinuparin (LoFparin®"', or in tha U.S. • nonpari n
U..ovenOlL'®lt~ JIG6f 23}: ~ initiat. warfarin thenpy . Heparin can
be stopped after _ $ days"
3. in pIIotien~ whtLre anticotlfUlation i. oontuindicattd, eon,ider Inferior venl elVo
interruption or piaeement of a filter (e.g. Greenfield filter)
4. in non·paralyzed p"tieo~, Clutiou.ly bertn to ambulate after_ 7· 10 d lYS
"
GENERAL CARE
5. wear anti·embolic stocking on affected LE indefinitely (limb ill always at risk of
T"<!<'urrentOVT)
1.5.3.
Extramedullary hematopoiesis
In chronic anemias (especially thalassemia major, AKA Ox.ley'a anemia), low he·
matocrit "'suit!; in chronic ove r.stimulation of bone mprTOW to produce RSC,. Thi, reo
8u lt.s in systemic bony abnormalities, cardiomyopathy (due to hewochromatosia caused
by increased breakdown of defective RBCsl.
Perti nent to the eNS, !.Mre are three aites wheN! e~trBmedullary hematopoiesis
( EMIl ) can call.'lll findings:
skull : produces "bair-<lo-end" appearance on skull x·ray
vertebral bodiu: may result in epidural cord comp re ssion" (Hf below )
choroid plexus
EPIDURAL CORD COMPRESSION FROM
EMH
The exuberant tissu e is very radiU6ensitive, however, the patient may be somewhat
dependent on the hematopoietic capacity of the tiuue.
Treatment
Sw-gical excisiun followed by radiation therapy has been tlle recommended treatmenL Repeated blood transfusions may help udure EMH and may be """ful po$t-op in·
stead ofRTX except for reft-actory cases" .
Su rgery on these patients is difficult because 0(:
I. lowplateletc:ount
2. poor condition of bone
3. cardiomyopathy: increased anesthetic risk
4. anemia, coupled with the fact that mOllt uftbese plI.tien:" are "iron·toxic" from
multiple previou t transfusions
5. total removal of the maBS is not always possible
1.6.
Pharmacology
1.6.1.
Analgesics
For a discussion of types of pain and pain procedures, H' pagt 376.
GENERAL PRINCIPLES
The key to good pain con!.rol is the early use of adequate levels of effective /Ulalge·
sics. For cancer pain, &eheduled dosing is superior to PRN dosing, aod "rescue" medication ~hould be available". Nonopioid analgesics should be tootinued 85 more pm..nl
medications an d iavasi"e techniques are utili2ed.
ANALGESICS FOR SCM: SPECIFIC TYPES OF PAIN
Visceral or deafferentation pain
May sometime. be effectively treated with tricyclic antidepress/Ults (ou pag~ 33).
Tryptophan may be effective (8# pagt 33).
Carbamuepioe (Tegretol®) may be useful for paroxysmal, lancinating pain.
n:u~ta.8tatic bone d i sease
Steroids, aspirin, or NSAIDa...,.., especiaUy helpful , probably by reduciog prostag·
landin mediated sen9i ti!.lltion of A·delta alld C ftbeno. and therefore may be preferred to
APAP.
Pain !'rom
GENERAL CARE
1.6. Pharmacology
Nonoploid analgesics
1.6.1.1.
ACETAMINOPHEN
'",
,....Iic 1OO>C\Iy '..".,IJ'''''
~wiII'>_l",
101jl'1'lllaY, '...
111_
c ~OOOmo,
_ _ .~ ,
oa:urM .... __ C-MI'IIQ!\ ...-'*_)IrI~,"'S1lt1g l>/l r.....'I. .xl!l'ol&l~'ng
~
""'SO ~·rncIldrlgQt. .
N ONSTEROIDAL ANTI-INFLAM MATORV DRUGS ( NSAIDS)
Tho! anU.i nfl&m",atot)' propertiell orNSAID. i. pri"" .,.;!), d"e to ; nhlMt'on orth~ ~n·
...,. ..... eycl_y,ftlHe (COX) .. hlch part,cipalell;" the !lyntheslll of pl'OIIl.I,!.nduul ond
thromoolu. nu'" .
Chal1lc~ri.tic:5
of nonwlective ""'ISUlroid al anti·;nnalJto'latory drug>::
.n a~ """n 0 . .11)' eao;ep4. Mtorol • ., t rornethDmine ('I'oradolol!l . (Ut below )
no dependence develofUI
addiliveeffKt imprOY'fllhe ptlin reHfJwith opioid anal,esies
NSAlo.land APAP) deruonnf1lte a "",mD, ened : a maximulIl dOlt! aboy" whlt h
no fU rthe r llIIaJaaiio ilobta.lned. Foraspirin and APAP, Ihi, lor " l ua lly bf:l;'ween
650-J300 me, and ia ofLen higher ror oUt... NS Al08 whkh m.~ alllO IUIYe a longer
d"f1Ition 0( ""lion
ri>; k or Gl "PMI;& ..,mlllOlI . 1I>Ore .."rioua rho of hel"'totox.idty"", or GI ulcer·
al iOll. hemotTbaee , 0 ' ;:>erlo .... tion Irt! I/!!!$ """mmon
lIking medication with mu la Or I nl.lcicb hal not been pI'1l'«'A effective in reduo-IniGi sideeffKW. ~ti~p fO$toI ICytotd). a pl'OIItagiandin, maybe "ff'« tiye in
mitipling NSAlD·U\d.lUd pamc el'Ollioo or peptic ulm I'. Colltl'l'nrlical.ed in
p. ......cy. Rx 200 Ili PO QID willi food as lone ... patient Is on NSAlDlI. Ifnol
tolenled. w;e 100 1-'( • • CAUTION; an .bwtjrjlCl~nL Should not be ,""en tCl preg.
nant womt n or women Clf clli ldbearing polen till
most l'ev",..ibly inhibit pI.telet runction and Pro1onl bl\'lO'd;nll tim .. (nonaceil}'llted .alkylal.ea hIve Ies& antiplat.elet action, e.l . • al ..late, trililli~l.te , n.b"lIIet.onle) ...... pirin. unlike all nthll' NSAlDS, irrflvtClibly bincb to c~IOOXYleniH and
thUll inhim .. platelel ruocUon for the &·10 day lire oflhe platelel
an c...... MkliuOl and .... leI' ~ntion and ca ny ~ rloI k ofNSAl D.lnd u«<i
nephrtltolrieity"' (raial JMul"fWie~, intelll titia l nt phri lb. M phrotk tynd rotM.
hyperkalemia)
Table
"
l ·a No nl1e rold .1
1.6. Pbarma..,logy
Tab'- 1-14 NOII.le.oldal
_
. . . . , _ " .... \I"'Mo ...
,
t
"'..-.aIIe$I IftK\i.. __
Sfl. _ .. _;EfI •• <lerCleo ._
: OOC.d'UQ~cI-Oce
..IW\!I: MS...-.. I'/ItoLlheotp IrI ~"Ir_ borI. mela_
ibo'Pr"..",os ...
r~ l00""'llml: dOSll IOl-'''''IT'O$!O 12~-sIII
~OS ~
loS-l0
110<;lii0i
,,~ :
-w."._
~WI\i\. ~
III 040~, (I>aI FDA _ _
~-,s.,..,.."....)
~
....... ""'"INSAIOs. _ _ _ _
ror_...
~
III pouIbI.
..-._piIo~luflCl.oCt'l
ketvrolae tromelhamine
(Toradol®)
n .. only p" ....te,..' NSAl.D appnw!td for ua in pain cont:ol ;n UI~ U.S. Anar-ic
.11'«1 iI mon! potent !.hili anll-Inflammatory .1T1ICt. lIal(·li r".6 hu. May be uurul to
control p&ln In the following . ituationa;
1. wh~1"f the avaidance afHdlltian ar I"flPlfll\.aly depTIIMion ir; critieal
2. when conlupatl(JolI unnot be tola..1.ed
3. for patienu who are ,",uaeated by nlrcotiCi
4. wher" narcotic depeadene," alWlnoul co~m
5. when epidunl rnorphin. has bNn u...:! Ind furthr anallft;" i. n~ed without
ril lt of rupi ..wry dl!pn!ilSion (Igofllet tn>e nll'ODtiQlllnl ooovailldiCited)
6. Clu t (onr.
A. no~ indicated for \1M" 72 hn; (complication. haYI been r~ported primarily
with pn)lonSed uw olthe onll (onn )
S . u.... wi th aoution in posl oprl"ltivi .. tienlll.",ce (I' with II'I(M:t NSAlo. )
bl~inc lime ia prolonled by platellt function inhibI tion (rialt orGi or ap.'te helQUlThl~ il.mall, but -. lMf"IIaHd in palllnlt > 75,.... 01(1, wMn
used .. 5 daye, end when used in high", do6et"'l
C. t'Vfl1 thou,h 1M dOlllnl n rCW\lYlnU ~ 01 Iyuem.I'llnI: mlKOll.l,rT;ta_
IIOn.net ef'Olrionl mil)' 0«11. N with all NSAIo./DYOld uR wilh PUDl
D .. with ell NSAlo., \1M WIth c.ulloo In pltI~n" .l,," rorrtnal.idll"fr~
Rx Parentl!ral: For anal" dOlll!lIdminJlttalion: 30 ma rv Dr60 maiM In healthy .dull.
For multi"l. cIooIill(: 30 me rv o.r 1M q 6 h!1l PRN, Masimurn donge.: 120 mgldllY.
GF..NERALCARE
1.6. PhinnaoolOC)'
z<)
For patient wright < 50 kg. age > 65}'n. or reduced rena l function (ereatin lnedear.
anea < 50 mVlnin). aU ortheabove dosag:es are halved emu daily dose; 60 mg).
Pa .... nt..ral UBe ~hould not""Cf!1l/I 5 daY" (3 dllyB may be a beUer guideline).
It% PO: lndica t.ed only ... II continuation or IV or JM lhaJ:llPY. not rOf routine USIIaa an
NSAJD. Swll.l:blng (rom 1M to po, Rtart. with 10 mg PO Cl 4-6 hr~ (combined PO and 1M
do~ $hould be" 120 nlg on tM day ort"'Mltion). SIIPI'IftII: 10 mg table~ .
1.6.1 .2.
Oplold analgesics
Narcotics are m09tc:(]mmonly llSo!d ror moderate to !levI'.... acute pain Or Cancer paIn
(sorne ""pert.s cha racteri ze canoer pain Il!I recu/Tt'nt acute pain nnd not dlronic pain ).
CharacU!rist ics or nan:otkr.
no ce iling e fte(l t {1I«{}Q{ft 281: i.e. iMreasing dlI,~g" illc rea&e!i the eife-cti"e,uSI
(although with welk opioid. [or moderate p!lin, aideeffecta INY wuil d05llgel to
ralatively (ow level,")
with .bronic use, l<llenuJee d~elop!l \ phyaical and pay<:hologiral )
overdm.e po$I!!ble, wi t h the. pOteRtI.1 for respiratory depresllion with all. and fiej·
"lU1N with som@. (u~ pGNII151)
MILO TO MOD ERATE PAIN
Some useful medIcations an!
~own
in Table /· J5.
Table 1-15 Weak oploicls lot mild 10 mod' falll pair!
CALITlON· ~n. can CilUW dio"l/OfOUS .... ""~ 01 CArba .......OI>I"._
Codeine and ill! OQng\ln~~, p!"QpOlQ'phl!1le aod pIIntllzO(:in~, are usuBlly no IIIDre ~r·
recliv~ thalASA Or APAP and are usually Olmbined with these dl""llp.
,--/
I.
tramadol (Ultfam®)
\
/
OfItIG I/¥o
\
1
All oral oploid agonist thatblnd$ to I'-opioio;l recapton, and is alMa centrally uting
"".. I&,,~ietbot inhihil.8"'''pt.ak""rl)o"<'pi''''phrin""no;l """,<onin. FOF 0.<01.<> poi;', 100 mil
comparable to codeine 60 mg with ASA or APA.P""·"'. Th~..., hO$ be~ n nn report or .......
pi ratory depres,ion whell oral dosing reoommendations are followed. Seilurea '/.Ild opio·
iel·like dependelWt! have been reported"
Rx 50 to 100 IDg PO q ~ ·6 1m; PRN pain up to II maximum of ~ OO mg/day (ar 300
mgfd roroJder PlI\ientl) ~OT moderately 8e,·~re acute pain, Oil initi.1 dose of l OO mg fol.
lowed by 50 JOg d06es may suffiCf!. S<lPI'LIED: ,;0 mg tabo!.
1.6. P hlltmllcology
GENERAL CARE
MODERATE TO SEVERE PAIN
,.
, ,,
nel '" &i<Gftd <0000 ~ 01 ~amor.opl>enl2~ hI'S I.... (001""'.'" r _ H3..,
\Or "$00 ..,ly In oploicl·l<lIe-..,l poII"en,.
~
2fII
SEVERE PAIN
Table 1-17 ~ doses lor SEVERE pain, AGONIST oplold.
(pa renleral roule I, rflerenced 10 10 mg 1M morphine)
Ta b la
t
!M:I'O poIency ,a;oo ,'" ~ Is "B 10< $I'lllilt _ " . but tiIar'9H 10 1:2-3 wf~ ctvDnCdoslnsI
~ _ ' " 1Ong' !M>lU$oI "1lQI '~
mtpIPI"KIiM is mtrI.ool.M<110 "0..,''''PII'oII.....
a . limul.nr.,.;th . I ~20 hour ~ .r.~,,,, . !11101 may accumulatt """ o.use agi"'!ion "'aiM< C~S t>yp.'1IC1iYIIv
(IrcIucIIng "",,",Ulll _ _ U'K), ....... '...., ".."iJeOi _given
nl~<l1IIg5 ~
""'I' OIl"" """"" se_era ,~"Ihy 8M dNl/O
given .. \II ~
"'" 10 /<>nIl nail· Nit. '''IlHled ~ can "'~ 10 .a:umultrionlll<l eNS <l8p'8""" (muSl rad<JDe 00..
• ~tor _ 3 days. ""on IhouCIh "'. anJI9ftIc hall·'r, _l'Ot I;I'ItI¥), osr:tedally In .,.. IIIde<Jo,o 01 ~II"'"
!)alieni. u.. _
De "",iled 10 ~ ....", ...1>tfItr<;e using _
drugs
_
""""'i....
w"""
t
INIY ""1M pta<;licIIJ 1<>, Il$e '" U!iIm ~II\ sinoD I T)'IO!OIl <.01'1 ....... only 5 mg ,,",{COCIOM I'''' ac.14mlrIOI)I\en llmlra 1M M<~).
UN OxyCotoIlrill'''' nlOner <lOI.II5 or O>yOOllc>nt
~
• s/IoUICIn<M De used Q"""UneP)<t ·",,~( r,.o;oI ,esg;l&lOIydepf85$lDn1 ,o.pp!y r 1"'\CI>louppe'
!O<SO. ~_ ~ n N., PAN
rTIlI'
Avinza® (extended release
rnorprune)
\ /
\
Onre daily oral morphine fonnulation ,,~inB 11 s philr\olll oral dru, a tlsorptioD. syswm
ISOoAS) (numerous ammoll to-ruethacryl8w eopolyrner bead$. _ \ mm (Ii • .).
1U: !K>liallll;s titruled baud on pD~ient·. oploid tolerance Hnd d<'gTf!e orpain. Taken
lUI I capsule p.o. q d. Not to be t.a.ken · PRN". Not fot post-op fIlIin . • CAUTION: 1'0 ptevent pot.entially 'aUlI doan of morphine., capBuln Bn! to be swallowed whole. and are not
III be~hewed, ~rushed ordiSS\llved. Howe""., the oontcnUrofthe <:apauJe(the beado) may
be sprinkled on epple-s .. uce for thaw uMule u. 6Wallow the eaP'llllei. but the bend~ an!
not to be ehl'wed ru'(rURhed. liIOC ~ Ou, to tlle potentillly nephn>t<OOc affeet off,,nl8ncacid uaOO in SODAS, the maximum dOlll'of Avin,.., is 1600 mg/d . Doses .. 60 milln!
fnropl nid u.lerant patienUr only_
SuPl'UI<D: 30. 60. 90 "" 12.0 mg ""p"u le!; .
/
,-/
P.iI,lIad one® (extended r elease
hydromorphone )
\
/
ORUO
INFO
~L_ _ _ __
_
\
-->'~
Once daily .,,,tlmded rel ell8e bydromorphanl! HCI (imm"wate reit&S1I fonn" includB
Oileudld®). ~ ... misyntlleticrongener of IllOllIhine Md HCtlVI'. metabolite of bydroo>done,
Risk for abua.e 0. lllco:idental a.·,.,rd01lage by viol8ting capsule Or ccmcII:ren t "" of eleohol.
Recommended only for opiaid tolerant pelienbi who have, failed other therapiea" .
Rx A lJChe~hde 1J dNg. Por oploid loh•• Iln\ patienbi only. ~t.rt with 12_82 mil" PO"
24 hOU ri. Titrate UpWArd by 25-60% incrcmCnL8lvery 2-3 d8Y$ PRN • • Capsulu are not
u. be opened . b~n. chewed, d.is$olvoo 0. c~ed or taken wilh al",bol. Do not use if
SlIve r<! hepat ic in.uAidency.
SIII'PU£o: 12.. Hi, 24 &, 32 mg CIIpfiull!ll.
\.6. I;>hannacolcgy
.."""
Tabl,1-18 Equ!,n. lgu!c dOlle. lor S EVERE pain , AGONIST/ANTAGONIST opIoldl
(relerenced 10 10 mg 1M morphine)
Drug 01l1li: genetic
...
1101,1'1
(!Iroprlel.r)8j
~(Supronexe)
'M
Sl
MIX
'M
"'......
...
(Nubm"f)
"""",
(T'twIr0f;)
demcina(~)
--
"
"POt
'M,
~
,.
'.3
,
....
",.,
""
(."
,
O.S. I
,,.>,.•
...,
10
I~O~
1&0 ($1M 0 SO) 1.S.2
10
.
"'~
..,••.
••
.,."",.,.
!)Ir1iI!J9OAI"
I
1'10 $Igm1l1C1j1101
.....~t
,...,
.. ..... lItfICIdIIte _8w.1'~" pI'lente pIIySIC8lIy rill"",,,..,, on ~
1I'0OI ~ "'''''. ~ oIg<twI ''''''114'''' (St.ocri;O ~ N~lint ..1IrCh ,n.~
c,""
1....., ....01_ (lGf 1M _Jc:cn_onIi' ~,.,.. T'''''".~ I_II'''''''''''
"'S'O"_bPlig/lPO-._ T. - N...,."",ccnI_nol<SAl..... r _ ", -\
-""
1.6,1.3.
Alpha-2 adrenoreceptor agoni8t8
.... lphll·2 ' Iloni,IIo ba"'l IIOIlI'leda tivs and '.lla1Ilwe pr(lperti811 aod dram~tieally ....
du~ thl rilir. o r "'pi nlt.oryde l'l"fiIIlon , nd Uulllmountorna ...... ti~ a nl1ll""j"" r~quim ,
~ Precedex~" (dexmedetomidine) \,~/,--_ _-__-_ _ _\
-,-~
Rr: ulUlIlloadi ng d_ it I mq1q \lVlr 10 ,gjoute., followed by CGlIlinuoul rv infuaion of 0.2·0,7 U1~glhr Utra!ed 1.0 delired effect., nul to ~ 24 houn.
SloE vncTS: cUniell lly aignilicant bradycardill s nd .inUI arnt!It hlsVII ~ in
)'II\Inll. hn llhy "ol un ~ .... ith i~..ed vlllial tone janticholinergics IUch IS atropine
0.2 mg IV or IIlycopymll.~ 0.2 m,r IV mly help/. U. with I:II lIlIon in patienta WIth ad ·
hu rt block.
sllt'....,.....:2 m! "ill. of 100 mq:Iml for IV u""'.
",nee<!
1.6.1.4.
Adjuvant pain medications
Th, following ."ay have efficacy in _hIIncing the.efTecti-.- of opiold llnalglfila.
land thercby may redu{'O!
the reqllitOO dC>H)
1'ric),elle a nl ldepre ..... n~:.~ ~ 376.
'rryptop b"n: an emillOlrid e nd • pl'l'CUrIIOI" ofwrotonm. wly work by illCTUti",
.crolonin !eye I,. ~u'"" high d(l<ellllnd luu bypnolH: ~ffectll , w....,fo.... 1.t..2 gro giv"'n
usually q hi , MIIII gi"c daily MVI U" chron ic trypcophln thel"llP1 depleta: viWoin 8..
ADtlhlelaro!netl: ~,II\.Aminel play I role in oociception . .... ntim-tamine.. wkith ant
,lao I nJUo!ytk 'ntillmBtic, and mildl y hypnotk Int@fTecll"eB. Bnll!ge8i.-or uadj,,·
"lints. HydroxYline (A(oIra41, VisLaril®): fU . tart with rx> mf PO q AM .nd 100 mg PO
q hi. May incre."" up III _ 200 mg dllily.
AnliconvulPnll; tlIroa .... zepine, c!onazepem, plMnyt.c>ill or flbilpttnlin mly he
effKti"e in ncuro{)ltthlc pa in from dinbel;t neuropttthy, lrigemin&l ".U".lgil, pafl. ""' ....
petie nlluNllgil, gl_pharyngeal ne urll!gill , lind neuraJgi". due t.o ne,,'e Injury or intil·
lration with C8nurOO
Phe'lOtblui o u : Inme cause mild reduction in nodoc:a pt;on. Mo .. are t".nqu,lldng
Ind IOliemetie. Best Imo.... n for tbis U~ ia fluphlJluinl! \ Prolwn®). usually given with
• lricyeli~ I ntidepresunt for n~uroPl'thic JNlin, .e.lJiI:JM/;t tl.f ~rop<1lhy, 7nalm~nl On
pap 556. PhenothillZUwa mlly NOdu .... th •• eilurl! thru hold .
CO l'\iOO$le ...... idl: in addition to the reductiou ortoxie efTKu " f .... dill t;on or chemo-
GENERAL CARE
therapy, they may PO~Qlj.~ nUCOl!ean.lgeaics. Ther~.~ .1", a numberllfoonspeci6c
benefici,l t lTIM:tI· men,8M appetile. Hme "r w,-II belnl. IInt;e,lIetie. Sid" I!fT<ICl3 ms)'
limit useruineM (aH Pou(bI"deletuiolU aWl tffn:1I of".r'OIds, pave lIl).
Catfeln.: althourh It
no intrinsic anwge$ic pl"Openie., dl>Sl:a 0(65.200
IDreo.l!'r>ee
."alp.ie ,ir.." of APAP, ASAoribuprofen in HlA., Ofllliutpry pIIill.nd
post.-partWll pIIm.
u..
1.6.2.
po-.._.
Antispasmodics/muscle relaxants
0 ...1tf'nlI"llUy·aclinll mUlti/! n!laxan18 have. Md/lting ,-Ifed. On the c:ent.raJ net'V\lU5
a),litem, a nd lben> I. little e>'ideuce of any othu beneficial f'fTO':(t. Elfa:acy ofu5e in~­
tienta WIth Mut@lowblockproblema r. dubioUl'" (uo: /XlIl!l291). Only d<)118 are h.r;~ btlow Be: f,mili.r wilt! appf'(lyed indication. nnd precautlonJI
~
cydobenzaprine (FleJleri1®)
\~.....I./~:-:-_
~;-~
___\...>..~
R.r Adult : 10 mil POTIO-QID. IIlu.n, 11011.0 uc:et!d 2·3
wtoI!ka.
\ /
\
~
RobllJtisal®: i8 a combination ofmRthoearbamol400 ITIi: ... /.SA 315 mg.
methocarbomol (Robaxin®)
Rz Adulloral dose: inilial dose. with 500 lI.g tab.: 3 tabs PO QID 11 48-72 htl,.nd
thell 2 tabli PO QID. With 150 mg t.atNI: 2 tab. PO QlD 11 48-12 htl, alld Iheo 1 tab PO q
~ h ... Or 2 tabs PO TID. With Robax.iul$: for RYe", 'IlUmlpai n 'ta rt at 3 tab. QID If
pll.t;enL eIIn tolerate Ihe ASA, tlHm drop down to mlin~nanee dOH of2 labs QlD
& Adult IV mer.hocarbarnol: 750 mil: IVPB Q 6-3 hrl ror _ r e 'p.II51JU_
SUI'I"lJ.EII: IT\ied.8ble 1 ,ill 10 mI . 0 ..1: 500 mil: tablet . Robnin$-150baI1SOm, methoeal'bamol .
chlorzoxazone
iPara.(on Forte®DSC)
\ /
\
Due to riak ofoeriou. "rwI p<'I5I;ibly fatal bepetoloricity and quutionabll e"ecti .....
neu lUI a muscle Alluanl., tb""" Is little indication to uM thia dnJ'"
~
diazepam (Valium®)
\
/
DRUOI'IFO
\
l
R.t: Adult dOSll for muide lp&SlNI: 2-10 mg PO TID-QID. AIaa •• pog.. 368 r"r mo",
lnrOI'lllBtlon and ror use In ~j':lalltidty_
~
carisoprodol (Soma®)
\
I
DIMlIHfO
\
\
Caution ' IlOl. a true mU1IC1e ~"lIt \ more of a sedative). M8J' pnldu~ euphoria wilh
,""ulltng potenlial lOr abuM.
& Adull.. 350 rug PO TID arwl q ....
~
quinineiulfate
\
/
~-o
\,
For "oi,hr crampl-. Over 10J0 of people> 65 yrs old uperience noc:tUn;laI crtlmpl at
-orne time IUluaU,. In 1M l~, _I~;n the han(II,. No weU-cnnlrolltd lrial' todoelI"",nl efl"ertivlllllM_Mda -aMl,ysl. luggesltd Ihlt lhe frequency ofCfDmp5 C~II be ~
duUld by ~ 2MI. _ r 2 weeks of trealnltlnl, and by InOT1! ",,"r' w ...1u. bu~ Ih"re WM 110
challie in ....enty o:r dunoo ...... Avoid in pr~n~ (aborti facien t). CaUlion: even low
dose can cau.. 'I'TP In stn,itive palienta_ re~nted doae&call cau5ecinchoism (watch for
tinnilus. HfA. NN, hearillj' Iou)-_Rulf:-out uremk neuropnth,. bero~ trl!(ltinl't-po,gt'
"",.
R..r Ad"l1 200 o:r:roo ..... PO 'I lis f'RN (better ..tficac;r seen wit .. n!t(Uhlr lI"";nl).
1.6. PhannacolocY
GENERAL CARE
1.6.3.
Benzodiazepines
Alto!1!e &dilfiliU & paralyticl, page 36. All are elre-c:tive for \.reating aru<i~ly lind
inllOrnni ll, and \'ary onl,. in phlLrnlll«lkinHice or lIite Gfmetabali.m. Those with ",harter
du:ration ofaction are ItS!! likely to 5ed/lI.e, but are 1tIGl'f! prone to tIIU!le rebound depru.ion "" withdrawl ayndrome (may include taehycllrdia, HTN. tremulouanes!l , dillpho.re.is, dY"phonll , confusion, mll""]" twitching, /loll $e;1urea) upon ~Iln"alion , TbDA<!
with hmg duration of action On! mGre likely to teIIult in cumul~tive sed ation. and Impair-
ment.of paychnmotor aDd iDtelleduw function". Lower doae8 are used for
~derly
pa-
tients. May be ",vel1!led with nUlYIIUeniJ (Ii'!! IH>/ow l.
SmK~' v.. ntilatory dep..-ioo anti hypowo,s.ion u"cer1l.t&d by opioids, w,,'ee
in palien"" with COPD. AlI contraindicetad in fin! trirn""ter orpre~lIn<y h:auseoongen.
ital malfomoation')",
1-19
oxazepam (Ser.tX®)
\ I
Thought not \.0 be metabolized in liver.
Ib: Adult: 10-15 mJ PO TJD·QID (increllse, to SO
IIr severe anxiety l.
,-/
alprazolam (Xanax®)
\
IIIgTl~ro
fnr EtOH withduwl
\~c:"-/_-.,.-~'_~
-""'
-c:--\
-"-'
May hav" antidepressant eff~ ijimilar to tri~y<:Ii <:6, with ,l1li", rapid Oll8l!t .
Rx Adul t: nart ItO.25·0.5 mg PO TID. tittato! to mllll'of4 mglday dividoo; come.! in
0.25,0.6 & I mg tabs.
,-/
..
midazr,lam (Versed®)
\
I
OfIUG INPO
\
3 to 4 timet 113 potent lIa dla:repam (VaJiumGll). DiQolves in a qut!<lua solution,
\
thu~
11'&8 burning IUld phle bi t is tho d,iaupam. M physiologic pH. i~ lipid soluble and readily
~roeel
BBB. Gl'1!lItat amnes tic elT'ed. thlUl diuepBm, Excotllent anticonvulsant proper·
liea. Given 1M. on!l-et ooeul'll 8t Hi min, peak at SO miD, duratiioo 1·2 hrs"" .
for e oollCiou8 ileda li!> D WQJ!t lVP): 1·2 mgoyO!r2 min (do not uteed 2. 6 rog with
init.i.al doore), wait 2-3 mimi, IlOd repeat up to total ofO.l-U.16 mg/kg. Reduce by a t
lellst 2~ if opiaid,8re 11&0 being u.;ed or in patient.s ,. 60 yrs. To mai ntain seda·
lion , "'peal dOBl' a of25$ ofinitia] . Clilltion: mida ... br.m has been associftted wilh
rtspiratory arTen (even in young ppt.ient.d. Monitor palientwntinll0U51y, II&(' e.·
Il"a caution in eJder ly
!!. ror 1M p .... o p : O.07.0.(N! n,gIkg (6 mgf70 kg) about 1 h. p",""op.
3. ror ind uction for geneul anesthesia:
A.. initial dose (.slow lVP) of:
I. for u"premedkllt.ed average adul~ age. '" 55 ynI : 0.25 mw'\<g
2. > 55 yfll, ASA Oltt'"S I or II: 0.2 nw'kg
I.
GENERAl- CARE
1.6. Pharmacology
JS
3.
ASAlI l orTV~ O.J5 n'f'9
B. t.o m.inLaIn: "'peM 25'" ormi t;.) delft.
Miduol.m dnp:
DilllkW mg llIiduol.m In lOOct: IV fluId (only ilLui boltJ'N<'OllIllIended,'5 plnt.ic
.deo r~ midB.lOlam); Itart lI.l 1-2 mg/hr .nd tilrHta 1..0 desired level orled.tion.
BENZOOIAZEPINE REVERSAL
J
flumuenil
( R Ofl\UicQllil))
I
\
DRUB"*<>
\
CtImpetl tively inhibilll b.1l,odiuepi nu (OOZ) lit , _p1..ot lita. Sinw dllntlon'or
IIcllon i. shorter thn mo.! BD?,,". reeeillltion 1lI8)' o«ur. elpeci.lly "'ltll hlT", dOlift of
B07.& glv.n OVl!r , Ions: \)r·OC!tdllni. BOZ,nLaton;,,,, ~I < 2 mi ni Il\fr TV dOlI!, pub
in 6_10 mini. end IA~lIl . /lO mini. l)o!dlOtioll i. only parti ally re,.. nad ;0 80m. palienl.l.
Rev6ran l of BDZ illdu""d t.pi'lIU,ry deprHll ion if partial or oil".
Con traindicated In pDtienu ~htonka lly Irul.ed with B07... (ro' II!JZllrI!II Or fGrothe.
indicational whAt . a ntagoni sm ma.)' prO)Voh. withd rawal Iyndrome and/or Hi~ u"".
May Pl'1WOlr6 a panic lIu.ack. Not approvlld. fDr liN in pregnlllt)'.
&To ...... eral! BD7.... u... d rOt(:On.cloUf~ation Oflalleral arlNtMlia' O,2 ma(2 ml)
over 15 SOK:Qnd l: rep!!& t at I minu~ intenal, ifle.1I1 of , evonal ia inadAq"ate up u,a
maximum or I mg (total of 5 dOllU). Ir relNid.tion occurs, I'll'), re~t doMinf at 20 minute
iotervds, keeping withlll a m"" lmllm or3 rug per hour. For .tUlpeded ovlP'doeap. civa
0.2 mil ovCT 30 sea, w.lt 30 &ea. lhan give 0.3 meover 30 lea al I minute itlU!rvall up
to 3 mg Or I,lJ\til ""lien t aroUlli!"
rv
1.6.4.
Sedatives & paralytics
The modi fied RamlJ./l)' ;oOOlItion !IC.!II~"';'
.howll in T",bk 1·20. This is u.seful e.g. for
QU llntitating th edl!liil1!d level ohed8tion .. hell
pll!scrihlng ~ativl!Ii for an I16itated patien!..
1,6.4.1.
··
·
Table 1-20 Modified R.mll~ sed ...
lion KIlt.
,.....
.... ,,
Conscious sedation
IWWous 'flO ~ 01 reess
_.....
oooperaIioe. orienled and ~
3 I8SJlOIlIIs 10 CDn'lIIl;II'd$ onIr
FIeIponM 10 I/gbI g11lMl11ullp Of 10lI0 IUCII-
miduolam (VIlt1'M'd®): M' ~ 35
pMtoba rbiu l (NembuI.llJe): a ba.n,itu.
raU!. 1U fgr 70 Jq adu.t; 100 me.dow
"" ......
•
,
......
.....
<VI'
tII!si< 1\!$9OftM.'
chloral hydraie-; ledation dOle to 25
mglkg (_ bflow)
1.6.4.2.
....
•
N .......
Sedatives for procedures
thiopenta1 (Pent.ot.ha}®)
\ I
\
A Ihort Ictinll ba . hi l un!L III d08l C8"1IU um:oDKiOtUlneu in 20-30 _(circulation time), de pt h InCTell.. lip to 40 &ea, du ration. 5 min. (terminated h)' rtdi'triblltion), _iOUf,nea return. O'tIH 20-30 min• .
8mI: DTIICT$I dOl' ....,1.1ed rupirau,1)' depre ..lIIO, !rTit.t>on il ... tran-.ated , intra_
.rterial ln~tioo ~ n~tOti., . git.ation itin,ieeted . Iowl)" lin IIntj.n. !gnic mJOC'/lrd ial deprUlll nl., hypotelWon in hypovolemic patlen"..
& Adult.: ini l ie! eonfflltra\.ion ,hollid oot ucae<! U,",
giva50 ml lUt d_ nlOdCraUlI)' rapKl rvP, then iftoleral.td give 100-2(1) m.lVPo .... r
20-30 IeCI \500 Ill( m.), be required in I.rp !'fItl .. nt).
J
methube.xital (Brevital'l»
\
/
CRUGINRl
Mort! potent and ahorU r lICtinr th.n th,oplinul l u."rule.r. for
1.6. Ph.rmacology
\
pI!~u"neou,
,
rhllO-
GENERAL CARE
where pellen! need. t.o be .edlted IUId I w&.ll.ent<irepeatejly). Last& 50· 7 mill. Similar CIIllliona "'ith thlld ded probl.m that meLhohuital may i.n!I.Y&lta~zlll'fl
IU Adult.: I sm':\soluti.on (add 60 ml diluent 1.0 WO mgto ,wId 10 mgl'mlJ. 2 ml tut
do. , then 6-12 lOl TYP at rata of 1 mll5~. then 2 W 4 m] q 4-7 mIn PRN .
1.011\)'
/
fentanyl (Sllblimaze®)
~
\
/
OfOUGIIlFO
\
-----L-_ _----''--"
N.rcotic, pOtency ~ 100 . mo~ine. ]n . mall dos~l. [alta 20·30 min. Unlike mor·
phonland meperidinl, doe. not Cftuae hi ltllmine «,Ieul. Low .. ra ICP. Sma D'nIC:J'H, dos~
d'pI'nde nt r IJpiratol)' d~prn"ion, IlIrp dOl" givfln rapidly may c:ause chelt ",.U rigid.
ity.
Rx Adult; 26·100 III (0.5·2
]VP, rlo'pe8t q 1-2 hra PRN. SIJl'~L.IJ!D; 50 IIgf.rnl, re·
'1uin!1 refrigtraUon.
mn
,--I
proporo\ (Diprivan®)
\
I
ORlI(;INFO
\
1
A 'feb.live hypnotic. A1~ ueeflll in high doses during "neury.m IU'll~1")' a. a neW'Oprotectant /tet p~ 808). Protectlon leem' to be leas than wiUl barblturateto.
IUt ror sedpl.JoQ : "'lIrt at Ij-IO I'g/k,gIQ:lin. loCI'1'IIM by 5-10 Hf'k.iImiD II 5·10 minULl!S
PRN d8sire<! seda tion ( ~p to a IOU 0(500 Wli'kgfmin ),
9t'1'rl.n;:0: 500 mg IUlpended [n 11 60 m1 boUleorfal emulsion. The bottle and tubing
II'IU8t be chlll\ged every 12 hOllI'll Sinte it ronLlirll nO baC1.eriolltatle IgenL
~
haloperidol (Haldol®)
\
I
0l'II.I0'*<1
\
1
SmJ: trn:crt rare neuroleptic ItlllilMnt Irndrome. a Contralndiall.ed [n Pl tkinlon', diseu&. An~imolinereic ",recta ml)' ..x_rbata uri ... !), ~lention.
Rz For "ra pid ~f!quenc .. U1Inqui!izal;on" (to Rdata "aile!) agiUlted p.olimt): 5-10
mg ha]operidol]M q 150 minutes until p.tientcontrolled.
PED1ATlllC SEDATION
The following agenla may be u8ed to sed8te pa1.tenl.• (or prut:edu~1 (e,g.
cr or MRlI.
Ahoy .. 1 ,.,at, anyoflheM mly be "sed. Forchildren < 1 rur 11>'. .... chloral hydrnteat
50 rog!kg C.- Niow).
pentobarbital (Nembutlll®~ 2 mg/'ka' IV II ~ hnlPRN
OR
OR
fentanyl (Sublimawe): 1 NIka: IVP
di,upam (V.liuum). 0.1-0.50 mglltg« not to ..xefti 10 mg) lit miduolam (V.r-.tIIl
0.1 mdkglVP
\ !
chlo:-al hydrate
\
Ilk... 30-60 minllLl!S all.er
SL'PPUm: . utpenlllGli 100
IIIlVml (_ 500 ~ till
wh~h
ilMlOmw'eatpoonJ
or 500 mg
oral
dOle to
c.~uJ"
WCN"t
"Dpr (DEMEROt., PHENERGAN
& THOI'V4ZJNE)
~ii~~~~;;~'~'~
!!'b!'!""!'!'
AKA -lytic r;Odt.lail" Corabine in
1 . ynnp.nd rive at deolp]M ;11-
.iac:tion:
•
...
IIW!peridine (Denu!rote): 2 mlVkf (mu: don 60 mg)
pl'OlIlethnina (PhenerganCl): 1 mgllo;g (a COnl rll;lId;clltad;n patient.! < 2 yn age)
chlOll'I'OIDI,iI\e rJ'hGradnt«l): J mN
GENEItU CARE
1.6. PhnnnlleolollY
"
1.6.4.3.
Paralytics (neuromuscular blocking agents)
CAU'J'ION: "'quirt's venc.ilatiDn (intubation or AmbtJ-bAglmnskl. Reminder: pH ... Iywd potienl.ll may still be~DnsciQIIII.lUld thereforellb!~ to !eel pll.in, th ,imultllneQua use.
of8edaliou i, !huJI required fD' cou$ciaus pMienu.
Early routine uae in head·injured patienulowens ICP (e.l . f.am lI.uctioning' O') and
mon...lity. but doe!> not improve ovenilU outcome'" .
Neuromuscular blQcking alente (NMBAa) Ille ch:ll<liified clini~ly by time tQ anaet
aodduration ofparlllyaislllOlbown in Tabl, 6·22. AdditiollllJ ioformlltioo for sorueagenb
follow! tbO! table along with $OlOe mru;ider1!tions for neuro.urgjcal patienu.
Table 6-22 On$&\ and dUr,llion of mUlcle relu8nla
ULTRA-S HORT ACTING PARALYTICS
.-I
succinylcholine (Anectine®)
\
I
0f:W'31N.FO
\
,
The anly depohl.ri~ing ganglionie blocker (the restate competitive blocke",). Rapidly
by pillsma pseudoc:hoLine6t.erllsel. A .ingle d.me produces fll5CiculaLions th~n
paraly$i.s. On..«et: 1 min. Duratian of adion: 5-10 min .
InIl~tiYIl1.ed
Indi cationll
Due Ul l ignificant side effecta (.Jet! tN!iDw), use is now IIrnlt<!d primarily t.o tbe following indlclltioo.ll. Adults: g>!nelllUy ~llU!Iended Dnly rDr emergency intubatia"" where
the airwaY;8 notCDnlrolled _lD child ren : Dl1.ly wben in tubaLion il Deeded with a fulluo"' _
aOO , o~ iflar:yngt>!lpa.m "",,1m! during IIttempted intubatiDn uRing othe~ IIgents.
S id e effeds
• CAUTIONS: usually increases serum K' by 0.5 mE:Qfl. (on rBre Decaf;on CBUses
"",veee bype rkalemia (!K·I up 10 12 m&yl.) in patient8 with nel,U'l)nal D~ mu..:ular pathol.
ogy. uu~ing tllTdiac compHt~UDru; which cannot 1Jo:o. blocked ). Lherefcre contraindiuted
in IlCUt.e phS$!! of iDjury fDllDwing major bUm6, multiple trauma Dr nt.e1Uive denervatioo
of.keletlll mUl!<:le or uppe' motor nwron if\iury . 00 noL use for routine inlubation~ in
adolescenlA and children (may couse tlirdillC IIrrest even In "pparen~ly healthy YDUngIt.e~ many Dfwhom h8ve undiagn<llled myDPllthi~). Linked t.o lIlaHg:lant hyperth~ rmia.
MAy cau.e dysrhythmia.. Kpt!cially ainu~ bradycardia (INO L with atropine). May
get autoDDm;c stimulation from ACh-like aCLion - HTN, and brady- Dr tachyCllld;a (e.._
pecially In pedl with repellt.ed dal es). The fasciculation! may ,n(felne Ie?, intngaatric.
t.6 . PhannacolOjp'
GENE:RAL CARE
pre""UTe. lInd inr.rQoeuL8~pre""ure (wnlTaiooitllted in pene~ra ljnge.y& injury. espeaally
to qnterior charober : OK in glaucoma).
Pl'1II'urorization with a .pri.ming do.se" ofa n<JfIdepoJllrlziDg bloeker lusua-lly ~ 10%
0/' the intubating dose, e.g. iUlQCu ronium 0.&·1 mg IV 3-& minutes prior to sucdnylch o>line) in pati~ntll with elevated ICP or increa""d "'traoe... l"r p r ...... ure (to am.-.Uornte further pressure Incru$ru! during failCiwlation ph illie) lind in patientll who have eaten
recently (c:ont.rovenial lO'). Phole II block (.lmi llirto nondcpolpr. zing bloekerl may develop with fillC\l8S; .... dOllIlll nr in patients willi a hoonnal pseudoebn~nl!l!terll88.
Dosing
Hz Adult: 0.6-1.1mglkg (2·3 ,nJ/70 kg) lVP (elT on high aide to allow time for procedure &. to avoi<:,L multi-dosing complica t ions), may repeaL t.his dose II I.
Rx Ped s (CAUTION: tim recommended for rou t ine use, sunbo<.'f!) Cl1i.ldn:n: 1, 1
mgfq. J.nfanY: (0( 1 rnOS); 2 mglkg.
SUWUt:ll; 20 nllVml coneontr&tlon.
~
rapacurooium (Raplon®)
\
/
OA\IG I!<fQ
\,
'fhe ahortalt scting nond epoJ~riJ:ing (coropetiLive) NMBA. DUl1ItiOll of action and
hisl amine re leolN! are both d""" dep!!ndeu L,
Rx Adult: for intubation. 1,[' mglkg.
SHORT ACTING PARAL'r'TlCS
~
mivacllrillm{Mivacron®)
\
I
0I!IIQ1NfO
\
,
Me tDbolillm i$ by pln~m& pSE udn<:holinl!!lter,,"E. indep.mdentofltidM)'W or liver. Po>t ian~ .... ,th pIIeudO)Choline!ltenrse defic,ency may vcperienee prolonged pa ralysilliuting
for h"u ....
Rx Adult~ (or in ~ub.ll t io n. to avoid hypotension. give 0.15 mglkgover!>-16 sees. or
0_20 mglk,g over 30 sen. Or 0.15 m&fki: followed 30 t;.Konda later by 0.1 mgIk,g.
~
\ !
roc:u.ronlum (Zemlln')n®)
OIIUOINFO
\
,
(n large dOA ..... ha$ speed of on!<!l that approaches sucriflylcholine. Hnv.·eYer, in
these dOllea, pa ralY$is ueualJy lo~ta _ 1· 2 II .... E~pe!llIive.
Ib: Adu Lt , initial dC08c 0.6 -1 ro""B. May be used os j~Bim of 10- 12 IlWklfruin .
INTERMEOIATE ACTING PARAL'r'TlCS
~
vccuronium {No rc u ron®)
\!
0RUCl1NFO
\
,
Nondepolariting (competit ive) NMRA, Adequatto pnra!Ylis for intubation within
2.5-.3 minut"" of pdmini~Lratlou, About onR third mol'll rtent th an plUlcuroruum •• hotter
dllI'Dti"" o{netion (huts _ 30 rnmutu "fl..>. tailisl dQlJOl . Unlike pe.n""...,,,i,,,,,, vcry I,ul o
vegal (i .~. ClIrdiOY ..scular) err-acta. No CNS .. dive mel.8bolite.s. DOoe'!I not alretl. lCP Or CPP.
Hepatically l1lel.8bol i~ed . Due to active metabolite, . partlly,Ca hn been reported to taM
6 hrs to 7 days to recede following diswnt;nuotiOll of the druB Dfler it 2 dll.)'8 uae in pIItient.s with I'f!nal f~Hllr.-.I". MU8L be mixed to use.
Doaing
BWP .... !(;g: .10 rng freeu-dried enkc. requiring rec,;mst;lution . Uao wit hin 24 h.....
Rx Adul~ahd ch ildren .> 10 yeors age: 0.1 mglkg (fOT llIoe~adults use 8-10 mg as ini_
tial dose). May repeo t q 1 hr PRN . lnfu gion : 1-2I'gfkglmin.
Hz Pedlatril:;!:hiI.dD:.Il ()- IOyrs) requil'll sligh tly higher dose and morefrequenLdOl!lIng than adult. lofllol.l (7 weeki - 1 yr); slightly more ~ensitive Iln a mglkg basi. thaD
adullil. tak"" ~ 1.5 ){ longer to recover. Use in n"'lnet.el and ~ont.inuou~ infu9ion in ch il _
drr.ll i~ in sufficiently studied.
GF.:NF.:RAL CARE
1.6. Phannacology
"
:-./
cisatncunum (NimbeX®)
\
/
DfI\IIlIHO'O
\
,
Nondepolarizing (rompetiti"e) blocker. Thi s illOmu of Btrll{:urium does no~ relelllle
unlike it& plU"eP l C(lmpOuud (lee ~Iow). Providllll about I bour ofparaly~i • •
Also undergoes HofmBM degradatifln. with laudanosine III one nfl1.3 metaboli1.(s.
Rx Adult and children> 12 years age: 0.15 or 0.2 mglkg 113 part of propOfoVnitroui
hi&tamin~
oxideJWi:ygen ioduction-intubdion ~ ique produ~ mU$ele paralyeil adequllte for intubation within 2 or l.~ min n.es, respedively. Infm<ioo: 1.:1 IIg1kglmi n .
Rx Pediatric: ~ (2·12 y rs): 0 .1 mglltg giwn over 5-10 S<!COllda dllMg hnl ",thang II. <>plaid lloeathe6ia.
,----/
atracuriurn (Tracrium®)
\
/
DRUClINF'tI
\
,
Nondepulariling (oompelitive) blocker. After IV bolulIl onBft 2·2..5 min&, ptak 3-5
mills , duration 15.20 mins (i nitial d""" may tB~t up 1.0 30 m;nutllll). Uudl'rg<H!" nonenzy mat ic HofmlUl.ll degradation 100 ealer hydroly$i, at normal ptly~iologic pH and tamperIHure, in~ct;"at;nll too drug iD ~ 30 rrunute$. Therefore \Uif!ful in pat~n\$""' ith li",u Dr
renal fallure. Reven ible with neostigrtlinl!. C~us~s h.isl.amine release which t~1) produce
hypotension (ronliider cil;lltraeurium inst<!lId, I<l'I! abooe!. A mel.llboliw, IAudnoo$ine, is
Muroextltatory. lind a!:<'umulation could theoretically cau$eHlzures (no doxume nted
~lISelI)l".
Do!:ling
SlIPPUUI: S " 10 ml ampule. c.f 10 mg/IDI concentration.
Rx Adult & ~hlldren > 2 yr$ age : 0.4·0.l~ mglkg lVP. ReduCOl ~b~quentdDfieli to 0.02
mg/kg
Rx ~(I month· 2yrs), 0.3·0.4 mglkg.
LONG ACTI NG PAR ALYTICS
,----/
pancunm;um (Pavu\on ®)
\
I
DAl./GItjR)
\
,
"Prototype" nondepolari-QIIij (CQm petitivtl) para lytil'- Puk; 3·5miDII, duration up to
60 mins . Revel'9ible with Bnticholineat.erage$lucil as neos tigmine. Renal elimination.
SlDI:D"1'ECTa1 usefulnel!s a limited because the drug is ~ and IIUl illliiNctlym·
pathOlnimBtic whid> incretlliell cardiac OUtput. pulse rate. and rcp ConsIder "l'curonium
II1S an alt.em ative.($n' aoo ... ).
DOlling
~
Rx ~(h.ild..r:m: 0.04-0.10 mglkg 1VP (lItaTtwith 3 mg}. Reduce suhsequenldos·
to 0.02 mgfkg.
Rx :t:i£::Imawl: espe-cialJy Hnaitive. t<!it dose 0.02 mlVkg-
1.6.5.
St~68
Acid inhIbitors
ulce ra; in oeuro!fllrge .y"
The m~ of st,...ss uicer' (SU);$ high in c,; tically HI patienUi w;~h CNS puthology.
17':lofSU. produ~ dio icallyaignificant hemorrhage. eNS risk r""tan. indude inlmen·
nial patholOgy: brain injury (upeda Uy Gl asgow Coma scale IfCOr e < 9), brain t\lOlO"" in·
tracerebral hemorrhage. SIADH, CNS infection, l~cbemic CVA, 118 ~11 as spinal cord
Injury. The odds a re jncreallf!<l with the coexiIJtem:e of extru-CNS risk r~ct.oTII including:
Iong·term U!ie orste roidll (\1I uaHy > 3 wlI'!lui), bums> 25% of body turfl1<'1! srea, hypoten·
sion. respitlltory failure, coagulopulhietl, renal Or hepatic flIiJure and 8epsis.
eNS palho10f0'. especially that involvin,g the dien~ph .. lon or brtlin stem, ""n low.d
to reduction orvagal outpul ... hich lead!! to hypersecretion ofllaatrie.acid and pepain .
Thm. ia a peak in add a nd pepsIn production 3~ d~ys alter CNS injury.
Propbyhlll is for s treSB ulce r ..,
There illtrong e vidence that reduction OfgasLrit acid {whether by anL9cidfi or
agents thatinhibitacid 8ecretion)reducef the Inciden~ofGJ bleedi"l from . tress ultenl
.1.6 . Pharmacology
GENERAL CARE
critically ill pllt.i"nbl. Elevllting gastric pH ". ".f> 0.1110 inactiyales pl'psin.
Other therapies that don't in~olve alterationa of pH thllt may be elf~tive indllde
ello.ralfa le and enteral notri tion (controver lial),". Titrated antscidl or s lIcralrale IIPpear
La be superior to'}l, antaconiu8 in reducing the inddence ofSL·••
RolltJ.ne prophylllJtia .... hen .leroma are used fs not .... PlTant.ed unle" one of the rol·
lowing r is!< fac:tors I ' e p~nt: prior PUD, tonCUrTen~ use or NSAlOs. lIepot'c or renal
failure, malno urish ment. or prolonged steroid therapy >:1 weeu.
In
1.7.
References
)l OWO J F. fki><h<rll S.SIJ •• ,. f , .. ~ · E>-""",,.
,.
1"'II'I<"""""~I"'d .. ", ........ 0.'<1< ........ ""' ...
·C . ... f<J>O" . N......... ~
~S C.Co\<
~ · 161·l. \'l~ ,
OS. "",.1 P M." oJ ~ fOul "".
rdnI'i«lI<mI, " " ' , " 1 _ " "ldoOl",,",,""'.
,
•
,
_ _ ... """"",,1&1. " ' _ ..... or ,"" •• •
'"'" '" 0<"""-1 io~ 1'1 ............,.., Jl' 74~·g,
IWl.
5hoplM H M 'I...,.,_,.,..I."",.rIo., ... ~I",""
......Jollijpo" ."... ""'. I.......,.bosI •• M" I<I R D.
(..J,) Ch ... ~~ILJ.l'J"""'."'" Yod . ln<l.u"
I9!/>. Vol 1. PI> 1ID-6111.
ricl"", T E........11<0 E H: TIle ............. ~yp<,.
...........)1'Il.-..1II t.1I 1 MooI 3O'I '16-1. I9!J.
ONJ' (Of h}""",~ol .. ~."" ... M<d Loll«
19' UI.. :ZO 11I@1 .
R Il . \lla»eo P If M)"I><ri<"' .....,",....
.if> ,od ..,,- . JAMA J5S I60J.II.1981o.
CoIueIII E..... <I K, "I'\onoloof lt . "01.: 1CP''''''jQ
ilhill·
"Kro~",1 ...... 1"""... 1 J'oI<u""" .. "3. Jl9.JI.
•• ""fl"_
,rdKedb)o"""iu"'' '''_''' ''p";.".. ..
.It. .... booo I. ')~""< 1"",,'~_' _ lImJ
"
"
".
".
"
''''.
~,"'Z.Spi<c<I .... R . f"...u..Q ."~" 001tyt4
"",~ •• """","'clcaIti<~ion f'"", rn>-
•
"
,.
"
D.
"
"
"
n.
".
"
•
"",i<d ..,.u.... ~""'.\,.."'" """,101, ...."",, J ~,".
....... ' 1 l!. 60S- I. 1¥ll9
QrIow.U I p. Sb;. ...J' D. llid, OC." 01., Wb.blol
10.......,,1 bloool PIt .."", .... ,
ran ....."""''' kJ,.
"''1 Col, Con M"" 16 lM--t. J9SII .
Eornolol AU!cn-iI<Ii"J 1\' Dna~ . M, 4l-t1·
;'9:l7·'. 1'II7.
T",,,,l>ie E R. M",,-iu<- J ~ . My... o. I ;5, eo..."~
..... hy .. rll1 ,... . ..... h<IolI ....b on .... ' .........."'01
....... P""" .. J ,. • • """'" a2: ~ 7. 1m.
Knli<lk>lF."'_" II P.r.<."""PL
pol_O<)' .....".· T ............, d o _ i...
.N_~ 19' 169·70. IWI
Bn"~ R L; WI<.\<I<"o ...1r...", &I_~ ,~ ....
py. N EDel J "hd XIS. »? \976s .."" G c .. W;,1lla- S R. WW.", ... I or 1i. _ I.
<oOitI iIoo ..r) .n ""~ ....
S~ ~.. roI
+\' 0l'1Il, 1995
K..... OS, A. oIJQt<do", rot' "...,k...... ,"'" ...;u..
<In ........ FIlm l'II,oJd&n 'J9: ~ .. , 19!9.
MmI"IoIl Lf".KI.,J.L.>o&fu<TW: Tho_Ik.'ion ur
,,,,,,,,",,"rom iIIenp, 1. _ _
JI<>I P'o',l<n<o: A
\Iud, AM J'oI<u,oI I
:101 · J.1917
O'".lbl<t J M. Hall E 0' CUm .. """10"'"'" or
. "''''_. IImold ,,."""" r.. Cl'is ,OJ"or. A,.,.,..
"""""Il'. J N...... . k 62. !06·ID.
\0<
N.,,,,,,,,,.,
J'O'"'.....
",1;11_
"""'\I'"''''
....
,.>oIozl.'"
LuW Y. R....... yOIl.l\oIilljl It,' 1I . ,,~r~ A ...·i o"
tI: " <ell
I""f'h)"ui, I. ,...
iro.......... _."M . N<~ ..... 'II<'<)" 41' .16-1&. I~J.
W.;"e. H L.Reu,AR.C-, PR.SiI_~''''''
10:". p<nor.,..... "'''''''''''TI<W
10; h'liHIow ....... ,,""..., ... ,.......... ~"..,. n .
0().}.1991
.1«,
"'"''''"'I''''''
po!"." ...., •.
'Z,,;o1" M. M..-. C.Il""t<"'oI~O S. • , !JI: Cot>
I' .... ,.!Oi<I 'iI<topy " IO<UIl=d ""'~ lo<hem o<,...,,,,"
GEN£RALCARE
~.
".
•
N.
•
".
".
"
,
"
~
"
M<d 7t. l97.«ll 1'111' .
S"'"Y' .... S................ Mold« HI C)o<Ii<aJ <\III ..
..... ......... _Iouol" ... ''''.. ''''''_"'''''
1<",", ,.
t.lIW<I~ ..... -...
"",I<t." ""'" ....
d""""'""","",,".""' J ,'o1«1'l9:l:J~-.Il. I~.
"I'l,booItot, M, ,wIdl.," ...._
. R,,~t~ .
~i.."y,.•. - ' _ I tTa/",,_ . I" ~ ......... __
..1110l0&I .0.....,... 0 L..-J Sol.... w. t.u.). cOn• ...... 1. ,••••""...,""'. WOliiAnlll_ Wjl~''''
Il.r.lli"""".I992. 0'01.5; PI' 19·.I!l
D!rio"" M.~ PW.DonIC... ",. SoiIr","
__ ..... c .. fIIl .. ioo;,.. pot_ wi'h ~bnl ~I
An:b Noo",1 .0& 921-JO. 1959
......1f ... . : H~ .< ..... I~"" .. """"""'y
....,."1
.""" .... "..,..-.. b<olr,~.r..,.le<.1i"
, ..""" '" '"'"''''~ _
. N [MII J MocI JI~ •
1329·)5. \986
11,-", J C. Kt<>'''>poll! R K. ",!orr" I: Ch."'....
<OftC<1)I, "" ", ..
n"......._
'1""""""'"' _y.
"""..,.",.., Ropil come_ oorj J><KIM< .. I0I0,,,,
", ....... II""'1'"'''Y'"nol)''' ... ", I MocI 7S, I~ \IO'2.I93S
Ft. ... C L.
" I S,..".. ..... ,'" ~,_""".;o:
""'..,. ..... , """ " 1M .... '0 _
)10/',1 ... m),<l1·
~"'S<III ""'. rvl4. "'I~n.19~.
"""",,)10. 11"_,1.1 M..... IIEL:C... 'rolpoo'l1IO
,"ydl""4'.i~ " "',""no
<Ii ..... ""....-
","'fI
""" •• _
._1>«1
.. ...-I~po! ... "
~5oI..:n,I?~ .
,.....' 011'57<111 .. , II '
Ardl
", •• 1 C. K".....,.,liItK .... rieff II I: T_"" .. or
'~i<hY]>Q"'''''''''''''''.' ~ ..... ",11<1 ..
<lo"'"'iO.roEu,I J M<dll7 II!IO.'. I'III
!krl T- T'Uli"1 L~ponou.""., It,'~" il 011 II>< """"
"".t«~ _
1 ..... ' "'"'' M«I 11):011.9. 1~
_If II n lt,,,,,,,,,,,,n>iIo ..1O<'-l"""perm&DIIDI
_<10 ...,... ...... 1-..0 M'" 11· )7j-OO. 19117
t...ur.. .. R. 1C"lI S I: M,.II""',-."
d b)poo.irMII • • Ann I. ..... M"" 176.. SJ-6~.
.n.""".,,,.,.
,m
!UN..... O. R_"" B.lobI_ R•.,ftI ~ /l.apidOOl .
.... ,"" of ~)""",,:n:mk> I. SIAOHI M ."."'..,""
U'U) ...... lOhy_., 001;".. ....... 10..". M<d 1..
'"lO·S . ltlJ
1.<*.601 C. III.I_ P B. :<.woIoc""'I • ...."... ...... •
_
..;.,.......... 1lw. ' 1""_ofl"'fII>'OP"'l<
••,<"";... oI ..<id»nnc._. Nell, ... , • ...,. .:
7:1l-00.1'I31
](<011 M, MoIc').' .li"",,,olm I. Hy_,..."" ..
... <'it Ino" ~I ....... J l nl Mod :131.: 191-1. 1992
H.vripo M ]t; Qn:m.i >01, "'''11' 1 ~ A
",,,,,, ... N<"' ..... l ..,. )8. ISHIO. '996.
O<T"'J«II. o."",,,",! c:C""""""'of ...loI .......
-Il, b)
N EoJ! J 1.1«1 ~J 91"' •
19JI
p.,-•• W It .MoW P.I..,.~LA: 00"",,10<)0.
citr,e ",1"'JIII"'IIri'" .0011.,,,,,_ L....", l
14!4. I976t .. ,,~1.
r-om-oJN .C.... lo-!.Kon'C. .. ."S"p<'fior.,o(
""""'kqoc:li,..,
". _Ito<)oo;l,,,.,,.., II"".,,,
on ill< ,......,.", of
1<- .y"d"""" of "'_Io , ~
or ...
ejl, . .
1.7. References
_,.,ion
"
"
00.
".
0>
".
".
•
...
".
-,
...
".
,id,.moo _
.N E» ~ J Mod l98, 17)·7 . 19J!
0..: •• , G. w. «rIo< Y.Gcr.<u< F. "Ill. Tru,,,,.,"
01 , ...yl"odtom< of i""PI""!'rio'" le<m ... 01.",,,,·
i."" .. """""""" with fu .... mid<. N i:nd J MId
3O<;l:l9·)(I. 19" .
).1. . - 1 c. NeI_ ? S· lIy_l<mb ,n ""... "
",III _Imoodho:""""",,: T_ _ ," ,,,,,,I, •
.,.,;.,... N .~""" ~ , y I : 2ll-6 • •m .
Wijdick> f F M. v""",.1<n M. lI'jdll .... " 1>1_ lIy·
pO<I. lrUIho.nd _
, ",r..,;tioo in pol" .... wj'h
",,".red inln<"""" .....u<)' ......, I. no'" ....
Iwmf.I1 ...... N....... 11; 137...00. I98S.
Wijdd, E F M. V. ....... Io. M.... 11 . ... 1 .... .. <4'
Vol."" d<plo.;"" on<! ""ri.",;, '" ""' ......
"'pout«! i"',"', .. iol • ......-y.... ...... No.",I ),.
111-6.1911' .
N. l<",,? S.S<irS M. M"""" I c ... <4_ Ky·
p"'''' ',,,,,,. i. i,.,.,." ..
• y _ o I i ... ~"' •••" .."""oI ... id ,. ..1I<
_(S'AOKI_ J 1'1""<0>.," ': 9) .... , . 19& 1.
II .... O.Lrodl.oy K W. Wip",h I: F 101, "~I, : Ef·
1«:10In_""' ____ " ... ~ ..........."h_
.....,~ fIOKI .. ~ . S """' ZO: 11'f>-61.19t9.
~ R F. Hotbo. , h R 1:: ... dtn .... ",,,, .... 01 ,n,"·
"reo on<! -..01 "Ii.. lot ,.. "" .. me," 01
byp"n."uni. in ... ""." ..... po1 ic,"", J Ne",.·
" <110, 20 1·6 . t~89 .
V_Ii. I G. ROI:>I""", "'O. M_ ' " 101 , Po."pef..i .....nd p""·<=maI [< di."",.. insip''''''. fron,
H"",, It"" 13: 147·6.1. 1!IaS.
... "" T
K.S_ N...... " Lylllpboc)'l'"
hy pop/1y•• ,,,C... « PO. · N.~, ..... " ..., J6, 10 169. 199' .
1m... H .N..... K.Sh,ma" . .... " 01" Ly"'P ..... ytic
i.I.O(Iiw_"""'ypoph,..'u ... . <.....f 0."",,1
d,Il><,.. i.",""," •. N EnJIJ Mod 319, (1).. 9. I99l.
Millt, M.O., ... "'T. M.......
R«OI.i.
tj.,,-, 01 1""'" <ltr""" ,n ... ,id,. ",'" _
.. , ,,,.
'''''' . ... '''' I., ... M«I 7}' 121·9. 1910.
Fresh·Fro ... 1'(.."" C>,},,*,,,, , po·~< ..... PI ...IeI.
Admini ..... ''''n Practice G<oid<!inc. D<v<lopmeo'
T.. l For« .ftheCon.,. or ... ,....., •• Po,toolo",""
Proro ... _ ' 0 ' f", tl>c ... of tl-c"'·fro,... pl ...
.... <1)••
ond pi..... " . Ji..MA 17,- 7n.
11. 1994.
M_ _ i' M. 0.:.....,..,.;0: ... _'...,.r.... ""
I..... of ,rca""e." r"'","-ital .l1li ""'l.i,.., hit..,·
1.,di_. 8 _ 12,,449.".1918.
SO W. lIug o _ 1I. 1Uc.... ~ 101 T: C<HI"4'iicatioo.
of.".....,..I .. ' ' ......., in PI'''''' ... "h kno"" un' .. , ........... yot<lII ........ C." J 5 •• ,26; lSI·).
1981,
RoffR._, I: ''''' ...... . I111' ......... "r po ...•
m! ,,,,",",,,,,,,, '0 poIi ...... i'" , Iiomo . AM N... •
r<>Ill: ))00·6. 198).
Olin J W.. y """, 1 R.O<aot R ....
Tre>t",..,
of de<p .... i. , _ i , ..... PU"' ''"'>'}' oMboli i.
..,... " ... ir~ pri.....,. ond ........ ,," b<oi" ,.""""
...... ieClO' ....... '" ;"f.<\of ,~ n. co., (<f,et"! A.-dI
......... ~.<d 147: 1177-" .. 1981 .
F~ 101 .... K. Stlk<r ~ G. '" 01.0 Tho nsJr
.....s . m...:y of • • ,icootot.". 'heropy '" the ,te..•
men, of "'rombo<mt>alic <ornplication. ,. ""itnt,
,..i'h pn.....,. moli&o",,' b.. i" fWI><>r> . New ..
.",,...,.l1. J. -7. 19'IO.
S'<nI W E. 1'''''fN'",I.. ...,1.",,,,,,: CM<plk~.
, ...... ,.. I, pr~. '~ P<I ".." ... " ,. r. N... """c>.... "" 1<1") . Y........ J.(.dJ . W. 8.Sounrl<n.
PhHOdclpl.io.1nd <d .• 19S1. VoI.l: PI' 105 1.. 116.
K. wom", T. T....~i" M. K_ O." 01. 101"'&0...., 0( i.' ..... i., _ 1 0 " >o<i...., ... i"' ....
'"",",u"" ''''rtpy 5 • • , 1'1 ... "" ...: 4J8"'J. 199,
N"".".-. for ...... hemopllili. "'...,,120;' . M«I
1.e""'46: 11 .... '2():")C.
Hinh I . 0.1<0 1 E. D< r\:.i. 0." ...: (lraj ""'i<:o>& •.
I.. ,,: M«"'n' .... 01 """0 • . el,.ie.' cffccu .......
,t>eropouti<: 121\&<- C.~ 102 (S"""')'
,io:,_
,..;0,.
i., ..."'....""""I" "'" ,...
v._,
.M.""""""
M.".'.
.,.""1"101<.
".
"
".
".
".
".
".
0>.
".
•
".
00.
0>.
.•
"
"
""..a."Ie,
1.7. References
KIwrwI>I. M .... C . _ M I. M.rOO F... aI" Th<
"""~""., or II"""""",. ,n the ""~ipid·
.. ,it>ody.ynd"""" . N r..... J ~ ))20 99)·1.
I99S.
Ill'<" T ).1 . 11 .11 R O.
I G; "'",~""""l>oI"
,ho:"9)' r.. ,...,.. ~_ic dila><. eI,..,
9S·lJ5-5IS. I9i9.
... ,. ,,,,,,,, 1 L 0.5 .... T M. Kumit, F I . .. oIo lie·
pori • . i_ _ ]'IOjIO. io_"""m_i.
i><h<1Itic """,<. Mo)'<lCu""..,. 6j: lS)-6 ' .I98S.
0.11<11"'" ...... h<t low· molo<.I".""""" ... pori • •
101 ........ '.' )1· 11.1-6. IWS.
Al6epat .. ot><I obtooporo;d r", "",_ion '" <k<p
"",. ,_ , •. M........... )9(10 11): 9'·S.I997.
fO ... P>'bll< hoo"b "" i<o<r. I'00<I ..... ON' ..... •
m;.i" ..
Ku ~ hSt"' .. < Ro<h il".M O.
O«<nIt>e, " . I99J .
Fordopari.. . loti" ..) •• """ on'icott. loOI. Mod
LoeucT "': 4 )-4. lOOl.
Lcpinodio I", .. p.t.r;n-i - " ,"rotnbo<ytOp<";.
Mod LeU, . 40. 9'·'.1998 .
fr«lri U IOn K. NOfro ins S. S,,,,.,...,\od L G: E<t>«•
g<1'<y ~", ... , or.,,,i<o,..,.. iOfl . 1«, i~ _ 1
_ " , . S' '''''e lJ: 912.7.1992.
Hom)I"", M O. 11.11 R 0. PU>co G F: V.".,., ,1IfOm.
"", ,.001;'111 i. 1'1<\1"".'1"')' ........ U<Olo., ~ .
'''n''' ... rev;'w. N....... UIl... y)l: 1flt}.%. I99< .
OI>oo J D. K.. fm •• 1I H. MooI.< I • .,DI,: Tho ioci·
dtJ>tl oN "Ini r~ "n•• mo_i< .bo",..,.'i,;',
i. I'".''''' " ',b """" "'Jorit'. N",,,,,,,",,,"y14:
82)-)2. 1989.
S''' '1' R.ll>« .... ,10 M. EI.KalhllJ" 101 : S .. ," ",.
""'" U\d ohromtlo<ml>Ql;sm: CI;oicaI. I\e ..,.",ic.
..... bio<"'mOcol """"I,,,,,,,,. J N, • ..,...,. 70·
JI <A. I989( ..... ,,",O .
Qutvotlo J F. S"' ..... , I C. Schmidr J L. ".,-,
ThrO<nbccmtool i,,,, I. »OIit,"" ... "h tHV>-lo.d< , 1;0..
mi. MoyoClI ........ 1I\I ll9-J2. 19901 .
Bloc ~ P M. S.... , M f. _
C P: £o.peri<n« ... ith
.... ",.1 ..... m.. '" <olf cO<nfI<U'i"" ... ",uroIot,
.t: 11/).4 . ' 9M.
S.)"<I<r M. Ro.. o<l'" I: '""oc, ..;" ~ ...
lOCi."", ""'h '.uootcoll1"," , ..... 11}" . S~'""C N<~'"
7: )I..o,19n
Cern'o O.... , ..... C •• """hr.. Po Deep .... i" Ihrom·
too<i •• lllllow._
bepa-i. proph".,;, ,n _ u r ·
, .... PO' "'"". J No-u .......... '9: 1J8-", 1m.
Frim 0 M. Bitt« f O. I'ole"i CEo .. or,: "",,-,.
"".., ..... _
... pooi"~""'"""""_or:
w.o,
,,,,,,.I'Iobl"
"
" "'" "'.roouttt'Y.No. '."'IO')'
"
"
".
"""'!II .... ;..,. i. "''''''"rV<oI palio ..... ""' .....
lO. 130-1. 1992 .
R.... S C.Z .... <II<I W I ,M.""". L E." 0/ ' ..... " .
.;'i.i,yol «>lor Doppler no... i"",,", r", <Iet..,_
of """ecolf d<ep ~_. ""","booi. in ",.."pomoI.
.. pO""I,." "i.. po,;" .... J V_ I....... R... ... . ,
""V'}'
"
.,1>1"
".
".
" "'" "1'''''''''
"
)'~26.1992 .
00
111 _7. !9'Jl.
"
n..
o.
Wei" PS ...... "'..... 0 R. RornwoilrJ. .. ..s. Vo/u<
of ..........,.. of
proboI)' Ii'y of do<p-'""'.
,~;, .. <lini<., ....... , .......... (..0.0«1 no1M -I. 1997.
O...bel1;1 s. "'olt. P S. " _ C ... ,,," St'';';'"y
on4"""iror:ilyol. rap;,: wt.o~_ ...., fo, 0d,me, ,. ' .. d",""';,olpul ...... ')' emboli.,".A,,"
r."", Mod 129: IQ06. I I. 1991.
H.II R 0 .R " ~ 0110 E.P;ntoG F........: S.b<:ut .... ·
.... Iow .. "..,r_I... wel.," hepori. coml"'1"l ""h
""",io_ . i.".......... !t<ponn ;,. , ..
pro.,.". I· .... ;" ' " _ . 1'1 """ J Mod 1.16: 97'·
12.1\192.
KuU R O. R..l ob 0 E....,...bloom 0." oj" Kep.
orio r", ~ .... d. " u ccmpoted with te.
i. ,he
i.itio! ,,"'""' 0' of pro ..n01 .. _ . tItr\ltnbO:r<is. N
£"" J M«I J22: 1160-1. IYiIO.
M.... K S. Yu<C P.CIu. K K... ..s, ~It",
""e 'o.,," IT-.e<toolloryh< ... '09Oiui.;. 'hol ....",i.·
eo.. ",pon . J N'.' '''''''I ~ 9)1...00, 1987 .
pre"'"
'_'Il1<0, '"
".
0>
da,.
GEN ERAL CARE
Sl.
SO .
35 .
86.
112.
811.
89.
90.
91.
M,o",,', "'''''or
MAl>l\>JI K A'
poUo' a.... poo;lIci·
pits "'" ;nv.. i.. ,... tnxo~ M. yo CliD !'ro< 71,
• 72-1.1996.
CcI..",..,blorOltbrili •. M«I Lelltr 41: 11·2. 1999.
11<111"" S M.Sonolbo".coot J. Z.I"m D. «<>Ie 0;.
<lo[. ........,.",i.olalk<p""'.,.ici'y .JAMA :!601 :
2660-2,1990.
1k"; ' ~W L: An&i&Gic nephropo<hy. AnoJ />I..,
S<t m: 56 1·!. 1m.
8mmf<na< I.......pi • . 1\1.., LeI .... l'/: 9J ....
1991.
S,"'"' B 1.. . 1I<~ ' o I A, Kinma" I L .,dl, Par<n,«>1
k.lOtOtooI: .nd rnk d. C.woln<e"ln.ll ond opo<l<i'<
"'. ble<\l'"I . JAMA l'J': :)1~1I2.1996 .
Trunadol · A"" ... or ...... ,I<'>' •. :.1 ........ ' .... J7:
W·ti(I. i 9'), .
ONI' for pai" . MOll U ..... 010". 79-&4. 19'11.
1'Ill1_f<>"h,,,,,,<poln. />I..,unorO.l l .J.
'. dd<~ y poOpl< . 8 MJ J 10:. IJ·7 . '99~ .
Qtioin< 10< "n,JIro cnmpo'. :.1'" ..... ne. 28: 110.
96.
Choice of b<.rodlaup>nn. M ... Uuo. XI: 26-1.
BiCO>S._)'<"fO. II,..G.« t>I, .... ~ .. Io.. _
p.obk .... 10 odullS . O",ical p", 'kc I" i~tli ..
no.14. AHCPR publitalioa ' 0. ~2. A _
lor H«ltlo
1'01;" ond !l<.. "",~ . ""1>1;, 1-Ic.ltIo
S..... i« .U.S Dc,..""",., oflt",-,,,, ond Itu",," Scr·
"ice • • ~O<kv i ll<:. MD. 1994 .
a.kno'UOD<h<po,", •• io:i'y. />I.., Uu<.J8; 06.
c...:
9J.
,~ .
to .
M .... So!:o. !i,., M.W.,IoG : M..... ao.rJY' .. or.lliu<y 01 "" - . . for , .......... "' <>I ...".ma!
<nm".
GENERAL CARE
1<,
,
IUS.
91.
98.
99.
lOG,
10 1.
ONp IO'1")"C ~ ~ ' ri< di_ " _
........ 21: 99·
100, 1986.
MidaiOlam. M«I un•• 2.: 71... . 1986 ,
f1u ..... ".I. Mod t.ert.. J<I; 66-I. 1992.
ltam>ayMAE. S.v<" TM .Si _ _ I RI . .,t>I_
c.,.,' rolloO oodatioo wir~ l1I'lw_"lphodoIoot.
Ir Mtd J 2: 6S6-9. 197 • .
W.rbaA. W. I"".~ C .I'rtr' '''k W,"dl.; V<,<utOn'"m ptn'< ... ;"'<Uf<.;n ...........'" p ...... .. d",·
i"'_"'lt"O<_~",.t><IioIti
......"oqi<oI poe" .... A,,-tlot' ... 4(1: J2t·JI.
1991 .
H"... ~) K. Cheon., II M. C.iIjlCD • .,,,," Early.
",",i.. "....,Y' .. :or i. _,..;a! _~ """tIOI i.
_rn: IIoOld ;"jII.ry: I. ~ """....".1 C ~, ca.. i'I'"
11; ,.71·6. '99<1
0101;"1<' M I.R"-1 0 H: No ............. i.vblO<k·
I", ...... i~ til<
i....,.;.. eort ..~
Surs N........ . 9:217·21. !m.
SCS'- II. C"d,,<1I1 E. M.""", M A, .. 0/.: !'or.
0;, ... ,
h 'rilic:' Uy ill pot;"'" oro.,. ""',.
..no odm' ........rion '" -.-""",i.m. N Ecolll J Mod
311: $24·1. 1992
••'"
102,
~, .
92.
..
~~
10),
!()O ,
"_iUI
"""ysi'
1.7. References
2.1.
Dementia
Definition: loas of in~llert ... al sbilit,.,. previl)tlJlly ellai ood (me,,,,,ry, judgement, abo
itract Lhought , and other high~r co rneal fuoctiona) severe enough to illt.e rfere with 80<:;111
andlo r occupational fUnclionillg' . Memory deficit i. the cardinal feature. however, the
DSM·rv definition reQuires impairment in a~ least Dna other domain (langue!:",. per«ptiM , visuO!Ipatia] function. calcu lation , judgement, abotrodion, problem.Bolving 8kjIl8).
Affe.:ta 3· 11% of community-dwelling odull..! '" 61> YI" of age, with II grealer pruenoa
among institutionalized reaidetlLs".
Ri sk faeta ....: advanced age, family hialor)' ofdementia , II.nd npolipuprot<';in E-'I ,I·
.,.
IMlerium: AKAacut.econfuaional atalf. Di.Gtinctfrom dementia, however, patients with
deD1Mtia lI.e at increased ri$~ ofdeveJopingdeJerium"', A prima')' dlSoroerofot1.entiOll
thalaubsequently &iI'!'Cl.$ all ~theT aspect.; ofCOjfllition'. Often repre$ents lir..·threBt.enjog illness, e.g. hYl"'xia. SRp.oi •. W'emic enCi!phaJopa thy ralllO;«< poffe 64), eJectrolyta .. bnonnality. drug into"ica tion. MI. 50'l0 ofpatienta die within 2 yr8 of t hisdiagnosia.
Unlike dementi., delerium b•• !H'ute Onllet, nlotor slgnJI (tremor. myoelonU5, "".
t.erw5). slurred speech. alterEd conscioualles& (hyperalertlagita1.ed o,-lethBrgic. Dr fluctuatioo,), hallucinations may be florid . EEG - proDounced diffusti a\()wi,ng.
B rain biopsy fo r d e m e nti a
Clinical criteria are .. aually .ufficient for the diagnosis of moet dementiaa. Biopsy
shouJd be res..rved for calle!; 01'11. chronIc progreulVe cerebral dillOrder wi t h an UnU!U,]
cli nica l coW'se where all other pOOlSible diagnOlitie method$ have ~o eKh ...... ted lind
h .. "e failed 1.0 provide adequate diagnostic certainty'. Biopay may d.iscl06e.CJD, low
grade 9St.rocytoma, and AD .mOllI: olhen. The high incideme oCCJO among pat.ieoUl.elected for biopsy under the .... criteris ~es5italeflllppropri&te pn!C&utions (IIH
Creu~reld'·Jokob dr_if. page 227 ). In .. repon of:;O brain bioplllH p&rformw t o _
progreo;aive neurodegenerative dllJease (If unclear etiology" the diagnC)l;tic yield ........ only
2{1% (6% WeN! only Hugguliv~ of. diagnosis. 66~ wert! abnonDal but nonspecific. B'l>
wen! normal ). The yield wa5 lIighHt in thoae"With focal MRI obnonulities. Among \he
10 potienl.i with diagn05ticbiopsies, the biopsy rHult led \0 a meaningful therapeutic in te ...... c!llt;on in on ly 4.
Rcoommend a t;on a, B~ M tbe above, the follo .... ing recommendation. are made for
patienu; ..... ith an olllerwi5c uneJeplained neu rodeg.merati.-e dis-em;e:
1. thOlle ...·ith a focal abnonnality on MRJ, stereot.llrtic biopi;y
:l. t h...... wltlloul foc",] abnormality (pouibly including SPECl'o. p£T ...,.n): b.ai.o
bioplly /lhould only be perfonned within an invntigative protocol
2.2.
Headache
Headache (W A) may be broadly categorized as foUows:
I. chronlc recurring headache.
A, vasculsr typE! (mig.-a.ine)' ... ~ bdo'"
B. muscle contraction (U!nrionl headachall
2. hudache due \0 pathology
A. systemic p8thol~
B. intracl1lnial pathology; II wide variety nf atiologi811 including:
1. aubarathnoid hemorrhage, Il!J12~Q onlie!, severe. uaually with vomit-ing, apoplexy. focal deficits pos$ible iM'e poga 7ff2lilr diifel"l!lItial diag-
2.1_ Dementia
NEUROLOGY
I'M" of paroxYlmal HlAJ
inctewaed intra","n ;.1 preMure linm a ny CII\lItI (tu mor, almmWlica l~
2
In, hydr1lOeph"I\I5, inna mmati on, Jli!IeudoluJ>>ur cereb ri .••)
3
4
irrita t ion!W Inflammlltion ofmeningel! m@ningiti.
tumor: with Or without ele~aU!d ICP (no. JXlIt 4!l.S)
C. lou! plIlhoiolD' oft~ eye, nuopha ryr\ll:, OT utracn.ni"J tiRuea (;"duding
~U"lt
<ell artenti.,.- pagt. 58)
o following head t ' II"llIa (~tcor>c:uU;Y" ayndrorne}: ~~ PfJ~ 682
E. f.lllowtllg ainlolllmy t".ynd rome 01 th. trephIned"): 1ft pagt 6J2
A ,,,!Yere new HlA. (It. chaos , in the plltI\!m oflllo"8.tarulinl,: Of' rKUrTenl HI" ( in~
eluding developing IInoclllt.l(l NN, Or ~n "lmormal neurologic enm) w.rran~ (.. r1MoT in·
Yt$tiption with CTorMR I' ,
2.2.1.
Migraine
Migraine attacks ua uallY'ICCLlr in indiyicillaLt pr.dilpeud IA'l ,h"condition, lind mly
be activated by factorl alleh a.\ urill,lli,ht, Itrfla. diilt ch, npll. trauma, adminiNrillioI'I
ofrttdiologic contrast
m~i.
(eJpedaUy 8JlgiOgtIlPhy) and vesodilalol'l ,
CLASSIFICATION
See aJfrO indu under HtodQl;/u" e.lI. [or; crash
pogr 782, pOIH,.. myeIOjfraUl headache ptJ~ 46".
migr~ine
(thundndap headachel
COMMON MIGRAINE
Ep;Booie HI" with:;.lN and photopl:lobil, w;thoutllu", or fleurologiedelkit,
CLASSIC MIGRAIIII£
migrai~
~Ive comp1t~ly
... aur. , May have HlA with occuional foelll neuro\orlC dt:firiuI )
in .. 24 hra .
Over halfofthe Ir""delll neurologie dilturblln~ ~f'It vilUll\' and uluan,. _no!"
poIIitiyt phenomena (lpArk photoplil, ,Ian., IXlmplu 1000metrie pIIuema, fortifiCAtion
apectra) which mllY leaye negative phenOOltl\a (goloma. hemianopia , monocular or bin.
orular yjauplloQ , .. ) in their wake. The HlCond IIIlXt malloon symptOma a,.. .amatoRn..
frOry involving the hand aod lower rac~ ..... fn!quently, defldu may (:QIUI\1t orapha&ia,
.... mipa ....,is. or unil,,~ral elu"",;n ...... A slaw mardl·like progrnllion ofdeficit i. Cha rllllVlril'itk. Tho! risk of ~Iroke is probably inatlaMd ;" palientll wilh mign,,""'.
Com mon
Ihlll
COMPLIC.'o TEO MIGAAIN£
Occuional IIll.8eU ofdaJ.4jcmigte;ne with minimal or no auociated HlA, and comple~ re&Olution ofneuroJorie deficit ..... 30 dap
M/OAAINE £OU/VAL£f'/T
Nelll'Olork 'ymplomf INN. visualaLlrJ.. etc. ) without HlA (_phaJg.e migraine),
Seen mc:.11y in childnn UsuIII,. dev&lopll into typical migraiae with I~ Au.. lIIay be
ehorVlned by opening and _an_inl contenb of a 10 IIll!I ni(ed,pine capw]e'".
HEMIPLEGIC MIGIM/Nf
lilA typiC*lly pr-'eII hemiplegia whkh may penlSt eve"
Il~r
HlA t«olves.
CWSTER HEADACHE
AKA h;'l.8min~ mllTlllIl.. Actually a neUl'OY8ICUIllt ""tnt. di$tincl from true mi.
IUrne. RtcutTtnl unila~tll altacks ofseYeN! pa;". Ulually oculoCrontal or IICulolempGfli wilh occuional radiation Intothejaw, ulu_Uy r«Ilnin,on theslme , id"of the head.
lpe:ila~ralautonomic: UVl~
(UW)juntliyal injectIon, nau.l
conlle~tion ,
th ino rrhea ,
lacfllUlltion, fad.1 nUllhin,) .... comtll(ln , PBrtial Hamer'aayndrome (ptoai. and ml .... \s)
_ellme. o«u,.. Male;f~ale ratio U. ~ 5;1, 25~ of pat ienlll hay" a petllOllal or fami ly
hi.tory of m igTIJM.
H"adache. ch'''doI'riu~Uy h.... no prodrome. I.t SO-SO minu\.O$, and ~r one
or mote limes daily u...al\y (or 4- 12 wHIu, often lit a .imila t time day. following which
ther. is typieally, remillion fat an average of 12 month.",
or
NEUROLOGY
2.'2.. Headache
BASILAR ARTERY MIGRAINE
Essentially restr icted to adnlellc~nce. RecurT~nt episod811 lastln!: minutes to hours
oftral"llnent neurologic ddidu. in distribution ofverwbrobMilar system , Defioil& iru:.iuu;
v~rt.igo \ moat common ), ga;~ ataxia, ..,pual disturbance(acotD,Data, "'Ialoeml blindn_),
dysarthria, fo1!owad by ... veu HlA and DC:C8IIjonaLly nausea a nd vomiting". Fami ly his_
tory of mrrrBln~ is present in 86%.
2.2.2.
Post LP (myelogram) HlA
AKA "poatapinai headach e" or "spinal helldath~·. MaY·IIIIG folio .... proc:edure. other
than l P/myelogmm, such 811 dunil opt!ninc (..." pa/le 308). Can alro o.....,ur with 5pontane·
O1.Ir intratrauial hypotension i!eep"'¥t 178).
CllDi ca1 rea tures
Important distinct ive cho.ract.eris t lc: HII'. (Ittt.ITS .. hen patient is e~, and ia corn plelely or partially (but eignifitantly) reliev..:! .. hen recumbent. May be lll!wcisted .... ith
nsusea. vomi ting. diuiness, or v;"'uaJ dioturbances.
Tim e CO~: MO$t pD6t_LP headachea IPLPllA) hav"-,, delayed OM~1 2" ....8 hl"l after
the LP, and although they may octU . ....eek~ poet-LP. mll&tal~o develop within 3 day".
The duraliao ofPLPHA varies, with a mean of 4 dBY"''', IUId r eports of dumtion of
mon t hs" IlIId even> 1 yeB. '".
Pat b o pbY!lio logy
Thought to be due \.0 continued CS F leakage IhrQugb the hole in the duro " . which
redUCN the CS F ' cuahion" of the brain, 10 the uprigh t po.9i ~iM\. the pull of gravity on II ...
bmi n produces t m clicmon lh~ blood veMelaQ nd any .trucluu s tetherinR the brlli n to t he
pain-sensitive dura. CSf' may sonleti mu be.delllon~trabl~ in the tl1id.w:a.I.pacc.
Ep id e mi o lo gy ro llowiog LP
Reported lnddenct: " ng" is2-40%(typically ~ 2~). bigheraftudiagnoatic LP than
for epidural anuthuia".
For variobles in LP tl1at impa~t upon the ri$k ofPLPHA, Sef' paMe.617
T REATMENT FOR tvA FOLLOWING LP
Ini(ial
1,
2.
3.
4_
5.
6.
'cOIlservative" me:saurea include!'.at in bOO for at leat1l24 hI"!!
hydm tion (PO or [V)
analgeuCii for lilA
~il!:ht abdominal binder
de,oxyrortiaone acetate 5 mg 1M q 8 brs"
colTeine lodiwn benzoate 500 mg in 2 ~c IV Q B hr. up to:l d mllll (70% of potienlS
had relief with 1 or 2 iqj.,dlo~"
7, high-doae .teroi,a, report ofsuccK8ln 8 case orinll1lUao.ial hypoWlls;on auoeis led witl1 "ponllln&OU8 Blit ventricles tapering down from a MArting d05l! "rd",,amethasone 2{j mgldayll
8. blood patch if refractory 1_ below)
E PIDURAL BLOOD PATCH
For refractory PQSt-lumb.o.r punctu r~ or poll-myelogram HlA. W-oru in one a pplica_
tion in over ~ of caul. mil)' ~ repea\.ed ;fine lTective" . Theoret.ital ri8q: inflKlioo,
caude equi na com prcasion, failure \.0 relieve HII'..
Tec hn iq u e
ACCl!uing epidurall1pace (one ofuvera! techniquu): prDC:etId as rouline LP. When
ligame4Ls a re Itavened. and lleedJe tip iB neating apiDel cane!. style!; is renwved. Then.
either plllC.l drop of st.erile u line in hub (hanging drop tE<:hnique) ud advance while
wa\.chi.ng rOt Jl Ie be. d ......... n iM" n~e at epidural apate if entered, or gtonLly try it\je<:tinK a lr with small !l.Yrinlle(prefera b!y glSMjwhile advlltlclng, wben the epidural space Ii
entered, rui.t aoca Ie ir\ie<'tion disa.pp8Q r~, but CSF cannot be aspi rat.ed .
A venlpunoture site. i~ prepared a.eptlcally, 10 IIlI oftl1e pollent'. blood is .... ith·
dl"lwn. After verifyiog CSf' c:annot be aspitaLed through the ~pin w l needle. the blood i.
il\iected i.n\.O the epidurelapa<:e. Afte r 30 minuw supine, patient m~y ambul.te ad lib.
NEUROLOGY
Parkinsonism
2,3,
PArkinaonjsm may be primll ry (irliQpath ie paralytis .gita", (IPAI , cllllllical Pa rki n.
\OOn', niUlle) or lW\:onrlaryLO olhu con dillon l. AU lUu lt from I Il!IaUVf; laM of the
dOp.llmine mediated in h lbltioo of th .... necL\ C>f acetylch ollne.n Ihl! b. , a! ganIl:1i,.
I DIOPATHIC PAAALVSIS A01TANS
CI .. ¥icn l Patkin!.On'. rlilellae. AKA ! lIaking pa l.,..
Table 2-1 Cla sele triad 01
C lin ica l
Parktnlon'l dlHalll
Aff«tA: -l'*'ofA,mt n canl>apliO)'f'I". M.le:remaJ.
I':
- :"= , ~1'*<nt)
....
1
flItlO i. 3:2. Not clea rly l!:I'I"lronmentllJ!y o. , enedeflUy in.
duted, bu\wu)' bo! Infl uenced by th~ f.etart.
The donie triad i, shown in TIl"~ 2· 1. Other .igI..
may indude; pos tu ...1 innabill l)', micrographl. , mask-like raae.. CHltl;'On&i.~ or ..... n.
J tlUffiin, ate"" l mll ",h", ' per.i lf; p,,) or feuinll!inr i.it ,
C lini uidly di~l ingui8hing IPA from .ceond "..,. padtin..,nitm (I« bfiout): MI.1 be
diffi cu lt urly. IP" IIfInflr.Uy uhibia ""dl.l"l on... 1 ofbr&d,yk.inell. with trelnor lNot i.
of'Wn lt8ymmetrica l, .nd initi a lly rH porKIl wen too Iev(ldopa. OIM. di_den! are .""",11.
ed with rapid progre..,OJ! of iymptGmll, ",bee the initia l rupome loCI .... odopIl n ~u;vo­
cal , or "'M!n U",rel. u.rly tnidli,ne 'Y!'lpWlII' (lluo1ia or hnpainrol!nl or ,ai t and blilel>Cf!,
&phiocter di!tl.lrb&r>«! ... ) or 1M! pl'l!Hn ce of oUlu fe.tulU .ud'! .. earty demen ti., H n_
1io01")' findinp. profol,llld orthOli talic h)1lOten!lion. OJ' .bnonnalitin: ofutraocular
m",,~nta"' '' .
Pa tb opbys iol ogy
Degeneration prim&rlly of pi~nted Ineuromelanin-Iaderl) d opaminel'(ic: netU'on.
oflhe pIIn! eompatta of the lub&Ulntia niera, <Qultmg in reduted levall ofdopernine in
thenOOHlriat l,lll\ (ca udate nude uR. pUL/unen. globu • .,.UidUII). Th i. decre&lfl the U t;vi ty
ofinhibil,ory neurons with predomimUllly D2 dUll ofdoparnine uoeploClMl which pl'OJftl
directly 1.0 the internal i;~nl ofthe "lobUi pallidu. (CPil, and al$o illttell~es (by lou
orinhlbilion) Dttivity of r.t'u rons with pndominanUy 01 ft'Ct'PlOf1I whil'h project. indifllOl:l'
Iy w the globui paJlidut exlllma {G Pe) .nd .ubthlllamic nudelU lI , The oet relUlt i. inCTt'a-' "c:tivi!y in GPi "'hieb hat inhibitory prq;..,tion. loCI the thalam~ "'hil'h tlMln
I UPpreJSel aclivity In the . upplemenl.l'll molDr cortex llIJIoul other locat.on..
HiJ.lologically: Lewy bodies (eoainoph llic int raneuranal h)'lllinoe indllSlOlil Ire tilt'
hllimlrkoflPA.
SECONDARY PARKINSONISM
The dift'~r tDt ;' 1 dl~OIiJ loeludell tht' following etiologiH or Htondary pa rkinMlnilln gr ParkinlOn-like «mditi01U{IOme. rmlTt'd to a. -ParlLlnlon plus"):
1- oli vopoDIcx:ereb~Jla. dege.nuel>Oo (OPC)
2. I lriato-ni{fal d~lI4! ration ISND): more .",!!ISi... Ihan parkinsooi.m
3. .-t.enoephaIiLie pIIrkin$oni,m: foliowed.n .. pidemk oft~PNoU lil ~tharg>ca
(von £,;onomo di~lI) in tIw 1920'" VIctim, I." no kmll'~r livir\i_ Distinauiahing
ruwrea: ClCulOC)'ric niail. In!mllr involv ... not only elItremlli ... butlllso trunk
and he.d, uym llletriclll. DO Lt'...,. bodi"
... progreaah'f. IlIpr'lDuciear palsy (PS.W): iropa ired v@rticalgne (eu0600»
6. m"l tiple .,stem IItrophy {SilY-Orager .yndrurne1. '" tHlc>w
6. d"., induced: iDdudn:
A. p~riplioB drop (alMdy females _m III~ I UlIOepllb ll!)
I . anllptycbolict (AKA neu.roleptict); hal0pen601 (Haldol*) whi<:h
work! by blocki", ponayn apuc dopamine receptors
2. phf,nclllillline Inliemeti~: pnxhlorperulne (Com pll1inl4)
3. me!odgpramide t~anll)
... . -rpinl
B. MPTP (1-methy l·.... phenyl · I .2,3.6-t.eu.hydrupyri"in~); II commert:illily
a ... iLable c:[email protected] illl.gaby-productofthe.ynlheai l
or MPPP(I rnependinll "",Ioel tha t w . . .ynthfll.ed lind ae lr·injeo:tl'li by II
NEUROLOGY
2 .3 Parlunaonilm
7.
S.
9.
10.
II.
12.
13.
14.
15.
graduate 6~udent". and later produced by illicit drug manufac~urers to be
sold as 'synthetic heroin " and unwittingly injected by some IV drug abusers
in northern Cal ifornia in 1983". MPTP was sul»equer.tly diacovered to be
a potent neurotoxi n for dopaminergic neuronB. N! a rule , the reBponse to
levodopa is dramatic, but short·lived
C. there ia an aa yet unproven assertion that metbylenedioxymethamphet·
amine (MDMAI AKA Ecstasy ( on the street), may ha"""n the onset ofP ...·
kinsoni sm
tox.ic: poisoning with carbon monoxide, manganese .. .
iscbemic(lacunes in basal ganglia): produces so-called arteriosclerotic parkin·
80nism AKA vaso;u!ar parkinllonism: "lowe... halr pIIrkinllOnism (gait distur·
banee predominates"). Also causes paeudobulbar deficits, emotional lability.
Tremor is rDre
posttraumatic: parkinsonian symptoms may ocCUr in chronic traumatic encepha·
lopatby (dementia pugilistica, _ JXJlI~ 68."l). There Dre usuD l1yother features not
nonnally present in IPA (e .g. cerebellar findings)
nonnal pr~8ure hydrocephalus (NPH): urinary incontinen(e ... (& .... fKlH'l 199)
neoplum in the region of the substantiD nigra
Riley·Oay (familial dysautonomia)
parkinson·dementia complex of Guam: dauic lPA + amyotroph.ic lateral l cleroais
(ALS). Pathologically ha l festure. of parkinsonism and Al~heimer'1 disease but
no Lewy bodies nor senile plaques
Huntington's diMase (lID): whereas adulu typically show morea , wben HO
manifesu in a young penon it may resemble IPA
(8 pontaneous) intracranial hypotension may present with findings mimicking
IPA\.-page178)
MULTIPLE S YSTEM ATROPHY (MSA)
AKA Shy· Drager syndrome. Parkinsonism (indisti nguisha ble from IPA), PLUS id·
iopa thic orthostatic hypotension, PLUS other , igna of autonomic ne.-voU$ system (ANS)
dysfunction (ANS findings may precede parkinsonism and may include urinary aphincter disturbance and bypenenaitivity to noradrenaline or tyramine infusioWl). Degenera·
tion ofpregangliQnic latenll>om neurons of thoracic 'pinal cord. NB: classic IPA may
eventually produce orth(l8tatic hypot..-naion from inactivity or 8$ a result ofprogresaive
autonomic failure. Unlike IPA, mO$t do not respond to dopa therapy.
PROGRESSIVE SUPRANUCLEAR PALSY (P$NP)
AKA Steele·Richardson·01alGWski syndrome"".
Triad:
l. progressive s upranuclear ophthalmoplegia (chiefly ver tical Caze): paresis ofvol·
untary vertieal eye movement, but atill moves to vertical doll·s eyes maneuver
2. i>*ludobulbar palsy (mask·like facies with marked dysarthria and dysphagia, hy·
peractive jaw jerk, emotional incontinence usually mild)
3. axial dystonia (especially of neck and upper trunk)
N!sociated finding" sutCQrtical dementia (inconstant), motor findings of pyramidal,
extrapyram id al and cerebellar systems. Average age of onset: 60 yrt!. Males comprise
60'1>. Response to antl.parkinson drugs i, u8ually very short lived. Averagesu ..... ,val after
diagnosis: 6:1 yrs .
Differelltiating from Parkinson·s disease (IPA):
Patienu with PSNP h8ve a pseudo-parkinsonism. They have mask facies, but do not
walk bent forward (they walk ered), and they do not have a tremor. They tend to rail
backwards.
Course
I. early:
A. mDny fall., due to dysequilibrium + downgaze palsy (can't !lei! noor)
B. eye findings may be normal initially, subsequently may develop difficulty
looking down (t"Specially to command, l~ to following), calories have nor·
mal tonic component but al»ent nystagmus (cortical component)
C. alurred spe~h
D. personality ch!lllges
E. difficulty eating: due to pseudobulbar palsy + ;nabili~ to look down at food
on plate
..
2.3. ParkinsoniBUI
NEUROLOGY
2.
I .~
It. eye. fIXed ~utTaUy too response to oxulocepbal ic. or otulovullbular1); OIl1.11 •• ImmotiU ty ill due Lo f. (Hltlll lobe laio n.
8
"""k atiffe ... in "",ten,lon l. etnK'OIllI)
SURG ICAL TREATMENT FOR P AAKINSON'S DISEASE
BerGn Ih .. introdudion or t..dGp. in til- I. te 19&0'., .te' f'Otactic tblilemo!.Omy ... n
widely used fGr Park ....... diteaae. Tb .. loaItlon ullimll.ely targelN for lel io",;ng"'u
the .... nll"Ol.III,...1 o"deu •. Th .. p.-lu...... Q1'ked better for Nlifl.vinr the t~mor tbflll for
the bradyllinUla. however It "'1\1 the lillie. lympLom tbllt we.. mOll;t.diubliog. Thi s ~
tedu ", eanoot be done bihllllrfl Uy ... ilhoul .igni licunl rislJ to 'PH\:h function The p.ocedun. f.1I oUt GfflYOr wh.n more effective drop ~lIme IIvIIU.b!e"
See SW-I,",lll'WOlm,M 0( f>Qr1ti1lWll', di __ 0"' pap 365 !'or rurther lofonnation.
2.4.
Multiple sclerosis
A derllYlLlin,ti.Q( dlll,",_ (Iffecti", "nly while malto.r) IIfth. al1!brom . optIC neTVl!II,
. nd s ploaJ mrd (espec:i.lI". oorti«llp!nal lUlU .nd the pOIIl@rior 'JOJumru). Ptod"Cftmultiple pl.que. of VII no ... ..,;n dilfu ... loxe~1\II in tl!ll CNS. eapec:illily in th" poi"riv~ntri.,.
UID r white maUer. LHiolalniti,lIy eYOQ a", innIR'ma~ response with monoqteo and
]ympl»cyllc pl:nvucul., ""mnfi;. bllt with 'g~ fedle down to el ial SClil ri.
EPIDEMIOLOGY
Utili] IIp.of onMt ; 10·59 yell,..., " 'i lh lb. gTellli'!lt peAk bet.... een agell20- ~O y,",,~.
Ma le 10 femal~ I'Itio: 1.J§,1.
Prevalence v.nOM __.th latitude, e.nd is < 1 peer 100,000 rtf:1I r iheequator, lind if - 3Q80 per 100,000 la Ihe north*m U.s. and Canada.
CUNICAL
Cauj;eS exac:erb.a tioRa.n d ~rnis­
T.ble 2-2 Cl1nk:aL
MS
l ions in variou$locationJ In the eNS
(diuemioati~ aDd liIDfl ). Com·
mon Iyrnploms! visual utu rbantu
(diplopill, bl"rring, fielcl :U1ll1I• .,.,1.0.
mil. ,pastic par.pa res;lI. and bJ,ddp...
distllrbllntK. N01'llf:11t1l1turfl for tbe. tima
1>'1,,'$11 o( MS if. . h ...... n i", 1'bbh: 1'. 2"1. Re1~P8iDg-rem'lting MS i, the IOOiit com·
mon pattem at OMet,.nd hal 1M beat
I'f!Sponlie to therapy, b,,~> 5~ of cues
ev"ntually become semn~al')' pt'<IgTeI.
slve MS. OnlY 10% have pri mll')' progrl!e$i,"~ MS. and tllKe ~ .. tienll tend to
be older at OUMI (.0-60 yea •• land (~1I""ntly develop p.ogrt'"ive DlyelopalbY"". ProgrHsiw I'tla~in, MS if. vel')' uncommon
De fi cit.:'! preHnt " 6 months "Iua lly penlllt.
D ifferentia l diagnOll is
Th e pletllora of possible sign. and lympl.oDll Ul MS taU5H tha di fferenllli di~
to e~t.ond to almost,,11 tOliciition . ",uli"i ~l or diffuac dyJ: fW>Ction ofthe CNS. Condl·
tiou. that mllY t losal)l aunic MS di nio:slly and Gn d iagnoltic to.lt;1\I include.;
I !\C1,ta d.i~rnin .t.ed en<"flpb,lomyeli lil (ADEIII); may alllO Ila>'e CSP-OCB, rener·
Ally monophasi c
2. eNS Iymphomll . ,u ~t 463
3. other flonly Nll B~ demyalin.t,"g diuaJeS: a.g. Dewic ,yndrome,,"~ ~ 90Jl
NEUROI.OCY
2.4 MultIple f('!ll'OIil
..
Signs 80d s ymptoms
Visual di s turbances: Disturbances of visual acuity may be csuaed by optieor retrobulbar neuritis ..... hich ia the pTflSenting symptom ofMS in 15%oftllSfls, and ..... hich OCI'UTS at
some time;n 50% orMS patients. The percentage ofpatientll ..... ith an attack of optic neu·
ritis and no prior attack that will g<I on tode~elop MS ran ges from 17-87% depending on
the series". Symptoms: scute vi sual l\lfIs in one or both eyell with mild paln (ofum On eye
movement).
Diplopia mey be due to internuclear ophthalmoplegia (INO ) from a plaque in the
MLF. INO is an important sign be<:ause it ra rely o<xurs in othu conditions b<lsides MS.
Mot-or findings: Extremity weakn""s (mono, para, OT quadriparesi s] and gait ataxia are
among the most oommon symptoms of MS. S pasticity of the LEa is often due to pyramidal
tract in~olvement. ScalUling speech results from cerebellar 1.... ions.
Sensory findings: P05terior column invol~ement ofWn causes 106S of proprioception.
Paresthesias of extremities, trunk, Or face oc:.:ur. Lhenuitt<!'s sign (electrie shock-like
pain radiating down the spi nl' on neck flexion) is common. but is not pathognomonic.
Trigeminal neuralgia occun in ~ 2%, and is mOre often bilateral and occurs ata younger
age thsn the population in general" .
Me ntal dis turbances:
E upboria (Ia bellI' in ·
difl"e.-enea) and depression
occu.r in ~ 50% ofpatlents.
Refl e", changes: Hypcrreflex.ia and Babinski signs
sre common. Abdominal cu·
taO!!9ua reflexes di$apPl'ar
in 70·80%.
Table 2-3 Diagnostic criteria for MS
,
GU SymptOIDll: Urinary
frequency, urgency, and incontinence arecommon. lmpotence in males and
reduced libido in either sex
isoften_n.
,.
D IAGNOSTIC CRITERIA
No single clinical feature ordiagnO$tic test i~ ad·
equate for the a<:eurat<!
diagnosis of MS. Therefore,
clinical information ia inl4lgrated with additional data.
Diagnosing MS after a ";n·
gle, aoute remitting clinical.
Iy isolated syndrome (CIS)
is ~ery risky . 50-70% ofpa·
ti~nu wit b "CIS ,u88~s tiv.
ofMS will have multifocal
MRI abnom:>alitiell charae·
l4lristie of MS. The presenoe
of these MRJ sbnormalitiell
increases the risk ofdeveJ·
oping MS in 1-3 yellNil (with
greal4lr prognostic signifi·
cance than CSF-OCB). The
mOTe MRJ lesiOl\lj, the higher the risk"'. Criteria for the
diagnosis ofMS" follow$.
The l4lnns "dinieally
~
definite MS· and -clinically
probable MS· are no longer
recommended. Preferred
terms: MS. possible MS (at ri5k
"
,
A.
,. 9 T2Wl lesions on MRI or
C.
D.
lId<IiIionaIlests no! required. " MFlI
Q<
CSF tesIs ore dane and ar.
""9"'ive. aPlOl\l e. lreme cautIOn In dlagr<>sing loiS
I"I'IU$I ","I cril<tr\ec In r _Z-f
POSillve CSF sI>owing o/IgocIc>nalt>an<lS.""
d'""-ninaUonTn
~on
t.!FlI
T.,.
U
must mM11hil ttIIeria in r.bleZ·5
aln)<mei Ykuol .....ol<od pOI",, ~ ol 8$ _
in loiS (IeIay wilh
~I·
p r e _ w..... lo1m)
for MS but diagnosis is equivocal). Or oot MS"'.
2.4. Multiple 5tlernsis
NEUROLOGY
Diagnostic criteria ate shown in Tobie 2·3".
Ddi"itions"
I . attack (exacerbation. relapse): neurologic
disturbance lasting> 2:4 hrs" typical of
MS when clinicopathological studies de·
termine that the cause ill demyelinating
or inflammatory lesiaM
2. typical of MS: sigruo &. syrnpwms (SIS)
known to occur fn-quently in MS. Thus
excludes gray matter lesions, peripheral
nervous 6ystem lesions, and non·specific
complaints such as HlA, depression, con·
vulsive .;eizurea, etc.
3. separate leaions: SIS cannot be explained
on bas;' of singI.. lesion (optic neuritis of
both eyes simultaneously or within 15 days
represents Bingle lesion)
Table 2-4 Brain MAl criteria lor MS
3 althe loIlowIlI9 4 cr~erit·
I. 1 gadollnU:!l-enhancing Iasion or, d no
gado5nlulI1 enhancing lesions, theo 9
T2WI!esQns
2. ,. 1 intratenloriallesion
3. ,. 1 jultlac:onicalleslon (i.e. lnYoMng
subcor1iclll u Jtlers)
4. ,. 3 pefiol .... \rio:uIaf lesions
1 ~ CQf(j lesiDn car!be- subs ~lu'ed 10,
1 bra i n _
Table 2-5 MAl criteria for d ieaemlnaUon ollesillns In time
MRI
MRI i. the prefeJTed imaging study in evaluating MSI> and can demOlI9tl'at& dissemination of Ie·
sions in time and space. Recommended" brain MRI
criteria for diagu08ing MS are . hown ill Table 2·4"'n . Le5ions are normally" 3 rum diameter". M~R[
shows multiple white matter abnormaliti8$ in 80%
of patients with MS (compared to 2:9% for CT)'"· ...
LesionJI are high signal 011 T2WI, and acute lesions
tend to enhance with gadolil!.ium mOre than old Iesion a do. Periventricular lesions may blend in with
the tignal from CSF in the ventricles on T2WI. these
leaioll8 are shown to better advantege On proton
density images as higher intensity than CSF. Spinal
~ming hOI cri1ical. buI 3 mont/I$ b
cord lesions normally show little or no .welling,
should be:it 3 mm but < 2: vertebral S<lgments, occu·
,~py on a portion of the cross·section of the cord, and
must be hyperintense on T2:W1". Spe<:ificity of MRI
ill _ 94%"', however, encephalitis as well as UBO. _Il in aging may mimic MS lesions.
Focal tuweractive demye lwatillg lelioo l
{TOLl may ()(:Cur in isolation or, more commonly. in
Tabif! 2-6 CSF c.iterla 10. MS
pa\.ieots with established MS. TDL way represent
1. ~,1alilative assessmeM or IgG is tt1e
an intermediate poaition between MS IlI!.d ADEM".
mas! inlormatiYe aroaIysis
TDLs may enhance, al!.d show perilesional edema
and !hUI be mistaken for neoplaSIIllI . Biopsy resulte
2. analjosls should be pi!I100ned on
~Irl\ted CSF al'lC! musI be
may be confusing. MRS may not be able to differen·
c:ornj:ilIed to sillu1taneoosly run setiate from neoplasm".
rum tampIe in Iha same assay
3. qua~·jtali'le aroalysis shook! be
CSF
made in termsol one or Iha 5recogCRF"n"lysi8CS1n IUPf'Ori.the di~E"'""i9in lome
nlleCSIalnlng pauems lor cell
cases, hut cannot document disaeminatiOll oflesiona
~. alO!I'1e, lestspeflooned on!heCSF
in time or space. The CSF in MS is dear and color.
r~ wac, protein & glucose,
less. The OP is normal. Totel CSF protein is < 55
lacfale) shoUcI be I8lwn iI1Io considmg/dl in - 75%ofpatienU, and < 108 mgldl in 99 .7%
e.aticn
(values near 100 should prompt a search for an al·
5. Hcm.cal suspQon is high 001 CSF
ternative diagnosis). The WBC e()unt is" 5 cells/Ill
res.jIs are equivocal. neoalive 01
in 70% ofpatienu, and only 1% have a count> 20
show on1y a single bar(!, conside,
cellslpl (high values may be seen in the acute myeli·
repeating
the LP
tis).
6. ~'.~a!WelgGisaCflr1lllemeota'Y
In _ 90% ofpatieoUl with MS, CSF·lgG is in.
teS!, but Is no! a S\bstitule lor qua1itreased relstive to other CSF protein., and a chara.,.
tative IgO t\1sting
teristic pattern occurs .... garose gel electrophoresis
shows a few IgG bands in t he gamma region (oligo;>clonal band. (OCB» that a re not present in the serum. CSF-OCB are not spe<:ific for
MS, and ean ooeur in CNS infections and lI'IIs commonly with eVAs or tumors. The praNEUROWGY
2:. 4. Multiple selerosis
"
dictive \l81u8 of tile ebtente oflgG in a potient w;tllauspcctcd MS lias not heeD satisfactorilyelucidated.
Recommended ~rilerie llavlI been publi, lIed", m~t of wlli(1I pertain to apecifiea of
laboratory analy.it. pertinent cliniClI1 e~wrpta ... e allown in Toblf 2·6.
2.5.
Amyotrophic lateral sclerosis
·
I
t Key fealur ..
a mi~ed uppe r an d lower motor neuroo di_an (UMN - mild lpaltici ty in LEI;
lMN - atroplly And f.w:icullllion i Ln Ur..)
• rw co~itive, .. ruory, nOr autonomic d funct.ion
• e/lu.ed by degllneration of ne...,...,n, in t),le tervic,,1 .pi ne end lD&duU. (bulb)
In llle U.s. emyotropllic iatflral sclcowi. fALS) i. AKA Lou GeIuig'1 dilellM.
EPIDEMIOLOGY'"
Preva lence: 4·61100,000. Incideote: 0 .8 · 1.21100.000.
Familial in 8·10'l00fca_. Familial ca$U Ulually folio ... autDtomal dominant inlier.
ita nte. but oecasionally demonstrate a r_ive patl.olm.
Onact usually aner 40 years of age.
PATHOLOGY
Degeneration of anterior 110m alpba·lDotonlluron. (io tho! lpi nal cord IIlli In brain
,tern motor nucllli) and cortioospina! tl1lCI& (lle/"lfle AKA motor neuron diseue). Thi, produces a mixed upper and lower motor DeuTOn discue, ... itll a great deal orv,ri lbi lity de.
p"nding on wllicll p""'om;nate, at any given t;n:>fI.
The etiology of ALS illtill not known with certainty.
CLINICAL
Involvement il ofvoluotary mu..:I.., eparing tile volunury ~ 1Il,,"lee and urinary
ephincter.
Classically, presents initially with weaueIII and auoplly of the hands (lower motor
ncuron) witll l PIIllicity and lIyperunexia of 1M lower extremiti"" (upper motor neuron).
However, LEI may be hypon!fleltic if the Io"'e r motor neuron delicita predominate.
Dyu.rthria and dysphagia a ... cau..sed by a combination of upp"r and lower motor
neuron pathology. Too,gue atroplly and fasciculations may occur.
Although eornitive deficits an! generally considered to be abosent m AlS. in aetual·
ity 1·2% ofca_ a ... auoc:ialed with dementia. and cognitive changes may occasioo.ally
predllte tha ul ual fea t ura of ALS" .
DIffERENTIAL DIAGNOSIS
It is important for the neurosu'¥e<ln to be able to dilrtinguisll A1.S (rom cervical
.pondylotic myelopathy. SeepG6t 33J for a di..:uHioo. of differenti.ting feetur"".
DIAGNOSTIC STUDIES
EMG: Not abaolutely I1«t'lS&ry to make diagnoei. in moIIt ca.&eI. Pibrillationa and posi·
tive I barp .... Vel are fouod in adva nced _
(may be abRnt early, "pedally ;fu pper
motor neuron pathology predominatel). LMN findin p in tho! LE in theabRnceon .. mbeor
Ipine di.."c. Or fibrillation potenti,l, in t he tonaue are luggestive of ALS.
LP (CSF): May have . lightly elevated prol.ein.
TRE~ TMENT
Onpng trial. with riluzole (Rilute14), whicll inhibita tile pruyn.ptle ........ of
glutamate, indiClitol that dOH' or50-200 mgld inCrf!8MII trach_tortly·free survival al9
&; 12 months, but tile improvemeot it roortlJ>OOkott Of" rnay be non-eJ.ittent by - 18
month," ". At tile tima of thi. writin" the d"., it aVlilabLe onLy for prema:rkl!tln. trials.
and cannot be procured comTOCTcially.
Much of care i. di~ted tow.rd, minimiain, diubility:
I. ..pintion may be treat$;\ witll
2.5. Amyotrophic iat.e!'al lCleroai,
NEUROLOGY
A. Iroch"""IllIllY
B. gtostroslllllll' tube III allow cootinued fceding
C. voce] eord ill,jedion wit h "(!f1on
2, a paslidty thaL occun wh(!11 upper Illntor neuron defrcit.s predomin~~ may ~
trea~d (usually With ! hort.· UO'ed response ) with:
A. bsdafen.: alM! may re~eve t.becommonly oc:currlng cramp. (,el': fX18t 368)
B
dia~epam
PROGNOSIS
~IOlIt patients die within 6 years oranset (median Bu,.".i"al, 3-4 yrsl. "h ... e wIth
prominent or(lpharynlfulsymptol1t$ may haO'e 8 . harter lif....span usually due ta compJi.
ClI.tio"" q{ IIspinl.lion .
2.6.
Guillain-Barre syndrome
t Key features
•
acule onselofpenphet a! neuropathy with pf'Oll"l!Sl ive .... uscle weakne.u (more
BeVe~ Drol{imal!~ with arefleria, Teaches mllll'lmum o"e r 3 dllYI t.o 3 waeu
cranIal neuropal : 8 180 conunotl, may include fadal diplegia, ophthalrnopltlf;ia
little ar nose.uory invo!veml'n t (paru thesiu lire not uncommon)
onset often 3 dayo.·6 weeki fo UowI,IlB" "ira! URI. Immunillltion, ar s urgery
p&thol~: foeal Rgnlental dem!eli nlltion with endoneuria1 monocyl.ic infll lrat.l!
elevated CSF protein wil.baul p eocytosia (albuminocytalogie d,s6Ociation)
AKA BCUU! id iopal.blc pol)'TlIdiculoneuritiB. "he IIlQIlt common acquired demyeli nat.ing neull>\>athy. lncidenoe is _ VIOO,OOO."he lifetime risk forar.y one indlvidulIl gettin!!
Guillain·Barri &yndro"" (GBS) is _ VI,GOO.
Mild cases of CBS m8y pre&ent only with alllJ<la, wh"reaJl fuhn;nllnt _
may u _
""nd to pllrslyu .... apirowry muscles and cranial ne~.
Frequen t (but not euentjal) p~ing even Ll: vinll ;nfKtion, &urgery. immuniu·
liM, rnycoplnma infection. May follow onfection with C"Il\P1{obod~r j(j.. ni (. 4 days of
Intenae diatThea). Higher frequen<;y in th" fo\lowing conditions Lhan ,1\ genera l popula·
tion : Hodgkin's disl!8se.lymphoma.1upu~.
The a<:tua! cauae i. not known. May be due to antibodies to J'l!ri pherllimyelin .
DIAGNOSTIC CRITERIA'"
I , fealuree requiNd for diagnosi s:
A. progT"'I'Iive motor weaM OlI!s of mor.. \hlln I limb (from minimal weaJrnes>o
,,-ataxia W para]yai~ , lJIIIy include bulba r or facial or EOM palsy ). Unl ike
mO&t neurO;lllthieli. proximal muule3 .re affected more then dista l
B. arene";. (usually univenal. bul distal Brene~ia WIth d .. finiLe hyporenexl a
of blCf!p5l1nd knee je rks suffices if other fellLUrei consisLent )
I!. featun!S strongly 8upporti~e o[diagnosis:
A. cHnicol featu res (in order ofi n,l'on.ance)
t. progT"e,jon: mowrwe3kness peaks aL2 wksm 60'll>, by S wI\! in 80%,
and by 4 wu in ,,9Q<I,
:l. relat!vellymmetry
3. mild sen!lOry sympt.mn;uaigns (e.g. mild pa rea\hesia8 in hands Or feet)
4. ~ involvew&nt: flW;l weak geH In 60%, \l.Wally.lilla!&uJ.
GBS ~nll initially in EOMs Of other Cr. N . in "6" of C3$eS.
Orop~,eryngeal mUlw:]l'lI may be 1Iife<:t.ed
6. ",cova ry usually by 2-4 wka aller progn!!IIIion stops, mlly btl delayed
by \WlnlbJr(mo.t pat ienu TOOoYer functionally)
6, ll uLOnomiedysfunction (may nucl uale): lBch~eardin and other a rrhyth:nias. poeturo l hypClten:DOIl, H'l'N, v8SomolOr symptoms
1. afebrile al onset of neu ritiesym ptomB
8. van.uUl (not ranked):
a. fever at onset of ne uritic symptoms
b. !J<jver8 MOSOr)' loss with pain
c. progreuion
wu
d. ~es6Btion of pral>"!ssioll without T«Overy
8. 3phin~r dys function (usually spared!: a,e. bladder paralyalo!
>"
NEURO/..OGY
2.6. Guillain.Bam; syndfOlD8
"
f.
eNS involvl!ment (controversial): e., . ataxia. dy!l8.lhria, Babin .k.i aigna
B. CSF !indings: a lb" m ,nocytolog"i<: diSllOCllltion (elevated CSF protein
witholll pleocytosi. )
1. protein: elev'l.o!d
I wk or aymptomt, > 55 O'Igidl
2. cell. : 10 or fewer mononuclear le ukocytHIml
ant.
3.
".nanta
no CSF prol.ei n rin 1·10 ... ka afW r oout (rare)
b. 11-50 mooocytulmi
c, elec t rodiagnolti~.: 8~ heve NeV Ilowing orblock atlOmetime
(may take several weeu in lome). NCV \auaUy < 6O'lt of no ....
•.
l,Ilal, but not in all nerve-
3. fealu," cu tin, doubt on di egno. i.:
A. marked. peraiat.t!nt, lI)'lllrMtry of_aknna
B. pertiaUlnt bowel or bladder dy.funttion
C. > 150 monocytesltDi CSF
D. PMNa in CSF
E. _hBrp sensory level
4. features that rule out diagnoei l (findinga that . uggeat 1M! preHnoe orone ortha
conditionll in the dj([ert0tjl l d jlR'm!Ja. e., . ' " Myck>pq.llly. pap 902):
A. current huacarboo use: volatile IiOlvenw In·hu.ne. methyln·butyl ketone), glue anilftng
D. .cut.. In te.rmita .. n l porphyria (AlP): a diliOrder of porphyrin metabolism. CS t' protein is not elevated 10 AlP. Recu rrent painfUl.bdomln. 1 eri.
&ei ...... eommon . Ch~k urine delta ·aminolevulinic scid or porphobilinogen
C. r~ent diphtheritic infection: diphtheritic polyneuropathy bu a lonCCr la·
\.ency Dnd •• Iower cresa!odo of . ymptomt
O. lead neuropathy: UE weakneu with wrin drop. May be uymmelrical
E. purely sensory syndrome
f '. poliomyelitis: u,ually uymmet.rn:, hat meningeal irritation
C. hypophosphatemia (may OCCUr in ch ronic IV hyperalimentation)
H. botuJi~m: diffi culttodis tioi'Jish clinically from CBS. Norm. l NCV . od . f• •
cilitating .-.sponse to repetitive nerve stimulation on electrodiagnoaliCl
I. toxic neuropathy (e.g. from nitrofU."ntoin, dapsone, thallium or arsenic)
J . tick paralysis: may ca. ...e an ucending motor neuropathy without sensory
impainneoL Careful eumination oft.he scalp for tickC.)
K. long time coune: mey indicate chronic im ... Wlc d .... yeli n . tmg polyra·
d icu lon .. uropatby (Cl OP) AKA chronic relapsing CBS, chronic rela psing
polyneuritis" . Similar w C BS. however symptoms must be present> 2 mOl.
CIDP produces progrellllive, symroetric:al, proximal &. diua l weaknes.s, depre.. ion of muscle atretch noflex .... and ,·.riable soellSOry laq. Cranial
ne""es are usually spared (faci al muades may be involved). Balance diffi·
cullin are common. NHd for respiraWry IUpport i. rare. I'l!ak incidence:
age 40-60 )'TI. ElectrodiagnOltjCl lllId nerve biopsy findings an!' indicative of
dem~lination. CS t' findings .r. aimilar w CBS (_ obow). Most respond
to immun""uppnuive therapy (npeciaUy predniliOlone &: plasmaphereaia)
but relapaea arecommDn. Refractorycuea may be Ina~ with IV gamma.
globulin , cyd"" porin ." ", tolal body lymphoid irradiation or inu.rferon-<>."
The MiIle, · t ·ilher v.nant of CBS indoo... ataxia. an!nexia and ophthalmoplegia.
TREATM£ftIT'
LoununoclobuliNi m.ybe helpfUl. lnKIWc.....,ea rlyplaamaph ..... is haa\.eM!.he
recovery and reduaoa the ....id""l defici L Its role in mild c:aaea Is l,In«rtain. S\.erOids . re
not. helpful". Mecba\1.ical venlilationlJ.>d meuu,"" to preven t aa piration , ... used .. a ppropriate , l n e. 1IQ of raci. 1 dipleril , the eyn muSl be protected from eXl""'ure keratitis.
CNTCOME
Recovery may not be complete !'or H veMl I montlu:. 35'" of untre,led patienla have
.... id""l wealtn .... and atrophy. Reairreneeor CBS .lUr achievina: maximal recovery DCronl in . 2...
2.6. Cuillain·a. ... . yndrome
NEUROLOGY
2.7.
Myelitis
AKA acute transverse myelitis (ATM). The terminology is confusing: myelitis over·
laps with "myelopathy". Both are pathologic conditions of the spinal eord. Myelitis indicot<!s inflaounotioo , lind includes infectiouB, post-infectious, autoim01une, and
idiopathic. Myelop9thy is generally reserved for compressive, wxic, Or metabolic
etiologies".
Er/Ol..OGY
Many so-called "causes" remain uoproven. ImmWlologic response against the e NS
(most likely via cell mediated corolX'Dent ) il the probab le COmmon mechanism. An.iroaJ
model : experimental allergic encephalomyeliti s (requ iN!8 myeli n basic protein areNS.
not peripheral).
Ger"~rally
1.
accepted etiologies include:
infectious and post-infectious
A , primary infectious myelitis
I. viral: poliomyelitis, myelitis with viral encephalomyelitis, herpes
~OIIter • • abie!<
2. bacterial: including tuberculoma of spinal rord
3. !pi.ro<:hetal: AKA ~yphHitit myelitia. Causes syphilitic endarteritia
4. fungal (aspergillosis. blastomytosis, tryptococcosis)
5. parasitic (Echinococcus, cystiterl;Ollis, paragonimiasis. schistQf!omia·
sis)
2.
3.
4.
5.
6.
7.
8.
9.
B. post-infectious: including posl-<!xanthematoU$, infiuen2a
po!IHl"8umatic
physical agents
A. decompreSll ion sickneas (dysbarism)
B. electrical injury '
C. post-irrad lation
para neoplastic ~yndro me (remote effect of cancer): mos~ common primary is lung,
but Pl"Ol!tau!, ovary and reclum have also been described"
metabolit
A. diabetes mellitus"
B pemiei",'! anemia'
C. chronic liver disease'
toxins
A. creayl phosphates·
B. intr8-arte";81 contrast agenta'
C. spin al anesthetics
D. myelographic contl"8st agents
E. following chemonuc\eolysil"
arachnoiditis
autoimmune
A. multiple sclerosis (MS), especially Devic eyndror:"ll'l ($« page 904)
B. following "lac:ciuation (smallpox . rabiea)
collage n v8sc ular diaea/le
A. systemic lupus erythema- Tabk! 2-7 Presenting sympto ms In myellti'
~". connective tissue
B. mixed
disesse
I~", .
_ .ted . .
WIth .. u ~ti.k "' .1 be ""Or'
properly
ro th. ,
u... o>y.M;.
ilb. my.lopothy
_
CLINICA L
A: 34
~nIj ";'~
ATM'"
W/lf$ B: 52 ~nts .,ijh OCU"' OI subaCUlfI tran ...
_myeli ~s""
PRESENTATION
34 patients with ATM ": age of On·
set ra nged 15-55 yrs, with 66'l1>occurTing in 3rd 8nd 4th d"",ade. 12 patienUl (35%) had s
Nt'UROLOGY
2.7. Myelitis
"
"iral ·like prodrome. Pruent;ng symptoms are shown in Tabk 2·1, with otherpresenting
. ymptoma of unspecified frequency including"': fev .. r and rash .
Pr elHlDling leve l
The level . at pretentation in 62 pationu with ATM aro
shown in Table 2·8". The thoradc le"el is the molt common ten ·
sory le~ l . ATM i. rarely the pre.enting.ymptom of MS I_ 306'11
of patiMtI with AT M de"elop MS).
Table 2-8 Level of
MnSOl'Y deficit
PROGRESSION
Pro8l'usion i. usually rapid, with 66% reaching maximal
deficit by 24 hn, however the interval between fint . ymptom
lind mlllUmal deficit "aries from 2 hn·14 days-. Finding. It th e
time of maximal deficit a re .hown in rabk 2·9.
EVALUATION
MY.florram CT &..M.SI: nO characteri.·
tic finding. One pape r reparts 2 patients
with fusiform cord enlargement". High ......
olution MRI with thin CUtl may be able to
demonstrate al'8S ofinvol~ment within the
cord . Patient.hould hIve imagi ng to IUO
compressive lesion.
C5.E: nonna l d ur ing acute phase in 38'11
ofLPs. &roaioder 162%) had elevated protein (usually:> 40 mg%) or ploocytOS i$ (Iym.
phocyte$. PMNs, or both ) or both.
Tabl.2·9 Symptom' " time 01 maJlk
mald.lell
(62 patieotl..-i l h ATM"')
,
EVALUATION SCHEME
10 a patient developing acute myelopa·
thy/paraplegia. espc(:ia lly when ATM is considered likely. the fint uslof choice is an
emergency MRL Iffl()t readily available, a royelogTam (with CT to foI!ow ) direc:ted at the
region of illesensory If!>'e l is perfonned ICSF may be sent in this ci rcumstan« once bloek
is ruled Dull.
T REATME NT
Suggested efficacy ofhigh..:lose s teroid treatmen t in 1 patient .... ith ATMG (methyl·
prednisolone 250 mg IV q 6 h,.. X 24 h ,.. . 125 Ing IV q 6 h,.. .. 24 h,.., 125 mg rv q 12 h1'$
I. 48 hrs. then 30 mg PO q 6 hno. Ulperilld gradually. Rc>&imen sllould probably be individ·
ua liud baaed On ..... ponsel.
P ROGNOSIS
In a $eries of34 ATM palien U willi" 5 yrs follow·up (FlU)"": 9 pal iellUl 126%' had
good rltCOYery (amb",1ale well mild urinary symp&o ....., minimal $eraory and UMN
l ign l ): 9 (26'110) lIad fai r recov ....y (functional g. il with $Orne degM!! of $p8sticily. urioary
u.rgency , obvioua .. ntory '[1"5, par' pereaill; 11 (aN) poor (paraplecic. a btent sphiDcter
fIOIItro\); 5 (15%) died wilhi n 4 ..- or illn ...... 18 palientl (62':1. of survivorsl becama am·
bulatory (in th_ cues,.1l c:ould walk with support by 3-6 ..-).
In a Hri " 01'59 pllienU-{FIU period unl pl!('ified 1: 22 (37'11) ....d ,ood recovery; 14
(24") poor; 3 died in K U\.a stage (ru pinotoTy inl ufficiency in 2, Hpli5 in U. R«overy oc·
curred between 4 weeki and 3 _
after on$et IfI() improvement oc:curred .fter 3 rnos).
2.8.
Neurosarcoidosis
SI.rcoidosi, i • • gran",lon,atou. di _ that il ulu,Uy I y, terni.:, and may indude
the CNS (_
lied neuroaan;:oidotl ia). Only 39& or cue. have CNS fiodinp without IY.'
temic: manifut.alion. ... The ('8uHorthe diM_ i, ",nknow n. An infeo:tiou l Igeol il pot.
NEUROLOGY
.ible. Organ~C(jmmon ly in~(Ilved indude \ulllP. ~k1n , lymph nole.. bones, eyn, mUliClu.
IlIld parolid glands'".
P ATHOLOGV
CNS lall:oid().9ia primanly InV()lvl!Ii the lep~omeningea, however parenchyma l invpaion often occu.rtI. Adhesive a rachnoiditia wilb nooule form.t.iOD may al-o oco.:u r llloduJ~
have" predil~iOll rOT the pc., nerior £(658). Oiffuse. meningitis ~r roellmgoeneephalitis
may occur, and may be 1II011! pronounced al the balll.! oft bl! brain {bR8IIl meningitia l Bnd
in the aubependymal region of the third ventricle (including the hypotbalamwo ).
Cons tan t min"Oll~pic featW"1!5 of neurO$&TCoidNi. in clude n~a;,eati ng JlTllllulomilS with Iymph<l<:ytic infil trates. Langhans giant .,.,lIs roay orm,y not be prelieM
E PIOEMIOLOGV
Ineide ",:., ofs.ar(Jlidosi6 Is - 3·50 "'IsesllOO,OOO popu lation; neu rOlla ra)idotlb O«UTI
in _ 5% Or(;llM1l (reporud ran Ke: 1_27'1» . In one • .,ries, the median 1ge monset of neuro.
l"(ie symptoms was 44 ~arl.
CLI NICAL FIN01 NGS
Clinlcallindings incl ude m ultiple cranial lIe .... e pal&iea, pl!flphe ral neuropathy, and
myopathy". Ottasional1y the le8ionl roIlY prOOuce mauelfe-c:l1'. IUld byd rocephalW! roIlY
res ult from adhe,,;vB basal ara~hnoidili$. Patiant>lUlay have 10.... grade r.. ve r. lntr&CrBoi.
al hypertension i~ common and UlAy be dangerou s.
HypolhalaJDie invol vero!';n t may produce dillorder~ or AD" fdiabetl>5 tru.ipidU6", disordered thirst).
LABORATOR Y
CBC: m ild
leuk~i.
IltId ",,,lnoph.llla may o<:cu r.
Se r u.D;l ang"iotenai n·co nvertiPi eo~ym" fACE): abnormally elevlto!d in 83% or
patienu with active pulmo",,!), aar<:oid08is, but io only II % with in8ctivD diJlellse"'_F~llle
posi tive ral.e: 2-S'IIio: ma) ..180 be eleval.ed in primary biliary cir:h08;s.
CSF : similar w any 8ubacuto! menlogitis: elevated p,et;SUN!, mild pleocyt.o8"ia ( 10200 oe:llslmllll ) IIIO$tJr.lymphoq'tu, elevated protein Cup to 2.0!lO mgfdl), mild Il.ypoglyc·
orrha~hia ( 15·40 mgldl), CSF ACE is eleva ted in .
Or CaI" with n eU'0$8rcnidoai.
(nonnal in patienu .... ith lIa",oidOllis not involving th6 C NS)"' . No organislllS are /"IIWV·
e red on clll t uTto, gram 'tain.
5-5"
DIAGNOSIS
Oifferentiati.nij ¥NnulolllatoUll8ngiitil (GA )
Table 2-10 Oltfe. enllal diagno-
froUl rlellTosarroido&is that invo]"1!!1 only the CNS ClIn
be dane 011 histologic &riteril: the in n ommatory rail¢>
lion in l,rt"Oid08i.t! il nat limited to Wle region imroed.i·
sis 01neurosareoldosla
au.ly ~uN"Ound;n G bl~ V_18 "" It;8 in CA, .... he ro
""len6;v8 disruption Qrrne vueel wall mayo<:cur.
Making the diap"";5 is relatively BII$y when
systemic involvement occurs: chara cteristic ti nd",~
on CXR. bioPIY of ak.iu Or live. n<>dulei . U\ LI.iIele biopey,
leTVUI ACE a""y .
holato!d neur~lra)idosiI Ul'y be Ulore diffi cult
to diagorn.e, alld IOsy requi re hioP")' ($o!"t' bd(!w ).
BIOPS.,.
In UOCfrt8iO~aH', biopsy mQy beindltated. Wheneverpo$aible, MRl a hou ld be used
to localize a SUpl"1ltentorial region ofinV(llvernen~. and biopsy should include alileye" or
IJIf!ninges .lJld QBrebro l cortex. Cul tlLr1!S and ~t/lin.s for fungus Ind acid·fMt bacteria ('1'8 )
8hould be performed in sddiUon to m icrwcopit exalUinMion.
NEUROLOGY
2.8, NeUrMOrcoidoo;$
TREATMENT
AntibioliCll hB~t not been proven!.O ~ofbentfit. Steroid. ore bc!n!':fidal for 'YI!.emie
u WtU •• nellrolo,ic involvemen t. Thtr. py with cycIOlpori". m.y allow a redoclion in
lteroiddos"e in r.fn ctoryuIQ". Otbtr I..., well ~~IId.ied trutman tll : methotl'i! "~' eytaun. CSF shunting Ui indk,~ if hydroceph,III,dtvelopa,
PROO NOSIS
UIu.Jly I bftlign disease. Periphuflllllld CtlUlilll nervli palsl" l"itWVer,lowly.
Vasculitis and vasculopathy
2.9.
Th. vlkUlitides ora . IJ"lIp of diaordtrl cho ... ~~riud by inflammation and MCrolia of blood v_la. VaKul;ti. ma, be prilllllt)' or IeQ)OOlry. Those thOL n'ay affect lhe
CNS Ire lilted in Table 2· 11 , all ofthel6CflUJe WIUt 'Khemla (even ,,/\ar the inflarnma tion it! quitlCl!nt) thlt mlY raup iJI elT'eo:t from nauroprllXi, tQ infa rction
Ta ble 2-11 Yueulillde. lhal
!(£Y:O."""""""'''' ....._
the eNS'"
: •• _''''''''''''''': >-t.'''''''''''''''ICI1 . onIr~_~
SAI-I.~~
_HCIIon"..
~I
Iot_tDIlia
J>AN"
IfIOUI>"'_~......,-...ybt~
2.9.1 .
Giant cell arteritis (GCA)
f
TKey fuw ....
formetll D~" ~fured ta al l.emporal arteritis
d ' romc vallCUht it!oflac]{e and ~um celibtr v_la, primlri l, LDvolvlnSeTl'
nill b",ncl;>ea of Ole Imnft trisioS from the .0000e...::h
age,. 50 yean: atrKU WOme<l IWlet .. otten .. Ultn
important poIIIIiblalal.e romplicatio ...: blilldneu, atroka, thane..: IOrtic lna .. ry~m. and aortic di~ioo.
temporal artery bioplJ' il rec'Ommtnded (or.1I Pl'Uenta IWll*ted ofOCA
rortlCOSl.erold. an tlledl"Ur of choice rer IrflIIlmenl
AKA Lcmpo r l'lrteriti. (TA,) , AKA crlltllal.rl.entlt. A chronicJrIlll.. lol7llt.o ... Ir_
I-tribS ofunltnown etioloo In.oMnS pnlUllrily tbecrtlDi.1 brandlftl or lha Ionic IIl'dI
(especillly Ih' uterTIal urotid af'Wry (ECA))". wluch Iruntl't'llted , mil)' IeJ.d 10 blind·
ntal. Talcay....·' art.eritit it . imill r VI GCA, but t.tnds 14 affect Iltse . rteries in )'Ounr
.. om~,
I
EPIOEIdIOl OO 'r
Stan ,lm Ollt e.:dU&i~1y in CauCII.;allt:> 60 '"' &Ie (mean'~ of o....,t it! 701. Ind·
denc:.; 17.8 ~r 100,000 paople" M1yearaold" (r.np:OA9·231 Pr .... a1enc.: _ 223 (aulOp., incidence may be much hiKrlIl"rl" MoreCODlOMlll in n-orthtm litiludea Ind lmoll,
2.9 VpeulitiJ and visculopalhy
NEUROI.OGr
individuals ofScandintwiaa descent". Female:male ratio is _ 2:1 (reported raage: 1.05·
7.4:1). 50% ofCCA pat ients 11180 hllve polymyalgia rhellmatica (PMR) (."" PQHe 61).
P ATHOLOGY
Discontinuous (so..clliled "skip lesions") inJlammlitory reaction oflymphocytell. pl asma cell s, macro phages, :t giant cells u fabsent , intimal proliferation may he prominent);
predominantly in n,edia ofirlVolved arterie~. Aruries plllferentially involved include the
ophthalmic and posterior ciliary branches and the entilll distribution of the eKternal ca ·
rotid system (ofwhith the STA i8 a terroinal branch). Other arter ies in the body mal' be
involved (reported invot-'ement ofabdominal aorta. femoral , brachial and mesenteric arteries a .... rarely symptomatic). Unlike PAN. CCA generally s pares the renal arteries.
C LINICAL
Various combinations of
Table 2· 12 Signs and aymploms 01 GCA". T7
symptoms of giant cell arteritis are
FreqU8fl1
listed in Tabl~ 2· 12. Onset is urual·
j> SO'4 01 ca_) jll).5(l'!{,ol c_) « 1,"- of cases)
Iy insidious. although OCCWlliOflaliy
-.i$Ua1 sympIQm$
it may be abrupt"".
' ~'-~~
~alMIlly
~11o$S
exlremi!y daudicalion
Details afso me findings
\Dng~ claudica1ion
,-~ !8'/e( (law gllOe)
1. HlA: the most common pre·
prounalmyalgi3$ earpai:l
senting symptom. May be
jaw claudicalion
nonspeciIicor located in One
I ~a:ial pa;.,
or both temporal areaa,
scalp lenderlleSS angina
forehead . or occiput. Mal'
be superficial or burning
with parolC)'smBI hmcin ating pain
2. symplQllul relating to ECA blood supply (Itrongly sugge~tive orCCA. bu t not
pathognomonic"):jaw claudication, tongue. or pharyngul muscles
3. ophthalmologic sym ptoms: due to arteritis and oodusion ofbranch.es of ophthalm·
ic artery Or posterior ciliary arteries
A. 6YI"PtomS inclllde: amaurosis rugax (pre<:edes permanent visual loss in
44%), bUnMa$!;. visual field cUtl. diplopia. plOt;'. o<:ullir pain. oomelll edema. chemosis
B. blindneu: incidence is - 7%. and once itoccutll, reeovery of'ight is unlikely
4. systemic aymptoms
A. nonspecifk constitutional symptom!: fever (may present as FUO in 15% of
cases). anorexia. weight 1088, fatigue, walaise
8 . 30'l0 have neurologic manifestations. 14% are neu..... pathies including
mononeuropathies and peripheral polyneu ropathies of the annS Or I~
C. musculoskeletal symptoms
1. PMR is the most common (o<:curs in 40'l0 ofpatienta): I« page 61
2 . periphersl arthriti s. swelling &. piltiog edelIlli of bands &. feet in 25%
3. arm wllldicatioo from ,tellOSi. of subclavian and 8lIillary arteries
D_ thoracic aortic aneurysms: 17 times as likely in GCA. Annual CXRs are adequate for screening
5. lel3tpo<al otter, ,,,, on phyeical exo.minntion may oKhibit tand .. me ... . swelling .
erythema ..... duced pulsations, or nodularity. Nonnal in 33%
6. the presence of systemic symptowscorrelates with a ~ incidence of blindness
or stroke
Oifferential diagnosis:
1. periarteritis nooOlla (PAN):
PQH~ 61
2. hypersensitivity vasculitis
3. atherosclerotic occlusive disease
4. malignancy: aymptom, of low grade fever. malaise and weight loss
5. infection
6. trigeminal neuralgia: _page378
7. ophthalmoplegic migraine
8. dental problems
"".....,
"'"
'"""'"
.-.
''''''
&""
NEUROLOGY
2.9. Vasculitis and vaaculopathy
"
E VALUATION
Laborlltory . tudi e.
I. ESR > 40 mrnlhr (usuIlIy > 50) II)' Wnwr,,"," method llf > 80 IIIm1hr with .bcJo,·e
CtUII<:8J ')'IIdromu, highly '''8I!el tlVl! orecAl. ESR i. norlllal in up to 22.5""
2. C·rellCuVi protein: 8uDther ftcul.ol phllse reactant thlt" n,Ore iII" S;t ;V!!. \hln ES R.
Hu th e .dvllnta84' thllt it o:.vo he perfon ned on frozen Olen
:1. c a c : ,,'.y I how tn.ild ao,moc hrom;e 8uemi"~
ot . rhe umatoid f.~tor. ANA . and Il!rum eomple.tnent ..... ally oo rmal
6. LIT. I bnomuiJ in 3O~ (usua lly elevated !llk.,li"e phoeiphalll.te.)
Ii. 1.e1.1I1"ot rheuma toid ractor and AN A "'" usually "w,lll;v.
7. to!mpor818rtery allglollTlPtr.y not tr.elpfuillngi0lrtlphy elsewMrl! Indicated if Sui·
pldofl "flll rgt! aI"Wry ili vo lv,",,<,nleltlllll
8. CT' uI"ally 00\ helpful. oce report dutriberl c..lci6ed area colTlllponrline to the
temporal ''''I",riu tJ
9. U:mporal arl.lry biopsy: '"' ~1f>W
TEM PORAl AItTE AY BIOPSY
Sensi tivity and ~pl!l:Itidty I re . ho... n in Tab/I
,./.1.
Indication, and timini
rlblcl2·'3 . ~.mpo,''''''''Y
Current reo;;ommend8Do .....: IOlmpwII artery biop.sy ill 8IL pa t.ient-J , UBpecloPd af I\avHl8 GCA".
Preferllbly. biopsy ahould bto dane bl!fore t retltmenl is inlti nt..,d ... Ho... """• • pAlhologie cha",,,, bI!
.....an after mOre tha" "2 weeu ~fthn-I I'Y"', th ....efor-e do
" ot withhol d steroid& to await biopIy.
Technique of tempora l a rtery hiopsy
Bioplly of the coutra lawral .ide if til<" n ..:n side 11 ~~tl.-e III tun when!! ciiDlul
lIuijplcioo is high innullell the yield by 5- 10'A-.
TREATMENT
No known cure . StMnids o;an produ .... ~ pl.o"'atic n!!lidand ueuIUy pr....ent blind.
(proc,..:t5ion of DC ul • • prohlenlllU--4a btl! _flu i""titution af . deq"ataateroid.ls
rare). Tot.llilyblind pauenUl or t110fie witb louenaodine partial VlJwoJ 10M ani! ulllikely to
nI!~pond to any tRUmeot.
t. for mo,n. ~.;
A. IItllrt with ~n.91tt:. 4().6Q mlfd PO divided BlD-QlD tqild doli", is "I,,·
I lly HOt ef'ff!d ive in Initillmanag",meut)
B. ifno reapoulI! aI\u TI! bn:. and diap108i. teTtlin, Ito 10·25 nlj QJD
C. OnCO! ""'POOBe ....:un (" suaUy ... ithin 3·7 days). giv," ,",,:..n. doH 81 q AM
dole. for:l-8 wet!u unlil l ympwoos relOlved and ESR oo""aliz... t~1,U"!! in
87~ oflNltienu with",_ ~ wftOka)or . u.bili:es at < oto..;.G.-nnVbr
D. once quiHc.mt., a if1Io\Iual u.per is performed lO preye n: encerbe.tions:- re-d\lee by 10 mgldq 2.4 w"klI to 40 mild. ~n by5 mgId 02--4 wb to20mgld.
then by 2.5 mgld q 2""", wu lO 5-7.5 metd ... b~b i& IDIIUll.ained for MYn-1I1
manu, •. fol lowed by I ",gld de(:l':'menllq 1-3 "'1111 (... ulIl .... n~h af tre31""",1
il &-2 4 m05: do ACll 00 llto.roida "~n ES R normaliau)
E. If Iym ptomt recur during trtaltn.tnt, prednisone d_ is tf:mporarily in·
Cl"tllaed until tympl.OmJ reMlv, (]JQ1.ted riM in ES R is lIot lumcie n~renon
to inc..... ltf:.-.idl")
F JUlUlflUlhou ld be foUowed clOHly for . 2 ~atl
2. '" .e~ertly III pltittnu: methylpredn1'lOlone, 15-20 mg IV QlD
3. II1ti_l\lllnt thenop,.; cont.l"OVeni.J
... .Cllte blind"... (on51': witbin 24·36 h,..) in Il*tien l with giant ",,1I11rt.eriUI:
11.. colI.lder up lO 500 me aleth,l'tpndnBollllIe IV over SO-flO ",I"" (no eontrolled
studi" thow I"e\WNI ar bhndnelMl)
B. lOme bave used intf:nnitwnt inhlllatlOn " r MII CII rbon dio,,,d~ and o~an
n eolll
OUTCOME.
Complication. of IW:roid tilen py occur in _ ~ or p&t ientl\mOlltare not lif. Ihlll!at·
erunl. Ind loclud. "eneoral DOllI plll!"t5lOn f"'cture.ln _ ~. pepUc "I.... diM... ln
"
NEUROLOGY
~ 12~,
proximal myopathy. cSUlrscUl. exacerbstion ordiobetes: also see Po.9iblt cld~je­
'''''''!litLt tI~t.of,teroids, P~i:" WI.
30-50% of pauenta will ha"e sJ.I(In\.<ln<!OUs exacerbations orGeA (especially dllnt;lg
the
yea ... ) .... gam.lus ofth tonicosleroid I"<lgimen".
.
S ......... ivaJ parallels that oftbe ~neral popuIRl;on. OnselafblindneM alter initiation
of steroid therapY;1I rllre.
finit 2
Polymyalgia rheumatlca
2.9.2.
PolymyaJgia Theumat;c:a (J' MR) and giant ",,\I arteritio (GeN i_fXJR£1i8) may be
diffe rUlj pointl! on /I condnuum orche ume disease.
Epidemiolo gy)'
Both GCA & PMR occur in peopl .. ~ 50 years old . The incidence increaaes with age
and peMa betw~n 70-80 yeat8 and is higher a~ higher latilud"".
Polymyalgia rb e umati cs (PMR) "
an inflammatory cond ition afunknow n etiology
clinical rna",clenst\a
A. aching and morning stiff/ieM in the c"rvical f'<!gion and shoulder & pe!\-ic
gi rdles lasting:> IlDOnth. The pain llstUllly increases with movement
I . sh oulder pIl;n: present in 7<1·95% of plltients. Radi~ te& t.oward elbow
2. hip & neck pain: :;O·70'!l>. Hlp pain radlat@$ eoward$ 1Lo_
8. age,. 50 yN1"8
C. ESR., '10 m.mI"hr (7-20% ha ve normal ESR")
D. W!ull1!y respond" rapidly t.o low dO!le corth:ost./!roid. I. 20 rng- predn',,'meiday) utlHlow
E. IYlt.eIl\lC lympt.olTl5lpl'e6t'nt in . 33<r.): fev"t, malaise Or fatigu~. ano"",.i,
and weight lUllS
prevalenct': mort' common than eCA
A. 5001HlO.OOO'"
B. I case per 133 people .. age50'"
favorable prognoais
TTeat m ec t
PMR TespGn<ill to eitber 10 low dosel of sten)id.o;l' ( 10·20 n\il prednisone/dayl or
sometimes I<> NSAIDs (Iesponse t.o ate roids ig much nlO"'" ",pia). The in it;lIl dose of Ste·
roids is maintained for 2.... weeks. lind then hy. 10$- oftheda;:y dose every 1-2 weeklY'
wrule observing fo r , ;gnl "fGCA.
2.9.3.
Other vasculitides
PERIIIRTERmS NOOOSA
AKA polyarteritil! nodol8 . Actually a gl"Oup ofllecrotidnK v~ulitjdes. ineludine;
dauic periarterili! rwd0811 (PAN): II multil!yn.em disease with infl:unmatory ne·
0I"0Il;&, thrQm ......,~ ( ocdu.ion ). Dnd hCnlorrh"so or Drt<:riDll and arteriDI"" in ow~ry
olgan except lung & ~pleen. Nodules may ~ palpated along medium sized mu&cular art~e •. Commonly produces monooeu';t!. multiple,.. weigbt!""' f"wer,
Bnd tachyca rdia . Peripberal nerve mllrUfntatioO!l Ol"l! attributed 10 arterilicocelusion ofvo"" OOrvonirn. C!,;S rnBnifestatlOlIS are uncommon . nd indude HlA .
$.ilUTt!! . SAH. felfnal hemorrhages, . nd eVA In - l~
• aJ.Iergic angiit", and granulomlltosi s (Churg-5trn uS!l syndrome)
systemic n""rolizing YII8Cnlit;s
These pa t;enl.ll do better when t~lIt..ed with cyclophospbllmide rather tban "erai""
WEGENER 'S GRANULOMATOSIS
)\, systemic n<!Crouilng granu!omat.ous "flarulitiB Involving the respiratory t ract
OWl" - cough/nemopt)'lli., snd/or n_1 airwal'l' - laTosanguinou! no""J d rainage ='"'p.
Ull perforation - characteri~lie "i8ddle DO'" de.formity") lind freq"ently the kidney. (no
ref"Jrted caBej; of kJdney inVOlvement without 1'f5pirotory.... .
NBUROLOcr
2.9. VRllCuliti! and
vB5fillop~thJ
"
Na .... obttruetion and e,ulting ... the ulual initial findill8l1. Arthralgia (nOt true
ill present in > 50'1&.
Neurologic involvement .... uaUy eon$isU of cl"lUlial oerve d,..runetion ( UIIUIUy II, 111,
IV, &. VI; 1_ often V, VlI, &. VI II ; and leal t commonly IX. X, XI, &. Xli) and peripheral
neuropathiU, wi t h diabetn illlipi du'(OOX.lionally pt«edingothet8)'ll1ptom. by up to 9
montha). Foealle.ionl of th e Drain lind spinal «Iro occur In. frequently.
.rthrit~)
Differenti.l diagnosis indudu!
"Ia tbal m idline I/Tanu lo ma" (may be similar or identical to Jl<)Iymorphie relic>ulosis) may evolve into lymphoma. ~boy cauu r... lminant loca l dutrud;on ofth.
nasal tiu ue. Dift'erenlilltion il crucial II thill cODdilion ;1 treated by radiation;
one l hould avoid immune.uppruaion (a.,. eyciophOllph,mide). Problblydoet: not
involve troe granulom... Reoal and tTacb •• 1 involvement do nOl. occur
fungal dille..e: SpOrothriz fChfncitii &. Cocci dioidet may ca\IM identicallyn.
drome
other vasculitidu: up«i~lIy Ch ul'1-Stnu.. I yndrome (uthma and peripheral
eosinophi lia usua lly _ n), and PAN (,,"anulomas ulvally IACki.ng)
LYMPHOMATOID GRA NULOt.'-"TOSIS
Rare; alfecu mainly the IUlISI, akin (erythemalOUs maeulu Or .. ndurat.ed plaequet
in 40%) and nervOuS Iy,tem (CNS in 20 .... p"'ripberal neuropathiell in 15'1» , Si nuee"
lymph nodn, Ind spleen are usually lpa red.
B EH(:ET'S SVNOROME
Relap!;ingoculaf lesion. and recu!l'entoraJ I nd genital ulcer., with occ.a.ional . k.in
les;ons, thrombophlebitis, and arthriti' .., H/A ooeur in,. 50". Neurologic involvement
includes peeudoturnor, cerebellar ataxia, paraplegia, aeilurea, and dural linus thrombo.i•. Only 5% have neurologic aymptoma as the presenting c:omplainL
86% bave CSP pleocyto&s and protein elevation . Cerebral Ingio(raphy is ul uaUy
nonnal. CT may show focal areal of enhancing low deMity.
Steroi<b usually ameliorate ocular and eereb'alsymptoma, but usually have ooef.
recton .ki n 100 genitallesionl. Uncontrolled triab ofcytotoxic agentl - lOme benefit
Thalidomide may be effective (uncontrolled studies), but carries risk of &erioua adyerse
effectl (teratollenicity, peripheral neuropl thy ... )"'.
Although painful, !.he disea6e il ulually ben ign. Neurologic inYIIIYementportenlb a
worse p'ogTI06il .
I SOLATED eNS VASCUUTIS
AKA i!lOIAt...:! IniP ili. o f the CNS. Rare (~ 20caaa repol'l.ed" &II of l 983); limited
\.Ov_11 ofCNS. Small veeel vuculiti. i. ~ alwlYI praent - segmental inflammation
and necrosis OflmlUleptomeningeallnd parenchymal blood v_18 witb lurrou.ndi ng
ti.,,,e itchemil or heO'lOrmlp".
PRESENTATION
Combinltion. ortYA, eoor"lion, dfmentia, I nd lethargy. OccuionIlly WilU' H . Poell and mullifocal brain dilturbanceotCurs in,. 8O'JI.. VifllalIympt.llllllIre frequ.,nt (se.:ondary either to involvemt nt of choroid.land retinllarteriH. or to involvement of villlal
cortex - vil ual hlllucinatio.-.).
EVALUATION
ESR &. W8C COWlt Ire usually DOrm. l. CSF DIlly be normal or hl~ pleocyta.il
andlor elevated protein. CT may ahow enhancin( areas of low denai ty.
AngiOCrlphy hequ.ind br di'enOl;a>: characteri.mally . ho,.... multiple area' of
Iymme\.rieal nlfTOwinll ("ltting ofp"'.rlt" cooflguration). If nannal, it don notuc1ude
dilgnotil.
Hiltolop:.l diagn06i1 (recommended>: III bioJMY materi.l.hould be cultured. Brain
parenchyma biapey ;nf~uently , how. vl.ICuliti .. LeptOmt ninpal bioJMY invariably
involvement.
.mow.
"
2.9. Vllculiti. and vllculopathy
NEUROLOGY
H YPERSENSITIVITY VASCULITIS
Neurol~c involv.ment if not I prominent fe~tl.Ire ofthis gl'j)up of"8MUlitidl!$,
whIch include:
drug induU:d enel'l1c V.~uli li.
cul.neo .... V8KUlill.
HrulTl siwOII': rna)' - ancep/llllopolh)" Mbu ...., coma, p!!nphe'!ll l>~urol"'Lhy
.nd br8th.ial pluopa tb,
H~noch-&:h6nlein purpura
D Rua INDUCED VI, SCULms
A numlHlrord",i' !l.""".lIOCieied with th"d~elopment of~".ebTl.I vlUlCUlit ia.
,odude metfulfllphellolfline. (".peed"), tOeIIine.{fl'llok vI\SCuliti. ClCCU ..... but is nlJ1!). he ..
n,ne
oln and ephedrine.
2.9.4.
Fibromuscular dysplasia
._i.ted
A vnculopa thy (oogiop.thylatrectilll pnm anly brllndMs o(!.he eoTta, wltll reo.1
nrtery involvement ill S5'i11 of caH. (thl. motl IlOmll"llln .Itel.nd eIImmonly
wIth hypertM5101>_no" di_1e hI' an i.otldenee of ~ 1'11> •• nd .esulls in mui t ifoaolll ......
rial cO"'l"lrietions ,"d i,rne"""nirlc regiol'l5 of.oeu~,n.l dilatallon,
The le<lOud mostllDmmollly involYed ,;UI;5 the c:&n>ical illt.emal carotid (priml rily
nenrCI_2), with fibromu!iC1.ll&.r dyspluill iFMD) 'Ppe.rinlon l \t.ofearotid llIriograml,
making FMD the &eCOnd molt ~mmon causeofexLr&crani.1 clrol.id 'UI~. Bllaleral
cervicnl lCA involvemrnl O«UI'II il> _ ~ or~. SKof pal"nla wi lh Uon)ljd Ji'MD
haye renal FMO, Patienls wilb FMO ""ye an Inc:rnted rUk d ontu"ranill I"'U.,..""
lind neophu;ms, ami ~ probably II higher ri&k of tllrotill di56edion
ETIOlOG Y
The ItCtual etlolo1O' remains unknown, alt.hout:h«lncenital df~ of the media
(muscula r layer) and ir.lem&i ~a.tk layer oftbe sr\eria bar bee.;> identified which mIoy
prediSpoII8 the arteries to injwy from otlll!T"o<riw ~I-tolel'llt..d trauma. A lulh ramllil,1
rftl~ of strokes, HTN, aDd rnllTai..e have supported th~ ,,,""lion thet FMO is an autoIIOmal domillant lrail"';!h reduced penetranee in mal ......
ANEURYSMS AND FI8ROMUSCtJU.R DYSPlASIA
1'be reported incidenNof aneuJYSln' with Fr.to'" I'8Dg.. from 20-50'11>.
TabS. 2· 14 PrevIOU .
CI",
.ymplOAW III 37
of aQfloc:rlflll' FMD'"
PRESENTATICJN
M <>It f)l.lielll.f hn,·. recurrent, multiple ftym plOml
Ihown in Tabl~ 2-14 ,
Up 10 so.. of patienta p......,nt witll epiaode. of transient
«rIb' ll itdlemia or itlr.,.ctlon, Haw"ver, FMD IDAy also be
an incidontal ttndi"l and lOme o:a...Hhaye beenJolkrwed for
IS ye.1'II WIthout recurTt"nte oflachemic .ymploml i~tinll
thll F MO a,sy be. ",1~livel)' benifn condition.
Hud lche. are ronunollly unilat..nllnd may be m;'"
taken for lypical mignllne. SynllOpe may be cauoed by illvotw.men~ofth" carol.od .;nUl_
Homet'••yndtvme Ottul'll in _ N ofCII ..... T.waw
ehanen on EKe DUly be seen ill up .... on.thlrd olca.sn, and
m.y be dUI to i.nyolvemtlllto! the roroo"y arteries.
OW;NOS<S
The °l6ld·.tandll\l" for the disl_1I orFMO i. the Ingiogram. TIwo th ... a nJiognphic I)'pes of FM D'" INI .hown In ThM. 'J-16.
TREATMENT
Medical t hHIPY Inc:luding entiplat..11I medicatloll (e." 45pmnl " .. been TeCOmCMndecl.
NEUROl.OCY
Dil'«1 5urgic~1 trealment;.
JW'oblem ridden due to the diffi.
tultl_uon (hith ca rotid . rury.
nU. the ban of th. al<uU), a nd
the friable ~turt ufthe ~Im
making anU!luno,,,. or o .teriOI~
my d o.ure difficu lt.
TT. ... lum'na!8ngiopl..
has achieved 110m!! degtH of l uo~. Ca rotid c .... mou.linul ••
and a rLi!tiall'Upture ha,". been
r.ported .. complie.t/OtlL
T. bl. 2·15
OlfMO
t,.
2.9.5.
Miscellaneous vasculopathies
"
I
CADASIL
t Key futures
clinical. mignllnl!a, deJ;1anua, TIAs. ptyeh,uric d iilurbanc:eI
• MRl: wllilt ~t"'r abnormahtiu
• autosomal dOI1l",an~ ir.!w.ritllr>Ce
• anticoaglliantl controversl.l. ,tneBUy di$CO\l.~ged
An a,,",nym enr ClTebrlll .... ulO$Omyl Dominant Artuiapll1hy with Subeorticallnf·
a r~.nd Lomkoe,""'phalnpath,.. . .... f.mililll d;~ with onnt in ea r;y ad ... 1thood (meDn
.ge lit omet: 45 '" II )'nil, mapped to chroflllMOfDt 19. Clinical and neuroradiglogic fca IU ' " IN!limilarlOlhoIe aeen wilh mullipielubcorticul mro~U from HTN, ucepl t here
II no eviden~ofH1'N. The vlISCUloplltlly i5 disti nct "om thot Ieiln in lipO/lyal'nasis. ar1.eri000erosi••nd amyloid lI.IIgiopal hy. and cause.s thiek. ning of the ~ia of lepl.ol!leniniNl ""d penOI1lI,,,,, anerie, m-.uring 11)0.400 "," ," dia.nw!Li!r.
Clinical inYillvell>ent: rerurnontsubmnkat io rlln:~ 184~), prawns;v"' .... u"pW'5e
dtmentia (3 1"), l1IigTaine "'ito'! li' UI"lI (2'~), a nd depress.on {\tOOIi-). AlIl}'mptomaU( Dnd
IS'l\ofUympt.omalie patlentil had prommenuu bcort.ieal whit..·matterand basal ,anlll ill
hypennten$it;u on 1'2",1 M Rl.
Trutment: Cownadinf>is ua.ed byaome.
2.10.
Vascular dysauloregulalory
encephalopalhy
This H<:tion encol1lpa$5fta IrouP Dftnn!phalopathiet that ma,y be I1'lati!d to dl.".
dered vai<'u lar autorqulatioc-. Et.ologies ami find il'll' iodud.:
1. tho~e due IO ,~ ...10Dd prfIMure .~vationa: imqilli "Udlellhow I)Im metric
(onnuentiesionl with mild ",a", ~tfect Ind pII t.(:hy "",ha_t primarily in the
, ,,beort.iCIII wtul.e matllt" of the awwJJl!!la"' {pouiblJl baaitule of limited .ym·
plthetk innervltion in the ~rjJlLcir:tuJ1IJ.lwl} whie'" may "rod"," coniCll1
bhndMM
.... hype rlf'n.;"", ""'c"ph.lop,thy j " may Ott'" w.th IIUIl ipant h~TUn.ionl
8 peripartu.,,; lluociauod wit h ferebrlll ed'm.'", on"", t'rnponlry, but (pi"manen~) infarctiOM IllIG OttUr
L may p,_n l (' .1. with blindnus) du tio ~ pre",. lIty complicated by
p,.edlm pua Or eclampsia"
2 rn.y develop 4.9 dlY" pO:lt.ptt rtum . nd ,n',)' be e_l~tt-d with
"._pMm"
2.
..
C cyc1Ot1porine lO~idty
uremic tllH phalopoth,e!o: imalJl ng iI"ditsshow multiple ..... or.ym~trieede,.
rna in the bani ""'glie. with Ie\'ert _ _ devdop11\i (oaollnfam. WIth or ",i lh.
0"1. hemoITha~ 'rh_ diNOl'derf lire asliOCiated w,th elevate:l 6tJN .nd im-tud ..:
A. u•• miD
2.10, Vlllnl iar dYliulOregu latol") eneephalopathy
Ni:UROLOGY
B. glomerulonephritis
C. hemo!ytic. u,..,mic . yndmme (HUS)
O. thmmbotic thmmbocytic purpura (TTP)
These pIItienUl may present with headache, seizures, mental status change.s and f.,.
cal neurologic deficit. Intracerebral hemorrhage (le U) may occur.
Tre a tm e n t
Disordered autoregulation mandates tight control of blood pressure to avoid hyper·
tension to reduce the risk ofICH.
2.11 .
I.
1.
l.
••
S.
6.
1.
S.
References
en.u......
Cool... """, o.ff.~.'i.1 di,,,,,,,i, of ...•
"'<0'; .... di,.,.,. •. JAMA 1": 30111.6. 1917
FI.ml.. I(C. A"' ... AC.i'd<TS<. R C:O' ..... '..:
0." """,0<16 ...1,,,",,,. M 01. c~. Proe lO:
IO')l·III7.199J.
l"J>O"I>ki Z J. 0."' ...... (""'''' <..... II<1II .. SUI ..)
JAMA nl. 1719·92.1987.
1'0'"1>0' p.r...."' •• M. R_,'M ,1. . . . .1, Orl.ri ·
• '" .. hOopi .. II'~Qkk1 po"""", O.1«>m<J >nil pl<'
diclOr>. J "'" Cm."Soe .2: I!O')·I~ . 1994.
1'<,...... RC: Ae.,""QllfII""".I .... " Donl mi_
iI I","'mo.,io. r..\V811 M.d92: 141 ·1 . 1m.
Hu le".C M.I'.MI N L. C,.m B J. E.aI.".,. oJ,*"
«MI1bopoin ((II" ""' di""",;, c l4< ....... ' ... ,!.«h
N,.,0149· 28·ll. 19111.
SP.T ....... IO RJ.O'''I'"'''''OC1icldoftnln
tMq>sY '" ... """"',....,..., •• d _ ". N.....
...... '1'41 ·123·)(1.1'191.
Fan,.h P ... . _ I 8 . ... >Wo<I><. ,. ~i<:"''''i'h
bt... I."""",, A >loo:Iy of III po,loN>. No",oIo&)
4): 1611.8) . 1m.
1o.""..
9.
W.l<hI(M A.U.i ... SR:M ...... ,,'N<I. t«l .....h
"' ,be " . " .., .... ''''' "'",",11.",,1 hell<l","" 1O<ie!y
d ... i(,o,,,;'" 01 h<ad poi . . ... rth Stu to141' 451.62.
10.
~J
II .
''''
W, T.... ""' .. otmi'.-l ... LMn1 JJ9:
IlOJ·9.lm .
~ m"'lk I P.(;_,,< DS .5<)'lxIkI M E:a."..
1.0<" .0000000io .born ••
Mell
h<Mk1lo:
N _ '2: _
Il.
ll.
I'.
"
•. 1915.
q..,".
L..opIti.M L.GoI<IrnG S: l\a$'I" .... 'Ym' ...... , ...
... iewo()Oco>c> . 1ImJ Db Chlld Ill: 111-!1.
197'
0;(;;.,... ••• , A I. Du.bot 8 S· E~.ttJ inje<li"'" of
' "101"1"" bloc<! leo- pooU"""*.po",,"te _ .
"''''' . ......... _ ......1,.9; 16a.71. 1970.
Stol>o<h .. J. R;bej", .... Lc (;.,11ou I L. .. "'" Epi.
"",,,I blood PIlCh i.,he , .... .,."'o(po>, ""'tl p!I"'"
..... """'''''' A ""ubi<
"...!y. Htad.oo:hO 19:
6)11-1. 1m.
1..>II«JW.B,.ndlC8,,...
lumb" PO"""" . (.0",," 301): ",. '!9.\ lle<' ... I.
\>I,,..,
i,,,,,h<Mk""""',
n.
".
.."
•
..
n.
».
".
".
poo.I"')'tIQl"'" Ioe>d",,""- lu"<b "" •• 0115: lOIS·
170.'971 .
Se<h ... , H. Aboll: 1'0<"'100, 1.....".. .. he""·
KIlo " ..,«, wOlt <.ff....: h . I... .". ... MII 4<"""'"
"",,""". P... I. C ... Tloor R.. :z,o, )(17·11. 19JI.
".
'I.
M.m>s ~ •
R.
i".oc...;'1
bypOltn>_ ...... ,Ii, "<."""In. J N",,01 S"' . ...
.." ,,"y<loi.,., 06: , '49.51 . 19SJ.
n.
19.
Mil<hell S L.K ..I,O ~. ~i< 1 DP .... QI, The~·
mioloU. ,,,.0;.1 <llara«<ri"" •• It-.! 011.",1 hillOr)'
0101"" .......... _
t<ti<le ... ",;'h . diq:_io ....
Porli"'o,,.. ~i ...... J Am C.,blt So< 004: )9<·9.
ClwtUc
I(olk, II.! C.SOI"", 0 E. u"b."" ...... .... . llorit~
foe.1>< m. ",,,,,,,, .. oIhrlil,,*,', di<at< .•~ .......
",,004(S"1'P410):S}·n19').O.
NEUROLOGY
.Y.,""....
..,.·.d.......
m ,.
F'oo<. C M. ""'1 0 W. Sch<ittbot. L.., ai, N,"' d~
lOt "",Itlp!< "10",, .. : (;!>kiel;"",
• ...... i< .. Hoe ...
I", <e$<lll<h
ptOID<O/o."".
Ntutol 'J' Ill·) I.
19n
S... "'",. I W: Mg" iplc .<I,ro,l" Upd'" if> di....,.
.;, """ ""itw .... !"'>I._ok r",lOn. ~ l.yo CI;.
17
,-
UnJ"""J w. Ball.,., P. TttNdJ W•..,11.: ClIrQoi<
porki.IOIIb m ,. hom.",,,,", '0 ' """'''''' Qf ""pori,
di,..4IIIl"l
ScI<e« 219, 979-10. 1911).
1..>111,1. E.I...<>wIOA"' : """i •
Fi ... 'o(
,..., pano. N Ell" J Mtod JJ9: 11)004.'1. l'11ll.
K" ...... o M ():~ ..... _katp.ol.,·IO
).. ... Iote,. Ae .. Nmtol S<an<I 71: 11).19. 1915.
C,idel\bcrJ: Pl: _
.., ."""".." ..... _ j c
'"'l<'1" S.........,,,.., lO: 91).7. 1m .
1..oJ~1i. f O. ~ .~ S C: Orr-lIlol ,be <linko!
""""" of mglllp', ..I<l00;': II;..~I" of on i/Mcm • •
liontl ...... , . Ne~ -46: \107·11 .1996.
lI;"'i' ~ R A. Coh<. I ... . Wei."",,\;.(;o"""" B•.,
QI •. "'.....""' .. 01 mgl'ipk ..:lolO<il. N ~"&l J
"'«I ll: 16001'11. 19117 .
R""I .... L 1'. (06.) Mo.riIl ·. 4..4 _ 01 ...... _
ty. I,006 .• Lc.> o.nd Feb\.&<,. """ .... Iplli•• '9fl9.
k .... T S. R.......... P.Il<.u·N;'r..~ E: .... ""'j.
..... o(lrico"'mal .... ttJp .... ilh m,ltipl... Ic<oois.
....... N..nII 6l, 182-9. 1912.
"iI,ppi M. Honr.. 1d 101 A. M""'-y S P. " Ill,
Qool1';,"i"" lni. "'ltl laion _ !'""lie.. ,he
«>Un< oIeilrucaJly 1"'111'"
","""i~of
"",I'ipk ><1<"", • . NeOll"OKlC ..: 6J5-4I. 1994.
"',OanaJd W I.Co>m~ A. Ed .. (; •.. <>I.: R"""",·
..._~i""""i.<';'m."" ","~;pk «ielOl'S:
(;,tdel .... I"""'fIe i.""''' ..... po .. lonthedi ...
-.I ..... "",j'ipl< .. Ie"";'. A •• Nmtol SO: 111·1.
.yndtome.
Cu. H.GoidI,.i.'" S.R.,k,.It, """
10
"<'"'.'''''
IQ79.
16
.,.,,..Il>0l,,, Spoo,._
y,.,., 1(, 1JpJ... on """""",·s <Ii ...... Am .'.",
PhpitiM59:1!S5.6J.I999.
1(""","'lk. D.l\onotoIi E .... ,-"nsf."... L O· P.IIi·
<Io«Imy I", P......-·. ~lsu;c. C ... _p Ntu ....
"""" (6~ H.I996.
D•• i,CC . W,UIan» ... C. MMItoy S P .~",' , CIwft·
ic pr.rI;_~m
10 i"", •• _ . i.jocrion
or""'p<ridi". .... """... "yell,.I., II .. I: 2A9·SO •
Proe6ol. S77.J16. 19f19.
aorklloff. f;lippi M.Millot OH ... n1" Compa" "",
01 MR
Cfilttlt .. n", "",,""IO. IO!'""licl
.... •• ,.;". '0 <1 .....11, ""nlli.. mukipl. ",,;""";'.
a,... 1» 1059-69. 1991.
T .. """ ..... R...i,. .... M ........\1 .... "I" boIOIt<1 Ge·
myol ... ,'''' '1ool""""" c.,.,.,...;_ <>f dlfl......
MR ;""S'"' rnl<ti, 10 prtdic' """.. nlooo <o.HIIi·
!mo.i.,
c.,ly 4<fi";« ",.hlpk ..Ie ....... AJSR 21: 702.6.
~.
". s....
an I M .II<>II..,Ow, B.... ' H L • .,al" M'a'
.. lie 0"DQIIIf><0 i ""Sinc afI!I clinical .. loIi"",hipo ,.
",oUipl< ",,"""i,. M.Y<'
Pr .. 6l: 17.·... .
•
cu.
1917
""""'[i. A I. 0.«", ... S. "..Ips C E." aI. ThO
2.11. Rderentea
00-
"
".,V.,.
aIIlI<) 01 mlsn<'"'
~
"
'"
...
"
.,
.........a
1/1 "",icnl'
.,,,11 ''''f'O<!O<I ",.111fI/< ",,10_ .. J.v.tA ll.9.
JI'O·'s I. I"J
KoJdC. Thcorp< I W. ~A I• .,., s,....1
corti i/uV •.• Io1Rl ",I'r ...kI.am) Cl)ill_ r."
III"'
II, F, .....,.. '" "",h.p", >tJm>oj .. /'1 •• ,oIocrH. 16:32·1, I"1
........ D L. u..... E 8 ' M ",~Ie ........-., ",,",in.
ofthtbnin ..... IfII... A""I ...... M«lIOll 001-
«""
l4.I~.
",_i, _
...
,'''11«_" .....
"' ... ""............
L>w~I.M.I"...-DE,CNS;S~mI_
M•
'I\".......
i< ~ 1""'1'" of
i.. ""my.II ... '"I k<ooo ~<1I""""'1oIogjI 001111); 9S6-9. :!OO"l.
D"" F A, M, ... !oJ ~ ft. D'JVurd," J 1.« .... AICi.·
r"1 .... ns< 0/ ....1, mlln poI;, ......iII> clh>leoll)
1... 10<001 , ) _.... Then*oftola-'- OfI MJU ,J
Nt .... "c.""",.. P,~cII .. lr ~ 70: J9I).J . lIlOl .
Ftu>J .... MS.n.o.,.p_[ J,O', .. ~O . .,
Ill.: R""""""ookoI ..1t>dM<I ",...-pIt>o1 nuol
.....y.;, ", "" d, . ~. 01 .-..IIlp1o Itlcroo,,_ ~
_ ....." ............. A«h /'Iou",I.:!', S6.l-10.
""yy G 101 , 11<n01 A C . 11u1... N r ."".. N<uJOp1_
dI_
_A"ponof""o ...... /'I ... roIocI'H: 1()(\oI'. 19'12,
e.",hno,o C. Lao:onolll ... L, M...",,'" V.•, . 1· A
... ~Iod lrial of .. I"";~ ,. "")'OU<II>Inc I.II<rai
H [nc1 J M«I 1>I: ~". 1990 .
Rl"' ..... rOf lnIJIlIInIjIi'Ii< bocnl \Cl ..... ,. 111«1 Lt\ .
"" '7' I 1)-'1. 1m
Loo:oomb:" L. &:.0.; ..... G. G"lile, ~ .... ,_ ~ i "'·
<0100 A """...·lIIiolil .. ~..., pi..,."""",, • •
,""'Ied_..... <I""ym >m)<lfl<>p/Ii< IlI<nl
><1«o",(",l.$). EI .. ' . ...... pb Clloo r>iou,opb,oioII
97; S6I.I9'lS(.botno<I),
A~AK,"""'''' D GW.1(1tI>1I R• .,..I" c..fvo;di>I""''' ofCu;llol • •e."" .j ....".,.., MA
N..... 01 J. ~"'.I97 I.
M.o&11 1 R. 0.-0.1< ..110........., ""m)'<li ....,.,
poIyollClr;;"',,,,o",,,,"'~" AM" II .. ""' .... lll~.
1991_
~>I1 .... "",,"1 W .C ......."'" O. IJ"m.1 W•• ,,,/,
T.......... '" <Jo .... k ,.n ... __ .,.<l<m,.I_i"l
poIY"'"'",""",Y ",i'h c"Jo>por ... A, J "'.uo .. 1'1 .....
....,.. "'~1.1'l'6O' It..I.;, 199Ii
Gotwo K C. Ropp« A H, CI'''' e O• .,.I.: T... ,_
mo.' or c~,.",;. ;,,11 . ...... ''''' <10",\,<1 ..",., pol,.
~ VII'" ion.ff• ......" 21, 1'1 ... ",,011' loO: JO_
1. 19'/1..
G'II'!I ..... Ilar7tS~ .......... _
Tn,l Oro.p, Doo ·
or _ .... er"""... """"'"
1<"'''''''
>.
"
"
lIIHp!i..:l IrtII "'
iIo!,...-., .....Il}''''''''''''''''-,.
Gu,tloi... 6ar.t.,ncIrDm&. IAJouI II I. lU.-?O.
I'I'1J .
"
".
~
~
"
M,
..
".
k'",,'" I c. OJ'''' M L! M1<lIrio...,J '":f<'~.
I. CIlnDl ..... n>IogJ. 6>1:" ..01. 8 _ I~", ~J.
(ed,.). Hupo, <h<l Rm• • II"..."'.... . 19\1" PI' l.Jl
_101 P II, Acw ~"""'"'" "'IoiopotIo,. o\.r<lI
NrtonI9 , 111·9. ,9&J
[p'" H· n .......... "),<1""
<\e<I;Iy •••. R.I""" '" ....'" J "" ...
So<tJ: 63" ,
IlU·9.19ll
t.lp<Do lit. " _ol lll 0: ~""I<''''.'''''''ml''"lopII1II, !"oJul", A IolloW-"P " LId, . Ar. h N... rt>I 11'
!H·1.'973
Rop,)c. A II . ro...~ .. '''' 0<;, Th< ~,,6f..,
tnd ",100""" 'ra","'", ",),<.h) boWll on uriy
A"" N",,,,I.· 11·9. 1971
a."", ... M. Ftldrro,. S . AlI"~.
...,.. .. peI_;', I ",,~ one! <II.",,;., ..... to<..
01....... N... rof"ll' " , 966-71 . 1981.
_ O, W.... II . KIo .... AJ, . r<LCT"'I' .....
"
O.
W
OkuMoV' ""'_D~C1o"I<WPI'"_
~_ ...... JOPI'''''' .. ..... ""' ..... Sca ... 7J
....
,,1M. ""'_'......
2.11. RafBNmce5
oloTri_,/'I. ~E:I"" ........ I .~"
""""""'IOII&k>rnpllo<"",., .,._1""""<0"'" S."/'irtonI 9-I~7 ' . I'I1 • •
RIItittIJotIIM S. D<lI<"... I: A' I'IIIn1orouy _
... &hIl .. """"'''''''"~'''''''''''''' '~)'''''
lI1.yo C ~" I"ro< 11. 601~ . 19~1 ,
01......., V 1'1<.. ~piNI n..w ......"""',.-.Iock.ol """ ..."n>IaoJ"'kl&I<ll .....1".,..... in 11>0
,,;.""" ....... "'U....... "'''''~....10 SIu-.
<Old ..... , IOS<IO. I9I1,
5 ..", D 1 .~1iI5 A,SewdIC,,/QI
""'.. or _ _ , .,~" c)'<l<>opormo. Acch
r< .... 01 .9· 106J-12. 19S11.
!'on 1 O. 6toud>omp H I, R.y.",.,... '",'"'_.,
~
""'<04'
p.olllDl<>J.it-•
..,.,ln ","",>I<Il by'....'.. .." ........
""Y~).IIIn<l"," . Rodlot:r>phI<1 II . HH'), 1991 .
Sd\o<! .. »w.e...,...,.,., F S.Cool.ll.. MG. .. ttl,
Dltroaioo_ ... I&IIL.... irnotit, dil<'liml ..... t>o<_
<)IIo>IO>ic 0lId
«_ 11\. ",,1<10< "",., . ...
1<mp\i. ,S......... n : IOaz·~ . IWI
Oucb
c.,..,p"md
..,..<10".,....,...... ",,.,_..,._ 1.«10,.,,,,.
~ by M..... _ ••ObsIeI C ~_ 60: l29-l 1.
"!IlI'''''
".
.
'
"
"
"
"
n
,
n.
~
"
r..I"""",,,._.
J""',
""" ... """"go....
s.rc._ "
lll-'Xl.1 9l16
"
" ,.ri.
"
,«...,c..,
.....
"
..... plool"",)'<ljoi.1 A .. oM!) of I I 1><,...... Ann
N< ...... U( I). IJ..n. 19IIJ
,.".
". 1f<lw>IoI...
".
".
M.
)(0: .... J J ~. I()<"OI '"III<)<"i" .s.r.ydj""'I Io.
''''''' oftht Inlo' 1........ "''' . ....
~pIo
r>f1111 ow MRI . f..,UI< tnnO, .... 10)'<11'," J C .....
p'" A..... T....... I' 6O'i.t.lonl .
0.-. .... " C, B_~ V V. Coole S 0: 1'01,,01< be.·
.r""01 off... Dr"'. . . . . I v ......... 1honoP)' i.
"'."<I<m"'".. 'I ... "'.......... 'n"' ...... m~ejktl
N<u ....."" JO, »-6. 1<teO
S..... B I , ItturoW>ol. 10..1010.,
01.
_ ................1 ....
Am.f\I ......
4l; \I09-I7.I'I!:'i.
n
"
"
".
_'II.
[E,
"'UIOIIIOCf;I"',
'9Sl.
~ .... F. C. Gol< ... S t.D_ ~ M.".I.
0."""
potor-""'" ""'.!<>polhy, C..ur.1 ""1.0"",,, . ......
iltd. A,," N. u,oI JJ . ~n~. 1m
Moon: " M,
It. Ntun>lol'" '''...pll",,!1on<
of,"",.~'I .. An. 1'I<~ ... 1. jS~7.19n .
Sol.""", C. COOl'" F. So,.d' L. .. ,,/, PoI1I"YlI'
".,h<~
-o:c!l_riW. N to.&1J
M«l :J.07· l61·11. 'XK1z'
SaI_iC,G"'-IS " .O'f. ILon W 101 , •• 0/ Tho
"",\dtru
1!~ i< ill 01",._
M..... _ : A~n""l ........ i.,."Y<I.. />OI .....
A". In ..... Mod Ill . 19J· •• 19II) .
1.1.. _
Ii: D, Mi<IR<C I, SoIlord 01 •.,0/.. T",,,,,,
1. 1",,1cImc<_ OIiIoI.. ll'fO'C"II'iullof"_lor,
IOn'" ,. 0tntw>0J
19loO·19t1.
A.. hl1lb: II"'.," JI : 7' S~. I 9U
o\lloft r< D. S,,,,,,,,,aJ S iI. P<>l~",).I, ...........1Ii<o
0lI<l ....,.,.. >rI<riIlt, M<4 C1ko N 0\ ..... 111. )69.
/10. 19".
11.001<.0 G GlM' «II (.. "'1'0'*1) ........... Rbno ..
Ob 0;" N II .... 110: 199-4D9. 1.9'10.
HoIIS.llo<>d<oOG: h ,... "",01 IMO)'biaply .......
_ 7 ~I .y. ClI........ W 7'lJ·O. IWoO .
c...lu RJ . Plnulotl R.IIJlId<l GG"'o-iJ ,.",...
"",I ."""PI'"" .)0lIl ....... 1• • "'" "II \lfmI'II"Il)
""....... r.: ....oIoQ ]i, W).9. 1981
SIll ....' C.tt_O C: G...... II on ...liI"';u,
lowtt)"AootJ" ..... i_ioo.-..,f_) 01
"""""""" "'. "",,"1M""'."""" ""'" A"~rlilo
1t"""",C1; IOIM.JOOI
0 ......1 D.E ..... , L S' O'-iooool ' ru<m<,. 01
_o<Jo<;n' .... ldorly Mrd CIloNA_,lS. i!61 .
11. 1"'
Kor-oco. ... o . 1..>:00 N. NW!I.,.;n 1': C"T Ii~'"
'" .. tnpoo>l ....... U' A .. portor'''''' .... 1'1"""",
rod 11: J7l. 1'116.
Mco...n.tl P I . _ . G ... . "" i l~:O It. .. uI
c..pp,"
..........
<>f.,..., ..
"'""'Y.
"""'y. "'"",.""'.
T.,""...I....,.,,"'A<I;"~_, . 0PI>-
' hlll""""'c:7 9], ~IJ..)O . 1"&,
A<I>h. A A. Lie I
tl G.It 0/" Iittw 0100,
pt< . .... , -,i<.,.,~ If."""",.ff<d u...1>IDpo)
't."""',,
NEUROwm·
•.".
lol'" II l.F....... 101. Co-rd>r " y""",~,.. . »o<_
a....cT,.. H_OO IbnpDM.,,~'.· ' '''
".
1<01 . .""", ~
...."'.. ......,.. A_ L....... rotod \11' 6U-1II. 1~11 .
Sol........ C. 00iIrC1S E. O'F,IIoo W rot. II 1>/ ' fit...".,.., '" pOIJ~""p:o _ 1 0 0hn<IMd
- , .. 101'-"". 1910- '991 ",••kio_""",
)I' »9-1J. I " ,
M;:~IoITI.M_flA ""..-' ............
".
r-.,.;" 11'-«11 ("~)""""d A... 110-
U.
"
U
U
W
"
..... _ ,lIJ.. WI~I . 1
.
c...;,,;F.WoarM C, OLIrieoi l.tltoI·. IitJ""""rl<
~ ..... ooodC·_~ .. _ " , .. ""
.. _ _ af_ ..,,,"' ...........,I. roI,·
",",," rtorolUlico; A pr(IIpO<I ... i",_.• , .. "",
_ Att~ IIo_JO: L'J." , JOOO.
..,'o!t:a._
A Io.,",~""
_. ~" 22D-JI . 1'lIJ
No .. _",.~ M«I ........ .It. 1S-6.
,,,,
~TlU,_'j.l .fecJ AS
1_"111"
" ' ' ' ' " _ ......... .,. ............ pocoi ... dI.opDI.
""_~
N6UROW OY
.. _ _ A.. JMooI 1. 97·
IM, 1981.
1100-6. 1m
H_ A N. IIWC l .ZnI« DL.,oI. F,,,,,,,,,,,,·
"'~~''Ill»l.<I ".. ......... <vOUd......" .....,. •
..1III.....,......_ . J .v.Ll lj~
_,_".0",
"'I~'''1' AJ R 1:16.9»-60.
,. ,
...,
l.L:rlc:oooo 1( . rc......,..,.""'I.. d,>pL.oI.
..,11<>1'.....
..... "'" 1Jnioo· ~ .......... 00
d! .. •
ai, ..... 1I<.. ,it..~ra<I<n., 1<o 51 ...... IJ ' 6-.31.
M"oI,1'" II L. n_.... L"u) ;p.......... ,""
koo ... III C..... '" '_1'101 II.. oIiou .., 5" . 1<0 HI
SH, Im .
~
"
_loJf_.".,.. d,.plUl.
O'I>oroAO ......... '- ~ i!::A"fJOI'''''''''' '''''' '''''''
"'Ofm... ....s ..
S'~"" ·' L7·~.1977
CI\oMI, H, Yoloodi 1( . lbo-Z" ...
M T" ."" Cion,·
dl"""""""or._II· A"""'''' ..... 1.....1i..,
........ 1<16: 9~9 , tw,o
"
3.1.
Surface anatomy
3.1.1 .
Cortical surface anatomy
Figun 3·/ shows
som" importanl""rti~1I1
surface landmaTlta.
This may be h~lpful in
corre1atinr with MRI to
detennine the location
orl~()n!lL. The MFG ;"
usually more .nnuou.s
CENTRAL SULCUS
(Rolandic fissure)
than the IYO Or SFG,
oonnec~ to
p~...,entraJ gyrus
lind (t oA.en
the
viII a thin i!lthmua. The
celltrsl ,uJcu~joins the
Sylvian fiuure in only
2% orcases (i.e. in 98%
of OilS"" there i , II -aubcentno!" i:'Y1'UJI) , The ;nte'l»'rieLaJ ~ulcus (ips )
I"parates the s uperior
lind inferior parieUli
lobules. The IPL is composed primllrily of the
AG lind S MG. The
SylviaD fissure lennina te.'! in tfle SMG
(8rodmann'. area 40),
The .uperior temporal
sylow; tenniollt.es in
the AG .
Figura 3·1 C",ebral collical ",lIace lIrlaLomy'
BI .~
Btodmann'l" ..... (~~ s... fllblll".,.rod f IllW3·ZlOIlbbr.
¥lotions,
Brodmann's "r"ali
Figun 3· / also identines the tiiniClllly significant al'"
ml/.p of th" cytoa reb; tectonic field~
of the human brain. FUnct,ionw aignificance ofthese areus
"all ofBrodOlann's (8r.)
ill /1$ (OUOWI;
Table 3-1 Cerebl1ll sulci
pr«>tntral SlJeus
poSI<&rlIIaI sulcvs
,a, if, SUperior,lr!IlIrior lron-
,..
,~
,,--
Sr. areas 3,1,2: prima ry tOmato8<!1l8ory corteK
Br. Hreas 41 & 42: primal)' audil.ory area/l (tra"""enle
~~""
gyri of He.!Chl)
$ 1.8, ,La superior, iolerior li!fTI'
Br, area 4: precentral gyrus, prim8/')' motor cort.!"
(AKA ~motor ~ tr ;p·). lA;"e conc~nt.rntiOlI of giant py.
lnwrpI!rietal sulcus
ips
ramidal cells of Betz
pre«Qpital notdl
Br. area 6: premotor area or supplemental motor area.
Immediately anterior to motor strip, ;t playll a role;o
CI,)lltraJateral motor pTOgl'amming
Br. area 4<1 : (dominant hemLllphere) Br oca'" a re .. (motor speecht-
"'"
"
3, Neuroa natomy and pbysiolocy
N1!UROSURGERY
Sr. area 17: primary vi .ual C<)rtel<
We",;" ke'. ar .... (lan,guager": ,nlhe
dominant hemisphere, most of Br.
area 40 a nd II portion orBr. are~ 59
(may .. 190 include _ tJOSl.erior third or
Table 3·2 cerebral
STG)
Br. arell 8: the strilWd portion in FIf;.
ey~ tield ) irtitiatc3 vol·
untary eye movements I.(l tha
oppOllite direction
"re3·1 (frontal
3.1.2.
Surface anatomy of the cranium
CRANIOMETRIC POINTS
Craniometrie poin!!!
in Fillure 3·2.
Pterion: ~gion wherf).
the following bonOIS a~ ilP'
prollimaU!!i: I'rontal, pari.
etlli. l.eroporaland sphenoid
(g>'1!IIter wing). Estim ated
as 2 finger-breadtlulab(.v"
the ~ygomatic arch. and a
thumb'. breadth bmind tbe
frontal p~ofthe ~y§l:l_
matic bon • .
Asterio n :jllndion of
ilImbdoid, occipitomastllid
and parietomllstoid . "t"us.
Overlie. thejllnoli(lll of
trnns"erae and lrigmoid .inu,;es .
Vene.., the \.Opmosl
point Ills skull.
LlIlIlbda : junction of
tll .. 1ambdoid and sllgltttli
sutu .... s.
S t e pbanio n: junction
oftbe coronal ,UIUreand
the 9up('rior tlllnporal line.
Fll1 ure 3-2 Cranlome.rIc pOOnl5' CfBlllailltll.vtes
G h.bclho: thB """" for- AtJtiIt!VJi!IQm; OWS ,. UIOtitCI w'ilg '" ~~ IIOoJe. Q\ " ..... 01l1li r;uward prtlject.ing painlof tbe Iol!. is " lambdoid SlJIuIe, sU ",supetiot II!IIpOI8i line, ZVO. z:ygomali:.
forehead lit the level of ch~
N;Jmed boneS awe~r irI.~ vppeI elise I!1t:e1~
supraorbital ridge in the
midline.
Opiathioll: th e p61terior ma rgin of tile foramen magn um II' the midUn e.
8 l"fl gm 1O: tbe junction of the eoronnillud ugittaJ BU1Ul'@a.
are
~ho\lln
or
A.
l~.~ r~octioo ... "" .... ~ <elitbJy I.... U.. d 00 . "",tuol< """,,,,,, d~n.. l<tdlv!du.1 Y''''oblll..,. In
I", euOI 1(I<IIlion; in Mltr lOpeno"" ",...;"",1 brain "'Mction.... ith ",i . imol n.k.,c oph..i. , 1«1>.
niqu .. "o<h u inl,....,I"',..liy.. bl'llin ",. ppm" Dr 10'l1unc I'or ph _ _ ....,1 on lo'nop."n;y•• 0....
ii •• 1 SSE'" ohould bo .... pl.)'d
NEUROSURGERY
3 Neuroanatomy and phY8loiogy
..
RELATION OF SKULL MARKINGS TO CERE8RAL ANATOMY
Taylor-Haughton IiDea
Taylor-Haughton (T_H)
line s ca.o bf! constructed on an
angiogram, CT scout film, or
uulllt-ray, and can IMn be reo
coll8lructed on the patient in the
O.R. bned on vi.ible external
Isndmsrk$'. T-H li""l1 are
shown 1108 dashed lines in Figure
3-3.
1. F't-ankfurt plan e, AKA
baseline: line from inferior margin of orbit
through the lIll.Iltt ma rgin of the exte rnal au dio
tory meatus (EAM) (as
distinguished from Reid's bn&e line: from infe_
rior orbital margin
through thec~lIj~rofth e
EAM)' lo llll
2.
the rustll1l<:e from the nasion to the inion is mea'-- ~"",., tine
su red 8"rt>55 t .... top of
the CIIIlvsria and is divided into qusrters (Clln be
done aimply with a piece
Figure 3--3 TayIor·Haught"" liMs
of tape which is then
and Other localizing methOds
folded in half twice)
3. posterior ear line: perpendicular to the bsseline through the mastoid process
4. oondylar line: perpendiculsr to the b8.$eline through the mandibular OI)ndyle
5. 'I'·H lines can then be used to app,oximste the sylvisn fissure (su />flow) snd the
motor OI)rtex (alao su ~low)
Sylyi an fissure AKA lale ral fi ss ure
Approximated by a line connecting the latera) canthuB to the point 314 of the way
pDl;tenor along the SrC running over convexity from nasion to inion (T·H lines).
Angula r gyrus
Locatedjust above the pinna, important on the dominant hemisphere aa part of
Wernicke's ares. Note: there is significant individual vanability in the location'.
Angular arte.-y
Located 6 cm sbove the EAM .
Motor cortex
Numerous method. utilize externallandmarb tol"""te the mowr strip(p~n tral
gyrus) or the ~ail.ull:l.m (Rolsndic fissure) which separates motor strip anteriorly
from primary sensory cortex poIIterior ly. These arejust approximations ain<:e individual
variability causes the motor ~trip to lie anywhere froro 4 to 5.4 cm behind the coronsl
8utUre', The centralaulcus cannot even be relisbly identified visually at 6urgery1.
llIethod 1, the superior aspect of the motor cortex is slm08tstrsighL up from the
EAM nea r the rnidlioe
method 2' : the <:entralsulcus is approximated by connecting:
A. the point2 cm posterior to the midpoaition of the ArC extending from nasion
to inioo (illustrated in Figu.re 3-3), to
B. the point 5 Clll straight up from the EAM
method 3: uBing T-H lil1f:s, the central ulcus is approximated by connecting:
A the point where tbe ' posterior eaT line" in tersects the ci",umference of the
skull (Ut Fi6W""1! 3·3) (usually about I em behirnl the vertex, and 3-4 em behind thO! COTOnal ~uture), to
B, the point where the 'condyla r line" intersects the line representing the
aylvian fissure
"
3. Neuroanatomy and physiolOiJ
NEUROSURGERY
me.Ulod 4: a line drawn
4S' to Re id's ba(.e liJ:,e
starling III tha f le.non
points in the dJ.tKl~ Gf
tbe. motor $tOp' .. ••... )
R ELATIONSHIP OF VENTRICLES
TO SKULL
f?iIf,un 3-4 ~bDW~ the. rei,,·
tionsbip of non -hydrocepbalic
v!!ntricJl!!I to t b!! $kull in t be lullral view . Sollie dimensions of Internl are 8110wn in T{Jbl~ 3_3'°.
In UH! nOIl-h~drocephaHc
adul t. t hE' latera] ventric~. lje 45 ~m below th outer ~ k ull !urf!ct!. The center an be bodyaftbe
lateral ventricle "UI in tile mid pupillary line, and the fronta l
hom i. intersected by lit line passing pe.rpendicu la.r to the colvaria
1\10118 this IIneu _ The anterior
bomsextend 1-2 CIIl IItnteriorto
the C/lTOlIlIl Bnllln,\'.
Averagl'llength of t hird ventricle _ 2.8 CIO.
The mid poin t af'J'wining'.line ( . in Fic''''' 3-4) should lie
wiUlin the 4th ven t riet • .
FIgura J-4 Retalioosl'>lp oj venll.c:le5lo $lWll lanclfTWksAI:It>«Iv~liont : jF E ~ OOlall»'n. B E t)II<I) ... . al~""' , 0 .. oceipotal nom. r
hOm) 01 "1~aI venlricloo. FM E lenmen 01 Morno, ,o,q .. lyI..l." ~u.dutl. V3 _ 1IWcl "",,1_ . ,,4
,.!OUIIh Y8I1IrIcI.. ct; .. """",,,I lUlu", ~!IIeIlSimII 0 ' -<1 SiMT_3-3
-'' ' '1'0' '
T"ble 3.3 Olmensions from FlgufII 3-4
"""""'"
,
(S!~
Description
lowerUmlt
I~I
F'PgIJfI1.NJ
DO
,.
OJ
3.1 .3.
Avrr.
,~,
&'tglll at IIOIltBI 110m atlieriDr LO FM
dis(&nCe!ram clivUs LO fOol at41h vl!lllriele I I
ievei oIllStiqium'
Iengm 01 411'1 ventricle at le-;eI oIlast¢Im'
'"10,0
dis18/1O&!rom lasb!lium' 10 opisthion
30.0
"".1
14.6
'"
Up$It1' lI mlt
(mm)
40.0
19.0
" .0
Surface landmarks of cervical levels
E.timalel gr""rvicallev~J. for "nterior cervl~"l
BpinelUfgery may be made using the lan<lmaru shuwn
in Tabl~3_4_ l ntro_0pe.rative C_spinex_ rnya artte ....... nli ol
to verify lhel!e e9tilnatu.
NEUROSURGERY
T" ble 3-4 ClWliClillevel. "
3_ Neuroanotomy and phyo;iology
"
3 .2.
Cranial foramina & their contents
Tllble 3·5 Cranial lO'811'1 1n8 and their eontent s'
, III
I
I
*_.
"lItn..alioN. a *~. U • ~ ~e(..... v,
W s .M'., n _ ........... M '"
~ . • .,. ...... _,I"," • Iorlrt'ol'n, doll . If;vl,,,,,,,
n~"'H.br .
_ Ill""",,, Ct.
Porus 8c u s ti c u s
!~ Fillur<': 8·5)
Th'l lilll lrulnts of th ...
aCQuuj" pon;on orVIIl
""netTate th e tiny open-
inp arthe lamina crlhrosa
of the t'tIChlea. "rea" .
T ... ns"t'r'IIecrest~
sra les auperior ves tibulHr
laool ca~1 (edt VI!)
wni::alaesl
,,<></ ,
area /lll\d fadal canal
(above) from the inferiCl'
vestib ular IIl"1'a lind cochl~
/Ir .. rea (below'"
Verr.ical Cn!!'It: ""pllo
ra tes superior v", tibular
a!l!1I from meatus to
canal.
"
Ito ulncIe
&. 5!!perior &. literal semiciroJlar dt.c\$)
supelPDT ~ ilIe!I
1IaMW!/$& tresl (CIlSIa lalQ/orlms)
lI1IeTIOf vestibu~ area. (10 $OICCule)
~~rnef\ sitIgtia.e (10
posterior semio::ireul~r IliXIJ
tlllCllJ$ 5jliraiis 1000miflOSU5 (oochlel r
~rea) (ae(N.Islic: pcttiJn 01Cr N Villi
r~ci~l
3. NeUroatliltomy a nd p hysiology
NEUROSURGERY
3.3.
Spinal cord anatomy
3.3.1.
Spinal cord tracts
~
..
MOTOA
(descending
Pllths)
bi..jlrectional
",
S = sacral
T = thoracic
C = cervical
SENSORY
(ascending
paths)
11
13
"-_.1.
anlooOf spinal
,"'"
15
anteriOr motor
nerve roo
A gure 3-6 Schemalic crClSS-sec1lOI1 0/ oervicaJ 'pinal !lOrd
Figun.3·6 depio~ a cl"OiSs-s« tion ora typi ..... l spinal cord Bl'gmenl. combinlng some
elemenU! from dirre~nt levela (e.g. the Int.ennediol~t.erlll grey nucleull is only present
from 'l' l "' _ L l or L2 where th"I"I! art! synlpllthetic lthoracolumbarou tOow ) nudei). It is
schematically divided into p;;<;ending lind descending halves, however, in actuality, as·
cending and desoending paths <x>e.ust on bolh aides.
Fisure 3·6 abo depicts sOme of the laminae according to theschemeofRexed. Lamina II j, equivalent to the l ubstantill gelalinosa. L.e.n.;nac III and TV are the nudeus propriu l. Laming V1 is locat.ed in the baJf.' IIflhe pOf!terior hom.
Table 3·6
NEUROSURGERY
tracts (
I
3. Neuroanatomy and physiology
Path
hllle 3-8
functlcln
Flgure3~
SeNSATION
PAIN & TEMPERATURE: BOOY
ReeeptO\'1l: tree nerve end ingJ Cproblib!e).
161 order neuron: amaU . nnely mye'inll~ aff,,",nta; ..,ma in d"",,1 "",l","glion
(no l)'1UJpae). Ent.croord aldor1!Olptllrallrllct (zone OrUOIU\ler). $)on_pH: lubltoanti' ....
(ati nooa CRaxed 11).
2nd order neuron ll.I.on CI"OQ obliquely in the pnterior white WllImlalmllll,c:endlnll
~ 1-3 Ilegme ne8 while CtoMing 1.0 e nter LM Illma' spinothallmic lracL
Syn>l~' VPL thalamus. 3Td order neurons pas. through Ie 10 poIItcentcaJ gyru&
(BrodDl8nn"...-u.s 3, 1,2)_
FINE TOUCH, DEEP PRESSURE & PROPRIOCEPTION: 8(XIY
F ine touch AKA di!lCl"iminative 101><'11. Rettptors: Me.i$ll.ol"\'"" &. parini8n a..-pu"..r ...,
Merkel'. d',b. frl!e nerveendlngs.
lit ord~ neuron : helvi'" myelinated 8tfe~nta; 1IOm8 in dQf"llll..ll'OOt pngJioa tno
IIYnBpse). Short branchnlynapte in nud eu. propnus (Rued 11\ &.1V)orpGliu rior grq.
long f,ben enter the ipsil at6-al poaterior CX)lumn. with(IUt lynapsit18 (below T6, fucic:-uIUlgratil ••; above 'l'6: rudeul u. uonutu.).
Synapse· nudeu. f'"3ei1is!cuneatul \ ... pec:li~,.). j ...t above pr.amid,1 dKUlHlion. 2nd order neuron axon. i;)nu iolemalan:uate fibers,decu!ISBte in \ower medu lla a~
m e dia lle ....... l..,,, •.
SynaJ)H: VPL thalamua. 3Td order neurona pHI throullh Ie primarily to P'II'tcentfal gynq.
L.1GHT (CRUDE) TOUCH: 800Y
RKeplOl$: ILl fuw tooch t- "bout). a110 peritridUa.i . rboriutiooa.
lit order neuron: larp, bovll,y myeli,..~ .I'fueIlU (Type IU; 50lIl. in do,...1 TOOl
pnelio" (no '1fUIpH). Sortlfl IlC:eod unc.--l in pIIIt.CDlumn. (with fine touth). lJIast
qnapu ,n Re.ed VI .. VII .
2nd order n-e .... on lUCon. trOM in anterior whiteC(IIDltuMmt fa few don't crou): enloer
anUorior .p;nOlh.lllDi~ 1r'~L
Syn'PH' VPI.. thlll.,O .... 3rd order ne .... on. PllIIlhrough Ie prim.ril,y 1.0 poIt<:en1r. 1CYflII.
3.3.2.
Dermatomes and sensory nerves
Fi8un 3·7 . hOWl anlerior.nd pCllUonor view. uch ICheQUltically Hpar.lltltd into
pi!riphera\ H n-..ry nerYll di.tnbuUon.
li!n~d«rm.tome. (M'fPDt!IIUoi) .nd
3. Neuroan .... tomy .nd ph,.iolOfDl
!-lEUROSURGERY
ANTERIOR
RMAT OMES
POSTERIOR
CUTANEOUS
NERVES
Flgure:1-7 o.,rmalomal and sensory nerve dislrl:>U1ion
(Red.awn lrom -Inlroduelion 10 BaoiC Neurology'". by Ha.ry O. PallOn. JoM W. Sun<lSlen. We1'" E". Crdland
Phlftlp O. Swanaon. C 1976. PI> 173. w. e , S.unclef. Co .. ""~_ lphiI. P.... ..;j~po<mi """ )
3.3.3.
Spinal cord vasculature
Although a radiculAr artery from the aorta acwmpanies the nerve root at many lev_
els, most of these C()ntrihute little flow t() the "pinal C()ro itself. The major blood supply
t() the IllIterior spinal C()ro is from 6-8 radicular arteries at the following levels (" Tlldicu·
lomedullary arteries·, the level.lUited are fairly C()osistent, but the 5ide vann" " " ""):
C3 - arises from vertebral artery
C6 . U$UBUy ari&es from deep cervical artery} _ 10% ofpOpulalion lack In anlcriQr
C8 . uyually from cost()cervical trunk
m ic:ulu ilIluy in lower cervical
. pine'·
T4 orTS
Adamkiewici (rUM/OW )
The paired posterior apinalarteries are leu well defined than the anterior apinal
artery, a nd are fed by 1(1·23 radicular branchl'$.
The mid thoracic I'<!gion hu a tenuou s vascular aupply ("watershed wne"), possessing only the above noted artery at T4 or T5. It is thus more susceptible t() v89Cular in ·
,ult.!!.
NEUROSURGERY
3. NeutOOnat()my and physiology
"gu,e 3-8 Sdlomillc ($11\Qf1l/T1 01 ~I COld a_1aI su~ty
(Modi!ie<l~om
Oiognosllc Neu,o'.~IoIogY . 2f11l"'~ VOl""" II. PII. II B1 . Tav." ... J M. WOO<IS E H. edilCn.
• 1918. IN ~ !_ .fIIl WiIkIrIa 00 • B.lllimQr • • ..,l/l
''1
p.''''......
.Artery of Adamkiewicz AKA arteria radi cwaris antl'riQr magna
the main .rtvnal tupply for the ,pi lUll cord from ~ T6 to the ronu.
located on tb. I"R in 80%
O<:c:ura ootwHn 1'9 &. 1.2 in 851l. (between '['9" TI2 in 75%); in remaining 15%
ootwoon T5 &. T8 (in t.... eaa latter cases. lhe~ may be a ~uppl 'mental radicular
artery further down)
usually fairly large, givtl8Qffrepila.lk IUId CAudal branch (J atur i. u3u811y larger)
giving II eheractcristie hair·pin appearance nil IIngiogruphy
3.4.
Cerebrovascular anatomy
3.4.1.
Cerebral vascular territories
FitJun 3-9 depicta apprnUmn!~ VlIOitulardi,tribut,oBR nf the major cerebral anories .
3. Neuroanatomy and phJlliology
NEUROSURGERY
ThenJ i . conaiderable "ariabili~y ohbe major o.wr il'll'. " willi ... the cen lrB l d i!Lr ibuti('>1I
{tJte.lentiadostrintH. recUrntlt artery of Hlllbner (ftH) (AKA media l uri.1.e artery). d c.
ha"e v,u:yin;: di$tributiaml'nod may have oligin!l ()/T' ofdill'l"'!cne Hgmentl oflhe middle
or an...nor cerebrw Itt.ery)
4XIAI. ... ,EW
CORON.I. ... ,IEW
3.4.2.
Cerebral arterial anatomy
The aymbol "-" i. used to denaw a region supplied by the indiCllted .~. SeeAn .
liography (NnbrafJ on pIIte 130 for anrlographic diagram .. of :.he folla...inC .....tomy.
CIRCLE OF W ilUS
A baJIIJlOOd eonfigurlluon o{ th e Ci.rcle of Willi. ,~p..-nt If! only Is.. of the populi'
!.loo. Hypoplasia of I nr both p-comms IIC:curl in 22-3K, llbam~ nf hypoplastic AI ,.g.
mentll oa:\.ll'll in 26".
AnatomicalllegmeDta of iotrllcranllll cere.br . l arteriell
carotid artery; the traditional numbering
(~un\.er t.~'~'~"~3~'~'~~~~~'~';Ih~'~'C~'~
to th ... dIrection
offiow.
nnd
theda!
nwnbering
ly,;teUl"
WlU &(,>IJI
rostra
l totocau
""bl!!nt "fth.. laher IIJ'Wri~). A number (,>f
ayl\.e1llS have been deacribed to addresses
thli in<:OlUj'tency and qlflO 10 IdeDtH'y I1l1n·
lomic:a lly impDrtant IMIgmenl:l oflhe leA th.t
wen! n .... oI'iginaUy delif'lf!al.l!d ('-1. "" Thblft
3·9'°). AlIo."" ~Iow for mOrl d.t~iI
an terio r cerebral It;
• AI: ACA f,,:n'U onain to ACoA
• A2: ACA rrom ACoA to branch-poinl or
wlOllOmargiDal
• A.3: from brandl· poi IlL orcaUOIoOtnirain·
al to , upenor aurface of ~rpul calloosun'
NEUROSURGERY
"
3 ~r;n posterior to the. genu
A4: pl!ri~al1ol8l
• A5: t..nninal branch
middle cerebrnl'":
• 11011: MeA from origin to blfurwtion (horizo ntal segment On AP angiogram)
• 11012: MeA from bifun:.!Ition to emergence from Sylvian fill>lure
• M3·4 : distal braoch ....
• 11015: t..nn;nal branch
post..rior cerebral (PC,I t ) (several nomenclature schem .... ""i8:"''' ~
• PI : PCA from thllQrigin l.O post..rior CQmmuni~ating artery (AKA melM!n ·
cephalic, precommlUlicating. circular, peduncular, ba,,;lar ... ). 1'be long lind
.. hon circumflex and tbalamoperforating atteri .... arise. frem PI
• P2; PCA from origin of p-comm to the origin of inferior toomporal arterieol
(AKA ambient, potitoommWlieating, perime!lencephaUcJ, P2 traverses the
nmbient ciBt..rn. Hippocampal, antoorior t..mporal, peduJlcular perforating
and medial po.tenor choroidal arterie!'rise from P2
• P3; PCA frem the origin of the inferior temporal branches to the origin of
the t..nninal brlU'che" (AKA quadrigeminal ~gmentl. P3 travenlu the
quadrigeminal d stem
• P4: ~egment BitU the origin oflhe parieto-oecipital and ca lcarine Qrteries.
indude~ the cortical branch"" of the PCA
•
•
oplicn.
(er N. II)
. I
FIgure '·10 C"tlf-ol WiUis viewed Irom In lronl of nne below 11>8 briM
Key po in t: the anterioroe~ral anenes PI'~9 over the supe.rior ," urface of the optic
chi asm.
"
3. NeuroanatQmy "lid
phy~jololO'
NEUROSURGERY
ANTERIOR CIRCULATION
INTERNAL CAR OTID (ICA)
Acutely occluding one carotid arr.ecry will eause a stroke in 15·'20'ltofpeople.
Segm e n ts of th e lCA and its branc hes
"Caroti d sipho n": begiO!l at the posterior oond of the CaVemoUli ICA. and enda at
the ICA bifurcation (thus incorporating the cavernous. ophthalmic and communicating
segmentsl" .
C I (ce rvic aJ): begins Dt carotid bifurcation. Travels in oarotid sheath with IN
and vagus nerve. encircled with postganglionicaympathetic nerves (PGSN). Lies
posterior & medial to the external carotid. Ends wheTe it enters carotid canal of
~trou8 bone. No branch~s
C2 (petroua): still surrounded by PGSNa. Ends at the posterior edge of the fon·
men laoerum (f.Lac) (inferomedial to lheedgeofthe Oso.serian ganglion io Meck.
el's cave ). Three legments:
A. verticalaegment: ICA ascends then bends as the ..
B, posterio;>r loop: anterior tocochlea, bends antem.medially becoming th e ...
C. horizontal segment: deep and medial \0 greater and lesser superficial ~tros.ol nerv'ea, anterior \0 tympanic membr/lne (TM )
ClI (Iace rum) : the ICA passes over (but not t hrough) the f·Lac fonning the lateralloop. Ascends in the canalicular portion of the f·Lac tojuxtaBeliar position,
piercing the dW'8 as it pasae8 the petrolingualligament \0 become the eavemo\UI
segment. Branc h.... (usually not visible angiogrnphicallyl:
A carotiwtyropanic (inconsistentl - tympanic cavit y
B. pterygoid (vidian) branch: passes through foramen laceTUm, pruent in
30%, may wotinue a~ artery of pte rygoid canal
C4 (cavernou s); covaNd by vascular memb.-ane linin, sinus, s!illsurrounded by
PGSNs . Passu anteriorly th~n supe~mediaJly, bell<.b J>OI!leriorly (mediall{){)p
ofiCAJ. travelshori:tOlltally, and bends antenorly(part of an len o r I{){)p oflCA)
to anterior clinoid process. Ends at the pro~mol dural ring (incomplete encircles
ICA). Many branchea, main ones indude:
A, meningohypophyseal trunk (1argeat & most proximal)
1. A. "ftentorium (AKA arte ry of Bernasconi & Cas6lnari)
2. dOnll!.l meningeal a.
3. inferior hypophyseal s. (- poIItenor lobe of pituitary): occlusion causes
pit uitary infarcts in post-partum Sheehan's necrosis, however , OJ is
rare because the stalk is spared
.
B. anterior meningeal a.
C. a, to inferior portion of cavernous sinus (present in ~)
D. cap$ular aa . of'McConnell (in 30%): supply the capsule of the pituitary"
C6 (clinoid ): eods at the distal dural ring (wmpletel)' encirdes ICA) where the
ICA becomes intradural
C6 (ophtha lmic): begins at distal dural ring, endsjuat proximal to p.comm
A. ophthalmic a.: the origin from the ICA is distal to me cavernous sinus in
89%(intracavemous in 8%, absent in 3%"). Pssses through the optic canal
into the orbiL Has s characteristic bayonet-like ~nk· 00 lateral angi~
iTam.
B. superior hypophyseal a. branches _ anlerior lobe of pi t uitary & stalk (1st
branoh ofsupraoiiooid ICA)
C. posterior commWlicating a. (p-comm )
I. few anterior thaJaOloperlorat(! .... (- opt ic tfllet, chiasm & po!Iwrior
bypothalamus): see Plnttrior t ireulation below
D. a.n te rlor c ho roldal a r tery": takeoff2-4 mm distal top-wmm - (variable)
portion of optic t r&ct, medial globus pallidus, g~nu of internal capsule a C)
(in 50%1, inferior half ofJ>Ol!lerior limb of IC, uncus, retrolenticular fibers
(optic rad iation), lateral geniculate i»dy (seepage 778 for occlusion syndromes)
I , plexal segment: enters supracomual reteU oflemporal horn, - only
this portion of choroid plexus
2, cisternal segment: passe! through CTUtal ciltern
C 7 (eommun;ea t ing): begi... just prox.iJnal to p-tomm or igin, tTavels bet"""",n
Cr. N, II & Ill. wnninstesjust below anterior perforated l ubstance where it bi.
furcates into the ACA & MCA
NEUROSURGERY
3. Neuroonatomy and physiology
"
ANTER IOR CEREBRAL (ACA)
r"un between Cr. N II . nd ante rior perfol'llurd 5ubostMce. Su 1'16",..5·2. pap
132 for angiornm lind bran~bBlo.
MIDDLE CEREBRAL (MC A)
$eU"lIurt 6 ·3, pag~ 132 fllr a"llogram and branch"'.
PO STER IOR CIRCULATION
VeRTEBRAL ARTERY (VAl
'The VA i8 t he first and usually the l.rGut brllncil ortlle.ubel.'·;"n a rt.l!1")'. V.rianl:
the len VA Bri., oJT the B()I'tje arch in . ... Oi.mft-olr. 3 101)'1. M"e blood flow _ ISO
mllm,n. Thlliell VA i, dominant in 6<H&. The right VA will be hypoplUtic in 1"•• nd the
left will be hypopillstic in S". The VA illltret;c and doe. Dot enmmUniClI1II with the BA
on the left in 3%. lind on the riGht in 2" .
PtCA~I'
a'fI _..urior II'IeII1oIi:Ir "9111'"
1m _lateral - . . . ~ !aud.llloop)
1m"~$Ij1m1.'t11
M _ ~ (wpra:onsIIol H9TII!"
(~.loop)
ts _ COIticiI
~
FllI"'rw 3-1' lI~aI<Ngt ... 1Ihowing In~""'. VA anD PICA RgmII<ItI
"'0<10/'1no<I}'-...,
. \oltIL 1"''''''
..... """" t.c... .. Sa ,ClLao,OI, _
o.o..LoItfln.", Do, AL- o.o.! _
. _ _ I..
...... ..r_r... ___ ...,....",. I_.lOO1.91•• ) 1S6-6111
Four Mlmen ...,
fil"lt legmen!! COUrHt a Upf:riorly and poatenorly and en ...... L'-w fora ruen tron ...
venariulll , "lual1y oftheGth vert.l!bl'lLl body
a«ond IIII(I'ITIen!! a_ndl vertically with in the tnl nlJVUW fortuninaoftheoervial
vetteh,.. . accompanied by a nelwork ofaympat.heu.: fibel"l """m the lteUale gan .
.
NEUROSURGERY
glion) lind II " .. Mug pi"""". It til"", JawraUy will,," the
{rB'llI~ proc: "~
oftl,1!'
~" ~gm~nt: exi t.\. the fOnllnen oftha IU<i~ and curves postl!'n orly and medinlly
third
in II JlToove on u-.e UPI""T ,urf9<1f! ofthll atlaa and en.... n th e foramen magnum
fourth segmen t: pie",a. the dura and imwedint.ely en16. eubarschnoid apate.
Joina t'On tT1lIIl .... ~al VA at tha verte bral co nn",,"a loe!Ited at tha k1wer pontine
border to form lba blUlilar II r!.llry (BA)
BrAnehea:
I . ""terior meningeal: arisea at body o(~ (axi s). may fe~d ~hort\omu or foramen
magnum rneningiomlLf, may also II<: t u collaterAl in "a.o;eular oo:elU!lion
2. pone.rior meningn l
3. medullary lbulbar) aa.
4. po~terior spinal
5, PICA (large&t b,am:h l: \ue Fill"" 3·J I) arise.(! _10 mm disUlI to point wh.re VA
!lacom" intradu ral , _ 15 lI:un proxima] to the vl!I"!ebrobasilar junction (in 5·8'10
the PICA Ila~ ar. extndurtd erigin j
A. "!egmenL&"(acuneaysteml80me deseribeon]y 4). During surgery, the lint
til," mWit De preserved. but lh. lut 2 may usually be I18crillCf!d with min·
imal deficit";
1. auw.rior meduilo.ry: from PICA origin to inferior olivary prominence.
I Or 2 ll bort medullary short circumflex branches _ yeolnl medulla
2. lalen.! medullary; worigin oCnerv"" [X, X& Xl , Up 14 5- \:u-anchut.bat
supply braillllt.em
3. tonllil]omedull"ry: to tonsillar mid portion (tonUlins caudalloolLon nngiol
4. lelov~lot.on6il18r (IU pratOl15iJ\ar): aJ;amdll in toQ.l!iUomedu ll ary liu ure
a
6.
(contain. rot.niPJJ\!:D.lI. on anglo)
5. cortical e~ents
3 branche!
I . o boroidul a. (BRANCH I) ~ri S\lli from crenialloop (cboroid!! l PQiruj,
_ cboroid !,lexus of 4th ventricle
2. tfrminal branche"
B. t onaUlobem.J.pberic (BRANCH 2 )
h. inferior vermian (BRANC H 3) inferior jnfle<:tion ~ ~
JI.!ilill, on Bngio
Mteriorapinal
BASILAR ARTERV (B A)
Formed by th aj unctiou of~lle 2 yert.ebral ~riea. Bran~h l!ll:
I . AlCA: from Lower part ufBA. runS post.erol~Lerally anteriurU) VI, VII & VI II . 0(.
ten give! oITo loop !hal runB loto tile lAC and give$ ofT the labyrinthine 1I.l:tery
lIod then emerge!! to a,,!,ply tll~ anietoLatera.l i"ferior co.:teb~Hum and then ""811tamoses with [lICA
2. intemal auditory {labyrinthinel
3. IJOOtine branch",
4. .uperior Cf!rebellar a. (SCA)
A. J Up. v~rmian
1'> .
pru&t.eriDr " ....... " .... 1: joined by
J>-<'O'T'm~
major origin of the PCA in 15% end ;.
_ 1 ern f...... m o rigin
\.I!rrD~
\ th~
tH-""nTT>m i£
lh~
· feLa]" ~it<:ulatiou, hilateral ill 2%1,
3 ~e,,'-' (named (or sUlTOuoding ciatem.l lind tbeir brnn~be!'
A. pedulltultlJ" .egment,(P l)
I. meseneepbalic )It' rforatmg Ga . (- teetum, ~erebral pedWlcles. and
thl'S~ n"deli: Edinge ... Wes;tphal , oculomotor and tl"l)Chl~a rl
2. int.erpeduncular t bnlamoperforatol'fl (l al of 2 groups e( poIIterior
Ihalamoperfor&ting aa.)
3. roedia! post. choroidal ( tn<l6t from Pl or P2)
B. Dn,bient ugme.ot{P2)
1. lat.e"'! poIlt. chorcidaL (mlllll from P2)
2. thal&mogeo iculate thalamopcrf"oratora (2nd of2 groupo! of po&w.rior
thal .. mOj.>l'.rWrating A~.)_ g@niculatebodiea+ pulvinar
3. antoorior t.empor"l (anastanwiell with anletior tempo",l br. ofMCA)
4. poot.erior !.IImpornl
" . pari~eo·ot'ci pital
NEUROSURGERY
3. Neurosnatomy and pby!iology
"
6. .,.learine
C, q\,ladrigeminal Sl!(l'ttM!nt (P3)
1, q ... lldrigeminal & genicula~ bnnchu _quadri,cminal plate
II post. pariulJoaal('plenia1) (1UlIl8tIlU:lOIu with periclIllOilftl of ACA)
E XTERNAL CAROTIO
1. aupermr thyroid' III anterior braneh
2. Alloeooine: pharynruJ
liogual
... r..,;a1: bran.ch.. ana,"'~ with ophthalm ;~ Ikwy in rol1ataralllnw l
5. oocipiUll
6. posterior lIuric:lliar
7 . aupcrficia! telJlporal
A. rmnlal branch
8. pAJielal hranch
8. maxillary - initially within parotid ,I.nd
A. "';ddle meni'IjIar.l
8.
IIHIninp.1
C. inferiwal .. toI)lar
D. inf'r...".bital
E. Dthen: dial.al branch" ofwhich me)' an.. lO_ with brarKh... orDph.
thalmlc artery in tlla orbit
a.
_.0.,.
3.4.3.
Cerebral venous anatomy
S UPRATENTORIAL VENOUS SYSTE M
SM FiB"" 5·4, page 133 r",. lltIp:.gr.m .nd braneh ea.
The len. end richt intema l JuguJar ... ina (IN.) are the l7Ia,ior -.un:e or outllow 01
blDod from tht: inlr&Crllo;al companment. 111, ri&hl. IJV i. u.uaUyd~minlUlt. Other
iOIJrce! or our.f]nw include orbi1.al veill.! lind the vertebral W!nDUS plul!!.. Diploic and
&Calp veina Illay act .. collate... 1 pathwayll, 01.1 . with ,uperior ~tu l t iDUM ohatructioo".
Th" followlne oUllloe uaces t.I'. e v"noW! drainage back from the UV • .
A.. inferior petroaa! Jin ...
B. aivrnoid . inuB
I. I " perior petrosallin u!
2. traru;ve~ sinw; (R,. L in 65'1»
A.. v. ofl,.a bbo. {inferior an astDmDtie v.1
B. ,xmfiuefl5 ef8illllSe~ (IOrcuiar benlphili)
1. 0«!pltaI61 ........
2. , u perior .agitUll 6 inus
g.
w. of'Trnlard tsuperior 8na.llwnlIItk ... ): the p ... m'j nen~,uparl'icial
vein lID the Illm·dominant!hie l .... bbtll it...",.. prominent on the
d(>minlll)t aide)
3. alrllight sinus
a. inrerl~r ugittallinu B
b. grWot cerebral v. (orOalen)
i. p re·cen t. a! cv.,.bel1l1J' ...
Ii . bsaal .. ein of Rc8t!nthal
iii. intemal cerebral ...: jolnl!<lat the fMalDen orMonro
Ivenous aIlel.) by:
I. /lnt.eriQr kptal v
2.. th,lama.lri.t.e Y,
CAVERNOUS SINUS
Althoulb ch'IMicaJ tel:lcb inl depitU: thl! caveruou , ~in"""" allr,e venoua,pfou
witb multip ~ trabo:!culatioll8, ll\il!Coou It"dlu" and ,urgical experi~ I IIPPOrl.ll thl
...{ t he caVlmoU' Binu,
pll :\uMofvelll8.
I. contrib ... tinl! "elnl :
concap~
"
u.
3. Nll'Umana1.om), ind phyRI(>logy
NEUROSURGERY
A. , upol'rior & torerior ophthD.lmic "em.i
B. l upemcia.l middle
cerebral vBinS
C. sphenoparietal ' i-
"0'
D. superior &: inf"'; OT petroSD.1 ainul
2. contents:»
OculoUiotu n.
(lll)
Trochlen r n. (IV)
Ophthllimic divi_
s ion o(trigeminal
(VI)
Muil illrydiviaion
of trigeminal (V2):
the only ne ..... e of
tbe CS"erDOUa ai-
'I
nu.th/l.t~.n'l
exilthe skull
through the iUpe_
rior orbitallissure
(it Hits through
Figura 3-12. Righi ca.emous sinus (ooronal sectloo)
(Modilie<lbom IM J OVmli OI ......
F. ~...., f1.
r"r"ln"n rotun_
N..lIIar!. VoI.~. pp. Z28-3oI, 1982 • ....., I)etmlo.oiOn)
dum)
C ",.ot id
Abducens n. (VI): thq only ne ....... NOT alUlehNi t.o IlIter!il dUTllI ... ttU
3. triAngul ll r 8J'Iacel"r PDrkin~"n ) : s uperior bord~r fonned by Cr. N. 11 1 &: IV, lind
the lower m8 r(in formed by VI & VI {II landmBTk ror BlJrgicD.I entrance to tbe ell .....
emou s SinUI»'·" '. ;wn
,_rv-r,
3 .5.
Internal capsule
Vasclilar ,"pply or the internal cap, "le (I e)
I. anterior choroidal: - all of ~trolenl.iCtllar part{indudes opti<: radial;on ) and ventral part of poat~rior limb oflC
2. latera l stri ate branebes (AKA capsular branch",) of middle cerebral artery: mMt of anterior AND posterior limbo of lC
3. genu uaually r«eivl!!! some direct branc b"" of the intemel. carotid artery
Most Ie lesions are eIIused by vascular e(~identa (thrombol!is or bemorrhage).
Table 3-10 Four Tl'Ialamic: "Iubradlallona" (AKA Ihalaml c: peclunc:les)
(!abeleo A.0 In F">gUIB3 /3)
-- ...,"'"
..."" ......
......
RadllUon
I~
oentrallh/Jlanie IIIJ- gere,al ~ Ir!lelS I'om boItt
,olandic:a'eEl$
'"
DCcipMl & posIerlor ))lin.
1'1
.~
posIerior
i1leoo,
101
"'"""'"'
ConMCIIon
medial & ~le<lOIltIiIamic
IllInlMlrstl temponli 1If'
rusol Hesctll
NEUROSURGERY
3.
-
'"
& head 10 tefn*lale In posICen-
MOB
(smaU) Ir1c\uOeIl ;JU(jitory radWil -
!IaI~s(OIJeu3,I .2l
CII\II8I )I'Ialamus
N~url)an8tomy
""
and physiology
"'
3.6.
Miscellaneous
OBERSTEINER·REOI.ICH ZONE ( O R Z)
AKA root entry toue. Tr&-'' liition f!'(lm eNS myelin to po!riphera! lI\)'clin of cranial
'" area whe~ root ~ntry zone p",ssure fmm inllll~rnniB] sW"ucrurea CIIn caUSftCrtl·
I\I!rv~
nial nerve 3ymptOmt (trigeminal
ne"ralgi~.
hemifl.dol apa3m, disabling pOllitional ver-
tigu, e!.l: ,)p. Also, zone where neopla.m5 U:'nd to occur, l!!lpecililly aal!l.tic neuroma . On
Cr. N. VIlI , the ORZ is 8-12 tum dilla! t.o exit point from brai1ll tem, Bad is dose to porot
8custicus (e&peci ally common on ve.tibular division Y" ....I.
DENTATE L~MENT
The spinal IICtellS(lry nerve is dOrMl to theden t.ate tigument. 1be denLllt.c! ligamenl
fi.ep8ratf's do""aJ from ,·.. ntral nerve fQOl.S in !.he spinal ""'rvel.
3.7.
Neurophysiology
3.7.1.
Blood-brain barrier
'!"he paaaage ofwater-lQlubJe substanCl'll from the blood to Ihe CNS is limlted by
tight jW1 t1.ionll (um ul" .. ocdud"D~ ) which lire found between cerebral ca pillary eodo1.belia! ""IL., limiti"!! penetration "r the "",,,bra! paraucbyma (b!<>Od·brain barrier,
(BBB»), lit well as between choroid pluuB epithelial celL. (blood·CSF' barrier)". A "urn·
berofspecialired mediated Lraru;port sysloelOSal]ow trIInlmisshm of, amc ngothcr tbinlJ$,
glucose and certain amino acide. (especially preeursOl"li to neurotranamitteTII ).
The "ffi""cy of the BBB i. eompr"",ised in ""rta'n p~tbological ~tates (e.g. tumor.
infection, lrauma. stroke, hep;atic elll.'I!phaiopathy. .. I, and can al!lO be manipulated pharmacologically (e.g. hypertonic monnllUl increases t he ~rmeahmty ...... her~s sloeroidl! 1'<1duce the penetration oramall hydrophilie molecules).
The BBB i~ ab&ent in the roUowinll areas: dlOroid plexus, hyp(lpl\)"IIi" tuber ci.
ne reum, srem paatrems, pinn l and preopl ie n!'CeSB.
3.
N~uroonatomy ~nd
phl'llioiOO
NEUROSURGERY
CEREBRAL EDEMA
Three balic types (dif!"u.ion·w.. ight.ed MRJ may be able to dif!"ert>nti.te, Ht JXl6t 136);
I. "ytotOld ,,: BBB is closed. the ... f,,", no protein utrav ..... tilln. then!fure nG en·
cr
hanoement on
or MRI . Cell ••well then .brink. Seer. e .•. in h u d i.,jury
2. v" lIOg .. ni,,: BBB disrupted . Prol.ein (serum) INk. out of v..cular IYttern. end
the ... fon may .. nhllJ\Ceoo imagin,. Extra"",llular'paee fECS) upand •• Ce ll •• re
stable. Responds to cortioosl.e...,id. (..... dex.met ........ nel. Seen ' " .lUrTOund inll
metastatic brain tUmGr
3. i,..,bemic : . combination of the.~ BBB c\oted initia lly, but th.n may open.
ECS shrinkll then upandl. Fluid .x tra vallal.ellate. May aUN d.. l.yed del.e'ioration following inlra"", ... bral hernorrh"'. (_ ~ 8.S$)
3.7.2.
Regional brain syndromes
This section IoervU to brieRy describe typiaol.ynd .... me .nociated with Ieoion. in
variou8 areu of the braIn. Unlu. otherwiMl not.ed, Inionl conlidered Ire dtJ!oli:m:...
I, r.on t allobo!!
A, unilaterlll il\iury:
l , may produ"", few clinic.1 findi .... ,x"'pt with very I.rge Inioou
2. bilaur.1 or I..ge unilal.e.,1 lesionl: apathy, abulia
3. the frontal.ye field (fGr contral8l.er.1 gazel dlocated in the poIIl.erio.
frontal lobe (8 • • a. ea 8, , hown I I th u triped area in Fitu", 3·J. page
68). Deetructive le,ions impair gaze to thecont •• lal.eral aide (patient
lookl .llU!Llllh the .lde of the lu iGn), whereas irritative lesions (i.e. lei ·
lurn) caule the center to activate, producing contralateral gau (pa.
tient looltll ~ )'!'lll. from the side Gfthe luion) . Also IIU pagt 584
B. bi lateral injury: may produce apat hy, abul ia
C. Glfactory fioova rtgiGn : may produce Foster· Kennedy syndrome (see bf,low)
0 , ~fronta lobet control "exec utive runction": planning, prioriti:;ng. orga·
niling tholl4lhta, suppressing impul8el, understanding the OOflsequencet of
dedsionl
2, parietal lobe: major featuretl Cst. pog# 87 for deta il9}
A , either ,Ide : conical aenlo,y ' yndrome, sensory extinction, contralate.ral
homonymous hemianopia . contralateral neglect
B. donei,,"n! parietal lobe luion (len in rn<>St): language disorders (aphasilll),
eerttmann', sy ndrome (_ M t 87). bilateral astereognosis
C. """.domin,"" parietal lobe lei''''''' topographie raemory Iosa, anosogTlOliia
and dressing apra~i.
3. occipiullobc: homonymGul hemianopsia
4, ""'rebellum
A. leaiGni of the cerebellar Mmi.pM", cause atuie In the jpsilateuJ l'robs
B. letion. o{ the cerebellar vennis cau"" truncal aluia
5. brainstem: usually produces a mixture o{cranial nerve deficilll and long tract
findings (1ft Mu.w fo.- some specific brainsl.em syndromes)
8. pineal region
A. p.rinaud'. ,yndl"OV'le; 8ft pap 86
FOSTER-KENNEOY SYtJQROME
Ul ually from olfactory groove CIt media l third aphenGid wif\i: tumo , (ulua)ly menin_
gioma). Now nlre due to earlier detection by CT KaD. ClaAic triad :
1. ipsil.teral anosmia
2. ~ centra l scotoma {wi th optic I.1aUili:t: due pressure on optic nerve}
3. contralatergl papilledema (from elevated lCP)
O«lIIiooally ipsilateru l proptosis will also OCCur due too.bi",l invuion of tumor.
3.7.2.1 .
Brain stem and related syndromes
W EBER'S SYNDROME
Cr. N. III pally with contra later.l Mmipa reti. (a lso 1M LDcu ..o. "fOott" PIIp 716).
Third nerve palsin frGm parenchymal leaionl may be ..l.tively pupil .pa rin • .
NEUROSURGERY
"
BENEDIKT'S SYNDROME
Similar to WebB'a, plus red nucleullellioll. Cr. N. 111 pals)'wilb rontrnl8~TlII hemi·
Uceplllml which hn hYP" rk.ine8ia , atu.io, and a CO'n<! ;nto;nlion tAmo •. Le·
s ion; m>dbrlin Io!ymentum i"Y01 ~; nl! ~ !lucie"., brllthium col'\lu llttl.V1,m , /llIIf fllaeitlel
oflU.
panstS
M II.I..ARD-GU8LER SYNDROME
Facial (VI I) " abducenl ]VJ) pal.y . contralat.er~ IM!miplegia ((:(Jr tlcoapinsl lTatt)
from Leaio<1 in hue. of po ... (1.IIIIall), iKhmic in faf1:t, oo:euionally tum or).
PAR/HAVD's SYNDROME
Con~rrence • • a:ommod.tilKl fInd IUpr'lllicla. r upwnd gaze pIIllIy \I .• . U ppl~ pill ·
a)' wilb nO"",11 .tllponsa to yO!l1.lc.l dol1'l e)'u' wittl lid retmetion (" Pia .. pilla), + lid reo
trlKlion .. ".euill' a UD . i.,.o). M-.y ha~e fuctd pupils, dinoo:iated liJht.-ne8r responae,
convtrgeme apelm and n),IIUIJIIlUI re lrac.toriu • . Skaw ~.tion mil' be a unil/1teraJ
~arianl. When combined wi !.h downga .. pall)', I'arinllud'aI)'JIdfOUll (P S ) i.lLnllWn 11.'
!.he I),od ""..." ollila Syl";lIn Iqued u c:l .
E ti o logi el
l. 1IUi.u1 pAHingdirec:tly on quad ripm;nl l plate (1I.g. pineal region tumOrl)
2. eJ~.ted ICP: MICOIIdary to c:ompl'ftSion of~phalic teclum by di\ated~u·
prapinul noI'' ', "" . In hyd.rol:tphllllli
Diffe rential diaguo. i.
Condition • • rrectine oo:utar mati lit)' thai could fOlmic the u pglal! prills)'of f'S:
l. Cuilla.in· Bam
2, m)'ll5th.nia pv15
3. bot'uLism
4. hypothyroidism
5. !.hen ma), t.. gradual benign 1_ OruPi'lI18 with sene_ nee
.,nd.o:ne
3.7.3.
Jugular foramen syndromes
Ccmuntf orjugular ro. al:'lea (JY):
Cr. N. IX. x, Xl , pelTO$ll K\nus, $IgmoId
.l nlll , lOma m~i ngeal branch .. tram the
__ ndin l ph8ryngeal and oo:cipiLal
aneri~.
Nearby: Cr. N. Xl i p.iI$~ Ihroulh
hypoKi08la\ t'III'Ial in the OttIpital
""nd),lll. Theca. oUd IIrt@l}'wi!.hthl!aym·
pathelic.pluu. enlerl the carotid canal.
See Tobk 3· // for II I UDUna1)' and
Fig",. 3 ·14 for a ochemalic diai"UD of
denc;\a in various JF synd romes.
~ha
Vernet'a "yn<irome: AKA ,),ndlOnle of
th ejugl.llar roramen . Damage or lll! .... es
;n J F it.llelf, mo. e Liktlydue to ;Ot rlC'rIDI.
1!11"10n.
Co lJe t.-SiC8rd syndrome: Mo re liJr;ely
with J"ion Qlm.iIlll.UwU. Ifcaused by an
inLnlc' llDialluion, ilwould hive to "" or
IIUW a la rge .iu l h. t it wou ld uluaHy
produce brain stem comproll:.on - lonl
tract finding ••
VlIlaret', .,.ndrome: Postarior 1'1111'11'
phl!ryng~a l
"yn d rome.
Agu.. 3·'.
~kllIne
Sc.he1Tllllil; a.~'.mol ~ lor..
mM .... ndromta
tnrough • nerve indIcIIlet a dIfId\)
IdW>ed line IncIical.,. ~
.
"WEUROSUROERY
Table 3-11
3.7.4.
P{lRIETAL L08EANAT04fY
The parietal lobt: II loelli.ed behlnd tha amU'a l .ulcu., abo¥e the Sylvian fiuure,
mel"flnll' posteriorly into tha ~pit.ol lobe (the border on the rDl!dial.urfB("e of brain i.
dllfi ned by II line connect ing \lMIl'ariet.o-o«ipitallulcu. ta lhe p...orcipit.ol nOld>l,
PARIETAL LOSE' Nf!UF/()PHYS/OI..OOY
elth~ r , id.: . ntenor parlet.ol CONK organi,," tactila pre.:ept.s (probably conUlllatera l) and inwt;ra~1!I with vUIII.I.nd IIliditar)' -.nsaOon to bu ild awareness IIf
body ond its IlPltial relaLioli'
domiNlnt $id. {on l"ttln 97-' of ad u lu }: unds",unding 18ngu11lf, iIIcludl!fl "cros.s.
mod.l mntchlnl'" (a uditory· vieu",], vlsual.u.rtik-, ete,). DysphMi.a pres<mt wit h
domina.nt lobe lulan. olU:n impedellWlln$men t
non.do minant .id~. (r i,hl in m()lll ): inleiTl'~ vi,ual and proprioceptive $\Inliation
to allow manipuillion of body and objl!"Ui, and ror e~r\.lli n toOSlroc:UonalllCtiVi-
tiwi
CLINICAL SYNOROMES OF PARIETAL LOBE DISEASE
l.
unilotel'lll pruil'tallobt di!M.'aat (domman l OT non -docoill8llt):
A. eorllcal HI'ISO r)' lyndrome /~ w lmu) aod HMOry eJ<ti.n~tian Cneglectilli l
of2 .imultanl!9us]y pre6f)llted GLllnuli ). Large lesion - hem i8nl!lt huil
B. congenital Injury - mild hemip~resil & conlrll iatetal nill.de atropllY
C. homonymous hemianopls or visual mattenli venM5
D. aa:a,i(lIIaJly: anOllCllnOO!lia
E. neglect. of eont.:ralaural balfof body .nd vi~u 91
(moli! COOlmon with
right . ide le$loruJ
P. .bolition of ontokjn,yc O\'atarmull ta OIle side
2. additiona l effect.! ofOOm;"''''1 parielS] lobe l!!Iioo (left i..., mOllt):
A. la ngual" d~rde~ (a phuias)
B . • p<!«h· related Or verball,. mll!distfd [email protected]·lIIodalm.u:hing
(e.g_pati~t unde.-.lJmda lpol",,,, word. lind eM .read , but o;/InnQt under·
nan(! Mnteneell with eleDlf.nlll of.elationmipa)
C. Geutm.nn ', .,...dr<>m~. clal!liQl.lI,.:
1. agraphia without alex.ia (pw.tienu Ull f1l&d but cannot wriU )
2. left..rigfu confusion
3, digit agnosia: inabUlly to idt= ntify tin&f-r br .... m.
4. aetlk .. li.
D. tacti le qnOllia (bilalAl.. I .. Ie!1!Ogr>uSi.)
E. bilateral ideomotor .p.....,u. [ioabllity to;.:any out vuba l tonunandl for lie·
dvi lles th a~ c:an oth_1M! be ~rformed apontanl!9U1ly wIth NN)
S. addiliOflaJ effecu of """,-d.omillOlll parietal lobe te.iollll C.... uaU,. nihtl:
A. topOgr:llphil: memory 10lIl
B. anOlOgnOllla and drealil\r.pn>t..
'p_
NEUROSURGeRY
87
CORTIC AL SENSORV SYNDROME
Letlion ",fpostamtrnl gyT11S, £specially 81"118 that mUJlII 10 hand.
llensory defitit ~
A. loss of position ,""nN and of pa!l8lVe mOVemCnl sanae
B. inability 10 Io<:ul.i ~ l1Iotile, therm&!, Ilnd noxious stimuli
C. ps~reogn06is (I nability to judge object Sil~, shape. and iden t ity by feel)
D. agnphesthesi. (carutot interpRt nu mbers ",riLUn on band)
E. 10llll o(1:WQ poio.l dilOi!rimination
preserYed un9alionl: pain. lOudl, pre!l!lure, vibrst ion, temperatu re
other feature!!
A. easy fatigsbility of.aen801"y pe=ptiOl:\I
B. difficulty distincuiahiog ,imull1lnOl(lu8 atimulanOlls
C. prolongstion ofauperfieial pain WiLh hyperpathia
D. toueh h 9Uueinaliool
A SOMATAGNOSIAS
A NTON· BABINSKI SYNDRQt.fE
Un ilaUiral a!lOlDIIltIgIlosia. May &I!~m more common with non-uomina nt (r ight) pa.
rietal luion, ~lIUU it maybe obscured by Ihe 8ph!llli~ that Ottu". ....ith dominant(len)
sided l"ioM.
1. 1ltI000000oaia (indiffereoce Or UnaWllTeneSli ofdefioit.s, patient may deny thal paraJyud exlremity il r.l1eiral
2, a p'llhy (indiffe rent" 10 failure )
3. olloc:heiria (one ... ided 'limuli percl!ived contrelaterally)
4. dre5Oiinl: apl"!ll<in: negl~tof one aide of body in dreslllnl: \llId grooming
5. utinttion' eontTnlaterall,y 1.0 double· sided SlInultaneo ua ~timu lation
6. inattention 10 nn en tiN visuallield (wilh or without homonymous hemianopia),
WIth dl!viation ofhud, eyea, and IOn;on of bod)' to unalf~d eide
APHASIAS
All related to parie13l lobe lesioll!!:
1. Wernicke's . ph .... ;,,; lea;on of \ludita-ry 8I1!111ciaLion 8""111 nr tbeir ,epa rati on
from anguJar gyrus am! primary auditory rorte". A.D.llllll aphasia (normal ten·
ten~1! length &. Intonatioo, devoid ofmean ing1- May indud .. paraph.a.silll. Lealon
in region of Wernicke·, area (Brodmann are~1 40 &. 39. l ee FiC"'" 3· 1, Pl'1:1! 68)
2. Broca'a (motor) aph_i.: in reality, "8praxla" of motor "",uenc;ng for speeoh
(Ipeech and phonation muKieR aren"l parll]y~ed, and fundlon for other nd-lVi·
t inl. prod ucing faltering, dyeaJ"\h.rit Jpeech . Lesion;n region ofBroea'a ar~
(Brodmann area 44 , ' '''' Fig"N! 3· 1, page 68)
3. globll illpha ,,;n; us\U. lly due to lulon that dellrOYI large port,on oflangual:a
tenUlr; aU IiBpects of speech and lanb'Uage affected
A. unab!" to apenk "xeept for lIO!tIe tlicho!s. habiu.al phrases. or expletives
B. anomia Unnbilit)' to name obje<,:ts Or POI'\.S or otl,iecta)
C. verbal and motor peTSeVenl t;on
D. unAble to und~'.tlltld an Ut .. pt fo r a r..... wo.d&
E. inability to read Or write
4. coaduction \lphasia: tua to disniptiOll o(connections l>etwee.:l fronl1ll and temporal apl!etb areas, usually involving supramarginal gyrus. Si milar to W~mjcke·a
U1uen~ spontane0U8 spe~ sod psrsphui,..l. b"'l patielltl! undel"lLllnd spoken or
wtitt.m words, and are aware.of the;r deficit. Repetition i9 severely s lTected
S. pu.re word bUndnf!S5: AKA Ilh~a ill without ag"I'lIph;1I (rare) due to lesion in pa.
rieto-oc:<:ipitallobe thu intf!rrupl.ll conn&etionl bIItween left angula r SY"U and
bot h oc:<:ipitallobes. Pntienta Mn write, bUlllJ"ll unable to read what th.ey've written, and freq ueotly uem Wlconco::moo nboUI thii. Often ncwmpanilld by low of
ability to name .:(lIon. Reading and naming number. usuall.Y preserYed
3.7.5.
.
AltllQugh
Babinski sign
~b'lltdlld
as the mO!lt f8mou ~ slgn in neurology, there it still di ugTHmI!nl
3. Neuroanatomy and phy!liology
NEURQSURGER1·
over what constlu.lles a notmal rupon"- and ... hcn .bnormlll r1!.!p<InSE1l !hould
'The following
rep~"nu
OC(U~'.
onc inl<lrpretation.
pl .. ntar ren ex (PR) (AKA BabiDski aign) i.!I" primitive rene)!., present in inr"ne)" conailting of extenslun of the GTeat lOt! m IUpOll!!<'! to" nCIlI:ioWi ! bl1lulUfll,lpplied
to th e foot , The~malll.oell may fan, but W . r. nott'l)ntii~knt no r cHlllully rmpO~nL The
PR diaappeanl u8ual1y aL - 10 lDont .... age (rang~ : 6 !liD!! to 12 Y1'S), pres umably UIlder
inhibitory control u myelination oftha eNS OOC\1r$, and the IIDI'1'DII] .espanae then eOn verU to plantarl\""ion of the greet toe. An upper motor neuron ruMN) Jellion anywbenl
along the pyramidal (eorl ioospinal) Irlltl ITom the mowr strip Wlwn to _lA will ruult in
a 108& orinhibition, arK! the PR will be "unmasked" producing u le/ltWJn ofLh .. great toe.
With auch IUl U/To(l'Ilealoo, there may also be eX3Jgeration arn.xor ,,),nerK)' n!l!ulting in
rlon;ifle..Uon ofth a ankle. and flexlon ofth~ iule8 and hip (AKA tripl e nOlIor ""lIpo ll fe).
Th~
Ne uroa n a tom y
Th~ affennt limb ofth~ reOex originale! in cu·
lAneous rl!Cepto~ restritted to th e first !;acraL dermalome (S1) and travel~ prQx.imal1 y via th~ tibial
nl!I'Ve. '!'he ~pin81 cord Hgruenta Invol..oo in the renex-an: lie within Li:li2. 'The efTe:rent limbto the t£Ie
exten50111 tnovela via tho !l!!roneal DCal!.
Eti o lo gi ea
Table 3-12 DI!ferentlal
d iagno,ls of the PR
spinalooro~ies'
cervicll SPinal !l'l)'elopall"t'
6on'l in <I'UOr SIIIp or tt:emal C8~
I\I~ lell.... 1Umor, conwskln .. )
Les;OIlS producing '- PR Deed not be ,\ruc!u... l.
but may be runctionalllnd rllWl!reible. etiologi~s an!
Ij,lA.ld fn Tobi~ 3-12.
wtQ,'aIO! epodulll! t-1«M
Ilydllmeraphaly
loldo;.melabok COII'IiI
Eli ci ting the PR, and vari a ti o n s
$8Ilures
lrau!!llo
Theoptimal stimu h,s consists ohHmulnlion flf
the lalera] plalllAr I Urf""", and l,anaverK areh in II
henIJp. mIg,;une
I llIgle movement IMtlng 5·6 1!IConM". Other means
moIOI neurm disuse (ALS)
ror applying noxio", atimuli may also elicit the plan... spinIIl CtlId Jr.tu--. 1M FR .... y
tar refln (even oUl.8ide L'>e 51 diormatoMe, although
~ I~· t>e _OIl d-.gl/le PlflClCloI
these do not produce toe nexion in lIorm.I~I. DI!.
$pfI\01"1I\Odo.°I_page ~
scribtld m.neU'·era inclu:le; C ha ddock (&er atch Ih\'laleral fOOl; pGIIitiveln 3'\to wb ..", plantar stimulat ion was negative), Schaeffer (pinch the Aehllles tandon ). Oppenheim (Ilide knuckles
down shinJ, COrdOll (momentarily 8Queeu.lower g~stroene.millil). mng (light pinpriciu
on darsolateral ~I ), GondaorStr QlUlky (pull thl! 4th or 5th toe down /lnd out a nd allow
it to snap back!.
"'"
Hoffmllnn', .iltD
MIlY signify a almilar UMN InlnTuplion to the upper extremitl<>&. Eli(;lted by Jna",
pillJl thedis!al phalanx cf the Iniddle finge-r; a p8thologicresPOIISllroll5is ~orthumb nexion (may be weskly presenl in nonna ls). Can $Omelimes be see" AS normal in YOWiG
individual wilh dilfu'l<!!) bri~ k renexes &. poiIitive jaw jerk, usually I yrometric. When
present pathologically, N!preunts disinhibition ofa CB re n8lt, .". ind ieale!llNion ~bcNf,
ca.
3.7.6.
Bladder neurophysiology
CENTRAL PATHWAYS
The primary
coordjn~ting
eenl.O't ror bladder fundion re-
sides within the nudeu8locu~ coerule u8 of the pons. Thi BOOnIA.lr 8ynchroniu!'I bladde r eontraction with relaxation orthe
urethral sph,lIcle, during voidin, ..
VOIW\t8ry cortieal rontrol primarily "wolvei inhibition
of the ponline ren~, "lid Otigin81.O'8 in the anternmedial por.
FlgrJr. 3-15 LocaliOfl 01
lion "rthe frontal lobes .lId in the genu of the rorpu~ callospinal cord bladoer eN.. •
8Um. In an uninhibitt!d bladder (e.g. infanQyl the pontine
voidingcelll.O'T rUllclions wilhuut ""rtiCIII il,lhibi tion !lIld lite
detrosor IIl"aderontr.ctswhen lite bladder ru.ch ua critia,,]
capaci ty. Voluntary .uppre"i~n from theeol'tel< via the pyl1llOidal tract may r:ontratL tha
e~ternal aptlinclerllnd t:lay alIIo inhibit detruwr rontraction . (."orticalle.e.iofUI in this 10eaU"n - urgency ineontinence willt inability to luppr,," th~ micturition renex"".'''IJ.
Elfen!llt.i; to Lhe bladd .... trllyel in IhedoNl~1 portian ofth .. !al<!ral ""Iullln. of the spi_
NEUROSURGf:RY
3. !'leuroanlllolny gnd phYlliology
"
nal cord (ahaded areas in Figan 3·/5).
MOTOF!
There are two aphinctera that pre,·ent the flow of urine from the bladder: internal
(a utonomic, involuntllry control), end external (striatOO mu""le, v"luntllry control).
Paruymp athe Hca (PS N): the detrusor mo""leofthe b!addercontracts and the in·
ternal sphincter relaxes under PSN stimolation. PSN preganglionic cell bodies reside in
the intennediolater al grey orspinal cord segmenta ~_ Fibe,... exit e8 ventral nel"l/e
root.s and travel via pelvic splanchnic nerves (n ervi e ri&"<!Dtea) to terminate On ganglia
within th e wall of the detrusor mu""le i.n the body and dome of the bladdCl'.
Som etl c ne rve ..: somatic voluntary oo nltol descends in the pyramidal trM! to syn·
apae On motor nerves in S2.4, and then t ravels via the pudendal ne rve to the e><temal
sphincter. Tbis sphincter may be voluntarily contracted, but relaxes reflu.ly with open·
ing of the internal sphi ncter at the ini tiation of micturition. Primarily mainl.pin8 <:<lnti ·
nence duriog I vesical pressure (e.g. val88lva),
Sympa the ti c.: sympathetic cell bodies lie within the intermediolateral gray column of lumba r api nal cord from segments T12· L2. Pregangl io nic uon. pass through
the sympathetic chain (witho'J t synapsing) to the inferior mesenteric ganglion. Postgan·
glionic fibers pass through the inferior hypogastric plexus to the bladder waU and inter·
nalilphincter. Sympathetics heavily innervate lhe bladder neck and trig!."'e.
Sympa thetics have little effect on bladder wowr activity, bu t alpha adrenergic stimula·
tion results in bladder neck dosu re which is neceQa ry for bladde r follinII'.
Pelv ic nerve stimulation - increased sympathetic tone - detrusor relaxation & in·
creased bladder neck tone (a llowing larger volume to be accommodated).
SENSORY
t...,.S!; well UJlderstood than motor innervation. Bladder wall stretch receptortl sense
bladder lilliI'll' lind send afferent signa19 via pelvic, pudendal and hypogastric nerves to
spi nal cord llegmentsT10·L2 '" S2·4. Fibers 85C8nd primarily in the spinothalamic traot.
UAJNAAY 8LADOEA DY SFUNCTION
The tenn ne uroge nic bladder describes blAdde r d}'$Function due to leBion~ within
thecentrai or peripheral nervous systems. Some use the tenn synonymously with detru·
sor arene1<.ia.
D0r881 (sensory) root.lll~ions interrupt the afferent limb, producing a n atonic blad·
der that fills unti\ dribbling and overflow incontinenC<l """",r. No sensation of bladder
fullness is appN!Ciated. Volun.tary voiding is still possible, but i~ usually incomplete.
D.:!trullOr hype .... eflcI la: Can result fron. inten-uption ofefTerents anywher e from cor·
tex to sacral cord. When a cri t ical volume is attained, renex bladde r emptying occurs.
Clinically associated with frequent, uncontrollable, precipitous VOiding. Cerebral lesions
indude: CVA, head injury, brain tumors. hydrocepbali.18, Parkinson'a disease, various de·
mentias, and MS. Cord lesions include anything that causes myelopRtby hee Myelopa ·
thy, page 902).
Detrusor llJ'eflcxia: Clinica lly correlates with difficulty initiating micturition, inter·
rupted now, and significant residual urine .lnro ntinence may re5ult from ovel'-rlilltention
of the bladder (o ve rflo w Incontin en ce), Or may be assodale(l with absence ofspblncter
tone. EtiologiC!:: indude: ch ro.:l.ic infection, l<'lng.tenn bladde r csU,eteriution, certain
droi:ll (es~;aUy phenothiazines), injury or lumor or!he cauda equina or conus med·
uUaris, myelomeningocele, aod diabetes mellitus (autonomic neuropathy).
In general . rega rding discrete neurologic lesion! affecting the blsdde ....:
I. IIuprlUlp;nel (lesions above the brain stem )' loss of centrally :nediated inhibition
of th e pontine voiding renex. Usually produces involuntllry bladder contrllction8
with smooth and striated ephioc\.Cl' ")'!Jergy, often with p~rved 8ensation and
volunUlry striated sphincter function . Symptoms: urinal)' frequency Or ucgency,
urgency incontinence, and nocturia". If sensory p!lthwa}'$ are interrupted, un·
consc1OUII incontinente oa:ur1I (incontinente of the unawares type). Since muscles
are coordinated, normal bladder pressures are main tained and there is low risk
of high· pressure related renal dysfunction. Voluntary bladder emptying i, usual ·
Iy maintained, lind ~imed voiding together with anlitholinertic medicationll ara
used in management. Areflex.ia may sometimes occur
2. complete (or nea r complete) "Pinel cord I~ioo"
"
3. Neuroanatomyand physiology
NEUROSURGERY
iI.bmr.e. the 52 ,pinal ~ level. which is ~ T I 2/l..1 ver'
tehral body level in an adult): the sacral voiding center is located in the co·
nus medullari$. Etiologies: spinal cord injuries (after spinal shock bas
5ub~idedAJ . tumon;. transverse myelitis _Usually develop de!,Cu80chyperre.
Jll:xi.lI- involuntary bladder contractions without sensation (autom at ic
bla dder). smooth sphincter synergy. but stri ated dyssynergy (involuntary
contraction of the extema l sphincter during voiding which produce. a fi.IJ1c·
tional outlet ohstruction with poor emptying and h.igh vesical pressures).
Bladder fills and emptiea .ponlaneously (or in respoOBe to lower extremity
cutaneous s timulation). Bladder compliance is ofu!n reduced. Managed by
intenl)ittent catheteri1ations + antichohnergia
B. intT8IIIIcraliH io n s (lesion below the S2 spinal cord level): includes injury
to conus tneduLlaris, cauda equina or periphe ral nerves (fo rmerly referred
to as lower motor neu ron lesions). Etiologies: large HLD. tnuma with com ·
promiseofapinal caDal. Usually develop detrusor sreflexia. and do not have:
involuntary bladdercontractioo8_ Red uced urinal'l flow rateorretentioll re-8ulta. and voluntary voiding may be lost. Over flow incontiDeDce develop6.
There may he reduced comphaoce during Iilling. a nd pa ralysis of the
smooth sphincte r. Usually associated with lou ofbulbocavemosusand anal
wink rene:.: (preserved in 8uprasacral lesions) and perineal sensory l088
inte lTUpti on o£the peripheral .... ne:o arc : may produce disturb.ilnces similar
to low spinal coni injury wit h detrusor arefle><ia, low compliance and inability to
relfUI the striated sphincter
herniated lumba r disc: (su fJOIlt 302) most consist initia lly of difficulty voiding,
.training. or urinary retention . Later . initative symptoms may develop
spinal8tenosi. (l umbar or cervical): W'Ologic symptoms vary. aod depend on the
spinal level(s) involved and the type of involvement
cauda equina syndrome: usually produces urinary reteotion. although sometimes
incontinence may OCCU r (some eases are overflow inton~inence) (sec fJOIlt 305)
peripheral oeuropathies: such !Ill wi t h dialxltes. usually produce impaired detru.
SOr activity
neurospina 1dysra phism: most myelodysplastic patients have an a reflexic bladder
with an open bladder neck. T he bladder usually fills until the resting residual
fIxed e~ temal spbincter pressure is exceeded and the leakage OCCUT$
multiple scleros is: ftO·9O%0fpatienl.8 develop voiding symptom$ at lOme time.
The demyelination primarily involves t he posterio r and lateral columns of the
cervical spinal cord . Detrusor hyperreflexia is t he moat OOmmOD urodynamic abo
normality (in &()..99'I>0fcnes), with bladder arefluia being le&l common (5-21)%)
A. IIuprasacr a l (lesion
3.
4.
ft.
6.
1.
8.
9.
URINARY RETENTION
Etiologies of urinary reten t ion:
1. bladder outlet obstruction (a briefdiffereDtiaJ diagnosis list is presented here)
A. urethral stridu re: reteotion tends to be progressive over time
B. prostatic enhu-gement in males:
1. benign prostatic hypertrophy (BPH) & prostate CIInCer: retention
tends to be progreSllive ove r time
2. acute prostatitis : onset of retention may be IIlId!I.m
3. rare: extruded prol!ta t ic stone
C. women may develop a cystocele whkh cao produce a urethral kink
D. rare: uret hral callter
2. detrusor arenexia (u, poe, 90) or hypotonia
A. s pinal cord injury
B, cauda eqUlJla syndrome (s« page 305)
C. chronic infection
D. long.tenn bladder c8 theteri~ation
E . certain dn.lgs (narcotics. pherlOthia~ioeal
F. injury of tbe cauda equina or COIIUS meduLlaris, o. of the spinal cord at or
below the sacrom
I. tmuma
2. tum<>r
3. myelomeningocele
A. durin&: , pin.1 'hook
<- pop 698). <h. bl .d~, i •• ttmtr. ",iI"
. phin ... , IO<le ...u. lly ~" .... ood urin. 1')'
d_ Ml O«\I r e. .. pt wi'" ov.rdi.lenhun)
NEUROSURGERY
~ te nli o n
""d ... Ihmc
[~truso, . ~n.,.;. ~
i. Lhe ",10 (urin.ry in<oon.i .... """ re • • "lIy
3, Neuroanatomy and phyaiology
"
G. di"betH mellitus (eutoll<lm,c neurop.thy)
H. hup" '<lISter at the lev.! flf Ih" u~r.1 do .... 1root langh . .. '..•..
I. ;nCllmplete openi ngofthe bladder neck; OCCUJ"I .Iroost exclusively in young
males with lonptandinl flbslructive and irri tative Iymptoml·. ··"'"
J . following severa blooder over disteo~lon froo, M)' flfthe abQ ... e
3. postoperative re~nlion: weU·rtc:...gruted but pOOrly und.,..,IP!ld. Mureeummoo Ir·
~r lower urinary tretl , perineal. pneoc:olnlk and f.l)flr~t.l1 o!'l •• tion•• Melilh",·
,ia and enal~.ia may colltribute to. nurn'M r offacto...... '. ...
4 psydl"lenic
EVALUATION OF QUDOER FUNCTlON
URODvN"M/CS
Urou.Uy tOmbined wIth :..."" (o;y6to .... lrnIfr.m (CfttG)1 or nUll"" (v id*"u.odynam.
ICil. MeMllrel inl ...... aieuJar pruaure. durin, ,..trognd~ blBdd~r mUn, through" urethral catheter. usullLy comhlMd with Iphlnct.l!r electrolD)'OllJ""phy. ~Hnce or ablente
td~lru""," .~n.l<.i. ,.u k/.,...)oI"detru"". ,..flu il detected. Ifp.uent. plVtedur. is repeeled. askin, plltient to .u~reSl thl! UTi" to void. Inability to I UPPI"dI i, CIJled "n un ·
mhibittd detrulO. re.nu IAKA detrulor hyperrenexil • .Ift oboo<! >.
SPHINCtER ELECtROMI'OGIIAPH'f (EMG)
Eillw.".. needle electr0Ge6, Or .... ith externaJly lD(>u n~ w rflrotl e:lectrodes. VoIu,,uny .phincter CUnlra~I>Ofl ...... IlIl.aM:tnea ol l uprlUlpinal innervllti(ln. When CClmhin!l<l
w,th CMG, det«ts eIHlrical.divity;n Iphinden during Usocillled "hue!" ordelruaof
contr1lrtion.
VOIDING CYSTOURETHROGI«'" "NO INTRAVENOUS PYELOGRAPHY (IVP)
Void"" c)'ltou.e~luvcrn m (VCVG ) del.e1:t\I u",wlIl paili(ltogy (di vertkula, stric·
tUtes ... )' abnonm.li til!l oIbla4der (diverticula, detroSOl' ~tabecul.lio.'1li" Usocillted with
ionpu..ding contracl iom apin.t high rN ilt.llnce ... ), Ind vesical-ureteral re!lulI: ,
T REATMENT
Goa.Ia II'f to prt&erve renal funttion (wh'~h lUI ually iovolvilS p,..,veotion ofUTb,"'"
filii clIlculi, and ureu.ral renu>; due III high int,..,yesiculu preslUres) and opti millition or
utinllry rontinem:e. Palient$ "',minad~uate emptying or incre.sed bladder preuure
I,.., often II\3nlged by intermittent c.th.~riutiGIII I nd I1Iticholinergica. Anlicholinerti""'lInd beiulvio ... 1 the..py an used fur patients with mIIintained voluntary blldder
emp~y'ng w,th Utlnl!"), frequef1cy or urgency incontinen~.
3.B.
,
,
References
_1<~ TI';",a ''''''' afn. .." ... -.-,..
_..........., ])tSowI~~.~,
0 , . - G. 0,-- J.ldlKlo E. n ... ~..;n'
' - ' '..... Il1<01 .............. _
.............
"'ft","""ltlot _
.. _"'"""'""-....:.~ , .
In 1'"''''''''
) ''''~.I,"
Sorut.I"'."',..IN 1..."""',.,... """', ..... _ ........
j,....,,""*""' "
...."" ........ ..,-"",-...,._,.,.. "
....... In ... _, . .....
•
,
•.
..
•
("_~ J_-.
76: 101-"10 . 199:WI" .. WD.Gt_.RG ,...""""_ ........
~ I.MeoIic>oIMMI"CIIIioIoslr ("V_.lI
1....~.),d .d
. ' 91j
pp'91,'.
W.. U;~ R. w ~Iw... ~ L,I" . ~
Grv-o_,.
}S"'..t. WII . S..........,IoIIoIjoIoI. '97)
Ki40D,LlMo1 M. LI.",_" .,• . C~ ....
"""..... lorolb.oo_oltht _ _ l)"IrO • •••
'"""",,1.J) 11'-T,IUO
M.MI,....Go.n...S.\I,_F .....~ I_""" .
""'''''' .... """", r.OM)oo.oIIo<"'''_ C....
"
w._ ........ . ..l1>li_.'''I.
~ 1I'
_
1»M. I"'-1.
I [ C,-·..u.. af~ "'<11, T.
101"...... 11 " •• _"""'S S.(.... ,): .......
-..., ~·IIiI.Nt .. Y.. ~ , t~ .
..--.,w.
lMMLI. K... rL"_"' ...
_ _ JooI ............... Mc<Ijnj_...
.... 0Ii<. ., 197l.
eo.o,.l.C.... I"l<Io .... ......,..".aI_,pI_
_
, . . , . . , . . _ )1'<......... " fIH. '9IS
W.. I.J"'IIG' ......... <____
....
_101,..,.... __............. I. . . .
" ...v
.."" f'Icw 't'-" ''ill' ' -6
roo.. . _ _ l>t'1Ioo
"
"
"
~
lIP
~"L, .. . ,...~-.Io-
poo.o.< ...
....
_~
~
1'I.. -.,..,4 10s..JIIII~S'.I).' 1'I ,
n_JM . Woocle" , ~
___
ItJ 2flCl0II w _ _ W.l... aoll_. 't'7t.
T _ I ~t Stria .... H..... O' ' _MlII"Yoi
NEUROSURGERY
,..."um"...
"
'''"«f''O<lI . .....
A",,~ph.
l<uob,.,,,1od) I N.",,,.. ,~ 1~ ~1 1 · 6S , 196ol .
" . do, Z ..... 11. . Hill.,. 8, TW. ~." CAl'. to oJ ..
v.",,,;mr
,.m'OI'ie>o/ 'IIe ...)OI' """'b .... ...
.." ... J """....... '1
IWl
g(,,,,,
'1, ,:r...o.
doI._
•
E.
"'lI'ab....!chunS'"
"c F;I<""
~lm ~"""Id. Z<.lnlbl "".I'fI<""'l'JOI).
»
"
"
" C
Die
"
"
"
U
"n .
,"C
tII~
l1. 1911.
Sot.,l\illiof II ..... I,.c""... H M. Kd" J1' kII·
...... 01 ,II< in.."", , orOl..! ~fJ" A ...... <I . .. ,n ·
.~,.'). I'M
K"1,.1>Uh1 H. y..,..,,, MG, R"",,~"'
_,,~,",j. tU~M"W/O'" I. 7......, ...... onKler.'
"'pblt!lo. ~I;nit. ."d p",". Hobo, r .led.)
TIl, .... Y.,IIS.S,""'"'" 1m : ".,*:016
""""" "".,,,,,,,,:,,,l1:
E<~ ..
...'...,,_d
Clout,
A. il.. _no<,iIorI " I\; '"A.~phlc
Io<.oU .. t~ofiat ..........w ......... ,ClI .."' C. n ·
""" •• s""",r.. kJ.III ,,,,,, •• ' 9" "".)l ,
K"I~.t.Ii,., H ,. . y ... ",,11ot G. In C...... "'I •• •
"",""~~r O"'" .... """..LDnd<>o. <n<l 00. 1%Ii ' pp
It<M W H. R"'"" II l.: M.crooIIr£lrnl_r"f
,...... It..-"',;,., J /'<'C\I ....... ~l· lU·". 191)
R""""'"L.II. Tb<_ ....
Nt-u .....
••• ,... , " (' S-rplI: SlJ.l20. '.!CIOl.
ll<t<,) R.R_ "L.~"', ... oI>I ... T "DI~ M """
.... JI<~ ."'''''''1 or .... "",:<<i<!1 ;01'...... """boll ..
...." ",...--.-..,.,. 10 . 11'\).99. 191:1.
C; ...... CC.O':i"*'''' ....) 0
91(,<1<11.,
s.u.,<01 """'"l"meni of ,_o&! _01)'''''' :..
".
"
".
N.
'_flf'l II
NEUROSURGERY
_""'I.
J N........"" 7~: 1IJ7.
y .... "') 1t.(N 1 "' ......... &1<..........,.,. ltt<l,,,j .
"'. 8 s..oden.Fh;~~; • . 198Z.
1....... rl, MoIlaM 8 .MoIkrA R-~r"'...,.
>11-.1 "¢IIi,o, /I t:nal J Mf<I )10' t100-).19SoI
_ ,n.._
Ncu"",~ EII.O"",. P .... MtCormo<k C ~ "DI<
O' ..."' _ _ 'Ht.om..
M...,.
.,.,.,.,""i_-".• lb~""",.uMl _ _ "'IkU•• "
U.
.. « _,"not IloMl.,a !>n". N"reAI'II<'" 11
.,9·11. "IllS.
$ ..... H). lIoI;" H I.. ~ : .... lot H' I.!.,. "" ......
.)'00""". ....,
".
11._
"
... ... ,....
0<IIc:.., """...... fo,,,,,', _ ,;.,.. •• ,r"9n .
u.. (toIU ..""
"
vol.,., .... (><»..- ..fu.,,«I'Ob:II .. ....,.,.c.....
U.
f'h<,
''''''''.n<1\n
""'P 1'''''''"'''11 26 (9)1 ,·7.:I00I
S<ltrnidU II II ,,,,,,, l M. ;'; ... p l P ' T"'~
""_, ')'SkIIl,Nor", ....,"'.,. 11 64.1.78.. 192~
TlpIa ) N' no: _.I""_~ " ~
k '"
oftl><_",,,,",,,,,, k. ,.,p(i<OI ... , r",,,..,......,.
' ...... I01 ...
712·1.11>11.
l>ioI:""'''''''' ,.....
.... 1119' .
~ , .
Gil>o H ,t..."~yC.~"L.. Mo<_~".'",",·
"'"r or,1I< .opn< IONHd ~"on of",. ,...mol ......
........ , ' J N"_"' J"· ~l'.l98l.
....".,
Soklla> I.N· ot>m>"~_"',
,0'
~0>1.3 '''' __ ..... , 1.. ",. 10 To"..,,,. of .h •• r.
aial_,
I>O •• ,.s........ I./'I
..., S<~_ Y L.I..:I>.I. fIio"," P\d)~""", . M""",
Jtn ",~, 1911. ppst~I~ .
u..-.~ , F. """"," H' Tht "'''''oj . . 011 or,,,",,,,.·
• .,.,." ....... "'iU 'l>"<t.1 ,..r....-1"1II< Moon ,.·
101.. ,,, • . J N."~" . , 16 22&.1'. 1~1
"01.40 .... II~. ,...11 .. JT.E'·KalIOI)' M. ,,~.
.U'''' ' r _ N....o!ou
:""..,. Mo;(in.".n,tl. "'~ yert\.. l'ltl
MaItu. I C Flo.", ~t.o .......""""'" I. ct..~1r<"
.. io~ """". _
""""'" Ic:< ...... olr<b " ...1'01 4'1
1, 9!t .• • lm.
OontnwInCJ. _0<1; W) , Th<
trn. "'"
O!>Ii ... l""""""of<I i< ~_I ......, \ J39.4 ' .
I9'7J.
~ -n. 1\J!C>' t>J" "'."".,'" bia'.l<l<r
1oI"•• .......,..,,_ . C"""""p
H.I999.
.(>10'"
• "'OI:Di_ '"
~.
(J,
191.!109.llio6l.
Mom' It D. Y'n. M: Pri"'lpI .. oe ........ ,"I1.
"'_0.,11(.,·
w, "' ... J N'"'_<></rIQ'dpf'<M''''''
."""'"".<, ,.,.,.,,,
~_'. ln
"'ii < "'_,
C_pboO', . _
"11'. w.l>~ P C.~,riIr II B. "'_""" t o . .,oII.•
fOll'.I. WO ~.I'b;"",,,lpioio. 1O/1«1 .• IWIi.
Y'" !. Cbopl<'" I'l' 9ll·loot;,
3. NIllJroanDt<nOlJl end phY8'(lingy
.''''
)
.....
•
4.1 .
Arachnoid cysts
4.1.1 .
Arachnoid cysts, intracranial
AKA le pto me ninge al cy~te . di stinct frompMllro",.."IU: J~pt.Gmeningeal cyst:!
(AKA growing sku ll frfIctW'ft, _pa£~ 668), and "nnlatt:d to i"f<!Cl ion. Arachnoid cy.1.a
(AC) am eongenlUillel!ion. tbat arise du ring d .... elopm(!.nt from splitting IIfsrac:hnoid
me.obrane (thu y they nre tecl1nica lly jntrfH.rochrwid eyst.s).
"Tem poral lobe agenes;, syndrome" ix II label that had been used to de/lcnbe the
findings wIth middlecranilll J"ossa ACs. This leon iii now obsolelesi..cebl"aln volumes on
uch side are actu ally the l ame'. bone expalUJon and shlfl of brai n malLe' accoun t fGr the
pa.renchymll that a ppellrll to be rl!plsced by the AC.
In cidence i5 5 per 1000 in ftUl.Op~y series.
Tw o type. of histological find.inga·,
L "!limpl\! IIncbnoid t yau": " .lIchnoid lining with ceUs that apP'!lI r to be tllpllule of
active CSF s.ecrelioJl. Middl ... fo;lSSl cyst.<! seem to be exclusively of IhiB tYJloi!
2.
cysts with tnore:complex lining which may slaoOllntain neuroglia, ependyma, and
O lh~r
l i,o;su.,
type~
PRESENTATION
MoslAe" thaLbecome symptomatic do so
in enrly childhood'. The
presentation varies with
location of th e ~Ylt. and
of'l.entiruu appear mild
con sideri ng the large 'Ii ze;
of some.
Typical prllsent.a-
tions are sMwn in Tllblf
"_1" and i ndud ..,
Tabla 4-1 Typical presenlaUona 0 1 araehnold cysta
- --Mldd ll los·
.. ,yt l.
SuprastUar cy5l1 wllh
hycl,ocep!lalul
-,
~ant.l1
headache
h)1le1lftnSior1
hemiparesis developmental CIeIir~
'iWa11oss
D,l1uaa I Up"'" or Inlra!flllOf1.
I I cyJts with hyc!racephalus
inUlICIa"lia! hype<1ensroo
ganiotr~
~mernaI 08Ia~
I.
~~"'!1<111'~
symptom$ o(;n·
t rBerani,,1 hypertension (ehwaLed l e p): H/A, NN,lethargy
2.
eei~urea
3, ludden ddt.(!rioration:
A. due to heloorrhage.(into cyst or au bdllul cum Pllrtment): middle fO&" cyst>;
are notoriou . for hemorrbagedu!! III t.ear1ng of bridging vejlUl . Solue sparta
organj~tion~ do notaUow participation in OIIntact$port5 for thue pat ienUr
B, dlletoruptureoflhecyat
at a focal protr"u~;o n aflh., s kull
wilh focal BignliaymptOn-.. ofa space occupying le~ion
incidental finding di scovered during evaluation for unrelated condition
7, su prasellar cysts mlly additionally prellent with':
A. Jl,)'drocephaJIUI (probably dne to compfl'alIion oflhl' third ventricle)
B. endocrine sympwma; QCCUN in up 1Il6O%.lncludea precociou./l puberty
C. head bobbing (th e t a.ca lled "bobble-bud doH ayndrolue"): con. idered lug.
gt!'St.iVl'-o{ , uprll'l4!!i IlT cYlib!. bu t O«UTS ,n aa few at 10'J>
4.
o.
6.
4. DevelopmenltlJ anom~Jres
NEUnOSUnGERY
D.
vi.ual lmp&ir!llen~
OISTRIElUTION
Almon all OC:CU r in ,ela lion to a n arachnoid cisU!rn {ncept;\ln: iotrasellu, the cmly one that;, (!>i tradural, • • TobI~ 4.2). RetrOCt<Tf!belbr arachn oid .:ya18 may mimic DandyWa lker malform9tion
{Hlgf! 110),
Table 4-2 O!stribullon
01 arachnoid cvst.·
<1ft!
EVALUATION
Routine evaluation WIth CT Or MRI Is u5ually l at15fao:tory_ Further eval uation with CS F c"ntra~t Olr now 6tudie,
<ciste.rnograms, ventricuIOlgralll s ... ) aN! only occasio na lly
"" _
ry for u,ediogn<>llis "fmldline suprOl!lIltar IlIld politerill' fosSIl !esioll/l' (ror DilTe~ntia l diagnOl;Ls,.", llllr<U:f'Qllj.
III C)'51~, page 928). See Fig~~ 4·1 for da..sification rOl,
middle fOSSll cysUl.
CTSCAN
Smo<>th bord ered non-caltilied ext.aparenchymal cyatic
Clan wilh densi ty .imilar t.o
CSF and no enh.ancemeDt with
IV cont,ost Expansion otollllrby
bon~ by remodelling is usually
""eD, con finoiog their chron ic
ORtUN!_ OlWn lISlIOCiated with
V\!otriculoClegaly (in 64% of 6U pl1lU!D t.o ri a llllld 110% ofinfrat.en!.Oria! cyata).
Convellity or middle fossa
cysl.9 exert mns5 effect on Blljaoonl brain and may com;J Te sslps HaU!rallate ral v"ntride and
[)ll u9O! midline shill. Supnuellor.
Q:uadrigeminal pl a te. IlIld midline posterior-fossil eyst.s may
compra.a thathird li nd founh
ventride aod c8 us~ hydrocepha lus by "bstnJcting the foramiDB
or MonrOl or lhe Sylvill.n aque-
Typtt l: ~ bioorrve~ kx:;ol
ed in anIIlrior letnpo!ll\ ~. No
mass etfeet. Communic::aIIlS
"'~h subilrac:ll1Oid Sf*:e on
water~DII! conlra>! CT cis·
ten\Og'iIII1 (WS<TC)
TI'JlII !t i'1'foflof!$pr~at'Id
jrtemmte segrnenls 01
SyMa~ flSSlJ rct. Comptelely
opeI'l Jnrdl giVes r~r
5hape.. P,ni,1l COOYIlIJRicaIIOO
on WS-CTC
dueL
MR/
Br.tler than CT '" different iatinll the CS F contained In
8,..dlnoid ey.;11 from !.h.. tI"'d or
ne<lpillstie cysts. May aJli<) show
cy5t
wal ls.
CISTERNOGRAMS ANDl'JR IIENTR/CULOGRAMS
Us ing "'i ther iDdinated cont.rast or radion uclide ttacer1
Variable rate of Opaeilic8\.ion W
.... ~ulted in diflkulty correltltin g
r p3u!ta with operntive findings_
Sollie cy~t3 are I>(:tuo]ly d ive rti.:.
u!p. aoo may fiUw lth rad.ia tracer
Type IP~ rr.ot.l!S entire S)1v~
an IissuID. Mallled mdile
shin. Borty e~panslot1 01 mod·
die lossa (elevalion o! lesser
wing o! spheooId. O'J1WartJ ell'
pansion of ~s terlIPGral bone). Minimal
communblion on WS{:T C.
$Ufglcl.llreatmem usuall'f
does not resu~ in IoIaI rtol'~
pension ot brain (may 3:1prOilch type Il te$iOll)
Qrcont,.,.s ~
NEUROSURGERY
"
TREATMENT
Mlllty t but n04 a ll ) a .. thon rf\COmmend not trealitll/ aracltnoid Cfst.& thai dOl not
tIOUN mlln elTect or symptom" ""lIrdll!M ofthei. ,iu and 10000tion. Sur';..,.) tMalmeRl
optiona are iummariU<! in 7"blfl4.:J.
Table . ·3 S u.glc..llr •• lmfill opl lonl lOf . rachnold eylls
CYST SHUNTING
Probe.bly Ihe ben O~1'1I1I treatment. For . hunting into peritoneum, """' a ~
I(u......, II ronm....,..t ~.nlrkulomeIt8Ly. on. may 8imult&n~u!ly place" ventocu.l •• Ihuntle.lI'_ I.htoUJb a -r conneccorl. Ultratound. ventricul<I8tQpe, or 1m.
guidaDCOlmay u.is till lcatlngsuprll.\lllllarqets. Shunlinrofmiddle f0Sll8 AC. mil) o[so
be a«OQ'lpiahed through tht Jaleralvenlride , thUil shunting bot-h almpartmvlI,s',
nIlS ... I.....
5uPAASElLAR CYSTS
TI'1I!8tmenlll propDlled intlude;
1 In!inS(:llIiI)$lJI tyt;~Wrmy "
I"'n:utaneous vlrolricukM;:yuostomy' procedure of eh oiA orPielT8- Kahn et "I.',
Puforroed via. paramedian roroaal bUIT hole through U\e IIIUlr.1 ventricle lind
fo.amf!n of M ooro (may be r.dlluted by u&ing a venlricul~~)
3. lubf'rontal.pprQoaCh ffor fenennl;on OT R!mo¥/ll~ dongerO<>Ii and indf~I !¥'"
4, • ¥entnculllr d .... in .. I~: inefT«tjv" (aclu;)lI), promoleS C)'lI I en.Iat'Jemen t)
2.
OUTCOME
E'I1!n follow.ng IU«esslu! tl'\'/Ilment . portion ofthec)'S( ma)' remain due to the rft.
modelinr of the bone Ind chronK ..hilt 01 brain tQIltenu . Hydl"OCl!ph al u8 rna" develop fo4·
Iowiug t ...... I~I. Enclocri.nopalhia tomd to pt!BlAllI>'en al\er IlIC"a!Q flll ,."lItm.. II' of
'"pn.sellBt C)'116.
4.1.2.
Arachnoid cysts. Intraspinal
4.2.
Intracranial lipomas
I nlTl~nl. lllnd .Mrupol!.allipom" /lR rel~ 1.0 be fir maldevelo;Jfl"lenltil orisin" ,. ....
ud mil" anN! from failunt otin¥otlluan oflha pnmilJve mMin".. 'l.
Epidemiology ot i.ntra~l"'llJ)!a l lipo m/ls
Inddo!nc.t: 81n 10,000 outopei"". U'''11I" round In or near lh.e llliduCl t tllJ pl.~,
pIIrticuiorl)' over the corpu'Qlllo.um (I'pomas UI ,hi, ",~n a re frequently • _ _ ted
"
4. De .. ~opmen\llI.llOmll;es
NEUROSURGERY
with »genesis ofthe eorpu.. (lIU""um,~, /Xl&" 114). 1'h('. tuber ti nereullllln.d quad rigem·
inal phl teare
frequl'ntly affected". Rarely , u.eCP angt,",orc~rehellar ...emlie may bf:
involved. May oc:cur in isolation , bu~ also has been dfSCribed in anociatiOIl with anum·
bu ofoongenital anomalillS. Includin,: tri$omy 21. Pai's syndrome. frontal encephala·
cele. fecial anomalies. ,.. Other midlineabnormolitielS may . lso be found: ogene8is of!.he.
tOrpu~ CIIllolJllm, myelomeningocele, and spina bifida" .
I",
E valu a tion
May be diagnosed by CT, MRI (study ofchoieel. and by ultrawUJ1d in Infanl8.
C'J': Low dene' Iy, rtl6Y hay,", peripheral caJcifie>llion (difficult Lo apprec'iate on
M RI J'~_ Oi rrerentisl diagrOllia on CT' primarily between dermo~ cyst, teratoma" and
ge rminoma " .
MR I: characteristic finding l& a midline lesion with signal ch... raCterlslU:~ orfot
(higb int.enaily on Tl.Wl. low inten5ity OIl '1'2\\'1/.
P r p.s e n ta tio n
Often discovered incidentally , u lr'ge Lipomas may be assoc:ial.ed with sei~un!8, hy.
pothalamic dyarunction, or hydrocephDlu8 (pos6lbly from oomp r1'Ssion of the eq ue<!uet).
..... sociated findinp that mayor tIlay not be directly related : .oeotal reUirdalion , behav.
iora! dillOTders ond headHche.
1'reatm ent
Direct eorgical approach is Hldom nE'Cll&Sll1')' for il)tlllcr~niallipom.81'·. Shuuting
OlDy be required ror caSO!'! where hydrocephalu8 n!sulta fron, obstruction ofCSP
circu lation"
4.3.
Hypothalamic hamartomas
Hypothalamic hamartomas 8m rnrll n(Hl-neop!a.tic oong.mitAl DUllfonnDliona <'lll1'
.ilit ing ofnuu;ses Ofec:lopic neuronal tissue thot arise rrOOl t he ioferiorhypoUllllamul or
luber cinen!uttL
Cliniea l rnanl festationfi include:
I. spedfic types of&fltures:
A. gelll.Stic (laughing) ""zurea: the mOt'll characteril;tic type , Res;$lant \0 med·
luI maml,ament and can lead to COf'titive and b~l!.avio.. 1defidl.ll
B. 19l.er development of complex pHrtial &f!izures, d rop aIUlckB-, tonic seizures.
tonic",lonlc I"'lures. and Sf:<:Ondarily generall.ed liei,un!a
2. behayioral disturbance3 : aggreniYe bfhavior, Toge allacu .. .
3. prec:ociou. puberty
4. menuol teurdation
5. visua! il1'lpairmfO:
'I'wa subtYJIU ofhypol ha18mic hamartom88".
1. pedunculp\.el:l 01' pIlrahypothaJamie: MrT'Ower base al taet.e-d to the floor of the hy·
pothalem\l.ll (not Bri8ing wilrun hypothalamu s), Tend to produce precociOO8 po ·
berty more t han they produCIi'-gelaslk sehure.
2. s-esaileor intrathalaml<:: broad atUldllnent to hypOthalar.:ou li. More often associ·
alA!d with gelsstie seilUre9
Treatment
Treatment .ltern&t'v8ll:
1. medic.] tTeat.men ~ for precocious puberty
2. .Iereotact.ic ..di .... uf'£')1')'
3. ~u tgieol resec:tion
Indieolion" fllr surgery:
I. precodOUI puberty tIl"t faiia \0 respond 10 meo:!icallhera?y
2. );I!lllfllc .eizo res: no effectiVil med~ll therapy'·
3. neuroll1(ic deflcit from maSlleffect or the tumor
SUrgicaloption8:
I. ptt>nonal approach
2. tran_lIosal anten or interfomiceal"
3. neuTOt!ndO>lCOpicapproach: difficull because vel1tritl" aM ra rely dilated
NEUROSURGER Y
4. [)"v.. lllpml!flUlI
anlllllDHe~
4.4.
Neurenteric cysts
No uniformly ao;cepl.ed nomendature. Working detinitOo n: . CNSc)'It lined byendo.
thelium primarily rtllembl..ina thatoftheGi tract, or le$&ol\en, the rapil1ltory tl'toct. Not
true neop{umll. The mostcolDnlon .ltenatt term ill e n ter oge no ul c y a t , with 1,.. oom·
mon
U,>rm:i
including: tel1ll.olllatol.1f; cr-t. intntinoma, ar(:hentenc C)'It". enttl"Ofene
cyst, and endodenllal c)'It. Uwally affect UM upper thoracic and cervical ,pine, a nd other
associated developmental vertebral.nomalin .r. commoo",
&'-0 oc<:u r Intrac... n;.
ally, including 6 reported en" in thi! «rebellopontine angle (CPA)" . S pinal neurenteric
cysts (NEe) may h.~ a fistulous or fibrou. connection 1.0 the GI l!'IId and lOOle c.1I
t hese e ndod erm a l .inu . eyat t. ' " - are thol1lhl tooccur al. rnu lt ofincompJett developmental separation of the noe.od!ord from the primitive guL 'MI lt is di, tinct from ;"'"
!.led intracrani.1 entero&eoou1 q at&..
fool.,.
C lin ical
MOII( commonly prueol d",rin, the r\l"5tdecade of Ii,. ... Pain or lQ~lopathy from
the intraspinalma.. are the mo&t common presentation. in older children and adulta.
Ne'mal.cl and)'Ol.l"l children may preMnt with cudiorupi ratory oompromi.e from an
iMrathoracic mas. or cervical Iplna! cord compreMion'". Meningitit may Ottur from the
fistulous tTact. upec:iaUy io newbornl and infanta.
Hi stology
MOit are sim ple c)'t'" lined by cuboidal_ lumnar epithelium and mucin secreting
goblet celli. Leu common typet of epithelium described include: stratified sqUll11l0UA and
psludostratified columnar, and ciliated epi thelial cells. Mesodennal componenu may be
presen~ including I mooth mu.-:le And Adipose tiuue, and some have called these Ulr·
stomatou. cy."'''·'' which it not to be confUHd .... ith teratomaa which are tn>e germinal
cell neoplum • .
Trea tme n t
Complete removal of.pina. NECI usually reverses the symptolll8. An aoiherenteap, ule msy prevent completo ~jon of intracnmial lesion&. which p..,wSp0se8 todelayed
reaJlT~mce and mandal.cllong.!.e nn follo...··up.
4.5.
Craniofacial development
4.5.1.
Normal development
F O NTANEL LES
6.u.tJtri~_ntJ!Mlli::
the largest fontanelle . Diamond shaped , ~ em CAP) _ 'Hi em
(transve ... e) at birth. Nor mally d ose. by age 2.5"..,
~~Q[
footwel!e; triangular. Nonnally doses by age 2·3 mos.
and mutoid fontandl«: arnall, ilTegular. Normally, forrnercl_. by a~
2-3 mos. latUlr by age I yr.
~
CRANIAL VAULT
Growth: largely determined by growth orbrain: 9~ oradult head size J. achieved
by age 1 yr; 95'lo by age 6 yn. Growth esse ntially ceaaes at age 7 y .... By end of 2nd yr.
bonn have interlocked at l utu"" and Further (I"Owth Ottu ... by accretion and absorption .
Skull i. unU.minar at birth. DiplOe appear by 4th yr and reach a ,oa.xJmum by age
35 yn (when diploic veilll fonn).
Mastoid pl'1Xftl: fonnationcommencu by age 2"... air cell formation ox;cUIli during
6th yr.
.
4. Developmental anomaliu
NEUROSURGERY
4.5.2.
Craniosynostosis
Ori(ina\ly caUed cr.n;Oiteno.i~. InCldf'llce: ~ 0.611000 liO(f: birth •.
Pn"lIl1ily' pT. natal derarlOit)', po. Lnatal cranio.ynOlltoaia (CSO) occu"' III><'OJl}monly (postnatal "ause. cone;~t pri n •• rUy orpoilitioD~I . lt. •• lIon. which roay not repre" "l trull l ynClltotitj. CSO ie ,...,,,Iy nlOci,t.d wilh bydl'l'lClphalui {II CP)". n.e
I&sftrtion that eso may foUow CSF Ihuntinl for HCP II unpNtVen Iior(' ~ J99). Other
calll~ (or f, ilure ornonnalaku U gTowth inc1ud a llickofbr.in growlh dl.le lo AAY orlhe
"~III""
orarrelted d8Yelopmf/ltol'the eerebnll
ria, ~e (.II~ea ofhyd'LlItnrtphaly... ).
hltllli , phe~1
Uiu enoa pha ly. micropalm-
'I"r'fatment;. WlUQUy furgiCIIJ. In roost LllllIIncE'll, the mdiar.tion ror 'U rJl!ry .. for
(0;1111"11 and ttl p",venl the H~re l"'y1: holoric;alefflct.! orh.""". didipnna d,l'orrni·
I)'. HOWl!vtlr, with mult.lple eso, brain Vrowth IN)' ~ im~~ hy th e unyielding .kuU.
Abo. fCP may be pIItholoBically eleYlited, lind a lthoulh th1& 1& morealmmonln multiple
CSO". el<!vjlt.!d lC P oc:~u,..ln_ 11 ~ or ca~uwllh, s iDI1e,t.enotiel utute. Coronal.,-na.·
w.i. ean ta use ~mblyoprll. MOiI\
of'inel. IUlunllnvolvemenl un be trea~ with
linear neiaion of the l utu re . Inv olvement Dfmuh.iple I Uluru or th s kull bue ulllla lly
tit."
r elluj"" theoomblned effort. of. neU(OiIurgtoOn and eraD.iof.cillllurgeon. and /NO)' nead
In till ~t8Hed in lOrD" ca_. Ri.u of I Uritry ,"elud.: blood 10M, te\1,,-,,",. I tnlU.
DIAG NOSIS
Many caJeiI of -'yoOllw.ia" .... ",Ilty dua to p(NI;tionlll noUe nil\f (e. r . "I.Ey l.tmb·
doid". au IH:lowJ. U thit i. '1Upeete\t. inslJ'uet parenU to kttlp need olfo(n"IWied are.
and tllcbl!Ck palie al in 6·8 wttlu: ifilwu poiIit.ional, it lhould tA impl1M!d. if II was CSO
then il ul uully dk l" ..... ILllelr. The di .......it a f CSO may be . i~ed by .
1. PIIlJaoti<>n of .. bony pl'OminellC1e DYer the IUspected 5ynoatotie autura\UOIption.
lambdoidall)'1l(lltDllil,.t b./ow)
2. I':~ntlfl finn pr~u~ ... IUl tha thumb. Wl.t to
I'\!1JU;Y8 moye~nt of the
bones on either lide of the luture
3 plaia sku\! x·ray.:
A. laek ofnBI'"/I'UIJ Juoen l;)' In centet"ohut"l"e. Someee_ with oonna l x· ....y"".
pearance of the ""tu", (even 00 CTt "'B)' be due \(J fOUl ! bon)' .picule
ronn .. tion""
B. boos ten coppt!r calvaria 1_ ~~ 101), sutural d'liSllIlht snd .."",iOll ofth",
Hils maybe seen in cases ofinc",8IIed ICE-t CT_n:
1<" hel .. demanal.raLe c:t'onlal rootour
B. ros)' .haw ~hickening andlor rid~ng st the aiLe of,.,..,_i.
C. ....11 demo .. alret.e hydrooephJ ... if preseIU
D. nuoy . h_ expuaion of lh. rl'Onl.ai l ubaraclmoid sp __
E. ~hree-dim~Ii~ CT may help be~ter vi .... liu aboormalities
6. ;n queationsbJe ......... a technetium bon .. Ile8n tIlIl be p:-rformed"':
the", it liWe ilolOpe uptllke byan)' ofthec:t'l ni el autu,," in the til'llt we;!Q
ot"Jife
• in prematurely clo-.nrsutures, intruHd aetiYJt1 almpam to the oth~
(normal) . uturel ...ilI be demonll:tnt.ed
in compl ..tely cI~ IU~U""" , no uptaka will be de",orun.T~ted
6. MRI: ul ua Uy ...........ed ftI, ~ "'Ilh auoria ted inU'kl'\lni.J e bnllnnllolit;eli.. <men
ell,,'"
7.
not " I helpful .. CT
measlltementa, ! ucb aaocc:,pilO-fnlnUo I-ci",umCe",1lOI! mII)'.wlJ, be sbnol'mlleve n
In the fa«. of .. deformed I kuU . hape
locrep,aed l e p
Evidenot ofi~aaed Ie? in the n....·born with cranio.ynOlUllis includ<!:
1. radlographic'lpa (00 pl iin 'kull x·rll.y or CT. $H 4boue1
2 f.ilure of calva nal rrowth (unlika the non-. ynolll.ol,iclkuU wh ..... ;no;-relled lep
cause. roacror:rania in the newbom. he", It ;' the lyn08toail thatrouRd the in·
treued Ie? a nc tAllk orakull rrowlh \
3 Pfoplliedemi
-t o 1I..... lopment.al delay
NEUROSURGeRY
-to Oevelopment.al s nomahe.
.
T YPES OF C RANIOSYNOSTOSIS
SAGITT,u, SYNOSTOSIS
The mo.t common CSO affeeting a " nl/le luture; 80% male. Heaulu in dollchoce pb a ly or lICa phoce ph a ly (boat l haped I kull) with fron .... 1 bnuinll' prominent 0cciput, p'1p'bI. keel-lib IJIlgi Ual ridlla . OPC remains close 1.0 norma l, but the bip'rie\.al
diaroeter Ui markedly ..dUM.
Surgicall r ea tm e nt
Skin inei.ion rolY b. longi tudinal or tralllverM. A linu r "ltri p" craniectomy i. per·
formed. excisi ng the .agittal J uLure from the coronal to the l&IUbdoid l uture. preferably
within the fiMlt 3·6 montlu of li fe. 'l'he wid th of th e "rip should bea t l.attS em, no proOf
exi'l$ that interpo.i ng artificial aublltaneu (e.lI. silauic sheeting (IV' r the exposed edg..
of the p'rietal bone) retarda the recurrenceor .yno.~i •. Great care i. \.aken toavoid durallaceration with potenti al itijury to the underlying , upenor ••Kitt..l . in ..... The chi ld i.
follo,,·ed and reoperated if fusion ree "MI before 6 montlu lIe. After . I YT 'ge, more extensive crenial remode llinll i. ulually required .
CORONAL SYNOSTOSIS
Accounts for 189lt ofCSO, roore common in feroal ... In Crou U)n'. I yndrom e th;.
is accompanied by abnormalitie-$ of , phel\(lid, orbi\.aland facit l bona (llypopJu;' tlimid.
face ), and in Apert'•• yndrome i. accompanied by .yrw:iactyty-. Unil ateral coronal
eso
- pla gioceph81y with forehead on affeeted .ide nattened Or concave above ~e(narmal
side fa lsely appesMl to bulge abnormally), luprao(l.bital margin higher than norma l .ide
((III skull x-ray - h8rl equin eye l ilt'l). The orbit rotates out On the abnormal l ide, ond
can produce omblyopia. Wi thou t treatmeot, flattened cheeks develop and \.he no. devi_
ates to the normal side ( mot of nOM tend . to rotate t.oward s deformity).
Bilateral coroaal eso (usually io craniofacial d)'lmorphi l m with mul t iple lut ure
CSO, e.g. Apert's) - brachycephal y with broad , nattened forehe"d (acrocepbaly).
When combiooo wilh p~malUre d08L1A offrootosphenoidlland front.oethmoidal l utLlrel, resu lts in foreshortened anterior f0618 with maxillary hypoplatill , . hallow orbits,
progN$Si,-e proptosis.
Surgiealtreatment
Simple strip craniect.oml oflhe involved sutUA has been used, often with excellent
cosmetic """It. HoweYer, some argument that this may nol be adequlte hili been presented. Therefore, a moreculTf!nt recommendation is todofrontal <raniotorny (uni· Or bi·
lateral) with lateral canthal adva ncement by taJUog off orbital har.
METOPIC SYNOSTOSIS
At birth , the frontal bone consistaoftwo halvH sepa rated by the froo\.al or metopic
lu t" re. Abnormal dosure result.a in II pointed forehead .... ith a midline ridge (trigonocephaly). Many of these have" 19p chromosome abnonn.ality and are retarded.
LAMBOOIO SYNOSTOSIS
Epid e miol ogy
Lons con.ider«la clinical rarity wilh " reported incidence of 1·9'/lo ofCSO'". re<:ent
reportll IUllgest. hisher ineiderw::a of IO.~ wbich may be due to an actual increased
incidence, or . imply \.0 increased aWareness orchangi"ll diagnostic t riteria. More common in males (male,fema le. 4 ;1), and the riaht'ide" involved in 7~ofcasn. Usually
present.s between S· 18 monlhl of age, but .... y b. HIIIal early .. 1-2 mooths of .ge.
Controve,..y emu realtdiRJ the criteria for Ih;' Qlndit ion, and !tOme autMMI differeu u . te bet ween those C88n whid> appe.r to have a primary abnormality of the lambdoid
lUtu re from !hOM which rna, be due to .,..itional flattenin«, the ....called "lazy 18mbdoid". Othe.. do lIot make thi. distinction. and tometime. refer to the condition as occipital pl"gioctcphaly to avoid the need to implicete abnonnalilies of lhllambdoid l uture.
Po.i tional na ttening (0. molding) may be produoed by;
I . deereated mobility; patients wMconltanUy Ii. lupine with the head 1.0 Ihe lame
lide,
cemral pally, men\.al retarda tion. prematurity, chronic illn....
2. abnormal postures: ~~I, Qln,enital dillOrde .. Of l he c:ervi~a l
, pine
3. int.cntional poIitioni,.: trend , ince 1992 to place newborn, in a lupine sleeping
position to ~u<:e the rill. orsudden infant death Iyndrome (SIOS )", IOmelimes
e.,.
".
4. Developmental anomalies
NEUROSURGERY
4.
with II fwom wedge toG tilt Lhe child to ,,"" .id.. to red",,", Ihe risk offUlpirati"n
mtraul .. rine etillbglu": intrllutennllcrowding (e.g. {rom multiparous birth. or
ll1rge futalsizel. uterine !IJlomaJiell
Clinical fiudiDglI
Flattening of the oo:ipu~ May be unilateral or bil!lter~J . If llnilllteral, It Is !lOmetilll'" termed laro bdold ph.gi ocephflly which when severillailo produces bulgingoft.h
ij>l:lillll.eraJ fo~he"d rtIIIuh.ing;n II "rhomboid" .kll il with !.he ipSlli.to'rai .,u located anterior and inferior toG the contralateral ear. TheoontTalateral orbi~ and forehud may also
be flattened. Th;, may be confll$M with hemifatial mitrosomia or with plagiocephaly
""en in unilatolul oorona1 craniosYt\06toois. Bilate ra,llambdoid synostosi. produces
brllchycepha ly with bilth eur.disploced antt'riorly 8IId inferiorly"'. Unlike \he palpable
rid,gt of ugittal Or oonm91 Kyn""wsis. on W4~ may be palpated along Ole synos'
totic lll.mbdoid l ulure (although II peri,u tural ridge may ~ round in alllIle).
DLagnos tic evalu a ti o D
The phy8ieal exllm illile mOBl impDrtlln~aB~Lofdiagn09i~ . SkIlUx'·rIlY mAy help
diff~rlntiate (8<>. below). Ifth e IkuU x.ray ill equivocal. preven t the infant from layin;g on
the .ffetted $ide rOT nvua] wl'ekll. ~ bons &tan Bhould be oblained. ifno improvement
OCCUT'll (8« below). In definil.t ca5e$ ofsyn(lftt<>sis, and for SOme taSlU of refradory posi·
tioll.ai flattening \ ... hi~h usually (OlTt'cr. with time. bu t may l.ake up to 2 yea..,,! 5llrgi~ol
lr'~Htment /WIy ~ indicated .
Skull ,.·ray : ShOWIl 8 ""lerotic luarg;n along one edge orth .. la..rubdoid 8",t"'"' in 71)~ of
ealle&, Local "beaten copper cranium" (BCC) occuion8Uy may be 6e'en due \0 indenta·
u.;.nll in llIe bone from underlying gyri .... hich may be due to locally increased ICP. Bce
producell a characteristic mottled appearance oftbe bone with lucendea orurying depth
having ro",nd a nd poorly mllrginated ed8"l!! . BCC correlole:lwitb generalized, ICP only
when it ia seen wllh sellar erosioll and sutural diastasis.. ,
c r .can, Bone windo ws may show eroded or thllllled Inner table In the occipital region
in li)·2~ ofcollell"', > 95~ a", DO the side of the Involvement. The lIuture moy appear
closed . Brain w;lIdow" 5how parenchymal bnti.n abnormalilies in" 2%: hel.erotopiaa, hy·
droci!phalus. ag~nuiB oflhe corpus c.alIosum ; but _ 70~ will ha~.. significant ex pfUl~ion
oflh., frontal " ubarochnoid l pace (mllY beaeen in syno.slOllis of other sutllres.~u above).
Bon.. scan : loot.ope uptake in the IllJ'IIbdoid 8uture itu!relUlell d uring the Ii",t year, wilh
a peak IIt3 month" of ~ (follow;"1: the u.~u31 ioact;vi~y of the. fin;l w",kli uf life). TIuI
finding. with "YTI06tosil.Rre those typ;ta] for CSO (_ fJ'J#1~ 99).
1TeRtmeot
Ea rly sur gical t,.atment iI indicated 10 cases with 5evere.,:ranio!""cial d;sfill" rementor those WIth ~videllce ofi.ncreased ICP. Otherwise, cltildre,n may be matUlged nOn·
~u rgl~llUy for 3·6 month •. Tbe mll,jority of CalleS wiU .... maln stotie or will improve with
time aDd limpl e nonsurgical ;nte .... ~Dlio". App roximately 15')& will oontinue wdevelop 8
significo.nt C<i!lmlltic defonnity.
NDnaurgieaL mana.""mentM:
Although ;n.ptovemenl ean usua)!y be attained, some degree of permanent didig.
urement ii frequent.
Rl!pllllilioning ""ill be effective to - 85% orciI.5I!i. Patienu; are plaeed OR theunaff~t­
ed sideD. on the abdom~n. Infanta wi t h occipita l fi;<lttening from torticollis ehould haye
.ggr..... jv~ phy .i~" I1h e ... PT and rr ..lulion ~ou ld be ob._ed .. ithin!l-G mOlltM.
More severe invo]y ... ment nlDybe veated with 0 trial ofmoldingh ... I01e~(however,
no controlled study hOI proveD the effiCACy!.
Surgitlll tr'1!8tm ... nt
Req,ojred (n only_ 20% o f calleS. Tile ideal age for lurgery is between 6 and 1&
mOrlthB. The pIIlien t i~ positioned pr one on e well·""dded cerebellar lIe~drest (the faoo
should be lined and gtntly massaged ,,"ery _ 30 minutes by tbl PtleathuiologisL to prevooL pTllssu re injuries).
Surgi~ol Option. u nge trom .imp]e u nilateral cronieetorny orthe suture til. elll.bo",U!
recunnruction hy a cranlofoc;al teom.
Linear c:raru~ctomy extends from tha ugiu.alsuLure 1.0 t he asterion il ofuln ade.
quate for palients $ 12 weeks ofoge withouLleveredi:ilig\lreme"l. Great care;i takell to
avoid durll)latt!rltion ou r the astorion whim Is in th e region nfthe traru;verH !in,,~ .
The exdsed suture derocn$lratel an inli..'mlIl ridge. B~tter re&ulta ar&obtainoo with earlier su rgery. more rlKiie.l] surgary ma.y ha nl!CeBoary nful r the age orB month • .
Averag... blood loas for unt'OlllpliCAted ca&el is 100·200 ml and therefore tronsfusion
NEUROSURGERY
4.
Developm~Dtal
anomaliee
'"
>II
often ""fIuirnd.
M UL T/PLE SYNOSTOSES
Fu~ion of man)' Dr all cr8 ni81.IltuR~ - oEyu pb • •)' {to w..- stui.! wilh
ainusI!II8Dd lh.lJ.".. (lrbibl).1'hese patienUi haye ~1e'<8ted ICP.
u"d~e'oped
CRANIOFACW. DYSMORPHIC SYNDROMES
Over 00 ayndromell have been de!oCl"ibed, 1'obk 4-4, snows a few ~Iec!.ood Dlle!!.
A number of ~r8niD6ynmt03il syud roIllBS are due to mutation. in the FGFR (fibro·
bJ~8t growth faclor receptor) B"l!lIeII. FGFR gane .related cranio~yno~t.oIIis syndrom"'! in.
elude l ome duaic synrlrOmell (Apert. CroUlon, Pfei ffer .•. ) lit" well as severn! newer
enti t ies {Be3N>-Ste¥!MOn, Muenke, Jaclu!on·Wei!lS ayndromell}. All exhibit autoBOm31
do.uinlllll inheritance.
Tablu 4-4 Selecte-d cranlolaelltl dysmorphlc: syndrome. (modifiedf! '.'.....~
, ,
,
.,
abb,..,..,,!OnS: AO ., 1N1OSaTIaI~: FG/'~ ... bIobII~ grOWIi> 1at:lGf' r~
cso .. ~lOOIs: ~ ~ rlyl!f'OCOIl/UI"" ; UE "' ~PJ>OI a.<l(8mililt
4.5.3.
~ed :
Encepha locele
Crsnium hifidum 18' defect i.o the ru~ion of the c:ranin! bone, j~ OttW"'ll in the mid·
line, IUld ilmOll! (om man in th e occipital region . Ifmeuingelloo CSf' hern iate tllrough
the defect, it i$ called I mening~le. Umenmgt'sand cer ebMlI tissue protrude. it (seni le!!
an encephalllOllle.
E ncephalocele AKA c:e pbahx,ele ;s an extenS;(lfL ofintracran' alatrllClUNII DI.ltllide
of the normal coufiue! of the sltu ll. One C8/i1! wlU seen for eyery fi ve C/l\le.t ofspinal
r:oy...[omen'Iij!oceles". A Ilasal polypoid mru;s in .. ~bolm should be C(lnaidered an en·
e.!phaklcele until proven otherwise. See al&9 Differentio/ diag'lCfis. J>9ge 936
CLASSIFICATION
Systt!m baaed on Su .... n"'el. and Suwanwela1'O:
1. occipital: often involvu v8lleular structu res
2. c ranial vault: compri!!!!~ _ 80% of ene.!phalocelea in Western hemi sphe re
A. int.erfrontaJ
n. .nterior fontanelle
C. interparietal: often involves vasculllJ" ~Iruetures
D. tempo rn!
E. po5t.erior fontap!!.lle
3. fronto-etbmoidll J, AKA $lncipital ; IS'N of encepbalOCftles, exterolll opening inlo
face in one oftha following 3 region ••
A. na,ofrontal: ex t;!ma.l def~ i.n the nll",on
B. nQllO-ethmoidal: defect between lIasal bone lind nanl cartilage
C. naB<Hlrbillll , defect in the aote ro-inferior portion of madill I whital wall
4. oosal: J.5~ of encephlocele~; (8ft billow)
A. transethiDoidal: protrudes into lIasn! cUlit)' th rough d~ect in cribrifonn
plate
B. s pheno-ethmoida[! protrudes into posterio r na!lal C'1lvitr
C. tranloliphenoidal; protrudes into . pl!;,noid alnus or nuophJlrynJI through
patent cranioph.ryngeal tansl (foNlmen teewn)
o froD tI)-sphenoidal or .ph~n<Hl rbit81: protrode.. into orbit through superior
I02
4. Oevelopm!'t\tal a non,ali.,.
NEUROSURGERY
orbital fissure
5. po,terior fossa : WluBlly oontllins cerebellar tissue and ventricular component
BASAL ENCEPHALOCELE
i'heonly group thatdoes not produ~ a visiblesof\ tissue ma8.ll. May present as CSF
leak or recurrent meningitis. May be aS$OCiated with other erB niofadal deformities, in·
duding: den lip, bifid nose, optic-narve dysplasia, coloboma and micropllthalmia, bypothalamic·pituitary dysfunction.
In iencepbaly is cllaracterizW by defe<:ts around tile foramen magnum, rachiscllis is and retrocollis. Mo.st are stillborn , $Orne survi ve up to age 17.
ETIOLOGY
Two main theories:
1. arrested clo.sure of normal confi ning tissue sJlow, ll emiation tllrougll per.iatent
defeo:t
2. early outgrowth of neural tissue prevents normal c")!Iure of cranial covering!!
TREATM Etrr
Occipital e ncepbaloce le
Surgical excision of the 88e and its contents ""ith water-tight dur..! do.sure. It must
be kept in mind thst vascular structures are often included in tile sac. Hydrocephalus is
of\en presen t and may n<!f!d to be trea-ted l eparately .
Basa l encepbalocele
Caution: a- trsnsnasal approach to a basal encephalocele (even for biopsy alone) may
be fraugllt witll intracrani81llernorrllage, meningitis, or pe",istent CSF leak . Us ually a
combined intracranisl approach (", itll amputation of tile extratra nial maM) and !-ransnasal approach is used .
OUTCOME
Occipital ence pha locele
The prognosis is better in occipital meningocele tllan in encepllalocele, The prognosis is worae if a significant amount cerebrel tissue is present in the sac, if the ventricle!
extend into tile sac. or if tIlere is hydrocepllal us. Less tllan ~ 5%ofinfan~ with encephalooele develop normally.
4.6.
Chiari malformation
The term "Clliari
malformation" (after pa.
thologiBt, H.. ". ChiDn) i .
preferred for tYP<! I malformations, with the term
"Arnold·Clliari malforma·
tion" re\lerved for typ<! 2
malformatic>n .
The Cb.iari malfor·
mations consista offou r
type!t ofllindbrain abnor·
malities, probably Uilrelate<! to each other. The
majority of Chiari malformations are type5 1 or 2
(set" Tobie 4·5). a very lim_
ited number of cases com·
prise tile remaining types.
NEUROSURGERY
Table 4-5 Comparisons 01 Chlarllype 1 and 2 a nomalies
(,..
1~J.'''''''''
4. DeV1':lopmentalenomalies
'03
TypE. 1 CH1ARl MALFORMATION
t K..y fealllrejl:
• a het..rugeneou~ entity with th"l:Ummo" future of impaired CSF circulation
through the fe".men magnulu
a:rebeUar tunsillar w rniation: varieble, '" 5 rom below the f(>~men magnum is
common. but i9 "at .. _ ntial nor d'agnOiltic ofth" co"dition
t ....... tment, wh .. n ind icated , 19 ONrl(ical, bu~ aspeel8 or what tha t 8urgery IIhould
e ntail areCQntroversial (enlB r~men t offonunen I1l.IIgIlum is Ul!ually In"oJved)
• auociated with syrinsomyelia in 30-70% ",hieh almost 1I1",ay. improvell ",jth
treatment of th a Chiari malformation
AKA primarycen!bell~r ec t.Opia" , AKA odultChiari mnlfonnatlon (.ince-it tenda t.O
be diagno&ed in the 2nd o r 3ni d''''''lde ofHfe j. A heterogenooWl grou;) ofrondiclons, with
the u[\de.lyil\& eommoml]ily of disruption of normal CSF now throu!I"h the foramen mlllr·
nurn (FM) . Sam.. ~.a."" Are ronB"olnital. but othef"8 are oClQuired.
Clall.!!icII.llyd ... etibed a. a r8r .. . bnol"1l'l~lity restricted tu noudal dUiplacernent ofcerebeJlum with t.onsillar hemiation be low the foramen magnum (_ MRI belnw fur enl,,·
na )and "~g-liJu, elnngation "F ton,it.". UnH.lr.r.Chlari type 2. the mooulla i~ Il.IIl. caudaUy
di . plllUd (some lIu1ho., dillllgTe"'!)n thlS paillto/) , the brainltem is lI!)t invDlved. lower
crll.Oial n erves.re II"t elollpted. lind uppe~ ceroiClitI li e""'" d!) not (ouI"Hcephlila d, Sy·
ringamyeliD" of the apin al cord il pnl.ent in 3O -7Q'K.... Hydrotephah,s Oc:eu rs in 7·9%
(lI<tien15 with Chian type I mlllfllrmalion and syrinllomyelia".
Certbel1ar ton9il descent below FM with ;mpaelion. while common, ;5 110 longer /I
sine qua non Of dillgll DlJis.
Etlo l"lO" may be fl..Sl!oc:ill ted with
), II . mlll poslerior fOIlBR
A, underdevelQprnellt of lhe oa:i pi La I bQne
B. low lyinil tenwnum (the roof nf the p-fOUil)
C. thickened Or el'"vtlted occi pital bone (the floor ofll,e p-fos.u)
O. space oc:eupyiOS" I~i"n in p.fosJl!l: tlrftchnoid, cyst, tumor (~.I. F'M m""ingi_
om~ or cerebell a r a&trocytOm a ), hypervallcular durn
2. tllli been d e~cribed withjll8t "bout a nything tbat tak~ u p intrNtrllnia) . Jl"ce
A. cbronic 8ubduI"1I1 hemawmas
B, hydroceph81us
3 f"lI"winl IUlnboperitoneal shunt <_ POll" 189) or multiplll (:rllumatic) LPs" , acq uired Chia n I malfc nn atioll (u, ually BsYmptomatic )
" . a rachnoid web Or 8car o r lib,osu around bndnstem and tonal1s near FM
6 a bnormalities of the up per cervical Bpin~
A. hypermobility oftlte c'll(I iove-ru::b rHljUllctinn
B. Klippel-Feil.yndrome
C_ OQCipitauZlItion of the aU lis
0 , anterinr indent.tion lit f"Mlmen "'lignum: e.g. basilll ' invaIPllatiO(1 or ret.-roversion ofth. pd"nwid p n>Ce911
6, Ehlerl!-Danlos sYDdrome
1. eTIIJli~ynOSt08ia: espedally ctlSe81,,~ol~ing 111 1suwrea
8. r1!taiCled mmnhoid roof: "H1J
"r
EP,DEMIOLOGY
Ave, age agio: at prellenlatiM ie "1 yell"l I ..... oge: 12.1a yn). Slight female preponde ....
anctl (female:mllie a 1.3:l t Average duration of.ympt.ows clearly rell'ltcd 1(1 Chlan malformalin" is :t t)'l"$ Irange: t mMth_20 )ITs); if non~pec:i fic eompJair,t/i, e.g. lilA , a re
induded, this bec:nmes 7.3 ye/ml". Thi. lateCley is probably low~r i~ the MRI ef$..
CLINICAL
Par.ient.6 with Chia ri type t malfonnatic)Il /lUI}· present due tu;my o r aU " f the fol-
lowing:
I. oompreasion " f brain stem "I the level of the ftooraroen mllgnum
2, hydrocephalus
A. True hydnom.y. l", probabl,y a_n'l O<ruT. C8F n...... lut. _ _n docum..,ud in mon, ond lIlt ~ n·
.
""Ity ""tp"nibl. III find ....,.,un;........ bctw .... tl,~
, """
.,riA. ond
4. Oevel"pmental ano'nalin
1h~ ""nl .. I<.l1.O l lnChl.ri
I ""-
NEUROSURGERY
3
4.
5.
syri ngomyelia
isolation ofthl! intracra nial PT1!5SUN! eompartmen! from the spina l CODlpartment
causing transient elevations of intra crania 1
pressure
15-30% of patient.. with adultChiari mal.
formation lIre asymptomstit""
SYMPTOMS
The most common sym ptom is pain (69%), especially headache which is usuatiy felt in the suboxcipital regilm (ut' Tobie 4-6). HlA are often
brought on by neck e ~ t.ension Or valsalva maneuver. Weakne$$ is also prominent, espe<.:ialJy unilat-
Table 4-6 Presenting IXIIUllllIDl
In CIII, nl mallolmllllOn
.,
(7 1 cases")
ned! (wboceipilal. ctrvica~
~"
eral gt'lIsp. U'ermitt.e's sign may nlsoocC'U t . L<lwer
ext""mity involvement usua liy consists ofbilateral
spasticity.
SiGNS
See Ta.ble
;ng of signs":
".7.Three main patterns orc1ust.e r·
1.
fqrllmen mamwn...CSlluPrtSsjoD "xndrpme
(22%): ataxia, corticospinal lind sensory
deficits, cerebellar signs. lower cranial
nerve pals; .... 37% have severe HlA
2.
~~~ ( 65%): diftsocia!.ed
!lens!)!), 105$ (lOllS of pain & t..>,mperature
eentlltion with preserved touch &'JPS), 0<:caaionaleegmental weaknes9, a nd lOll!!
tract signs (.yrilljl:Olllye lic sYlldrome").
11% have lower cranial nerve pal.9ies
3. ~e(l!be!!ar 1Iv.ndt!wl£ (11%): trunCliI and
limb al.a.ll.ia, nystagmus, dysarthria
Downbeat lIystagmus is considered II
charact4l ristic of this coooitioll. 10% will have
a normal neurologic e~lIm wi l h occipital WA
as their only complaint. Som e patients may
pre.ent prillUlrily wi th spasticity,
lalnting
Iada! numbness
.,
Table 4-7 Preaentlng IilulI
In Cillarl l ma lformallon
NATURAL HISTORY
The natural history ia not known with
certainty (ollly 2 reports on "natunlJ history").
A patient may remain stable for years, witb intermitt.ent period s of deterioration. Rarely,
spontaneous improvement may OCcur Cdebat.-
od'.
E VALUATION
Plain x_rays
Of10 skull x-ra}'ll, only 36% were a bnormal (26% s howed basilar impression, 7%
platybasin, and 1 patient each with Paget's
and concave clivus): in 60 C·Bpine x-rnya, 35%
were abnormal (including assimilation of at.las, widened calla !. cervical fusions, agenesi s
of posterior arch of aUMl.
MRI
d.~ -..beal ~1agmuIl oo...-..c:al
_men~ and ftllalory nysIagm ... on horl·
zenlal movemenI: no o.:ludes osellop$ia""
Diagnostic ",st of choice. Ea.sily shows
many of the d al!9ic abnormalities described <1aflier. including tonsillar herniation, u
well as hydrosyringomyelia which oceUrli ill 20-30% of Ca8U. AJ !IO demo!'lStrates venITal
NEUROSURGERY
4. Developmental anomalies
"s
brain nem eompl'<!&!Iion when presen t.
Tonsillar berniation : Cri~ri B for the d~BCent of thl! tonRi llar t ip" belDW Lhe fommM
mal):num (FM) to dilltm06e Chillri ty~ I malform.1tioll ha"e co ne Lh rough II number of
reeon8ide rati~.
I.....'"
1:"
ClIiIIrI m.lronzaalicm IIQd
.
•
In itially." Ii DUll wIIs ddined 8lI dearly pathologic:"'lwith 3-6 mm heincbordt'rlina).
Bark.ovieh" found t.<>n$illar positions 88 Bho .... n inTabl~ 4·8. and Tabl~ 4 ·9 ehow. th e ef.
feet of utililing 2 Vt. 3 mm (Ii the lowe$t lIo rmal position .
Table 4-9 Cri lerla lor
Chlarll ~
Crileri.lor Iownt Sensitivity Speclllcity
e~t 01 tanslls at> lor Cll\lrli IorC\'ltlrl I
cepled II norlll!ll
21T)1'T1 below FM
t OO'l\o
~.5"
~ 0<1 ""' ..... 'emo~lS In 2(0 !III"I1a1s i<I<I 25
C/Ii/Id I pallenlilaken In "'11100 !D .,... Iow<It pan
O! tile torame~ 1IlOIlIOO'"
The lnnsih. normally u<:end .... ith age" u s hown in
Tabl~4· JO.
P.tUml.s with syrj ngohydl'Qnlyelia without hindbrain
h erniation that responded til p"fos~s decomprj>osion have
been deKribed~ (aGoC!l ll ed · Chi"rl zero Il1l1lrormatlon"l.
Conversely, 14% of patienl.s with tonsillllr hernilltion " Ii
mID al'flllsyrnplomati c'" fa verage utent of l!C\.OpiR in this
group .... as 11.4,. 4.86 mm).
POlentially moruigoificanl than the absolute t onail·
lar desce nt i~ Ihe aU1Ou,n.l. or<:oropreuion ot the brainSleJll
81 the PM, best appreciated en axial T2Wl MRllllough t.l1e
FM. Cnmplete.obliteration or CS I' Hignal llnd com pre56ion
oflhe brainSlem at th e I'M by impeeted tonsil, it e (ommQll .'gtU!icanl r,nding.
Cine. MRl : May oerooOSt rllte blodr.age orCS I' flo .... at PM .
....
Table 4-1D Tonaillar debelow FM related 10
s~nt
'
s.o. • _,d
"""'a\lon.
DIIsoonI:>2 S O. beyond
<lO'mO.1", ""9OI'S1N" 8 t&
I..... !of loelilJ. , e<:Io\liIl
Myelogr8p hy
Only6'Jb false nega tive. Muit 1'\111 dye all t ile way up
10 the foramen magnum .
CT
CT baS dimwl ty eVlllu a t ingthe fom men mQgIlum region dueto bony artrfad. When
combined .... ith intnllheca l ,..a\Jlr·IQluble contras t (myelogt'tl m). rehahility improveB.
Filldings: tonsiUard .... cellt ""d/or ve ntricular dilata t ion .
T REATM£NT
Ind iclil lions tor lIurgery
Since patientll respond best wilen opl!I'Hted on within 2 yea~ of the on.q el or~)'l1'Ipo­
tornli (!lee Operoliw f«U/IS bela....}. early a urgery ie reeonlmended for symptomatk pa·
tien (4. A!;ymptomatie pa t ,enlll may be followed and operat.ed UpOn iraod wll~ they
be<:ooIe s)'II'ptom alie. P8tieals .... ho hsVII be@nsymptoma tieandst.t.hle for y<!8fS mlll'bAoon!ide red for observation ... it.l18urg«ry indicated for aigna ofdeterioratlon.
Surgical techniq u ell
The mllSL frequently pe:rformed operation is poaterior fOSlln decomp",,,,,ion (su bocd pitlll er..rue<:tomyJ, with or without other proced ures (uluaUy combined w i~h duul
patch (l'aft inc aod ee rv icallaminect4my of Cl, soDletiml>fi to C2 or C3l.
Some lIuthoT& advocate performing 8 tra"'30ra1 c1ivus·odon\.Oid r esection in eaSl'S
wit b v@O lralbrain ·.temoompreBsioll.fiBtheyfeel thesepaLient . may pot.entia lly deleri .
orutewith p<lllterior rosaadocompr OlSSion alon ..... Since this deterioration wm$ I'Ilve,."ible
with odontoideetomy, it mny be rensonl1ble to perform t m. proeedure on patien ts who
show signs ofdeterioration Or progression of basilu impression on ~mil MRI. alter p<III.
'"
NEUROSURGERY
UlrOor fossa derompression .
OPERA TIVE FINDINGS
5ff Table 4·// . Tonsillar herniation
is present in all eases (by definition); the
most commo;>o position being atCt ( 6~) .
Fibrous adhes ions between dura, arachnoid s nd tonails with occlusion of forami _
na ofLUlIChka snd Magendie in 41%. The
toMils sepa rated easily in 40%.
Table 4-11
r
In Chlarl I
I I
below loramen magnum
"
"
SURGICAL COMPLICATIONS
CO
After suboccipital craniectomy plus
Cl·Slaminectomy in 71 patients, with
dursl patch grat\iog in 69, One death due
to s leep apnea oceurTed 36 hra post-op.
Respiratory depression was the most
COmmon post..,p eomplicetion (in 10 pa·
tients ), ..... u.al1y withi n 5 days. mostly at
night. Clou respiratory monitoring is
therefore rerommended". Other r isks of
the procedure indude: CSF leak. hern iation of eerebellar hemisphe res. vascular
illiuries (to PICA ... ).
unspeciIied level
~"
inverted foramen m8ll"1lm
keel rJ bone
Cl aret! alresia
.tIn"'....
vncular abnOrmal ..... P ICA d~ate<I '"
1
""",.,. in B1'0"••>1, ",ICA ollen deSOllnel' 1 0 _
margin or ""'$IIs"I: lor"" 11 ..... 1","""U, Iolta in 3
OPERATIVE RESULTS
See Table 4 ·12. PalLante with. pre·op
romplain ts of paio geoarally respond well (Q
s urge ry. Wea kness is less responsive 10 Sur·
gery, elIpecially .... hen musde atrophy;s
pre!lent". Sensation roay improve when th e
posterior columns are unaffected and the defieit is due to s pi notha la Ulic involvement
alone.
Rhoton f""ls that the main benefIt DrOperation is to alTest progression.
The moat favorable results OCCUlTed in
patients with ureb<>llar syodrome (87%
showing improvement. no la~ detf!rioration).
Factors that colTelate ""jIb a worse outcom e
are the presenc.e of atrophy, ataxia, scoliosis,
.",rJ ¥Y"'I'wrn» 1~¥t;nJj IOll ger th"n 2 ye~,..,," .
Table 4-12 Long-term follow-up aner
surg ery lor CIIlarl 1 malformation
(69 patients, 4 ~ea(S mean IQj!ow-uP")
lI1ese parionl6 dflhtriolah'<l Ie ptfI..QIl , l atus
(none dele.."..lod 10000hllr) witt*l2-3 yews or
S<lrgery: relapS<l <>CC:\I<f8d in 30% will> lor ...
11>10 magnum c<lmj)ressioo IO)Indrome.
_In
21 % ... In cenltal 00td IO)Indrotnfl
TYPE 2 (ARNOLO}-CHIARI MALFORMATION
Usually associated with myelomeningocele
CMM"!. Or rarely spina bifi ds occulta.
PATHOPHYSIOLOGY
Probably does ~ result from tethering of t he cord by the acrompanying MM . Pri_
mary dysgenesis of the brainst.em with multiple other developm e ntal anomalies is mOre
likely"".
Major findin gs
Caudally dislocated cervicornedullary j unction , poIll. 4th ....entricle and med ulla.
Cerebellar tonsils located at Or below the foramen magnum. Replacement of normal
cervicomedullary junction flexure with a "kink- like deformity".
NEUROSURGERY
4. Developmental anomalies
'"
Other possible associated findings:
1. !.>eaking of tectum
2. absence of the septum peJlucidum with enlarged interthalamic adhesion' absen~
of the septum pellucidum it thought to be due to necro.is with resorption secondary to hydrocephalus, and not a congenital absence'''''' ,,',
3. poorly myelinated <:e"lbella r folia
4 . hydrocephalu s: present in most
5. heterotopia.
6. hY'popIDS~a offal"
7.
mlCrogyrlO
8. degeneration of lower uanial nerve nudei
9.
bony abnormalities:
A. of ~rvicomedullary junction
8. assimilation of atlas
C. platybasia
O. basilar impression
E. Klippel-Feil deConoity: su page 119
10. hydromyelia
II . c.aniolacunia of the Iku ll (8ft ~Iow )
PRESENTATION
Findings an d~ to brain stem and lower cranial nel"\'e dysfunction . Onset is rare
in adulthood . The presentation ofneonataadiffs .. substantially from older childnn, and
neonates ,,'eO! mON! likely to develop rapid neurologi~al deterioration with profOWld
brain stem dysfunction over a period of several days than were older children in whom
symptoms were more insidious and rarely as severe".
Findings include>'·II:
I . swallowing difficulties (neu rogenic dysphagia) (69%)". Manifests as poor feeding.
cyan0!5is during feeding, nasal regurgitation, prolonged feeding time, or pooling
of oral secretions. Oag rene~ often decreased . More severe in neonat.e~
2. apneic spells (58%): due to impaired ventilatory drive. More common;n neonates
3. stridor (56%): more common in neonates. usually WOn;\! on inspiration (abductor
and occasionally adductor ,'O<:al cord paralysis seen on laryngoscopy) d ~ to 10th
nel"\'e pa res i.; usually transient. but may Progn'-SS to n'!!pi ratory arrest
4 . aspi ration (40'>\)
5. ann weakness (27%) that may progre~! to quadriparesi~"
6. opisthotonos (18%)
7. nystagmul: especially dl.lwnbeat nystagmus
8. weak or absent cry
9. facial weakness
DIAGNOSTIC EVALUATION
Skull films
May demonstrate cephalofscial disproportion from congenital HCP. Cl'II.n iolacu.
oi. (AKA liick.e nschiide l) ;n 85% (roWld defects in the skull with sharp bordel'$, &epaMlted by irregularly branching bands of bone). Low lying intemaloccipitol protuberance
(foreshortened poIItenor fossa ). "; nla rged foran,en magoun' in 7()<.{,; elongation of upper
cervical lamina".
CT and/or MRI find ings
("
,l<! .... with.n •• ",n.k ... t...at.pprf<'i.Led On MRI)
primary findings
A. ·Z· I.>eod deformity of medulla~
B. cerebellar peg
C. tectal fusion ("tectal beaking")
O. enlarged massa interml?dia (int.erthab.mic adhesion )·
E . elongatiolV'cavicall;zation of medulla
F. low attachment of tentorium
associated findings
A. hydrocephalus
n. syringomyelia in the area of the cervicomedullary junction (reported inci·
dence in pre MRI era" ranges from 48·88%)
C. trapped fourth wnlride
O. agenuisldysgeneais or corpus callosun,·
'"'
4. ee,·elopmenLalal'1Omo.lies
NEUROSURGERY
E. cerebe llomedullBI)' e<>mpr"''''on
Lary ll gOSCOpy
Performed in pa t i.nQ with lirido r to rule out croup or other upper ~"piratory tracl
i"fection.
TREATMENT
inw,t CSF . hunt for hydro«pholua (or check funct.ion 0( ex ialing ahunt )
if neurogenic dy.phagia, Htndor . or apneic apell. occur, upeditious poiI~rior r....
l a d«omp~ .. lon i. recommended (_ Nlo",) (r.quired in 18.7<;\0 of MM
pat ienll"); btfore recommending de«>mpression. alway. n,ake aurt tM pa~nt
h .. a functioninB .h untl
S u rgical d eco mp re.. io n
NB : it hPi been arllled that part of the explon-'lon for t he poor operative r..ulUl
in infants ia thot many of the ne urological fiedine' may be dut in part to intnnaie (u ncorrectable) abnorma litie. which l urgie. l decompreuion unroot improve"·", A diutnting view i. that the hi.tologic luion.s.1'1! du e to chronie bl'llin ltoem compreuion and
conoomitant isehemia, aosd that upeditiou. brain I tem deoompreuion .hould bt:carned
out when any of th e followingm t ical warning . ign. dev.lop: nlUr<l!rfnjc dy:apbagja . t ri·
~tiu.ndll".
Surgical t.ech nique:
Oeoompreuion of cerebellar ton l il., ulually with du",l rraft to dec<)mpreu dur • .
Patienll i. pla""d prone, wi th the neck nexf<!. A . uboccipital Cl'1Iniectomy ia tombin@<!
wit h a cervical laminectomy which must be cam@<! down to the bottom of the ton . lIlIr
ti ..... A thick COn$tncting d ura l baed is ulually found between the CI arch .nd ro",men
magnum . The duro is open@<! in a "Y" shaped Ind. ion . Caution when openi ng the dura
above t he level of the forllOlen magnum in infant. as they have I well developed Ottipiu l
sinus and may have lar!,'le dural Ink",". 00 NOT .!.tempt to dissect tonsils from underlying medulla. In c.ses with a . ignif..:.nt .yringomyelic cavity,.a .yrin&o. .... b.rachnoid
sh unt is pla"fd".
T ra cheostomy (usually temporary) i. ",oommftM!ed ifltrido r and .abductor laryn.
geal palsy were present pre-op. CI06e po$t..op respi ratory mon itoring i. nc@(\ed for obstruction W reduced vmtilatory drive fmech.niul ventilation i. indicated ror hypoxia
or hypercarbi.).
OUTCOME
68<;\0 h.d complete (Q' ne.r oomplete resolution of.ymptoms, 12<;\0 h.d mild to mod·
erate residual de6eilll, and 2091: had no improvement (in Bent'r.l, neona," far1!d WO!'lle
tb.n older ch ildrM )I'.
Rupiratol)' arr«1 is the most oomroon uuse ofroorlality (8 or 17 patienll who
died ), with the rell due to meningitisfvent riculitia (6 patients), .. spiration (2 patientl),
.nd bi liary "l'8i. ( L padent)"".
In follow · up ranging 7 m....6".., 37.8'\lo mort.lity in ~rated patienl!l.
PreoOp It.a tUl and the rapidity of rotu.rologic deterioration ~re the Il>0l>1 important
progoostica"" .... l'oIort.al"y ri te it 71'110 in in fants h."in, cardiopulmonary arrest, vocal
cord panly." or ann wnluwas within 2 W(M!U of presentation; compared to 23<;\0 mor·
ulity in pIItienlll with . more rradu.1 deterioflltion . Bil.teral vocal eortl paralysis was a
particularly poor pr(lfrnOSticator for ,"poNe to . urgeryf'.
OTHER C H1 ARJ MALFORMATIONS
CHIAR/ TYPE 3
Ran. The mot! ICIvere IOrm. Dilpl&Cement of poIterio r r...u strudUreII, with cerebellum hemiated through fo"men magnum into oervic.1 canal, often with a high ce ....·;·
c.l Of' lubottipiul ene.epha lomeningocell. Ulually inoompatiblt with li fe.
CHIAR/ TYPe 4
Cerebell a, hypopluia without cerebellar herniat ion .
NEUROSURGERY
... Developmental a roomal ,es
,.,
4.7.
Dandy-Walker malformation
At.",;a offo' 8111'n. of Magtndie and Lu.c:h k,". Thl, l"uulU in &&frlesi, of tile ~r­
I I I~ posurior roan cyatcommunicating with lin enla rged 4th ventricle (.orne retrotl'l'i'beUar .nchnoid cyaU mi mic Oandy. Walker, but theAl! do not heve
vennia" agene.is and the c)'IIt does I1l!& open into the 4th ventricle)
lObelia. venn's with
Hyd.""",phaJuaQ«un in 9O'Jl, ofcl.U$, and Dandy- Walker malformui(ln is present
of.n caHI 01 hyd.rocepha!IlI,
Associated ab normalit ie.
in
2-4 ~
eNS .bDOnJUllitia include .gents;, oft'" o;(Irp'" caIto-u rn in 17,.... a nd occipital
encephaloc.le in 7<JIo., Olhu lindi"p indude heterotopi.., apina bifid" syringomyelia,
microoephaly, den::ooid cyau. poreneephaly. and Klippel-Feil def<lnnity. MOlt have an enI. Tled post.erior rou. ",lUI elevation of the torcul. r herophili.
Syattm>e .bnonn.li~ include"": r.d.1 abnormalitiu (e., . angiOD1I1, cleft. palatft,
roacroslOHi •• r.cial dyl!morphiaJ. 01:\11 • • IIbnon:aaUuu (• ., _coloboma. retinal dysgen e-
.il. microphthalmi.), and cardiovascular l oomlliea (e.l . septal defect.l. patent ductus Ir·
teTiot .... lorti, f;OITClItion. clextroo;ardia). Note: be .w.~ of the lihlihood of I ean:ii3C:
abnormality when considerinllurgery on theae patient.l.
Treatment
In t he IbMn.. of hydrooephalUl. thue .... y be follow«l. Whell t~atlllent is ~8'
lary.ihunt the pwterior f.... cyst-. In the rare patien t wi th aqued..el.llatena5;'. shunt
the lateral ventri<:lea all(l. Sh untinl the venlric ln alone ;. c:ontraindiclted because of the
ri,1t ofupwlU'd herniation.
Prol11ol i,
7~ 1 00'lIt tha"ce of l urvival . Only 00'l0 have nonnal lQ. Ataxia, spastic:i ty. and poor
fine motor c:on t rol arl common. SeiIU,"" ooeut in I~.
4.8.
Aqueductal stenosis
Aqueducl.ll s tellO'llS (AqS) produces what;$ tometimn ",lied t rivenlri<,:ul ar hy_
droce phal .... charatteri~ by a normal .i~ 4th ventricle Ind erJerged third.nd lateral ventritLl'A on MR I or CT. Most ""." occur in ch.ild~lI, however some p~aent ror the
first time in adulthood.
ETIOLOGIES
a congenital ma lformation, ""y be nlOcial.ed with Chiari .... Iformlluon or neu·
rofibromatosis
2. acqui red
A. due t.o inflal"JUl)9tion (foll owing hemorrhage 01' in fedion, e .g. I yphil .., T.B.)
B. neoplasm: esp~i.Hy brainstem utroeyt.omu{ineluding I«ta l gllom... ~
(XJgf 422), lipom ..
C. quad rige min al pl ate a rachnoid C)'Ita
I.
IN INFANCY
AqS i. 8 freq uen tea UH of congenital hydrocephllus (HCP ) (up to 70!l0 ofca.es"'J.
but OC<:8BiooaHy may be t he WIi.Il of HCP. Patient.l with co.nital AqS ulually hive
HCP at birth or develop it wi thin - 2-3 m~. CongenitalAqS may be due to an X·Hnked
recellSive gene"'. Fo ... r t~ of ron genita l AqSdetcribed by Ruaaell (.um ... l riud'O);
1. forking: mul tiple channel. (o!\en n, rrowed) with norroal epi:.he UlllInina that do
not ",eet. leparal.ed by normal nervous tissue . Usually uaod"led with other oon·
genita l "bnonnaHtie.; (spin, biMo. royelomenlngo«le)
2. periaq ...educ:tlll gliosis: lumina l narrowing due t.o lubependymala.tn>ty!ie prolir.
eration
3. t rue ltenO'l i. : aqueduct hiltologically nonn.l
4. u pturn
'"
4. Developmental aQoroBliea
NEUROSURGERY
IN ADUI. THOOO
AqS may be on overlooked eaU5e of "normal preAure hydr<l"ephalus" in !.headultfl.
It it u[Jk,n(lwn why .arne CMea of AQS would remain oooult, a nd mA,;ife/i ~ only in adullhood. In one seritl of:;:; case"', 35% b ad duration ofsymptoma < 1 yea r , 471t> for 1-5
yun: lbe longe.8~ W>i!;' '' 0 yrs. Although moat folio ..... !.hi! longstanding benign cou ~
there Ol'll rt!poru of "Ievue<! Ie? and . udden death .
Symptom!!
See Table 4·13 . Headachf 1'181 the QlOllI
Cllmmon symptom. lind ~ ad charae .... rialiC4 of
HlA 1I000000;au,d with e!e~ated ICP. Viauru
~h.ngu were next , lind liBuaJiy etlM'.lfod of
blurring or 1051 of acuity End""rine cb lngu
induded menstruol irre(Ularities, hypOthyroidism, aod h irsuti6m ,
Signs
Papllledema was the most COmmOn lind·
ini: (53%). Vi~ual fLel,u were normal in 78~,
lM remainder having l'1:!duced puiphe ral vi,
.ion, increased blind spota, quadranlic or
hemianopic f'eld euta, or OU:Oto1ll8ta. lnwlle<:-lual impairment waa pruent in " I Ita6136'11o.
Ol.her signs included; alma 129%), "pyramidal ttoct signi" in 44':; (m"l ld hem;. or paraparesilll2'2%), 6pntkjly (22"1. or BabUl$ki's
(20%»), an(l3n';a (9W».
E VALUATION
MRI ill lhe t1!~lof cholee. MRI will ~how
~be absto.oce of Iha nonnal now ,."id ill the
Sylvinn aqueduct. Con l rn l s hou ld b8given Lo
n, l~ut tumor,
T REATMENT (OF NON-TUMORAl. AOS)
Although treatmeo~ of the prifllllt)' leaion h."" been atu.Olpted (e,g , Jysi~ or"que·
dllct.al ""plum), thi~ haa fall"" intndi. ravor with ~be improved """ QlC)' "fCSF ahunting.
CSF i3 uRuaity ahllnled Lo the peritonellQl or the va!clll~r ~Yfit~m, however ahlintjng to
auhaT8chooid ~pa~ Ie al~o f"'iL'l,bl~ (once. OMlroction at the levi. ofth a rad!llQld grtInu·
latione iuLIJ ~n ruled out). A 'I'orkiltU~n 6hunt nloy work in adult eas£Sil, however pe.
diatric patienlll wit h oba~ruet've hydrocephalus may not ha"11 >UI /ldlHlua~ly developed
auhsraehnoid ~pace for I..,;. to funcllon properly,
FoUow.u p o(ot iea..ll ...." y ... ars to rule-out tumor ... recQmllli!ndM.
4.9.
Neural tube defects
CLASSIFICATI ON
Various elassification IY6umS elDSt, thi' OIIe;. j\dj\pled from Lemire".
1. neurulation d@fl'<ta:non-clO$ureoftheneural tube n!B ulU! in Opf'n lesions
A. CT8niomchi~hiai<l! Lotal dynaph;6Ql . Many die aij ,pon taneoul abo rtiun
R. an en e e pbaly; AKA e~enCO!phj\ly. DUO! to failure 0~f"8ion of th e anterior
neuropore. NeltberCTaniuJ vj\"lt oor ~alp eoverll Ihe partially de6lroyed
brain . Uniformly fata l. Ri,k ofrel'urn!nce in fu t ure pregnancies: 3'ifo
C. ,neningoI\l)'i!loeele: mOfl;I Cl.Imrnon in lumbar n!gior,
1. my! lomeningoceie (MM) : _ page 115
2. myelocele
'iL postneurulat ion defel'u, produces . kin-covl!red (AKA cl~ ) k$iDn~ (some m.. y
al80 be ooru;idered "m igralion "bnonnllJitie. "•• u MIO<A»
A, crani.. l
NEUROSURGERY
4 . Developmental Bnomat. ..il
'"
microcephaly: U~ below
bydrimence phaJy: loss of significllllt portion of cerebral hemi·
spheres which a re replaced by CSF. M u~t be diff.... entiated from maximal hydrocepha lus (Sft po.ge 180)
3. holoprosencephaly: Set bdow
4. l iue ncephaly: ""'f be/t)w
5 porencephaly: _ bdow to distinguisb Nom sch iuncephaly
6. agenesis ofl:Orpus callosum:.n b<!low
7. cerebellar hypoplasiafOandy-Walker synd rome: Set Patlt 110
8. macroencephaly AKA megalencephaly: U t b<!loUJ
B. spinal
1. diastematomyelia, diplomyelia: seeSplit cord mal{ormalu:m, page 122
2. hydromy~lialsyringomyelia:
Patlt 319
1.
2.
'u
Migration abnorm a lities
A I lightly different clauification scheme defines the following u abnormal ities of
neuronal migration (!fOme are considered posl neurulation defect • . .."" "bow ):
1. l; _nce phaly: The most severe neuronal migration abnor mality. Maldevelopment of cerebral convolu t ions (probably an arrest of cortical development at an
early fetal age). Infants are severely retarded and usually don't survive:> 2)'T11
A. agyri a : completely smooth s urface
B. pac h ygyria: few broad &0 flat gyri with shallnw l ulci
C. polymicrogyTh. , small gyri with shallow sulci. May be difficult to diagnose
by CT/MRI , and may be confused with pachygyria
2. b et eroto pi a: abno rmal fod of gray matter which may be located anywhere from
the auboortical white matter to the aubependymallining of the ventricles
3. ""hh.en ce pb .. ly:
A. den that com municates with the ventricle (as lTU'Iy be<lemonstrated on CT
cistemogt"llm)
B. lined with cortical grey matte r. Thi.s i9 the key to <lifferentiate from p o ren _
cepbaly, 0 cyst ic lesion lined with ~onnect.ive Or glial ti ssue that may cOmmunicate with the ventricular syste m. often caused bJ' vllJICular infarcts or
foUowing ;utracerebral hemorrhage or penetrating trauma (induding repeated. ventricular pWlclures)
C. pia and arachnoid fuse
D. t,,",oforms: open lipped (large clen to velltride) and close lipped (wallo fused)
HOlOPROSENCEPHALY
AKA arhin en ce pbnly . Failure orthe telencephalic vesicle to cleave into two cerebral hemispheres. The degree of cleavage failure rDuges from the severe alohar (aingle
ventricle, no ;nterhemisphe,;c fISsura) to semilobar and loba r (less severe malformation s). The olfactory bulbs are usually small and the cingulate gyrus remains fused. Median faciOCilrebra! dysplasia is common, lind the<legree of severity parallels the extent of
the deavage failure (see TobIt 1 · 11). Trisomy is often the cause oftb,s malformatioll, although normal karyotype_ ate tommon. Survival beyond infa ncy is uncommon, moat s u.v;vo", are , eve rely retarded. a minority are able to functioll in society. Shunt dependent
hydrocephalus develope in 80me of thea" children. The risk ofholoprouncephaly ie increase<! in subsequent pregnancies of the 8ame couple.
TaDIe 4-14 Tile lI ve I&Cle9 01 severe
"
'"
4. Developmental anomalies
NEUROSURGERY
MICROCEPHALY
Definition: head circumference mare than 2 standard devia,jol\ll belnw the mean fnr
sex and geSl.8tional age. Terms thalare sometimes used synonymously: mionx:rania, mi_
crocephalus, NCIt a Bi ngle entity, many afthe «mditions in TabU: 4-14 may be a!lSO<iated
with microcephaly, It ml.Y al80 result from mal<!rnal cocaine abuse"', It is important to
differential<! micro<:ephaly from a small skull resulting from craniOllynOlltosis in which
s urgicsl treatment IDay prnvide opportunity for improved cerebral develnpment,
MACROENCEPHAL Y'" ,.. ,DO,
AKA macrencephsly, AKA megalencephaly (not to be confused with mru:rouphaly,
which ;8 enla rgement of l he s kull (",e page 919)), Not a tingle pathologic entity, ~ enlarged brain wltich may be due to: hypertrophy of gray matteralone, gray and white mat.ter, presence of additional structu res (glial overgrowth, diffuse gliomu, heterotopias,
metabolic storage diseases, .. ). May be soon in neurocutaneous ~yndromes (especially
neurofibromatosi s).
Brains may weigh upto 1600-2650 grams.IQ may be nnrmal, but developmental de·
lay, retardation, spasticity and hypotonia may oc<: ur. Head circumference is 4- 7 em above
mean. T he usual sigTI8 of hydrocephalus (frontal bossing, bulgi ng fontanelle, "setting
sun" sign, scalp vein engorgement) are absent. I maging studies (CT or MRI) show normal
ailed ventricles and can be used to rule out extra·a~ial nuid colle<:tiont.
R ISK FACTORS
I . early administration of prenatal vitamil1ll (especially OA mg offolic acid daily'"
") may ~~ the incidence ofneurnl tube defe<:kI (NTDs) (confirm that vitamin
B" level~ are normal, see ptlgf 9{/4 )
malernal heat e~;lOsure in tbe fonn ofbQt.tubs, saunat or fever(but not ele~tri<:
blankets) in the f,,,t t n mesler was aijsociated with an increased n sk ofNTDs"
3, use ofvalproic ac;d \ Depakene®)during pregnanty iss»ociated with a 1_2% risk
ofNTO'"
4 . obesi ty (before and dunng pregnancy) increaee!l the nsk ofNTO.... "
5. m~l.erna! cocaine abuse may inCTease the nsk of mi~roo:ephaly, disol'de" ofneu·
rona! migration, neuronal diITerentiation and myelination'"
2.
P RENATAL DETECTtON OF NEURAL TUBE DEFECTS
.5:«!.!.m a\pha-fetoprotein IAFP)
(See Alpha .{rloprolrin On page 5-01 for background ). A higb maternal serum AFP
(.. 2 multiples of the median for t he appropriate week of gestation) between 15-20 woou
gestation cames a relative risk of224 for neural tube defe<:ta, and an abnormal value
(high or low ) was associated with 34%ofall major congenita i detects" . The sensitivity of
maternalseruIJI AFP for spina bifida was 91%{10 of II C8Se$), it was 100% for 9 cases of
anencephaly. However, other senes show a lower sensitivity. Closed lumbDlj.8o ral spi""
defe<:ts , accounting for ~ 20% ohpina bifida patients" , will prooobly be miQed by serum
AFP &ereening, and may also be I'\li$se-d on ultrasound . Since en. l.ernal serum AFP riee!l
during nonnal pregnancy, an overest;male of gestational age may cause an elevated AFP
in1Prpreu..:!~ . norm" t, .. nd JOn ,,"""r"8ti"'~te """Y """ ..... norm911evel to be inu-r_
preted 8S elevated..,
to""
U1tr aSOUDd
Prenatal ultrasound will detect 90-95% of casea of spina bifida, and thus in cases of
elevated AFP, itcan help differential<! NTOs from non·neurologic oauses of elevated AFP
(e.g. omphaloce le), and can help to mOre accural<!ly estimate gestational age.
Amnioce n tesis
For pregnancies subsequent to a MM, if prenatal ultrasound does not show spinal
dysraphism, then amniocentesis is recommended (even ifabort,on i. not oonsidered, it
may allow for optima l post-partum Care ifMM is diagnosed). A.m.D.i.21k nuid AFP levels
are elevated with open neural tube defe<:ts, with a peak betwoon weekll13·15 ofpregnancy. Amniocentesis also carries a ~ 6% nsk offetal Iou in this population.
NEUROSURGERY
4. Developmental anomalies
4.9.1.
Agenesis of the corpus callosum
A failute of commiuu l'1Ilion oceurrin, ~ :2 weeu .ftu con<>eption. The COflI .... tllllo.
I ll"" (CC) rorm. from l'Ol tn.un (gen u) to I pltnl um" . thu. in m08l caaea there mil)' be on
anterior JlO rtion (genu) with noapienium (the conyerte «ell ... Lelia frequently). IW~ult.s in
txp&Glion of th, thkd ventricLe and te p. ration orlh,late".1 ventricle. (w hich deve lop
dilated occipi tal !lorna li nd atria, and concave mediol bordeTll).
me ide nee
I in 2,()()()"'3,OOO ne\ul.rndioIO(ical exami nations.
As&oe ia ted neuropa tho logic fi ndin g."
pore_ph_I),
microgyria
interhemi.phe.ric 1iJl2mu and li poma. or lbe COrpUI callosu m (Ht page 96)
art.ineo",*phaly
optic atrophy
~obom..
hypopl ••if, oftha limbic ' ,Item
bundl" ofProbtt: aborted btcion inp of corpu. .,.Ikwum, b'Jlge into late",1 ven_
lrid.
10.. ofhorizonta] orien lation of d ngu late gyro,
t<:hiz.en«ph aly (He pap 112)
anterior and hlppocM)pal comm iuwu may be totally Or partiaUy a'oosent't
hydroceph"lul
o;y&t& in the recioll of the COrpUi a ll osurn
I pin" hilidA witb or without rn~omeningocele
"bsenee oftne septu ... peUUCiOUOl: ' " ptJgf 122
Po... ible p r esen t a t io n
hydroceph.lul
microceph"ly
aei lu~1
(rare)
precocioUl pube rty
disconnKtion syndrome: 100"" likely with ~ CC defect th.., in congeniUlI
May be an in<:idental linding. and by itse lflllay have no clinical $igniflCar>ee. How_
ever, m.y be occu r al part ofa more ... mplex clinical ayndroD\f! Or chromoeomal abnor·
mality (e.g. Aicaro i syndroroe: .nesis ofCC, seilures. retard ation , pst.<:hes of retinal
pigmenUltion).
4.9.2.
Spinal dysraphism (spi na bifida)
DEFINITIONS"
s;ma bffida oa:uIla CongerWII l absence 011 5jli'Ioos process and Yllri1b1e IIlIOOIlIsd Ie...... No ...iiii
~e oIl'I'IItWIges 0InN". b5$Ut ($NO b*ool.
The following two entiti es are IITOuped togethfor und er the term spilla bit'id a .pe....
III (aperla from the Latin fo~ "open") Or apilla bind. cYltic • .
menf~te
CorIgerWIIk!ed: in vertebrlllrtflH WIll epIle dISIe/I5IOn 01 mriIgH, Iii no .t>nQHr\ll~1y 01 ~Ml"'IisIue . C/rIe t.iftl1la'III _
rIIIIIOIogoc deId.
myelomeni'lgocelt ~I 6e1ecl in v&!Iebr&Iardles wilt! eys!ic diltUlliorl of mri'oge$ and IlTul;luIil
01 f\n;IiOrIallbnormal'fy 01 spiIIl eord 01 caUIIIlQUN [see~.
SPINA BIFIDA OCCULTA
OcCUI"l in ~ 20·SO'h of North Amt rk l.nl. Often.n inciden tal finding. u ..... lly ofllO
clinical im por\llnce wh en it o«un alona. However. it II)II YOCClllion.lly beassoci.ated with
diutematornyeli a, \.ethe...o cord. ]i porno, or de rmoid tumor.
Wh eo IYlllplomatit from one of the IlUOc:lll\ed c:onditionl, the ~senl.&tioo i" tha t or
'"
4.
~veloproenUl I
anomalies
NEUROSURGERY
tettlered tord (gai t dinurbance, leg weakness and atroptly, urinary diaturba nce, foot d~
(oralities ... , see Tf/heret! t»rd .yndromf, page 120). The derl!(:t trUly be palJ.>llble. a nd
there may be ove rlyiog C'J lsmloua mani festation. (.ee culo:rnrour " igrruolo: 0( dylnlphi,m
in Tablt 4· 17, ""ge 121).
M YELOMENINGOCELE
EPIDEMIOLOOY/OENETICS
In cidence of.pina bifida with meningo«le or myelomeningocele (MM) 1.1 1-211000
live birtlll (O.I .O.21to). Rislr inc rea_ to 2-31to ifttler. i. one previou. birttl with MM .•nd
6-81to after t ..·o "fTec\ed ctilldren. The nlk i•• Iso IncruHd in f. milies where cloH relllUvel (e.g.• iblinp) hav, given birth to MM clUldren, esp.<:i.Uy ...·hen on the mother'•• ide
arthe family. Incidence may increllK in ti nle' of wa r . famine o. economic diu.atera. but
it may be gradually ded ining overallt;l. 1'ran.million fo llowt nan·Mendelian geneticl.
and i. probably multiractona!'
Hydroce pbalus in myelom eningocele
Hydrocephalu. (H C P ) develo p' in 65-86~ of J.>lltlen u with MM , and 6· I()<I, of MM
patienU have ciinicelly overt HCP at birth" . Over ~ofMM patientl whowill develop
HCPdo sa before age 6 mos. Mo.t MM patientl will have a n a"""jeted Chian type 2 mal _
formation (~Type 2 (ArnoId)·C h iari maiforJ'J'l(JliM, J.>Ilge 107). Cloaur.ofthl MM defect
may conve rt a lat.o.>nt HCP to ""tive HCP by eliminating a route oftgn!U oICSF.
PRENATAL OIAGNOSIS
See P...
dflKliOll o{nfurallu~ dtft!CU on fIOIge 113.
"",al
MANAGEMENT
AOMISSION
1. assessment and managemen t of lesion:
A. mt!lsure she of defect
B. aseeN whet her lesion is ruptured Or unruptured
I. ruptured: . tart antibioties (e.g. n.reillin and gentamicin; DIe 6 hre afur MM closure. or continue if Jhunt anticipated in next 5 or 6 days)
2. unruptured : no antibioties neeesslU"y
C. «wer lesion with toolfa. then ,ponges soaked in lactated ringers o. normal
taline (fono a atenle &:I ute n ng around the lesion if it i. cystic: and protruding) to prll'o'ent desiceation
O. Trendelenburg position. patient on .tomach (keeps pressure off lesion)
E. perform su.-gieal closure within 36 hre unless there i. a contraindi<:ation to
, urger)' (.io> ultanlOus . hunt if overt hydl"ll«phalul (HCP) at birth): see
1'I'm i"4 of MM dNU,.. below
2. neurological . . . ssmenl and manaK"mlnt:
A. it.o.>ml related to . pinal lesion
I . watch for l pontaneoUS roovemelltofU>e LEs(good spontaneous melVe-ment correlates with better later functional outeam"')
2 . alMss Iownt level ofneurologic function (_ TCJblf 4·1$ ) byd'e<:Iti"8
.... poole of LE. to paioful ltimulUl: .Ithough some infantl will have
• cle... demlJ"Cl.tion between nor mal and abnorma l level" at leut
l how.am. mixture of normal.
aod a utonoroou. acuvity
(...uing from uninhibited anwrior hom motor neurona)"
a. dirrel'flnlil t ing ren.. movement from voluntary mly be difficult.
In general, voluntary movement i. not . tere-otyped with repetit ive tti muh.. and ran.. moven>ent usua.Uyonly pe.. iatla.long
.. the noxioUi lti mulua ia applied
B. itema related to t h. commonly lllOdal&'<l Chiari type 2 cnalform ation:
I. meaaure OFC: risk o(developing hydroc:eph.lul (_a bood. U.. OFC
griP'" (_ P'J#' J84), . nd alao look fo r abnormal rate of growth (e.g.
> 1 cr.Vday)
2. head UJS within ~ 24 hn
so..
NEUROSURGERY
ren...
4. Developmental anomalies
us
3,
3. check for .nspiratory stridor, apneic episodell
ancillary alI_ment and management'
A. evaluation by neonatologist to aue&S for other abnonualitiu. eapeciaJly
thOM' that may prech.de l urgery (e .•. pulmol;lary immaturity). The~ i. an
average incidence of2-2.5 additionalanomalin in MM patienr..
B. bladder. start pat,enton regular urinaryutheteriutiona. obt.in urological
ronsultation (non-emergent)
C. AP & lit s pine film" asses. KOI 'OOIi. (base liM )
D. orthOped IC tonUllalion for !leVI "" k,yphotie Or trollotic I plnl deformlti..
and for hip Or knee derormitiu
Tabll " 1S
SURGICAL CONSIOER ATIONS
TIMING OF MM ClOSURE
Ear ly dosu re of MM dered is.D.l!l. .... odated with improvement of neurologic fWlc,
tion. but evidence luPPOrti lower in.feetion rate with early closu~. MM I hould be dosed
within 24 hns whether or not membrane is iotact (afU:or _ 36 hrs the back le$ion is coloniud and there;, increased risk of postoperative inf~ion).
S imultaneou s r.W r e pair a nd VP s hunting
In patients witbout hyrlroce phalus . most su rg..,ns wait.t least _ 3 days after MM
repai r before shunting . In MM patients with clinically overt HC P at birth (ventriculomegaly with enlarged OPC andlor symptoms), MM repai r and shunting ml Y be performed
in the &ame sitting without increased incidence or inreelion. and with shortu
hospitaliz.atiorr" ·... It may also reduce the risk ofMM repair breakdown previoualy IIftn
during the interval before shunting. Pa t ien t is pOl it ioned prone, head turned tori&hl Cto
expose the right occiput), right knee and thigh ne~ed to e~Jl"OM right n~nk (consider u..
ing left. nank to prevent confusion with pppendeetomy..:a r l. ter in lif~).
POST-QP MANAGEMENT OF
MM REPAIR
1. keep patient orr aJl illciaions
2. bladder c.atheteriution ~gimen
3. da ily OFC measurements
4. ifnotihunted
A. regular head UJS (twice weekly to weekly)
B. keep pltient nat to I CSF p~u~ on inci. ion
LATE PROBLEMS
Include:
1. hydrocephalus! may mimie - anything li. ted
'"
4.
De~lopmentaJ
.noml li ..
~low .
Al.Yl.6XSlW.LEJlJJ.I..
NeUROSURGERY
SHUNT MALfUNCT ION when. MM patien~ de~rioratn
Iyri ngomyelia (a nd/or Iyringobulbil): lin JH16~ 349
tethered cord (8M rtlhtr~d corcl.,.lIdrome, plge 120): ~ all pfltient.f with MM d o.
lUres hive. tethered cord radiographically. hut only I mlnori~y arelymptom.t.lc.
Unfo rtunl~ly the~ i, no good telt to eheck for Iymptoml tie retetheriog(SSEI'.
may deterioratel""
A. acoli08i. : early un~therini of cord m.y imp rove .eoli08is <_ScolU:illi4 ill
u!lh~rfd <:rI,d, pfI~ 120)
B. .ymptomalie tetherin, [, of\en manifNted 8$ neurological deterioration of
delayed OrlMt-t. medullary compreuioo It foramen m.gnum (lymptonl!.tic Chi.ri 11 m.lforma .
tion , 1ft page lG-71
2.
3.
OUTCOME
WitboUlllllY t~atmen~, only 14-3K of MM inf.. ntl IUrvi~ infancy: these usually
repretent thel...t Mve~ly involved; 70'10 will h,ve nonn.IIQ' •. 5O'lt are .mbulatory.
With ItIOdem tre.tment, of MM ;nfanu .u rvive. The most common caUile of
e.rly mortality are complication. frOIO the Chi.ri m.Jfonnati<::n (re.piratory arrest, as·
piration ... ), where late mortality is Ulu,Uy due to . hu nt m.lfWlCtion. 80% will have no ..
cnallQ. Meotal retardllion ;. mOltdoeely linked to .hunt in fection. 4(1..85% ar<l
ambul.tory with bracin" hoWfl~r , mou ch_ to UlK! wheekhaira for ease . 3-10-.. have
normal urinary cont~. but molt mtly be able to remain dry with intermi ttent cath.
eterization.
as...
LIPOMYElOSCHISIS
Carol.pm.1d yora phiam with lipoma. Six fonnsa re described", th~ fol1owing3a~
clinkaJly important .. poseible e.... ses of progressive neumlogj.c dysfunction via tether.
ing (_ Td~nd arrJ .,.ndro",." pa~ 120) ancllor comp ression:
1. (jntra)du ral lipoma
2. lipomyelomeningocele (Ift~)
3. fibrolipoma of the filum t.ennina\e
UPOMYELOMEHINGOCElE
A subcutaneoul lipoma. that"",_ through a midline defect in the lumhodo .....1 r...
cia , vertebral neural arch, and du.,., and mell:" with an IIbnormlllly low tethered cord".
'l'hne .....y be tenninal. do .... l. Or trallsilion.t (between the two).
The int.,.durel fatty tu",..r may alao be known 115 lipoma .,r thec:.uda equio • . l n
addition to bein,lIbnormelly low. the conus cneduU.ri. i. split in the mid line do .... lly
usually at the IIIIIJJe lev.el as the bifid Ipine, end th.i. dors.l Dlye!OIChi.il may utend su·
periorly under intact . pin.l.rches'". There ia a thick Iibrovucular bend t.htjoin. the
lamina oftbe most cephalic vert.eb"e with the bifid I .. mina . Tbil h.o.lld coDitrict. the
cneniogooele aac.od neural u. .... e. caUtin, a killlt in the"uperior , "rl"II<;I of the menin·
IIJCf!le.
The du ra i. delli_nt at the level of the do ..al mye"-'hisi., and reflecu onto the
pl.code. The lipoma paSSI!I through thill dehitoen<:l to hKoOJe attached to the dor..llu ..
face of the placode, and m.y continue COI!phalad u!;lder intact arch.. with the pouibility
of extenlion into the central ca.o.al.uperiorly to level. without dorsal lOyeIOlChi. is. The
lipoma i. di.tinctfrom the normal epidural fat which .. looser and more areolar. The.ubar.chnoid .pace typically bul,N to the aide contr.I.t.ral to the lipocna. TheM lipomas
accou nt for 2K of COV«ed IwttbOlacral maMU.
PRES£NTAnDN
In a pedi.tric seriN, 56,. preaented with. back 1DIlM, S2";Il. wi th bladder problema.,
"nd 10,. beaoute of foot deformitiN, parelyoi. or le, pflin".
PHYSICAL EXAMINA TION
A1OlOIt an patient.l have cuta~ .li(O"lata of the auotlated .pin. biflda: fauy
.ubalt.aneo.... pad. UoeIIted ovar the midli"" end usually extend, asymmetric:ally to one
lida) with or witho ... t dimple" port-wine Stainl, abnomul] h.ir, derm.lsin ... open;ng,or
NEUROSURGERY
'"
akin appendages" . Clubbing ofth ~ feet (talipes equinova rns) may ~UT.
The neurologic eKarn may be normal in up to 50% of patients (most presenting with
skin lesion only) . The most COmmon neurologic abnormality ""as 8eUSOl}' 1069 in the sacral derma tomes.
EVALUATION
Plain LS spine x-rays will show spina bifida in most cases (present in almost Bil by
definition, but some may have sefOlentation anomalies instead such n butterfly vertebrae). AbnormaLitiu of fusion and sacral defects may also be se<!n .
The abnomlally low conus cao be demonstrated on myelogramlCT or on MR!. MRI
also demonstrBte$ tbe lipomatous mUa (high signal on Tl WI. low signal on T2WI).
All patients should have pre·op urologieal evaluation to document any deficit
TREATMENT
Since sympl.Oln$ are due to \ 1) tethering orthe spinal cord. especially during growth
spurta, and ( 2) compression due to progussive deposition offat, especially duri ng periods
ofrapid w.. ight gain; the goals ofsu rgery are to release the tethering and redu"" the bulk
of fatty tumor. Simple cos",etic treatment of the subcutaneous fat pad does not prevent
neurologic defIcit, and lJIay !Oake later definitive repair mOre difficult Or impossible.
Surgical treatment is indicated when the patient reaches 2 months or age, or at the
time of diagn osis if the patient preaents later in life. Adjuncts to su rgica l treatment inel""' .. evoked potential monitoring and laser. Overall, with ,urgel}', 19'1> will improve,
75% will be ullchanged , lind 6% will worsen. Foot deformitiee olten progress regardless.
D ER MAL SINU S
A tract begilUling at the sk.in surfllce, lined with epithelium. UsuaUy Ioc8ted at ei·
ther end of neural tube: ceph alic Or caudal; most common location i, lumho$ll.cml. Prob·
ahly results from failure oftbecutaneous ectoderm to separate from the neuro~toderm
at the time afelosure of the neural groov .....
SPINAL DERMAL SINUS
May appear as a dimple or as a sinus, with Or without hai rs, usually very close to
midline. witb an opening of only 1-2 nun. SUrTl)unding sk.in may be uormal. pigmented
(·port wine~ diseoloration), or disl.Orted by an underlying mass.
The si nus may terminate s uperficially, may connect wil-h the coccyx, Or may
travenle hetween normal vertebrae or through bifid spinee to the dural tube. It may wid_
ell at any point along its path to form a cyst; called an e p id e rmoid cyst iflined with
stratified $quamous epithelium and containIng only keratin from desquamated epitheJium,orcalled a dermo id cy3t ifalso lined with dermis(conUiningskm appendages. such
as hili< follicles and seba~u . glandsl and also containing sebum snd hair.
Although inDOCuous in e ppearance. they are a potentIal PIIthway for intradural in·
fection wlUch mlly result in meningitis (sometimes recu,nmt) and/or intra thecal abscess.
Le"" serious, a local infection may occur. The lining dermis contains normal skin appendages which may result in hair , sebum, desquamated epithelium and choleeterol, withln
th" t,·"d. lui. Ii re~ult, u,~ ..... "~" .... "f1.4,, .i"u~ trae1. ,.. ~ inil ..!i", ,ULJ ~ ...., eli""" ... ...,nl"
(chemical) meningitis with possible de)IIyed uechnojdjtjs ;tit enters the dural sPlIce.
InCidence ora prf's"med sacr al sinus (a dimple whO$<! bottom Quid not be Seen on
skin retmction): l.~ of neonates".
Dermal ainuses are s im ilar but distillct fro", p ilo nid a l cysls whkh may also be
congenital <although 80me authors say they are acquired), coouin hai r, BrB located 8uperficial to the postsacral fa8l:ia , and may been!))e infected.
lfthe tract expands intrathecally 1.0 form a cyst, the maSS may present as a tethered
cord or as an intradural tumor. Bladde r dysfunction ill usually the f'rst manifestation .
The tract from a spinal dermal sinus always courses ceph alad as it dives inwerd. An
occipital sinus mlly penetrat.e the skull and can communicate with dermoid cy~ts as deep
as th e ""rebellum or fourth ventricle_
EVALUATION
Thes-e tracts are NOT tel be probed or injected with contrBst U thiS can precipitate
infection or sterile meningitis .
'"
4. Developmental anomalies
NEUROSURGERY
ElIaRI i~ dJrectt:d IoOw(utb detllClinllablIOnuali!.iee in .phincter runttion lanai and
unnaryf. lumbosacral reflne.. and lower extremity 1le"0Qtion and function.
Radiologic e va luation
When lean at blrlh,llikJI.I~.lI.U'1 i. the belt meanl to evaluate for 'vim. bifida and a
poIIsible nlll.. in. ide the o;8nlll.
Ifleen initially followinll biM, lin MRI .hould be oOLained. Sagittal ima&d may
demon$t.r~te the ttllct .nd ia pOint of.tWo.hmenl. MRlal*O Optimally demoNtc.t.eI
m..uea (lipomas. epidermoids ... ) within Ihe CllnaJ.
Pillin ,,·tII),1 lind CT Ira unllble to do:tmOr\&lrate Ihe fine ttllct which 01/lJ' .. ist between th skin lI11ld Ih<l dura.
PI"n x·ra),1 mult be done when embarkinll on ,ursery u part of open;ti ... e p1ln .
uinS, III p~lI"r'tion for It.. possibility of II rompl,te Ilm;nKICIl\Y.
TR~TMENT
Sinuod abo ...e Ihe ,umbolllocral ,..,gion ahooJld be IUTfl""'U" ,..,moved. Mol'll ea udl1ly
located ,;nusea ere I lillMly controversial. Although. 2&lI. o!vruwned Acnl.inUHI
liel!n el birth will regreaa to II de~p dimple on follow·up (time not specified). il i, recom·
mtlnd.,d th~t 11.11 dermallinnllell should bllur&ic.Uy explored and fully exc:.1Ied IIri!u to
lhe development of neurolCliic delitit or &iJTl& oflnfKtlOn. The r Hult. foIlowi llil inlndu ·
r41 inI~tion ar, never _good. aiwhtn und"'rllken prior to infleUon. s...rgm within th4
week of djusnl)lli~ ilappropriate. Sinuu. that U!rminale on the tip oll.he COC<:)'l' Mlrely
penetrate th"'du ra. ftnd may not need to be tnoated unlc~ local infKtioll DOeU .....
Surgical tecbnique
CRANIAL DERMAL SINUS
Stalk begins ....,th a d imple in the occipital
0' nasal region . CutAneoul.tigmata of
h",mangioma, 8ubn,Jtaneout dermoid cyst. 0 ' .bnormal hair form.tion mayootur. Ottipila.lsinu&e5 extend <:IIU~.Uy, lUld ifthey enter th".kul\. theydosoel>udll to the wraoh.,
herophili. Preoentation rna,. ' ndud" recurrent toa.:t.Hi,1 (usually S. ""nrwo)or _ptio:
men.i.11git.i, . .Evalultion should inelude MRI to 100». for intr!lCraDial ext.e"'lion I.lId .,...xi.
lted ~ nomalies , including an intnlmonial dermoid cyst.
TJoeatme nt
WbeD opetllt;ng 00 • cr.rrial dermal sOn" •. uroe II sagiualtv based Incision to pumit
do-ep eJlploration. Th& tract must be followed eompletel)'. Be p~pared to enter th .. pOlIl,(!rior foasa.
4.10.
Klippel-Feil syndrome
Conllcni\al f... ion of two Or more«!ovic.ll1 ~e~rH_ Rangoeo froln fusion ofon ly thle
bodiN (conpnltaJ block verubrae) to fuiion of!.hl mtlre veub' H (iocluding posteri·
oraJ",mlnlll). Result. from fallureol nonnal ~tation ofccrvtc.1 sornitef betw~n 38 weeks llllation. In~oI vltd vRfUb...1bodies ueoften flau.cned IlQd .......aaIM dioclpllcU .... abMnto, hypoplutit. tiemiv",lUbraa .....y also DOeur. Neutlll forumina are 8malle,
thin nonnaJ aGel oval. Cervka J lterlOSi.Ia ....... Com plitt> .bnn~orthe patteno, t iementa with an enlarged foramen m'fIlum and fiud hyperemmion postu re I.ItaUed In.
ieocepbal)' and il ,arl. lneio;lenceofKlippo:l·r",il il unknown dIN! 100 iLl rarity alld tbe
fact that it " frequrnlly uymptomatk
Clauic clinkal triad (an 3 at'" pHUnt in < 6011>): low poIoterlor hairline, ,oofU""d
neck (brevictlJli.), aod limitalion of neeIt motinn (may nDt. be e~ident if < 3 venebne ar.
fuMd, iffusion illimitl!d only to the 1 _ et1'VieaIl_lJIO. or ifhYJll'rmobllily of non·
ruNd """iI!n~ compensala). Limit.tiDtI ofmovlrnent I, more wmmon In rotation than
flexion.f:lltanl1Dn 0' lat>eral bending,
May a«u r in COI\iunction with othu fonpnital o:em",llpine al'lOmaliH
t>a.eilar iDlprfiSion and atlanto-ottipitalhDioo. Other dini"",l.ssociftt;onl include fICOl;·
01;' io 6O'lto. f.eial .. sym meuy. tortinoUMi , _tlbinl or the ofCk (~aUed pttlryVwa colli
wbeo II!Yrre). Spre~I'a d efnrmity in 25-3S'it {raiHd IleIPull due 100 fal lure o1the
",pula to properly d l'AOC'nd from ita recton 01 rarmetion !\ilh in the ned< to itt normal
position lbout!,he Um' time elllle KlIppe.L·Feillnion oce ..... l. IY"k lnwl ]mirror mo·
.,,<,'h ..
NEUROSURGERY
n.
tions. primarily of hands but ()(Xuionally arms also) and less commonly fadal nerve pal_
sy. ptosis. cleft Or high arched palate. Systemic congenital abnormalities may al80 OCCur
induding: genitourinary (the most frequen~ being unilateral abllenoo of a k.idney l, car·
diopulmonary. eNS. and in ~ 30%deafnells"' (due to defective development of the osseoUs
inner ea rl.
No Iymptoms have ever bHo directly attributed to the rused vertebrae. however
symptoms may occur from nonfused segments (less common in $hort-segment fusionR)
which may be hyper mobile possibly leading to instability Or degene.ative arthritic
changes.
TREATMENT
Usually directed at dele(:ting and managing the aQO<:iated systemic anomalies. Patients should have cardiac eVllluation (EKG). CXR. and a renal ultrasound. Serial examinatio"" with lateral flex.ion~xtel\Hion lateral C.spine x·raY5 to monitor for illlltability.
Oc.:lIsional1y.judicious fusioo oren unstable nonruaed aegmen~maybe needed at the risk
of {urther 1000s of mobility. Alaosu p<J~ 142, for recommendations rega rding athleti~
competition.
4.11 .
Tethered cord syndrome
Abnormally low OOt""'S med·
uHarie u90Ciated with a short, t.b..ick· Table 4-16 Presenllng aigoa and aymplom."
ened filum term ina Ie. or with an
intradurallipom. (other lesions. e.g.
as Lipoma extending through dura. or
diutematomyelia a/'1l ooneidered III
separate entities). Mast commOn in
n,yelomeningocele (MM) . Diagnosis
must be made clinically in MM. 88 al most all of these patients will have
tethering radiographically.
P RESENTATION
PTes.enting signs and 8)'1llPtoms
in patients with tethered cord are
shown in Tabl~ 4·16.
MYELOMENINGOCELE PATIENTS
If 8 MM patient has increllsing
high irJ:idence oIscoliosis arid ~ due Ie incIusio:wl
scoliosis, inen'!asing spaaticity. wo"',
of series by HQltm:an
enlng gait (in those previously ambu·
latory). o;>r deteriorating
uradynamics-:
• always make lure thM there is II worlting shunt with normal ICP
if painful. should be con~idered tethered cord until proven otherwise
if painleSl. should be considered syringomyelia until proven otherwise
may be due to brainstem compreuion ($ymptomatic Chieri II malformation. M~
fXJl:e Ion reqUIring posterior fossa decompression
Scolios is in tethered cord
Progressive scoliD6is may be seen in conjunction with tethered cOTd; early untether_
ing of the cord may r~ul~ in improvement ofsco\i(l6is. however. untethering mus~ be
done when the scoliosis is mild . When cases of s 10' S(;Oliosis were untethered. 68% had
neurologic imptovementend the remaining 32% were stabil ized. whereas when scoHosis
is leven'! (., 50°) ~ 16% deteriorated.
TETHEREO CORD IN ADULTS
Although most casel of tethered cord present in childhood, casH of adult tethered
cord have been reported (_ 50 publi.hed ClIseS a s of 1982). For comparison of adult and
childhood form • • au Table 4·17.
n,
4. Developmental anomalies
NEl/ROSURGERY
"
E VA LUATION
Rediograph,icaUy; low con .... medllilana (below L2 ) aDd thickened /ilumlerminaJe
(nonTI81 diameter < I ".m; diam'ltars > 2 mm are pathological). NB : apP" ..... nl mum di·
ameteron c;r-rnyeJogram m'IY '1Rry with concentration of room ' l mllt4!rllll.
It isd'fficult UldifTenmtiate a t4!tbl!red cord fl'Qnl a congen itally low lyingrord {filum
diameter i ~ &eo"'alLy normal in 18tlilr).
P re·op evaiuatiolJ
PrIMlpt'rative ill.\I!(JlPttoIl1'Ol i •• trongly recommended, e8llecia II)' if the I'P(ient
ronlinen! (po!Itoperalive chang es;(1 bladder function are not unl\Ommon, po6IIibly
due to Itret.d".ing oflh" lawe. liberl! oftbe cauda equina).
_\til
T AEATMENT
Ifth t only abnormality
IS
II thickened, Bhortened fIlum, then .. lim ited lumbosacral
laminectOXl'lY may suffice. with diviSIon of the filum once identified.
IfaiipOms is fa.und, it may be removed with tbe filum if ilaeparal.lla easilyfrorn neuraj t.iuul\I .
Di.lltitlJU illh in g feat .... res o r the filum t<!.rmillaJe
The filum Is dIfferentiaLed f'r<>m nel"V~ roots by presenoe oftbllucteiistic lIquiggly
vtssel on Buriace of rtlum . Also, under tbe micros~ope.. the filum 11M Ddistinctively wh i{er
app"'aran<:e than th nerve roo-tII, lind li!/amentoua_like . 1I"IInda eaJI be ..."n ",nn;nlC
t.hIVugh it.. NB : ;nl... -op .1"ctriO>ll a Umula Uon wnd "",urlling of.n .. l . phlno"", EMG .... e
more definitive.
OUTCOME
In MM , it if; us ually ImpmlllibJe 1.<1 pennanenl.ly un tethera a,"I, however, In a grOw_
ing MM cbild, il may be thai after2·4 IlJltetherinp that tbeth;ld will be fi.nlahed grOwing
and tethering may ees"" :0 be II problem . ClOSe. that are un.Let.Mred early in childhood
moy rl<\:ur laLer, e.reciall, dunng !.be adole""en! growtb·spurt. !/lciden<.:e ofpollt-op CSF
leak; 1&9&.
Adull form : " ".gica! relelOlie
.elum of bladder function.
NE.UROSURCERY
i~
UIIuidly good fo. pain ",lier. Howlflver , il is poOr for
~.
OevalopmenuoJ8J\omalies
'"
4.12.
Split cord malformation
There is nO uniformly lICCf!pted nomencllltu,"" for malfonnations characteri~ed by
duplicate Or splil spinal cords. Pang et a1.'·' have proposed the following .
The term split cord malformation (SCM ) should be u$ed for all double spins] cords.
aU of which appear to have II eommon embryologic etiology.
Type I SCM
Defined u two hemiC(JJ"ds, each with i1$ OWIl oentral eaRs]"nd aurl1:mnding pia,
each within /I separatedurlll tube separated by sdural -sheathed rigid osseocartilaginous
(bony) median septwn. This hll8 0ften (but not consistently) been referred to asdillote m·
lllomye lia . ThereaTe abm>rrlllllities of the opine at Ihe level oflhe 6plit (absent di&<:, dol'*
sal hypertrophic bone where the median ·spike" attaches)"", TwO-tll' roB have over lying
skin abnormalities including: nevi, hypertrichosis (turt of hai r ), lipomas, d imples or hemangiomfl.'l. These patients onen have and an orthopedk foot deformity (neurogenic high
arches).
T're.atment: 6ymptoms are moat commonly due to tethering of the cord; and liTe uau·
ally improved by untethering. In addition w untethering, the bony septum must be removed snd the dun reconstituted as a single tube (these spillO!s aN! ol'l<!n very distorted
a nd rotated, therefore start at norma! anatomy and work wwardsdefect). • DO NOTcut
the tethered filum until afkl: the medilln septum is removed to llvoid having the cord retract up against leptum .
Type II SCM
Consists of two hemioords within a single dural tube, sePllr ated by II nOllrigid fibrous median ""ptwn. This has 80metirnes been referred w 88 dlplomyel iR. E~h hemi·
cord hlUl nerve root. arising from it. There i& usually no apine abllormality at the level of
the split, but there is usullily .spina bifidll occult.n in the lumbosacrlll region.
T'reatment: cons ists of un tethering the cord at the level of the spina bifida occulta,
and occasionally lit the le'·el of the split'''.
4.13.
Miscellaneous developmental anomalies
Some anomalies that may be seen by the lIO!urosurgeon indude the following.
Septo-Qptie dySpJ aS;8 W '.11 ..... ' ..
AKA de Morsier syndrome. Incomplete early morphogenesis of anterior midline
structures produces hypoph.sill of the optic nerves and possibly optic chiasm (affected PIItienta are blind) and pituitlll)" infundibulum. The septum pellucidum is absent in about
half the cases. About balfthe cases also I"lave schhencepha1y (_ ~f 112).
Pr-esentation may be due to secondary hypopitu.itsrisrn morufesting as dwarfism,
i$Qlated growtb hormone deficiency. or pa.ohypopituitarism. Occasionally hypersecretion
of growth hormone, corticotropin or prolactin may occur, and sexual precocity may OCCur.
Most patienw are of normal intelligence although ~tardation !lilly occur. SeptO-optic
dysplasia may be a less severe form of holoprosencepl"la1y. and O«lIs;onslly may occur lIS
part Of lhis anomaly (with its attendant J"KIO",r prognosis for functio." or survival, Ut
PQ8e 112). The ventricles cna~ be oonnal or dilated. May beseen by the neurosurgeon because ofeoncems of possible hydrocephalus .
Absen ce or the septum peUu c!du,m .. l. '7ll
Absence of the septum pelluc:dum may oc:cur in:
I. holoprosencephaly:.u pase 112
2. 8chizencephaly: IU ~e 112
3. agenesis oft.he corpus calloeucn: _ PGIIe 1/4
4. Ch.iari type 2 malformation: see page /07
5. basal encephalocele
6. porencepbalylhydranencephaly
7. may occur in severe h:odrocephalus: thought to be due to necrosis with ,"""rption
8. septo-optic dytlplasia: sON! .. bo""
4. Developmental anomlllies
NE:UROSUROE:RY
References
4.14.
v... {)O:, Me<h. f. B<Ul;"..'. It An<hooid <,~.
'"
.... ,nidd). "..!01 r.....,c........... ,><iIIm<., Qf ",I>1"";"'III!<l_'~~11'_, J fIIe.to!
1.
M.yrU.Ao<~ .... f. _,O . "..r" ~_"""",
PQ<Iolll ,_"~~ "'... or II>< _lhI ,.""....
001 klb<.
J ... _ , Nn.~ '~ ~ , .
6,1'lli2.
K_OR . Fnw"""MS.,W, ..... C81_..",.
.r .~"".icI"l"""'<lUldmI J ,..".-. ... ~ . IJ,11.1981>
Pi< .... .: ... , A. Copell< l ..U,".,,' R,.' .0/,' Pre",. _
..,I... • od
of .... ~II ..
R..l .w or lO ...... J N•• , .... "" 73: '""' .
...w••
"
_ ,.""".J.......""'....
"""""''l "'r< ItIo , .J'~ 11 1)101, I~l.
' ''''''' _'ro""rlll. o:>o<l(Ilt<r&!".1 10«>. A ...
<,.,,:
ma,, ,,._
".
~,
orE!LoOid
""'' ' ' 'VIJ'
po~.Qr-....- ~ t.""' ~ _<,....
tIl,,,.--,..«y
_tono>od_.
<>1111<
I~!tl ,
to
.,odd,. ......."r.,... s.... I'!<. ror 17 JM·'.
ttoprHl,_rA· E"""""'P<"""""'......,
.w:..............
,.no.......f"Y
....,.r~ ....
one! .~h""
U<IIInOIO'
ioI <.ro<>.
ofu. __
0,
.0.
II
11
~) .
1))1).1, 1991
"". Lit; ,.......... "" I\lboJII" I.< T..... "' ..... 01
""."""'I'JUY
1991 \Itt'''' 1
~.Iu
0100
IS
l~
17.
"
.,.It....,,.",,,,,,.,",,,,",
1((I ,)' S.62 . 1~
IC.&lMJ F.Si"'1MIotp/1 O. Wcn60 S ... oJ, I• .....,...
. io' Ii"" .... D",_,I< .PIII .000000001c «w,,,,,,.
N.~ ' 2 . n40.u, 198CI
"""'.J
F.
III: Tho .. Io,;",w.'r
,."w...K. ...".......
_... "(. .......
''&I11'''',.. ....
el'l\O<ol m•• ,I.... tioo. of t fp<ll!>oJ"";': Mtoon--..
~,..
I "~,
~.,
'9 ,
::0 .
.1.1<>"" y. ,.,...."""'" Cf"
JI.
,_".0:
17<I.lII). 199" I ..... ')
Cola'" M. fJI ... nn M 5 6 . 0....:"""" D
:u.
(If ,.",,,,,,,,_ 'l'''' )
SO; 179, 19\I<411<i1<')
tfu R' N<",.'.. ncCf .. o' .....".,. ..... c~ .. . J No .·
/I.""""".
NEUROSURGER Y
~, G'JM-
I ~a):
!·7. 19'>11.
f""""",
_la"
PlllllaurQl" 1r20-<i. 1m
HiU"'_MC. '_,K L.J ....... H ~ """."".
I.. <01'1>11-"", ooJ """;.,.,_;.. ""''''''1l.<'1
6 39.!98(1;
H.".. 0 ~ . 8c< ..'L ll. M.... 1<aY K F. .,~J ,:
l.-ombck>tG .".,.,0.... "'" ): ThE !1IIt!I:ooIoI~ ,"I...
...",lojl...
"'oo.l~""loIa'ol · 'J _' ~
"............
,~,
". on.
. . ....1~ 1r,cqo._ 11<1 ........ ' ....... ) p<dr.lc 9ll,
"
1911 ,
S....... of Ptdr_ N.......,<zOtY of ~ ... """Qq
......... "OII 01 "'LIIOfoaru,l S"" ..... ,{..J.) Ptdlo,·
ri<""""""'l"Il'I .. «l., Clnr .... "".';'''''IOII. N...
'r"" .,n:.
M ...... 0 Do ~IIrp" of r.fon<)' ",d <",(.d.
_
.l.oII<d O - 'C """"'.Spoi",nclol. I%9
s..w••""d. c.S.......... ],O N: ... _phIIlDa""l <,",.
..r",.I."" '" ....: p".r ''''pbo_'""loocIt•.J
N..........
,,*
lO H I. 1972.
OrtmcIPW M..." ... "'oftll<r.~I .. I/IIoII""",.
,1000. in " " ' _, CJ;>r1cil N<",."...,,)CJ
~. 1911J
"
LoP<Mr, M 5, r.po,....""" 0 M ........... p~ . L.m _
_
.. I " .. ~ c,1I .... ""... J "' ......... "
71,U I-5.19IIJ.
"f, Coo,-P ~."..- ..
""""OlIO 0 l , ",""E.... C D. 0:w0,..i1aJ ..."",1>1
1Ottl<01I", ~~"io<I> "&OJI1i"I.h<MCII
.. vxIMod,ooo!i" -.•",h•.daor"...-,,, J ....
O,u.o, 1 ' ~', !9il.
o.n..SIC. ~oIJ...,j","i:oIlkl r.o ~.
NI'f ,R•••",HL,Kcnol."JF. .. IOI" T"""''''_1
.-- ~f)'4l;MS·8 . 1~
...,., !'on
~ Rr." "' ofc.,..",, ..
,II< Ioo<p.w ro, ..... obi"""', 19n.1982 )
M<Comlr r G: T.......... 01 r....o<looollomlo<lood
'~_i.
,CUrr /Mnb ...... '2. 66' .
) 1'1,.,...,..91 OJ: 211-lO. 199\1
S'O_ S, M oo R. Bila l, ,,,J_c..1A<oo< .... I<pof.
Sf"''''.'''.....1Id try.."" "", "",,", t,i!q>slo,j()
l))r1!l4-JOl.lm
,..,... II:'fI Q1>&I'Iorlf ZO. 1}'1.2CJO.I .
r.,o .. l.cwi. 1'1 l.~ .<".. N. s.:..,.iIU 1"."aJ
N.........ri< oy .. of"'" _ 1 " , -1... ",,10 . N..•
O!
1'1............. 61 . JoIO.7.'9&o!.
Knr", II F,OoQdnoh I T' '--bdoi<! pio;o-pil'
JJ'I",, __ .,.61 . 11l-9.I'IU.
~"",of ' ~~lrIIIC""""''''': c...~
If.
~ .~""
. pel
_
"1....
SW.Zinu!><,,,, •• ~"' . II IIu ," ~ l T .• , ....
c"'P"' ••n....., 0I>d lifllbC
R..,"" O.,.",1IIIl E, Ciooai'i G... (1{~ "'",,",M' r.:.-
.......11>.'''... II> "'pcn'• • )'<\I<> .... J "'......... "
., 66-/1. \9\11:1,
M.'".... I( F, HoiTIIWI H J, _
011, ,, . "
""""n''''I\~ ofPodiornnT..1. Fotoo o. 1. ! ... 1'bti\""',"I_ SIDS. Pooi' .... i.o&>noilSrus
Iki"_ ..
Mit ......1.... of "" .... IDJIII"" "" ~ . Rodl·
I_
"
"
"
bobb_ ....l l.)_lrl"~ .....l<r.. _
""",. ,. •• __ ......,., :PI), 1'JlI1
~Ibri,," , L Ttt.r.1""'''' 011Xlbbl • .,..,4d 1Io1l .,odromo
b)' 1.. ...,.11.,..1 cl"'«"''''¥
A S9).
S. 19111 .
RU...1I 05,b!><,,, .... \.. ,·p",,,,,,,,,or......-ro
of llk ...........)'>! .... . S<IoOll. Will,_ ODd
WiI ......
m
~.t>loC.G'""1 GuljoC. M,11o<lo J J. MR mil CT
d.oo"-;' "' .. ""' .... " 11,,.,... ,\,I R lS7
'l
u.
JI'I< • •
ropalaol £<p1'l . ...... otl;-III · Il, 1911
0 • ...., E, Tcpo ~1 F.O.ilol O• .,<tIJ CT_.,od
...."lumldo CT d ... """""", to >n<~ooJd cyu>
"'"P'' ' ' ........u.u.
_OflIO>I""" ...
,~
I\~OC1OuIctEM . I """'''C A.S.U.... L N, ".>I.
Op.no:" ."'0><'" or_.....;.j..,idonnotdc.IU
• 1Id'~ " . . . _. R<pO~ onl ......
~: 006-11 , 1990,
R< ..IIOb..,SS . W...,..\>O< 1 UI .....W<1u ...I>II
io\)-1'O''''. .. '''' h~"', N<It"""'l<ry li t
6}'1. 19V
~, • ..,. O.So'"lo·R.... C, M.. <IIoc O. "Ill" rOl'''''
,.."1_",,,;"
l7 ·
)70.7. I~l .
e"' cM J. W... ,"" K ~, WIIH. ""S, NQrrnoI,,,",.
01 'oa"", 1IIIl"'" .. "*'Il<of".... >01 .... .......
'J""""",, The _oo""",,1e
N...... " .. 11, :101-<0. 1M.
T..."O F. r _
I,1;I)oo1 WK , .,ot~ Th< b<o>en
~lariool>tl_ A i .....,...io '
_
......... ,01 ...."""""' •• .-.1 "",.....1Od _
...pII;., ..... lo ollil4l .... ,111....., ..., _••
J~; fj91-9. '11'16,
Cbodd",, ~ W M.C\IotW"". J 8 , 600p F .... Th< .ut.18""""'1"""0.", No ......
.... .or) lO.II6I·7 !, '9n,
G.... G F.Duo< E I( 0....:,.,.0(.... .,.,.,..,.."'..
II)' " " " ' ' ' ' ' _ R... lokro 1I.5; 6U.7 1. 1915.
".
M~
Spdl .... I O. Po'o!! C. Jonco ... M: o.-.cloptncnoll
-..0.1"... 10 "'" """",of ,Iw. I",""",n ...."""' •
_-o.t...
8.... 80, lI ·st 19»-
1'001 K S, LI" R fl .St/Iwo, F"',n oj . ...
",.11......." .., Ro ..... aJ7 1,-"J N.......v ,~ !3'
!D·7.19IIl
O. _G . ~C.llbmi ...... F. «61. a.;...
l .,oI/onno, 1ott Pan I. Con ' .... p
16
r.m. I·7,:/004.
No,,,........
$I11d S,So.,P II! • "'<:qIIlmJ- Ooiari I ..-..If""""""
of,", ... fIi~ 1e "' _ _ ....:
'q>on. J'I ....
4. Of!veIQPn:tenU,t! anomB lie$
c...
".
".
"
".
.
".
".
n.
".
".
".
".
n.
"""'~ J2: J06.9 . 1\19)
1..<")' W J. M._I-. HoMI F: OI.an "..1 _ ",,,
1"<.."'I",I. .dol,,, A "'1",,,1 • .,.,,._;,, 171
...... rI_'lU)' 12c J77-110. 19n.
8<;"'.; C K. Cock<rllun K p. Mul' OIi." ",t.\fo.I .
"' .. _ . C01I'<mpN"" 'O""121 (2(;): 1.7.l(Xl1.
RI>oIoo" L: Mi<'-'V'I'of AnIOId·OI..,; ..,.If",·
.... "'" '" """'" ,."h an(! " ' ' ' _ h,dromy<l io. J
N<'ur-a~' : OlJ·ll. 1976.
Ci"iOId S I. w I"r..1d I "' : Oscillc>p.i, lind pri""'I'
~"I1., «10]>'" C...
vitw olth< lit·
''''.'' . N"",,".'1"y 29: 912-4, 11/91 .
Abool ... " O. So"", K .(;0)'0' C "-" (1/,: I'o.t'KIIl
of «",.. II...,n"Is In '''" _lfIOI>\liobon ond I.
pOl"''''' ...;'" Ch,an mallormat_ "'I" ... 'i"""
. _ h wi," MR imo,i.J. J Com"". "..", To""'V9! IOll·6.I'ISS.
8..-1:". ... " J. Wippold FJ .Shmno"J L. ,, <11"
SI""fKon« of <... bell ... IOMIlior pooit .... "" MR .
..... NR 7: 1\IS·9. 1916.
M", . 11s 0 I. Dj .. O. EJllin T K, <I Ill" Vlrione. or
II.. pooit;'" of ,he «rebon .. "''''''' ",jlt. .,.: "",.
11m;""')' .. """ . Rodlolop- In (1). 111·1. 1991 .
lik>r>du B I. He<lh•.., C 1...
P A," tIl _ Tho
fCIOl .. "," of 'yrioJOll)W<> .. y<b ..... Il00. biodbr>oll
hom~ af.. ,
f.,... dt<~ . J
N"'_'139'(1): 111-4.19\11.
M• •" , J. " ,.., M.c..rn "'ri M." .," "'yml>,_Chi"';,ypt I m>J(".,......_ i<I<.'if0<6011
..... In<lk "son>n« 1""'1"'1 . J Nou..... '11 '12 (6):
"pM"" ..
(i,,,
--
1'0>"""
"
~.
".
"
".
".
...."
w.
n.
n
"
".
OM..-' tnalfoln.o""n .... hlla .. " ~vi_l y lfO,lOd
wilt. my,Iome.;'.-k ,kI'1ft ,,"" 1I0I0.,,. J N... •
......... n: 181-1.1992.
Part. T S. Holfman H ' . """"rie l E B." 111_ Eool!<'
n..... wi", ... _itol <!<comlft_n or tho ""'"'d·
a.....1...
,.....~. i.f..... "'illl mY'''''"'
''''''t<>«It. N<""""""1 1]' 101-.12 . IllS)
PoII",,_ I F.,..,. O. K""ooh,. S . .. 0/.: 1<1< • .".....
d)'IfWJi ..... U;'" ,.,... OIl"; OIoI/omIoo_.
N....-. ..." )O: 7I»· I ~, 1m .
HoflmM H J. II<t>dri<l E B. H.,"""",,,, Jl P: M... ·
,I.... '"'". ,,"" 1IIHoIV ..... of -""oI<I.a..".; mal·
fotmo'ion on ~"..... w"h my._,n"",,".
Cbild. 8",1<1 I: 2lS·9. 1'lI~ .
CI]bt.. , N. 1- . k 1..1IOft< I.. a. <,til., C<-non.l
"."."'" ')""'''' 0"""",1",. "10<1, ,,,, .. i,h m1'1om'
......"".... hydnx.phoi",.""" ,Ioe """'ld--Chlori
"'.If_.... , R.. ppg; ..1ofth< ..... " ."dl", ,II<
po~;' 01 poo«'"" .. oral ,.be <I","," dor..... N."""""".,. 11: "9--601. 1986,
Bell W O.Cilsnlty E 8. _
DA. ,,0/" Sy"'l'........ Ic !<ff>old-C1>i"'; ",.lfOI1"O""": Ilevlo .. 01 , • •
perle"", ..,," 22 """-•. J 10'<1"... , .116: 11:-6,
If,,,,,,,,_ ..
1~7 .
Ral""">!i A I.Samo<l .... G. Y"""'P") I.. .,0/"
" ..... , olll!< fo'''''''n. of l-"",ht. ond
Tho D""'y·W.lko, ,y" .J N.u,... ..... ll: 202· 16•
1.1.""",,,:
,,<>I.'
lI"'h! F.,... ~ K _ ~ .Jl<.;.:- O.
Tho
INwIy.WOIk<r ....1/"""";",.' " to.",,,, 01 40 <AI<>.
JN ~61 : JIJ ·n.19 "' .
. ".
Nott·,,,,,,,,,,,, •
" 0,7 K. F.1oonor M ,, :
....osl. of
II>< oqo«tOCl i" """I,,. BrU M«I J 1: ' !~-1O.
..
".
".
"
"
M.
U.
".
0> .
...
...
".
".
V_ _ I . H1_R,"""'·' ....... oI_6o<' ... ~
>t. and _ ! ""....... hr6<o«~u, l" ,110 oldo,-
'"
4. Development.al a nomalie$
Nou'''u.rc 1'Io ,<~ io.,.,. 0\9 ' '19·J'.
61.1~1 ,
Do-My<. w. z"",.. w. ~.I ..... C G: Th< f..,. pr< .
d", .. ""- ""I., Oi'ioonic ,11"lf""""" of mtdl&.
f.. '01 .nomol... for ho~"""""", (0111,,,,,.«phlly). hoIl",rb)ol ' 156-63. 196&.
VOII!< 1J: EI"""ol .oni...... "", Ihc fo'ol, N Eod
J Mod n7: )99-407. 1992.
Wtrl<fMM,SI1>j1 I",S. M;"""lI"" : ~
....1 foil< Kid <>p<>SU'" on<! ri,;; of 0«>1«" ". ,,,'"
,.be d.reru. JAMA 2~ IlH-6I. 1991 .
C<nIt~ I", 0 - - eo.."",: II.e<:om_ioN fOf
... or foil< .dd " ' . - !lUmbe, or 'P'' ' ~,ffda
<&SOO ond 0I1oer .... ",1 ,"'" ""Ienl. MMWR 41 :
RR·I •• IWl
Daly L E. Korle P N. Molloy " , ,, 111_ I'0I0 .. ,....1.
,"" noun! 01'''' ""(e....
174: 1691-1702.
,oUt"
M;I ... oky ". l<1"""''' M. Ro<hma<> ••<I .1 .. MIlO!'
001 ......"",.. , •• ne! .. " .... "be ""ft.cu. J"M~
2(;1: 381·~.lm .
P.II"'" G M. Vol"""", """,pi", Mid• .
IJr Mid J 19a. 1300-1. 1989,
M M.U.,n k C. S"'pioo S... oI.:
...-.111" i" .. I." .. '0,i>J, or .."",I 'obo ""1« ...
JA M ~ 27': 1089·91 . ,~,
S~wG M. Velie E M.S<~"<, 0 : Ri.. of .... ""'1
...... do.r"",·afkcte<I p"'p'.""I<t 'mont-..
"""""" . JA_17S : 1(11),6. 1996.
Milo"""y A: Pudic" .. ·,oI ....... b'lv.rl ..... ond
"""on be""r." of holh ond low ",,'ornol .. "'.. ol ·
phI.fotoJ"'Ol<i. ""-ire;" .JJ.V<,on P'1'''''''''''',
Su'1:0tooo .. Gyn«oI 161 : 191 · 7.1~9.
S.""" B K: ",pha.(otoprnl<in .. «<.j",. ,,~. P..
dl ...-3): 111 ·96.1986.
Be" ... , I. 81,. K.1o",_ R 0.0"" " $om<
pr\lblomI "f olplq·I_,. Kf«"'"I. LaD«! 2:
1296-7.1978 .
D.v,dso/I H 0 ." _ R.S,,"', Jl E, "JO""'''
of 'bo_ull'''~''1: M,,,,,,,,,,, "''''''''''''. """.
"'I· 1t&d\OlOcY "S' )71.]. 11lS.I .
\..O<t<t I D. "lvOfd E c: ~. 01'111< <OfPUI ul ·
ic<um. B""" ~ I : "'· 1O.I~.
l.o<t><, I. W""''' M . S~l .. bif"",· ~ ''''''''''''1
"'I"' ....... • " "'b 011 01116 60: 1086-91 . I'ISS.
Ski" S C. Soh .. to Hj<I<octphl"" in my<Jonw"'ft.
""... . Child. 8",1. " .1 )·9. 1919.
$Iwntd W I W: .............. , of ,lor "1'_<ni~fO"
«!,.hlld, ]" Mn_"'''lO''''I<. Ml:1..o.no R 1...
(ed.). G",,,,",,,, S... ",,". 1'«'* Y""' . lm: PI' 1&9·
410,
Shatrotd W I W. Tholl<P"<1lul ,,,,,,,,,.. ;on of ....
....... Iimh "", .. lo.;" ..... ' A~" R CoIIS~,_
(foI11))oI: 106-n.I~ .
E"",1n N E,Rooent.t.ol R 0.;:"01. <I~I.. Shu",
pioocmt'" "'" tnyelooneni"yX<1o « pair. Si",.I .. •
................ ""II'<"tl'l "''''i"l. ClPI"," N". SJ"
" 14S ·7.IIlSS,
H.bboIl>h i0oi Y ,1I0ffnwl II !: fMl1 """",or my·
oklmoo,oJIX01o ODd
tion of VI'
. h.",: T""b";q.""'" "",I ... ","",,,,.,...,- 20: 2 1·
3.1987
Unoo SI.s-..
eruon PC: Evol:od to""""'"0I0fY """,,'iol. in mo.. Moll No.<OI " .
11·91,1%6.
lWinz£R ,R _ _ .\ E.SoarffTB,"d'_ T,",·
<"",p;ul <Ofd f"'''''''"" ... "i.,,,,,,y.,,,,.1< ...
pai" Rodlolot:r Ill : 1s:l-60. 1979.
Emery J l-.l<tod"" R G, Upo .... of OI>e<""" «J"'.. ,"",_t fait, ' ''''''''' ,.b "'; '" ..... <O$pIooI 6y>'*1*11, .... 0.: .. Med Cbllof Nwrolll {Supp~: 62·70,
" cu.."""
". w.".,
n.
N... , ... '1: JI : 1S9-63. 1989 .
Pto<h 8 : Tho Amold·OII,,] m.If"""" ..... """'_
phoa< ..... . Ar<h rI .. <OI 12: S21_lS. I~ .
Tl ..... 1 M ,PlJe.Spdl"". J: /'IounH'adlolop-. lrd
<4, Willl.m• • nd WiI~in:.,8ol' I"."., 1996.
PoII .. k I F.J>u1 D. "'~hI" L<ld!" 0.1<",""
N~
H _ i0oi J G. Robert C M. U""'1 0, 8<,,1.,,"'1'
...:I"" "".",i. ;" ";"1" J N.~,01 rI ..., ....... 1'101'
. ~ it. "Y 37: 1312·S. 197(.
1..<",;,. R J. No"",1 ,ob,,.;.,,,,,,,,. J "MA n9: "s·
". '"'
Dy$t<C N. M."" ... " II . V...c..' do, J C:S, .....
_",011"'; ""11""""'_· ........ ly ... or_
,~ .
O.
,~
...",..... """'Jo<m<".,.nd I.... '."" ",,<rom • . J
f.II""'io,h_"nll«""'~"of·1m_,k
"
ly. J
1'Teprt""",
1.1
.imuI..,...,.. ,.,..
".a.n..
,~
NEUROSURGER Y
"
•"
~
N .,d~IIT p . II4 .I..oneDG. Iot "ll _S l .......
-'lind .... 01 """ .. I ~,....pIoi3m
_ ...."'..
cluld_. nU.t. e lSbo J:
1n.~J . I919 .
SolO K, Sh,,,.,jI T. 50 .. ;0 H. .. «I ~ s.,~!lY ___
f_",).~ .....;r"' ...... of_&<"~.I;".
'~Ii,......
.. .... ~ ..
_.i' ' ' 5.aI,. " . . .
j)OII
t1dId.
No .... 5", "t.II , lOll',
1'o",.UI[ R.Chrfll'J D.Hohpool'J ....,_ ... lIfO"
<p>:tl ... >eo«h r""
1 ob<>on:nalit ...
01<_... u; •. J
81, 7U-jQ , ,.,,~ .
~Sw.R""'",II<CB . 5i:._I ..... JE>C_ _ ·
•• ,ul r..."", 01
".
lt/IIl<f·
..0'" Ilpotno (Iopam)'
.l_"~' R..,~.""kl"""
""" ' " ... AJI'IR . , IOl· I',19U.
8...00: D .... S(iIuo L. $pi.., Ii.,.,..,.. 1<1 iof'"" """
<IIt« ....... • , ...
"""'.s..,..G,......,
OboIu III, Jl)lS.l91\4
!;o~""rct /I 1", l..an£ I R. ~Io<E ..... G 0: !(BliP"'·
1'<;1 'l""f<jMr." _'fel ....,.
or.,_w.., - .
• ~ ... J lJond"rII s.."~.,, . 114(;:». '97~
NEUROSURGERY
•
•
V"""""'JR.\<d J ""'~I ..... ,.., . 2M~ .,
W. D. s....c!rft. "u1oclc1phlo,191i:l
" ... T S.Ca~ w S. lola";' W M •.,ooI .. ~ ••
.~,~ """ """.." In chilclral "'~~ my .." .......
RIoIioIoJoaI t. ....lp'.,. .... -.,coI
_,....." JI'Iw, ..,,,,,6L -1061·1'. I~U.
PIn, D. W;U",'I"' J E: T......l<4rord ' ) ' _ io
0.,0«""
'00.
'"
,~
oduJ .... J 1'01 ......... ,,'7 J~·41, 1982
ho, D. PI .. 101 S .... _ 0 .......... 101: Spb. <0«1
....11....,.. I00' !'»11 t ... ~'"r I/W"'l' of, .. "",,·
, ...... Jot _blo """" «Wd ....
,-..pI) 31 : (,;1 ·110, 1'I91.
. . . 1"""",....,., _
1ioIf..... H J:C_",,1'tti( 0.<1.1 . SplU ......
... II~ , ,,",,I ", ...;r..o''''''''l'or...,!>t:I<>&<...,l.r"'_~t_",..r"""""",,_
......,~ )( .IIO , I<I9l.
'". ",.n
_ _ I(
po!l"''' III ~".
W." .S ....".,.,., . ""~ • •
• Srn;'1fo r«opInble
"'~If""",'k n . """.o
ddpiu •• I9U •
4. Dellelapmelltolonamal)el\
'"
~
-
I,..
,
,~
......
....;,
,
5.1.
Contrast agents in neuroradiology
IOOINATUl CONTRAST AGENTS
Wlt4' ...olubla eonlralt ltfIent.l IIlve ,upC!.neded aide. llan-waWr·fQluble anee . uth
.. Palltopaqudl (Mbyl iodophel1Y lundecyl.te or [ophendylate IIlE'glurtUne).
• C. ution: iodin.ted Q)nln.1t (IV or inu-I·arterial) may delay tXenotion of m e!.romo.; o (Clueopll",t4, AVllKitmed), In 01"11 hypoglycelllic agent u,ed in di.betes ~ype
II. and cln beu.odlted with I.ctic.eidosi.and renal failure. The manufaclun'r recommend. withholding metfonnill 48 hn- prior to and fallowirl( ccmtJ"lUt administration (0.
lance. if the ... ito ev)denceordeclininc re .... 1 function following uae or~anlr8 !t). Metlonn_
[II .hould al50 be h4'ld ~ 48 hollrs before . ny I U.gery, and should not be reatllrted posWlp
until the pIItient lias fully /'eCQvered and is eati'li Md drinking normally.
INTRA THECIU. CONTRAST AGENTS
'J'he,primary .pproved ",eM e mployed ror intrntheal UBe t.oda, is iohex"l (0",·
nIpaqudlH_ Mw...).
madverte 'lt intra thecal inject ioD or ion ie contrast agenu
• C.ution: seriou1 reaction. can oa:ur with in.dvertent inlrathecaL inj!!d.iQn Ie./(.
fill' 1Il,)'e1ot:JllPhy, cill.emography, ~entricu lography , .•) ofiodinated contrail media thai
.re not specifically indicated wrjntrat~lu8e (inclu.ding Ionic cont rast agentll II weI!
a. some non-ionic agenta I. -C. Optir.l)4. Reno-60 . _ )), Thil can ClUS<; uocontrol1able sei2.U"", ;nuace....,bt-.L m-morrh.tp, <:erebn.1 edema. <'Oma. patalysis, anchnoidit;', ml'oelonWl ftonJc.clonic ruu""le SpaII.,s), rhalxklmyolYl'i~ with .... bMqu4'nt n",al failure.
hyperthenni. , and re&pi .... tory compromise, with a signiflCl nl r.talily nte'.
Manag;>ment suggeslioQS ioc:lude:
I . immediately remove CSf' .. conl . .. t irthe e rror il recogniled ... hlll the opportu ·
nity i. avail.ble (._g. withdraw nuid througll ",yelO(Tlplly oeedle)
2. alevllte be.d orbed ~ ":i"lto keep Qlntl'l.at oulol he.d )
8. if there i. a question abuut whllt may hllve OI:CUlTed (i.IL it II not cartain ifan inappropriate conb'aat "ent ... at u-ed) JUld blood lind <:SF with contrest for high ·
perfo'1Il8n/it liqllid chromlltograplly fOf Idt:ntifi<:ation of "rent"
4_ .ntihilumin.., e .g. diphenhydr.mine (8en.drylill) ISO "'II deep 1M
5. respiret.ion : tuppl.mellul oxygen .• nd if needed. inluhlotM>n
6. conuol HTN
7. IV hydratio'l
8. TV l!.eroids
9, IftI.t.ion!fpat.ient;'qita!ed
10. Ir.at fever with eertaminophen and ifllftdftl with. coolinc blanket
11 phermacola,;c pe ..\yJ.i. if _ _ el")' 10 man.ga mu.de 'Cl.ivity (e , . a tomidate)
12. enuoonvultant medicauon: IlIOn th. n one ecent I'''y be nqUl .td (IL,. pheuytoin
.. phenobarbital .. a benl(ldiazepine)
13. conaide r un.nhe l1(lt(l bndll CT tea n· m.y help..-. if((lnt,..,t h e dift'usad in·
Ina.nielly, I7uI thi. requira plactnlf pjltlent nal e nd may 11:14. be .dviaable
14_ InH.tion ollwnbar l ubarechnold drain
l~. monitor. electrolyte., ftntkonvulllni 1....11, cru tina kinaR.(C K)
16_ repeat EEGe 10 lileS' _iture activity while Mdat.edffMItalyzed
'"
5 . Neuroradiology
NEUROSURGeRY
lobeJ<ol (Omnipaque®)
A non·ioni~ l";iodinated com·
pol,lnd. It has replaced metri:l.8mide.
Concentrut.ioo5 €Xpres$OO as follows:
e.g. Omnipaque SOO contain~ the
equivalentof300 mg of organic iodine
per ml of media (300 mgllroll.
UsuaUy reS(!rved for IV contnst
CT scan of brain primarily for pa.
tients with previouY dye reaction. e.g.
to Renor60. Uores and cooC('ntrationll
are shown in Table 5·1.
wtratbecal U$e: Na: only Om.
nipaque 180, 210. 240 and 300 are labeled for intratheca l use . 140 and 350
are n2l FDA approved fOT intrathecal
use, however, some neurllTlldiolOjiists
will use Omnipaque 140 or diLl,lt<!d
180 e.g. for CT ventrkwography .
COlISider discontinuing neurolep'
tic dl"\lgs (i ncluding' pi>enothiazines.
e.g. chlorpromazine, prochlorpera·
zine, and promethazine) at least 48
hours prior to procedure. Elevate
Hoa .. 30' for the first few bours afU>r
the procedure. Hydrate orally or TV.
U..... witb cal,ltion in patienta with
sej~l,Ire history, severe caniiovaacul.r
disease, ehronic alcoholism Or multi.
pie ..:lel"()5is.
lohe¥ol uodergoea alow diffusion
from the intrathecal "pace to tbe systemic circulatioo and is eliminated by
renal excretion with nO significa.nl
metabolism or deiodination .
Ma:rimum dosage : a total dose
of3060 mg iodine should not be ex·
ceeded in an a.dl,llt dl,lring a single my_
elognlln (r.ome say I,Ip to 4500 mg is
OK)(e.g. 15 C1: ofOrnnipaql,le 300. 15
ml ,,300 mgllmlm 4500 mg ofiodine).
Table 5-1 lohexo l coneentrations lor adl,llts
most centers use Op\or.y5. see reX! .
lolow wolh 250 rnl tlOIvs ot 0."5"," NS I(> '$!\y<Ir. '$ po.
"",
180 WlII be ~ _
on CT,....:I $(Ime US(Il-3 rnt 01
1~ or r:f~UI'" l E1CPf. (dtIuIe apprnxrnalely 2 parts CO<>-
u.S! to 1 par1 praseNalMo-\r ... normal saline)
N QN· //IlTRA THECAL CONTRAST
AGENTS
For inadvertent in~ralhecal inject.ion of contrast agents not intended fo r intrathecal
&te obo"".
Diatrizoale mcgJumine (e .g.
1,18e,
Reoo·~,
Reno-di p!!)
Nol for ill lrathoc .. 1 ...." (sloe oboveJ.
A tri·jodinated benzine derivative similarto Conray. BoO! have been avai lable for a
long time . Due to tbe fact th at it ionizes, it is ~and byoerosrnoJar. Widely used TV, in
nel,lr oradiology for TV Mnlrast enhanced CAT scan when there is no history of prior re·
action to TV tQntrnst agenta (I,ISI! iohexol in patienta with previous reaction , sow obowl.
IV contra8tenhanced CTscan of the brain in adult patient with no history of previou$ dye reaction:
A. 300 ml TV drip of Renordip® (30'l1> 8Olution, i.e. 300 mg/ml) over - 15 ",ins
B. 50-150 ml of Reno-SO (60%50]l,It iol11. 1'ypicaHy: ISO ml is I,Ised
body C1': boll,ls of 150 ml of Re nor60® (3 vials of50 ml each ), followed e.g. by 250
rnl of 0.45% NS tohelp preventdehydrat;on. UsuaUy given more slowly lodiab'n·
its and the elderly whe re there is increased risk of reDal fa ill,lre
II
love r8(li (Optiray®)
U~
• NOl ror int rathecal use (ret Clbot.!).
and eoncentration$ include:
NEUROSURGERY
s . Neuroradiology
arteriography: Optirtly 300 (lov".80164%) or Optiray 320 (iovenwl68'l&). Total
procedural dose should oot usually exceed 200 ml
IV contrast enhanced CT I<'an of b rain :
A adult: 50-150 ml ofOptiray 300, 320. or 100-250 ml ofOptilllY 240.
Typically: 100 ml ofOpti ray 320
e. pediatric.: 1...J mllkg ofOptirllY 320
5.1.1 .
Iodinated contrast allergy prep
lndieated for patienta with previOWl hi8Wry of ..... action to IV iodinated eontrast rnB.terial. Minor prevIous reactiOf1s such all hivell and itching . hould Olen! preparation with
this regimen whenever p<>6IIIible . Patienta with IInaphylsctic ! hock Or severe edema cauS'
ing compromise of the airway ~hould probably 1>01 receive IV iodine e"~en with thi~ prep,
unless absolutely lI~aaary. Caution: th e patient may still have serious reaction
(modified').
utilize 'IOn-ionic oontrast medium (e,g. iohuo]) whenever poII.'Iible
steroid ($I" pogt 8 for further details ofsterDid doting)
• prednisone 50 mg PO: 20-24 h rs, 8-12 hi'll & 2 hra before study
• equivalent dOlle <:Jf&>lumedrol® (tnethylprednisolone) f~r TV use would be
~25 mg
diphenhyd ramine (Beoadry~) 50 mg, EITHER 1M 1 hr before,
OR TV 5 min before st udy
optional: H1 antagonis:, e.g. cimetidine 300 mg PO Or TV I hr before Sludy
have emergency equipment a vailab)e durin8" study
5.1 .2.
Reactions to intravascular contrast media
BETA BLOCKERS
Beta blockersea.n increall'l the risk of contrast media ,..,action8. a nd may mask Some
manifestations of an anaphylactoid reaction.
They al$o make use of epinephrine inadvisable since the alpha effects of epinephrine
will predomioat.! (bronchospasm, vasoconstriction, increased vagal tone). If treatment is
required for hypot.!nsion. OlS)· try g lucagon 2-3 rog TV bolus, followo:d by 5 mg TV drip
OVer 1 hour (glucag<>n has positive inotropic and chronotropicefTect that i$ oot mediated
through adrenergic pathways).
I DIOSVNCRATIC REACTIONS AND TREATMENT
For treatment ofinadvertent intrathecal injection ofionie contran agents,:lee fIOIl~ 126.
HYPOTENSION WI1l-i TACHYCARDIA (ANAPHYlACTOID REACTION)
1. mild: 1Tendelenburg position . IV fluids
2. ifno response but remeins mild:
e pin ep hrin e (use with caution in patienta with COl"Qllory artery disease. limited
cardiac reserve, hypertension, Or unclipped cerebrsllUleurysm)
A. 0.J.O.5 ",I "f 1:\000 SQ (0.3·0.5 !ilK) q 1:;...20 UJim. (...,w.: 0.01 "'~ )
B. OR, ASEP recommendations (especially for elderlyor patienLa in ahock): 10
ml of 1:100,000 TV over 5 to 10 min (put 0.1 ml of 1:1000 in 10 rnl ofNS, or
dilute 1 amp of 1:10,000 to 10 ml with NS)
3. moderate to $f!ver~ or ....Qrsenin8" (anaphylaxis): add:
A. rv colloidal nuids. e.g. hetasl.arch (Hespan®)6%(colloids a re required si nce
there is extravascular shift.ofnuids due to seepage, then agents also caIT)'
a Bmall risk of aOerg'ic reaction)
B. epinephrine (..... ",00",,). May repeat It I
C . 0 1 2-6 Urnin per NC. Intubate ifnl!<;essary
D. EKG to RIO ischemic changes
4 . if shock develops: add dopamine, start at 51lg/kgllllin (~" page 7 )
HYPOTENSION WITH BRADYCARDIA (VASOVAGAL REACTION)
1. mild :
A. 'I'rendelenburg JlO8ition
'"
5. Neuroradiology
NEUROSURGERY
B. tv nuid.
2. if 1>0
~IPOru~,
add,
A. atropine 0.15
mr tv. may rep~at up to 2·3 mg over 15 mille PRN. VII'! with
u ... t ion in patients with ... nderlying hean dillea..
B. t:KG andlor emiae monitor: eapedaJly if atropine OT dopamine are uBed
3. ifl>O rupon"": add dopam ine •• tart at5 I'r/kglmin (.n 1X'Il. 7)
URTICARIA
L.
2.
ro.ild : . elf limited. No t reatment ne«Mllry
moderate:
A. diphe nbydramlne(Benadryl<!) $0 mg PO or deep 1M (aVilid tv.tann .....
anaphylnxi . iUelO
B. elme Li di n e (T agamet«l) 300 mg PO or tv dil ... ted to 20 ml aDd gi""n O"'er
20 min •. H t receptol'8 wntribute to whu.l and Oa re ofruetion
3. ""Yere: treat aa llbove for moderate readion , and .dd:
A. epi nephri ne t- 000"")
B. maintain tv line
FACIAL OR LARYNGEAL ANGIOEDEMA
I. epinephrine: I « aoo~. May ",peat up to I m,
2. if respiratory di.tr...: 0 1 2·6 Um;n . Intubate if nece. S&ry
3. diphenhyd ramine: I « ooot.oe
4 . eimetidine:.u o~
5. if angioedemail accessible. add iee pack
6. maintain IV line
B RONCHOSPASM
I. mild to moderate:
A. epinephrine: I « obotot. May repeat up to I ml
B. if respi ratory distreu: 0,2-6 Umin. lntubete ifne«sury
C. maintain tv line
D. inhalatioll3L therapy with a IJ-adrenergic agon;lt. e.g. albutenll (Pl"'OYen·
til®) if respiratory therapy is availablll, otherwise, me\.ered dOH inhaler e., .
pirbuterol (Maxai.rGl) OT metaprotertnol (Meta pre Ie). 2 purrs
2. MVere: l~at as above for moderate reaction. and add:
A. aminophylline 250-500 mg in to-20a: NS.low tv over I~O miru. Monitor
for hypoteruion and arrhythmias
B. intubate
3. prolonged: add the following (will not have immediat.e e!Tect):
A. hydromrtisone 250 mg tv
B. diphenhydramine: 1ft obcM:
C. cimetidine: I « oboue
PUlMONARY EOEMA
L 0, 2·6 Umin per NC. Intubate if necessary
2. raise bead and body
3. futoMmide (l.asixe) 40 I'DI tv
4. EKG
5. if hypo>tia deYeln.. (fDlly manifest aa agitation Or oombativene.u), add:
A. morphine 8- 15 ml tv. May ~au" rupi ratorydepreuion, III! prepand to in·
tubate
B. epilllpbrlne: _ oOOw . • CAIJI'ION: UN only if MI can be RIO all cause of
the pulmanllT)l edema. Patienlll with acute ;n \.raeran'al pathology may be
at riak ofneul"OKf!lI;c pulmonary ede.ma (I« pose 7)
SEIZURES
IflH'ilUIl! is notlH'lflimited . • tart with [oraaepam (Ativ~) 2.... mg tv for a n adul t.
Take precautio... for .t.lul epi lept;"" (IJft pof. 265) and p~ to othe r d ....p .. in·
dkated (I« pose 266).
NEUROSURGERY
'"
5.2.
CAT scan
Attenuation of the x- ray beam on Ii
CT Scan i.o defined in HGunsfield units.
Table 5>2 Hounslield unll,
'f'Iwse unit.9 are not abll(llute. and vary
'canner
'01' II I8mple CT
between CT scanner models, ..... ith II
SlImple beiog shown in T"bI~ 5·2.
If there are no calibration marks
on BClln, ooe Cll n estimate average
adult globe (eyeball) is 25 m m diameter
(through. its equator).
Hcl '" 23% wIH cause an oeule SOH to be isod_
with brain
5.3.
Angiography (cerebral)
Risks
Risk varies with the natw"(! afthe patholOgy being investigated and w;th the e~pe­
rienee of the angiogTophy team. Overall risk of II complication resulting in II pennanent
neurologic deficit" '; 0.1%. [n ACAS, there was II 1.2% oom plication rate ($u P"8~ 873).
General information'
In gen<)ral: non-vascular deep lesions cause changes in venou s structures. BUperficiallcsions affect arterial Btructures. The classic future of II malignant neoplull'I (e_g_
glioblastoma multifonne) on angiography is an early draining vein.
Bovine circulation: anatomic variant where the oommon CIlTotids arise from a comm<m tn.>nk "rrthc oort.o.
Hypoid : having only one anterior cerebral artery las in a horse).
Al lcock ttlat: evaluates flow through the posterior communicating &Tte~s by ver·
tebral angiography during commoll carotid compression.
Fetal circulatio n : 15·36'1> of patieoq supply their poste rior cerebralllrtery on one
or both sidCli from the carotid (via p-oomm) inl tead of via the vertebrobaeilar syetem.
1'0 help find the middle meningeal artery on lateral ECA angio, follow the ante rior
_O'<)p of the ~phenoid ai r einul.
Caroti d-baai lar anastamolJes
A p"r eil<t.ent primitive trigeminal !lr"tery (PPTA) is!lCCn in ~ 0.6'1> of cerebral
angiograms, and is the mOBt COm mon ofthe persistent carotid-huilar IInntam08eS. Arisu from the leA proximal to the origin ofthe meningohypophyseal trunk and connects to
the u pper basilar artery. The VAll are usually small. Occasionally the p-comm8 may be
hypoplastic and the PITA may provide s ignificant blood supply to the distributions of the
distal ba5ilar artery, the posterior cerebral artery and the superior cerebellar arteries,
particularly jfthe basilar artery is also hypoplastic (Saltzman type I ena tomy). A PPl'A
'"
5. Neuroradiology
NEUROSURGERY
may be auociat.cd with v'Ku l" anoOl.l ies.• uch U .oe urysnu Or AVM •. Rarely, aoeu·
r')'1JII1 may directly im'Olve thelle venel!. May "$0 be ''''!leiatoll "'ith lri~minal neural·
gia
(H~ pa6~
;119).
ANTERIOR CIRCULATION
--...,
ANTERIOR CEREBRAL ARnRY ( ACA)
See Fi&""" ,5·2. BrallChee:
reeummt Dr\.o!ry (of Ue ubn er ): II01l.
arise from Al (one of the largu medi, )
lenticulG11t riaU!8. re mainder of lenti ....
ulOltriac.es mDy ariooe from tbi.1a~1
- head ofcaudote. pulamen. and an·
!.enor internal capsule
2. media l orbitofrontal ,rtery
S. fronl.opolar artery
4. cinosomlll"lin'"
A. internal frontal brandle.
L /Interior
2. mlddl,
3. poaterior
1.
8.
P'lnleentMlla~
5. peric:aUoul arte.,. (rootinuation or AGA)
A. IUperior ,nternal parietal (pretunHte) artery
8 inferior ;nlernal P'lrietal.rtery
MIOOLE CEREBRA L ARn.RY (MCA)
See Fil/urt 6-3. Bn.ocbtll ....,. "'idely. 10 relativ. ly tOl1'ImOn ong:
1. medi.1 f3-6 per sidel and l.terallenUc:ul..tri.ta Aneries
2• • nterior telllpo ... 1
3. po$tenor I.ImporaJ
"
l.tenolorbitofrontal
NEUROSURGE.RY
Ii Neurorad.ioloC
'"
5. ascending fronta l (candelabra )
6. pn'!<:(!nU'al (p rerolandic)
7. cent'l.l (rolandie)
8. anterior parietal (postrclandic)
9. posterior pariellll
to. angular
Figure 5-2 Anlerior cerebral arteriogram (lallra! oiew)
FIgure 5-3 Middle cerebral arleriogtam (Ia!eml _J
'"
5. NeuroriJdiology
NEUROSURGERY
(ltoprint«i CO\I~y of Euut>an Kodak COQl .... ",,1
, 1IlIeri'l' caudal' vein
w_
Ihalarn05IIia te VIII)
Slginal
:... I
..~
'"~
su~ anastamotk:
ve!rI (01 TrGlardj
dImdlateralv,
i'lIemal cereblal y.
(
posIerior se-plal V
grW~reblal
==~
".::::- J
-,~
""., (of Galen)
vein 01
poS!erior hom
- slnig-tdsrr"lllS
j
def!!l middle cerebrlll'l!ln
basal cerebril
ve.Io (01 RosenlhilQ
'rIt~O/anastatnoIic
TC .. k,nsverse cauda~ vtUl$
Ve91 (oi llIbbtl
IVs = insoIar .... ins
Fig "" 5-4 In!emit! carotid venogtam (laWai vi ew)
llertebral arl,rIts
PICA SlgmefIt$
am 80letiormedrllary
jon s laletal medullary
1m z lOr1SillorroeQ.rlary (W/Cao.Gal loop)
M z 1~ (SUp!3tonsalil) (wtaarllalloop)
cs" cor1ic:aI se~1
1
Fig"" 5-5 V"rI&brObaSll a, Merlogram (Ial."al v~)
NEUROSURGERY
5. NeuroNldiology
P OSTER IOR CIRCULATION
P OSTERIOR CERE8R.AL ART ERY ( p eA)
See
"'iSLl~ ~.~,
P OSTERIOR FOSSA VENOUS ANATOMY
g~al
cerebral YeI'1 (Galen)
1X~1 t41rebel~r ' .
- - - SI.p!ior pelrosai $inus
anterior mec1ul\ary y.
pelrosal"m
VM of I/le !a1~raI ..cess oj lhe 4lh ventricle
5.4.
Magnetic resonance imaging (MRI)
5.4.1.
General information
DEFINITIONS'
AbbrlWiations
..."
T!lble 5-.3 Range 01 acquisltloo dsl8
...,,, ""''''
"'"
.."TR
(la eSC)
(Ie ~ IKI)
(TfI< 1000)
prolo1 denslly
(TR~2OOO)
Of
"..,
SIlln denSIty
T , weighted image (T 1WIl
Short T, - high .igmll{brigbll. ~Anator:nic image", !OmeWhllll'l'H mbles CT. Shorter
ocquisi Lion timll than T2WI. ?roton nch tissue (e.g. H~O) hoslongT"
'The only objt(:\.S Urat appellr whiteon TIW1 are fat , melanin. lind subacute blood
(" 48 hnI old). Whitematter is higher signallha o grey motter (myeli n has _ high fat con·
tlmt). Most pathology is low signal on T1WI.
n.
5, Nosurorodiology
NEUROSURGERY
::::
::
T. weighte d im a ge ('T'l Wl )
("'"R T l - hiCh 8igns J /bright). -PAtholcciullmRle", Malt pIIth<>lovy .bow. UpRB
bilCk .l&r\i.I. in th.ldinr • .,rroun ding edema.
.."' ........
866) .... hi,h
S pin d e D9ity illUlKe
AKA bIIlAnced ima~, AKA prGlon denait)' i~p. Part"'"1 bttwun TlWI",nd
T2Wl, CSF. gr~y. app.ol<ill,)a~ly i.oodense with br.in (meM in whit.\! "\lH~rct.m)'.ti·
nating diseruoe).
FLAIR
Atrnnym for ~"Lu.id-Atl.l!nWl!.M lnve ..ion
~efY.
CSP appeaNI darlL MO'II I..icln.
Including" MS pla'luu. other wh ite matl.l!rle!liOOll. WrMn. edama, and acu\.e lnr.ret. apJM!or btillht. PetiVVltricular lesion. such as MS plaques becolllll! _
(UMlpicuou"
Ec bo tra in
{AKA rast spin echo (FSE»
tr il held COf'Ist.anl . I.e ia progreasively inenued utilizing ",ulliple echoes (8- 16)
r atber thlln 1. Image approawes T2WI but with lubsuintiaJly ndutad Iioeql.lisitiOtl IHne
(rat il brighter 00 FSE, whith m.y
~
I1!Ctilied by !'at IUpp~;C)n tKt\niqullll),
"GRASS" image
Aero",..., for ·C rad ..."t Recalled Acqu~ltion in a Steady 5111W", A · fast" T2W I uti·
pan.ial flip a~Je. CRASS;5 a GE lnIMIDark. othy manuradunI!n uSl!! dUfe"'"t
nlme5 . a.1I FlSP. CS~ appelll"ll "'hit.. bone ill billdl.. lind nowmg vese" lire ",hil4.1'yp;CIII Kq\Ii"t;ot\ dar..: Til ,. 22. TE • 11, Mille 8", UHd e.g. in ca ..... ical MRI to pcoduc.a
"ruyelogr8pllic" lmlge, imp ....u
ability to deli ...... te bony ~Ur1l.
~STlR~ image
Acronym ro.- "ihon. tau ;nven""., ....:overY'. Swnmate! T, '" T f ! 'gnala. CaLlIIeII rat
to drop out (lOnIeti"," II-acall~ ra~ l upp rftOlloo imIIgel. , 11(1"" gadoliniu m enhance·
rtlent 1.0 Ihow up belter in .~.. orfal. UtoefuJ primarily in spine and ...-bit..
H~inlla
MR" .
C O NT RAlNDtCATIONS TO MRI
P repaDcy aDd MlU, Dunng the lirat l rimuter. MRI can Clute rubtorption of prod·
.. UI orcon~pUon (..uK.mlte). Thera.A. no " udin to deta rmina thalOf\i tann efJeclli
ofMRI On a fet .... al'ler the firlll.nmester {the low ri,kofMRI in this,ilu8lion II problbly
pl1'(... bLe 1.0 the knowo dan~rI orion;lin& rMfiRlion of.·ny.{including CTl"~ eadolin·
;wn eonlnll it ronlrW~tad dun",.U oIprflT\,nc.l', and lit not IPpt(lVed for u"" in
*II < 2 ye.n. SntNl·fftdinl mut' be inlem.l p\.Od for2 dly, after adminisuation of Ka·
do!in;u," to the molbar.
NEUROSURGERY
5 Nlutor.diolorr
'"
Cont.nindieutioM to MRI!
l . cardiae pacemaker, implanled neuro.ot;mulaL<!l"8, """h lea. im],lllntt: may U"IOI!
~m pol'llry or pennammt malfunction
2. ferromagneti" lIoeuryam clips (Ut II....""' ); .r;ome «!nt!'rllucl uOe all patients with
aDY typo! o(aneuTY"m clip
3. meUl11ie implants OT foreign bodies with large compooentofiron or cotxllt (may
move;n field, mlly heat up)
4. metal1lt fragments within the eye
5. placement of a v~la r otent, coil or fll t.er witliin the pau 6 week:!
6. sh ra pnel; BB', (tome bullets are OK)
1. reJlIliv~ oontrawdicatioua:
A. da"atrophllbic pBtieDI.S: may b., abl~ to sedat.> adequately to perfoftU nud)'
B. rntically ill patH'!nt.s: ability to monir.o. And BOO!!811 to pllit.nl are impaired.
SpeciaUy designed non.magnetit ventilator may be reqIlLN!d. Cannot Ill;(!
m<lH brands ofele<:tl'Onic fY pumf"l/regulatoMl
C. obeae patient.l: may I\Qt 1,llyaieali), fil inUl many do$O!d bon! MRI acanoe .....
Open bore .canners IIlay circumvent thil but mallY util !>.e lo ..... er lield
st~n gr.h ma~eL!! and prod"",e inferior '1uality ilD~ge, in llL1';;e p~t;&l U!
D. metal irnplanU! in the region of,nl4!re&t (or IlrevioUB Burgery with high
~petd drills ..... h,ch may leave meUlI nJin~J: may produre 5u!Ceptibility ,,tlfact which can distort the image in thaI area
ANEVRYSM CLIPS AND MRI
MRI conaider~tJol\I in patients ...·ith a
cerebral aneu,),,,n, clip'
Tabla 5-4 Magnallc remnance 01 ane urys m
cli p'"
I . the d/lnger oCthe MRllllilgt1et.ic: field </luring the "lIeUl:Yitt>
clip to be pulled or torqutd off
of the anellr)'Sffi or to tear the
..,k
.rlifBC~ produ~ed by the
metal or the dip in the magnetic litld
3, beatgen.era~ ill the regioo of
the di p: not elinicRlly . ;gni»cant
2. the
Th" moTe fel't\lmagt11ltlc the dip,
the IlLI'gu lhf rorce exerUld on it by
thema(!llelic lield and the gre~ter the
image di.lltortion near the dip.
Sta inless ateel (55) i. da&Sifi~d
PH m arteDBWe (ferromagnetic) Or
IIUJltenitic lnon·rerromagnetk). CO)balt.-baSl'dJluperall(>yl lUe ru)Il·felTOm~gnetie and include ElgilllY (Sugit.a dipl), Phynox (Yesargil), and \·ari-Angle
(M cfadden!.
Tobl~ 5·4 ahow. thenUlgnetic ~mnall<:i! ofvariou$ dip. which it .... lelfd totheir lerNI.uagl1uic- proptrtiell, If in daub!. al the. time ofBMurysm lurg"I'Y, apply the following
si mple test: nllo·ferTOrnHgnetk dipll canno~ be lifted Qr dragged with II 5II1.II11 magr>f'L.
H EMOR RHAGE ON MRI
One of the JtI09t c:ompjea: lll!lioll.ll to interpret on MRI . Su p~ 8ti6.
5.4.2.
Diffusion-weighted imaging (OWl) and
perfusion-imaging (PWI)
O.inin8 usa8e in ischelnic brain disease (80me MRI machinu da not )'et have the
n\!CUllary Vadien" fordiffuaion weightin8 or the apeed needed for both DWI and pv.'Ij.
Dil'fusinn _w eigh ted imaging:. DWI illen.itive to random Brownian motion Ofw814!r
molocule&, and an apparent diffusion roeffident (ADC) iA detennined for each areD based
OJ'
5. Neuror$diology
N~UROSURGERY
.n. number olvtrilblH {lime. I ll ..... unent.aliofl ... )".
f'nety dlffuJin, w l~r (~.I. ill CSf) appta1$ dark on OWl. Areas of acute brain is~h.mia show up as lncnaRd algnallnll'! ... ity on DWI .. ithin m' nu~" I', DWI mlly also
be able 10 dLstinguisli (')'totQllic from vBI5O~nit .,d em o"· " (_pagt 85), HI)W~"~r. racton
o!.her lhan (Ot,1 i~~mi .. (.'1'. ,lobaL ischelllip, hypogly..... mi •• ltat\!5 epitepUcul ••. ) eat!
produ<:e AOC decline lod 1.1>. OWl ;nlllgel rmllt therefore be interprtr.N in relalion to
the dink.] -"lllin," . Some. bul nOlllll ", TIA .... ~iat.ed with abnonnalltiH on OWl .
Oill'usion deftc\5 do not indkate irreveriibleirUury. bul imueates till$ue that ill !\ear cell
dutll.
PerfW!;oo imuIPIll' P:o~idf!l infonnation rel.ted !.o the ""rful;"" '\.8LUI orthe microcirculation The ... are sewrll rnethod.eurrendy In u~e ...,th the bolUJI-<:llnlr1lnapPrtlach
he; ... , t.he mo. t widely employed" , Ultrafangradient ima,in, UI u~ 10 foll_ the gradw.1 rtductllm loG nor m.1 fol1!IWin. Administration Of COn1rh1 (u!I.1II Lly •• dolinium), A .i~­
nlll .... uhoOul CUf'I. is der.voo lind is compAred loG eonlrast In III lI.ury .
V ••
In theQry. OW l nnd PWI maybeeomblntd I<lloeate .~ ofperfl'Sion deficit 0fI PWl
th. t e:<cl!4lds the lOns of diffusion defICit on DWI, I.hu. idmtlfyin. . .Ivageable brainti...
sue ..1 rislr. of iufol"Ct;on ("pI:llumbn", Ht polJ' 806) •.•• III sereen for pounti.1 candj·
daU!1l for thrombolytic \.herapy"
5.4.3.
Magnetic resonance spectroscopy (M RS)
Thi • .e.:tioll . pec'f"ally
COVerS protan (H'J MRS .... hith
~all be performed on .. lmostony
MRI Kallller (eaped .. lI)" unita
., 1,5 1') ",im the appmprist.e
INlnwllrll. Specl.ro6oopy ofo\.her
Dude, (e .•. ph08phorou~) t.o be
ev.lu.u.d only with s peci.lirec!
eQuipmenL
T,bI.5·5 I
MRS
SINGLE VOXEL MRS
A • ..,.11 aR:1I is sel!'Cted 00
lhe '1l:OU1" MlU and the apeclrOfiCOpi<:. pe.... for that ~o . ...
displayed in reltOnaOU as, fWlCt.i0Sl orparl4-per 'lQiUio~ ( ppm l,
Therd"o .... may be .u~ 10
IIImplill' emir.
CUnielllly importllnt dwt·
.cwn.tic pew uti d.hM.t<Id
in TohJe 6·5.
lUusr~nvE
PATTERNS
Norma l brain; SH PI'IP''' 5 .1.
T\uuor: SuF.,ure5-7. 1 NAA .
C<'- _ _ _ _ _ ,.11actal.e, f li pId, f choh ne(ruJ.
of thumb: WIth ,lloma., the
lUther the choline, W hi. t - the rr-ck up to vade 3, thereal'..er nKfQIIUl reduce!! Ria.
Ii"" choline Ievels."d U..lipid peak rull,. be ut iliwdJ.
CVA: , lactate pe.k pn!domina\.el . Cholwe i, characllriuiclIlIy law.
Abaoceu" : Reduced NAA , Cr &: dloliroe peaka, and ",typic.l .,..aka" {$\I~nate, acetat.e.. .. 1 from bKtenal.ynthna il pathopomonic ror .b.ctu Inot always prellentJ. LacUI.e may to. elev.ted
M o11tip le .cl!!"",;,: Bland pattern. NAA _llghtly reduced. Lactate and lipId _lightly fltvato-d . Choline oot el .... sLed.
NEUROSURGERY
POSSIBLE USES OF MRS
I. differentia tin, .b_n from l'leoplll8m
2. poIt-op enh~nceD\ent va. reculTe nce of tumor
3. di.tingui,hinr tumor from M5 plaque.: occuioDaUy c.annot be differen tiated
• . in AIDS: may bt: able t.(I help differentiate toxo from lymphoma from PML(PM L:
I NAA, no . ignifie.nt illerene in choline, ladate or lipid)
5. !.he promie. ofd lfferentialinr tumor infiltration froID edema hll not been bonw
,"
6 . loroe utility in distinl{Uiahing tumor from ndi.tion MCfOllia (SH ~ 535)
"
"
•
"
•
."
-'"
~
OJ> 15 U
U
U
... ' 0 01 00
(A) NORMAl SRAIN
Figure 5-7 PrC>lOn MRSoI {A) nonnaI brain, ""II (6) high Ii''''''' glioma
MULTI-VOKEL MRS
Colorroded KIn with &eleded overlay for NAA, eholine .. [email protected]\>«
risk ofumpling error.
5.5.
Plain films
5.5.1.
Skull films
Tabla s.6 Norrtull d imension. 01
. he aellll iurcica ( _ Pl9ure 5-8)
~
S ElLA TURCICA
o {depIhj {mm)
NORMAL AOULT DIMENSIONS ON SKULL X-RAY
Teehniqua: t",. late.. L, 91 em u.r~1.O lilm
Max
Min
" •5
"
An
10.6
d.istan«, centnl AY 2.5 COl anterior IDd 1.9 tD1
lu penor 10 EAr.!. See FiI"'" 6 ·8 for mUSlTation oflbe diroentiont. and Tob/.~ 6·6 for nOr·
ma l vIlu ...
Deptb (0 ): defined .. Ihe gn!atel~ mua urement from Iloor IG diaphraama seliH.
Lenrth (L) : defined a. !.he gn!att.t AP diameter.
ABNoRIML FINDINGS
Pituitary adenoma. tend 1.0 enl'rfl:e lb. sella, in «Intnost 1.0 ~ ..niopha.ryngiomu
whkh erode th. posterior clinoidt.. Empty ..lIa .yndrome tendll to bIolioon the sella . ymmetrically. and "so ~ noterode the clinoid..
1)8
5. Neuronod)oloty
NEUROSURGERY
al50
",f' ahspell seUa 8U.tiM'- opti~ nuve glioma. It o;an
tongenitally In H urler·.$aynlirom<! (a mllCO-
oco;,W"
polysaccharidosis).
MISCELLANEOUS
Water's view: x-l1I.y tube ungled up.~S· lperpendiculli r to divusl . AKA submental verteK view.
1'91"01 '5 'tiel" ; K· ray tube angled down 45' . 1.1) vie .....
occipo,a.
BASILAR IMPRESSION
~ure 5-8 M.nu,emaOl5 01
Several conditiol15 whose nomu are often (eNtlnem. sella IU'dca (lalora! view)
OUllty) uged Interchangeab!y(eKact defirutionsara nOI en·
tirelyagreed upon for all oCthe!;l!);
1. plnlyb8.llla, abcol"Ulal bll6ilar angle. OCHllle mOldkal i.:llporta,,~ (usO!"d in an·
thropological dalal. May Cr may nOI btl s!i/!oci Med with basilar !mp~8!l ion
2. baallar ;mp", " ioZl (B1): UP"'lI.rd di&placeme nt offo ra men magnum IlIl1rglrur
(i nc ludiog ocdpit(ll bon. l and urviclil ,pine lineluding :Jdo[ll.Qjd process) inlo Pfossa. Some use thi s term for upward di Splacement of dens only. May be selm in:
A. tonpn"ital condilions (BI is !.he mon tommon congenilal anomaly of lhe
crani<lce.rvi.cal jundion. it ii" often aceomp.&nied by other 9.nOfl.lalles'·I.'-1
L
Down'. !\)'ndrome
2. KlipPl'I·F"il ~yndrome ]stt pGSe 119)
3 . Cbiari malfoMUation (.n fHlC~ 1M)
4. ayringomyeHa
B. acquired conditions
I.
3.
rhe umlll.oid ar1.hriti5 (in p.&r1. due do 'nccmp.elence oftransve .... e ligsmenL..aee Brullar imprtuwn in rh eUtllOlOid orlhrilU. page 339)
2 . ~t-:raumlltie
basilar invaginAtion , AKA c r anlalseUli nl:: upward indentation of5kull b!W!
usuallY due 1.0 a~uired IIOftenmg or bone. often allllodat.e<l with atlanto-ottip ital
fU$ion. Soma consider this synonymous with BI. Seen in":
A. Paget's dlseDse
B. o$teogeneliis imperfecta
C. osteomala<!ill
D, rickets
E.
hype.tpan~idlsm
Same IO"asu remenl.& of ...... (rerer to FiG" '"" 5.10, page 141, and Figu,",,5·9 below/:
I. Mc Rae's line ("MeR" in FiellrY. 5· /0): drown acTOlls rammeD magnum ttip of clivus (buion) loopist!Uon )'". Should 00 :> 19 mill ( avera~ : 35). No part of odontoid
should be SOOv t !.hisl'ne (th e /DOIIt sccumta fo~
2. C hnmber laLn·.lin e ("CL"
in Figurt ';· 10)" : posterior
hard pailite \.(I p05terior margill offonmeo lIIagown
lop;&thlon,. l.cno Ilio n 3 mm
or half ofdena should be
above thill line, ..ith 6 mm
being definitelY p,uhologit.
Seldom UKild be.cau8e
opi sthion i' ofu!n hard to we
on plain film IIna mayaJso be
invaginAted )
3. McCre£or'. bilKli.,,,
Flgu", 5-8 AP Yiew ih,ough ",al'k>cervk:al lul"lCtion'
(~MtG·ln FisurI5·/0"f"': POi'
FOOL ", FISd"IgOId'. divUlric line. F~L ~ FiScilgOld "
tenor margin of hard palate
_.~ line, " ~ , .)CIaI 0Wft>a/!g '" C1 CIt> C2 (SI!'
to most CAudal poinl ofoo_oi~PIIIl·7Zl)
ciput. No more thaI> ~ . 5 m.m
ofdeDll shOuld be above thia
4 . Wac k e.,belm'8 e livu8-<:a.
nalline t·WCCL· in FicUNl5.10): tha odontoid ahould be tangential to Or below
the line that utends the coune of the cliy us (the clivus baseline). lftbe divus.is
ao
NEUROSURGERY
5. Neurondiology
'"
colICa"" or OI)nVU, this loNI!lin" ~ dr,wn to C(I"n""t tlte basion ttllhfl ba~e or~bll
poIItarior clin<lida on t.h clivu,"
6. (Fl..,hi<lld '",) dlgllat rlf! 1I0fl(~YOGL"in F;'un6·9):joins dipstncnolches. The
nann.1 duta~ from thlil liM ttl the midd Ie of the atlanto-occipital jerint Is 10 mm
tdet;rened In 81)". N<I put <lroxlont<lid should be libov, thislwe. More accuraUl
than the !timutoid linll {FBML
6. .' i ll(:b gold'. bimutul d l ine ("YBML" in Figl<1"r 5·9): join8 ti;. or ", ..tQid pn)ceiISH. The odontoid up ."erllillll 2 rrun above thifi lirll! (rsnge: 3 mm IM!l0w to 10
mm llbove) lind thi,litle .I>ould trots th,lIlhUlt(l-oteipit.lj<li..1
5.5.2.
Lumbosacral (LS) spine
LA-5 i, nonnllily the lumbllo. disc ,pace with thlllf1!lIlOSt "frttul height . Abo_
.,.g,
N(>J'mlJ/ LS .plM '"~twu"""",,,",
327.
AP view: 1000k fur defact Qr non visualhlllion Ofthf ·Qwl'. IYes" " 'hkh i. dUil to peeli.
c\e.erollion wlUch may oecur .. Ith lytic tumo •• (rommon with metutau( dl.waseJ.
Oblique villw" look for diarontlnuity in n""k of"Srott)' dot" ror dero!(:l in J>WlI i"!.eran;eularia.
5.5.3.
C..splne
NORMAL FlN OINGS
For radlolftlPhitllignl afO! ..... itlll ~pine trauma , _ Tablr 25.1, Plllf 706. and
guidelintl" ror diagn~Jnr dinical h1/;tability,.see Table 25·11, pIIgc 13• .
ro..
CONTOUR LINES
On a lall1ral c.:.pine "·.Ili> tl>o. ... an!" ronl.Our lin ... (AKA arcu.!.e liOQ). Non..aU),
f8C"h should ronn II smooth, pMle "" .....e UN FiIlUrl5·10);
I . po6terior mIlrIPna.llin. (PML) ; _10113 poIIUrio. Cl)n~ lunace. or" ....I~b ....1 \.Jod.
jllll (VB). Marks the uteriOf' llIargin or'pinal eanal
2. a"!.eriOl" margiruolline (.4.' 1L): alonr anterior cortical surfac:ee of VB,
3. "Pi nQI. ",;n ll . lin ", (SU,: along base ohpinou s proalS ...L Tb. pIIII!.erior ",argin
of the . pinal eMal
4. pclllLerior spinal.ll line {PSW: akmr lips or s pinaul pro<:I!Io5N
R~I..A TION OF A 1l.AS TO OCCIPUT
See~
119 lOr erikrill for atlantoaaial di,IOCllu..n.
REl..AT1ON OF AnAS roAXIS
Atl an to-d llDtal i n terval (.ADO
'!be ADI il the d~tal>Ol! between the aot.e.rior margin of the dens and the clO6e!l1
pOin~ "rtheantemr arch orel ("Cl bUlton"lon alatval G-spine " .... ), Ute Figurl5·10).
The normal mPill1ll1 ADI uvanoullly
in the ran~ 01'2 to .. mmll.". Commooly a~·
c:ept.ed upPf'r IiJ;a.ita ItA! show .. in Tabi~ 5·1.
Atl . .. IoUi..... u bh.... lioo IAAS): Two POK;brlitiee:
Tabte S-7 Normal
I. AD I :> norma l' may Qtt.\I.I" ... itb inmmpewnc:eorthemns~e. . li"PlenL (Ammon in rheumatoid arthritis /.Ite
AOI
P"lII! 3381. may llao roUow uaumal_ ptl6C 722)
, ....."
2 normal ADI ' i .. tb_ prllHTlUQfan odontoid rractura ""
/X'R' 721)
.,~
"'V" . b .pe<t p N>-CIen a . pa«~l: Wideninrofthe upper speQ be,. 2.5....,
tween the"n~r arch orCland IheodOfttoid feen o n tau .. r C·
. pine nulon ,,·11Iy. ll i, not bown ,(this inc:re1lHd nlObi lit)'''''prftIIntaalonpuon or lWty oCt.he \r8M~elV Ileam""t andlor the
ISyt,)
"'' ' eI!
,
.
.".......
""'"
poII.terior lia'~tou' ~p,"
"'.
S. Neul'OT'adlolop
-- ..c,.
NEUROSURGERY
WCCL
,
..
AD'
KEY
(see
te~
fo,ootalts)
ACI" aUaNG-deolaI interval
MeA " McFUe's ~ne
MeG " t.lcGrego~s line
CL",Chambeilain'S Une
WCCL ~ Wackenhe!m's cf'NUScanalw
fl.gu r. 5-10 Sponul contour 1InII$ IIOI'l linus vsed 10 dilqlOSl'l basilar lIw ~glr>Bllon
ult." ';ow I"""-'!I~ C>'~ jun<:IIorl
CANAL DIAMETER
Normal canal d'amew. 00 laternl Capine x-.ay (from spinulBlllinar line (SLL) to
pullte rior ""neb.nl b".!.y with 6 foot wbe to mill dJstance)A: 17 '"' I!I onm, In lIIe p~noe
of osteophytic IpW'8, ~BS\Jre from the back of the Spur to tbe SLL.
Cervic al s pinal stenosia: varioul cutoffs for !.he normal minimum AP d iameter
h,,·. been 8ugge!t.ed1;l. On a plain lateral C-a piM ,....,.y tbio i$UliualJy measured from the
posterior vertebral body (or !.he posterior aspect of an o~t.eoph..vteJ to the spinolaminar
line. Some ull<! 15 mlll_Maet agree that ILen08l.$is p rnsen~ when lhe At' diameter 1$ .. 12
m.m in an adu l ~ (,UPfJ8~ 3U ror ool"Tf!lMion with myelopathy).
PREVERTEBIW.. SOFT TISSUE
Abnonnnily increased preV1!nebral
tissue (PVST) on late.al C_spine xr>IY may inditllte t.he preseuce ora verte-
1 0ft.
Teble W
NOm"lal preverlebral ,oft Ilssue
bral fractW"e, d islocation, or ligamentou l
,,
dis ruption". NonuaJ values are shown in
Tobie 5-8. NB : the IU!Ilsitivity ofth.esJe
measurement'! ie only ~ 60% a~ C8 and
5% aLC6" . Increased PVST i . more like·
ly with anterior than posterior injwie5" .
FaJae pD.itivllS may (Je(ur with bessl
skulVfaci al fr8~tUrl!'B, e~peciaJly with
NEUROSURGERY
.5. Naurorad iology
'"
rTliclure of the pterygOid
pI9te~ ,
INTERSPINOUS DISTANCES
C·~pine AP: a fractl,lUldi,tacation or [jgarnent d1i!ruption ","y be diagnDSe<i ifth~ inteNlpinou~ d'5tAnta is 1.5 l in'eII lh"lal both "djaunt levels (I'lle""u,...d from «,n1£' of
spinous pr~ l"", Aleo look for II mallllignment afspinoWi PI'D'I'I'$!Its below" certain
level which may be evidence ofrot.auan due to a unilAter1lOl1y locked fa .,.t .
C-sp'n e lateral: look for "fanni ng'" or -n aring'" which ~ lin "bnotma] lipread of one
p~iT of "p'nous pl"OCt'lSoOel that may alao iodicate ligllmenl disruption.
PEOI ATRIC C-SPINE
C1 (ATlAS)(8e<! F;' ..,e5- /1 )
Ossi fication centers": usually 3
I. 1 (&ometi mes2) far body (001 osr;.;lied lit \:Iirth, OPI"lar8 on x_'"Y during tit yr)
2. I far each neu ra l sTeh (appea r hil"tel1lll,. ~ 7th fetal week)
SynckoncU1lseal1 :
5ynchondro!JilI of tile ~pinou. PI"(I_
ce!&: fUSES by ~ 3 )'TS age
2 nl!!'l"Od!ntrnlllyndlOndro~",, : ruse
by ~ age 7 Yl1I
synchondrosis: of
sillflDUS Pfocess
F'1Iuf6S-11
C2 (All iS) C,.,e FIB"'" 6-12)
4 primlll)' naificat;on cenlers:
odootoid P"""""
ve.whr,,] body
2 nE:uml arches
A ReCOndlll}' QSljl6cst,on oenlo!r 3pppaOl
at till! iummit of tile dens between 3-6 Y"". Iilld
fuse~ with dr.os by age 12"'.
Syncbondro!iEtl: aonnaJly fusa between 36yeal'l;orag~.
AP VIEW
....
~
neura
P~I "'ieC1
g-
[alias)
neurocenlra)
s ynchondrosis
.
"""
.
derllocen!rtll
syncnondrosls
~I
~
nau
I1eurocenlral
synchondrosis
FIou,. 5-1 2 pecillmlc C2 lllXls)
C3·7
Co!rvical bodies a.re normally wedge
shaped in pedi9t.ric populstlon (narrower anteriorly). Wedging decrealu with oee.
5.6.
Myelography
L umbar myelogram
Using iohexol (Omnipaql.lO"!® 140 Or 180) /U showo in
Thbl~
5-1.
Cervi cal myelogra m with wate r w lubl e contril8't v ia LP
Use iohexo\ (Om.oipaque® 300 or 240) n sbown in Tobit 5-1_{moen spina! need(e
into lumbtar !ubaraehnoid Il'pace, tilt the bead o(th~ my~lllgr.Im ta1>le down with the pa_
tient', n~k extended and then inject dye. Ita conlplelectrrvical block i.'I5~n, bll\"e pa.
5. Neuroradiology
NEUROSURGERY
t'~Qt flex neoek. Irttle block ClilIlJOt betTue~d , patient may need Ct·2 p\lllc:tuJe (IT MRI
(firttobt.ain a CT ",hith may 8ho'" dye above theblock VtlltCWlnQ! be appreciated (In my.
eIOlT,phy . IQQe).
Poet myelQgra p hic. CT
u,errallY Iellsi tiY ily and l pe<lifidty of",yeloiTaphy (.u pagt 2951. U, cues "fcom.
plete block on myelQSTim, CT ",ill ontn , how dye.distal to the apparellllll.eofthe block.
5.7.
Bone scan
Te<:hnet.ium·99 ("-Ttl pertKhnetate ill radlolllOtope that IfIIJ' be attached to v_
io ... l ubst.r&te . r(lT use in bone .cllnninJ' It mllY be ueed to libel polyphOlphate(nttl,y
uled l«I.y), diphQlphonite" (MDP), OT HOP (the rnot~ "'Idely agtnlll~ cutn'nuy).
Bone ICIM ",ilh technetium·labeled compound. depend. 00 the p..sente of oateoblaillc
activity for thede~iUon of tracer into the bQol~
GIlIium may alao t;.e uSl'd 14 look fOT mort d]fllnitOlt.oo~hti •.
ApplleatioOi for bone 1C<l1ll indude:
1.
infewoo
A. O!1teolDyeli U-l orth•• kull Dr I pine (verubral OIItoo Dlyeliul, aN ptJI8 244')
B. dillCitis; 1ft pap 247
2. tumor
J\.. I pine nle\.8$t_=ut p~ flJS
B. primary bone lum ~ 01" the spi ne: _ P"P 6 12
C. 6kuU (uman: ~ fKlI/t f8Q
3. d;.\ot'QeI involvir.g aboormll bone metabol"m
A. PlIJlet"5 disease; ohhe ,kul! (1ft PQ6t 3·U ) or Ipine (1ft" ptVJe 3411
B. hyPerOiltosis frontalis interna: ~ ~ 483
... craniosynOl!-tQsu; ut Pfl#. 99
5. r.. tturn; spille lsu P<>I{t 701 ) or I kull
6. ·10'" back problema~: to help id~ufy ... me Dr Lhe above esamplel (.... p<J8t 2!U)
5.8.
References
R,
...._
£.Honl;I_
Io4 .W
.." eK ....... _
_
orionc _
_
;,,",~
"""ond_,....... .....
I.
.
pIof. C_ ..
IiDu.
,.. ........ ~,p<]"16 0I)·,. 19U.
8aI"OI Ii P. R,a L. Soijof.... J<IId 1L _ _
••,iMII<nI _oI"""" ...."..
noocI;.,.,.~
P'O(ICftIt. """ -... ....1_ J "" ........... lO.
'If>.ll . lm_
I I.
__
Il
_
"""
_~
.....1<oUot: 1U<1io.- ....
,.. _ _ .... .-.joI
... )I 1"
U.
,..u~JM
,.
4.
A~ . . ."'"
.......,r.,.,...,""•.
..
Ij.
"""1OOo T H.,", OG. "odI.., ~ .. ....
.C. y Mo!.llr.s-. ....... IVII
,hU_ .... "
10
~
9,
10.
_""tl1 "",,,,,, . loe. . SoII~.C. , . UUI\..
!IOOl: p"S6.
8010"".. .. 11. .......... s. 04."";' _
. . ..
.".,f'Irto ........ ,...) ,.. £ot:l J 101.,. m
''''
_ _"
NEUROSURGERY
"" H. 8 _ _ FS.S<hod<o pw, ...... 1'Il*riao
_ __
$t_ ' W. ' _ f .s.Gctoo.ok>R G. .. ",~
.......
....... ,.....,. ..... "".
o..m-._1pI<Id ......... ~..." ...,...,."
~
S" ohlS. 1011·5. 1')97
"'t ll. a - FS. _ _ C . .. .,t _ l l l If·
"""""_;pit<I MR llioh.. _!;kc<ld1t, ...
-....,. U. l l ~ , 199\1
M..... M,. . T~OC. IIo.o.d ;. .C. ....... E_;.".
01 oori)'
tv "'A ,I><np)" ....... diflII ·
top-""""'_
_"""puf"'_""~ MIII ~""oIOc!" n:
17
1792..... 1999
_otn
_ _ ., _ _ .._ .. _
M .........,..' I, _""A."loMol .......
m.·_
,_
_16,
0II_1oI . \.JlOOC$<"~8 •• , ... ~
_ _ ,i_os
.... _....,.,.<bpl: M_ " ,
1<001-..11
1l69·76. 1991.
_IIF.Fe",..G .s...wt.." ...... ~ OompIka­
IId_ ll F.e:;-..LLs.:_O f ... ., "
.. _
.. MIII,.... _ _ ...
..
sa..l1od
_ ....Froe:;·
.. _
s..''''''''''}·115-M.
___ I__
ItIllIt , ...
I\I\19.
UOi"'.<lfd~~~I. I'I....-.:r S ' ·
II
50""'. II ""·I(M)oI. 1"1
..... of.-bnl ...
d .. _
...... ofl"l>k. AJ. loOl. W·'J, I ....
1731)..6 .
......""'pIIoI.podI~ """"""-....~~:
W.'.'''1
Dooo I£ .G_p c: r ... "" . ..... o..uc.l_
ron...... ~~,
~ ): ·
PndIon1IW. G _ RI. "" ... _ Iot:~
_01 101111 . _ N.... '*'CJ 3l 11)l-6. I99'i
plOJo "Jl'IR U; IJ I)"9.1M"1
u..... 6C, IImtCC. T",-\. e.•, .." ,..,._.
f".."..IoI.AIt>«>GW· ...", _ _ of<llf_
potf..... _ ...- I < _ •..--"'O<II1ot ...
It
R<pOn"'lW<I_ . J~"""".lIIi
10/1·
1). 1997.
"""'k VC.KopI.>MCE. M............. ..,".... I. .
JII_I&fto<IlJl.o..
.u.... T ..... N.... MH .. 9ol)'JI. l'9M.
_1_,.,oI,,""'_."' ..
S. Neurorlldiotogy
".
M""", K A E.. ••• 6<"" ~ ""'()T , L")fi"J (jI W. ..
0;,10<", ... or.". """ltal .,.... w '", oot<I 00 ...
ttI ~
l. fI'c1, ... O>i<I", ~ ,,'h J _
4M:.fO. 1 '7I~
p<n>I<oo
)611'
~
......... II. MoIltt ,., O,I(nt]O<7I1.S.".,J , Tt.. _,~
•• "'fIOI .. ' .... o._ip, .. , Gi.lon"" •. :-...' -. .."
~,
"
"
"
':4.
JOI.' S.....
12_1,19'19
1Ioh,., s P. K,k," M O. M.oIIi.
...... ~ SIo: ..... , Rod,IoIl • .
W 'Y ' >I\lpc.j!>'l"
"
..
,
~
111-l>.lqsS.
ScI... od< k H tI, S" ... W H. (0.1>.). Op. ... ~ ........
....~rrI ..,l«h"'q_ 1...".G" ",, ~S"a"." .
W .. Yort , lqll
£1""'" "', ......;.1 ",800,_ y . .. .!.. T_·
it III)'< ..... OIIy io po"........,," ....... , ~ ""..,.
,'" wi.,."., f_"", ,,,d,_,,,o' ""<""",,or
dl.,.-. . .............. , >ad _ i s. S.."""
I'm)
0.:_ 1( , I{;,.-.:' C li1i1j" '" p<n'<fI<:bnI""", " ..
...................... "",,,,,f,,,,,,,.i<oou ... 1II> .,.,.. ••
W ..... "'j"') ". ~[ ....... M... 2. · ,11,.2.
""-!IIi.
".
"
"
"
"
111 .1 ... 1( A. FI .... ~ D.1'I"' '''cC!<:>I oof, ,......
, ...I~ .. . _1\11.1 •• '" I";""'of ... , ..... oa/ 'P<"'~
I I\I~'} 19' iTJ·9. 19II1.
N';"i<!o.J 8 . "'i<I~hT P.GorMn C. " ... ~ n.. .. III·
""d,""'~dw...c.."..,.{...""of ..""...
bdloiolp' Ill: I iJ-<o. 1977.
1I1l..,. D,.;,The_" .,....;...,I.¢n< ",.,fMaMII
~,,'"' 0;....,.'100 .
6, Nellroradiology
"
n.
"
"
"
<ltildn!tl. Rodi"""", W. 1 Iz.. •• It11.
The Cet>onl S,""" I! _ _ ~ S.. OC1Y.'<G,j 'no .....
" ... .,._''' .... , 1 8. L~.""il>OOlpIo; • .
IWl.
J~
G, 81«k..- H H; P.......,........... _of ....
.... IIIc:b.i~ . .. "' JII..... '~
.. DL
>OW
,., <~
Th<~ lnir"
n . 1z..3\,
__ .f.b_I".... ft ..
«n-kol ",' r><, ""II 70. 'D~, IQro.
c..mben.,. VI E: 8 ..11. '"",,",,"'" I,p....,bbio):
eiwre "" ..1o;wnon.1I ...,.".IJ' o f _ip i ~ _
..... "~ r<U";,," >Pi""
aool ",..10.>4.
'"'''~'' lnlllo!
V.ld 81011>1«1 I I
0;"" ......u.a
.._ .
1~J9
M~JOf II Tho \o& ..
'11-%,
f..-_ 01"""" " 111''''' __
"'II,,,
of Ibo ,~.u in !lot dl'l""'"
, ..... . ,J MNkIIZ,
'" w ,l .. I..,!I<U·
17 ' -3 1.1900'.
VoaGWu J C. 101 . ... ... " Il .DDI.. I( 0: lfadloloJJy
""~_m""..,_IN.I~.""'.I" TkrnnIeo. nob, .. ju ..""" &lid ... . _!nOIiIlol. F......
I'\ItIIW,i • •• foI ... . 19J1.CM!U' l! pp19-61
lI ... t VC. llopl:J"' C E,S. .... nS. I>iI""",l<m·
"')1 ofl)l>.I... .mp<e .. ;OII •. - . . , . 15:!19. 1961
II.ondo I, V............. I. Mo,; .. II... al ~ _T<-pd,..
~...,.,
99oooTc"",,.,.,.pIIo"" _
..1",~
t>Pl, ;" ...............1<&1 ptlaiI:< 500ra N.....all; lD1_
10 . 197• •
NEUROSUR.GERY
6.1.
Electroencephalogram (EEG)
Common EEG rhythms lIrf!shown in Tobit 6·/ . The
primary use ofEEG i~ in !.he diagnosis and n1DnBgemen~
ofseizur\'. diiordetll . Non-c:orlVuJ~ive use of BEG I, ellilcntiaUy limited to monitoOril1g for bun;~ 8upprullion <su~·
/OI"! (e.g. during C1lrotid endarteuctomy )o r for d ifferential
dingnOliis of diffu!'l! en~~phDlop.t.hy, Including:
1. differentiating psychogenic. unrespons;veneas from
orga ni~: a n'mnll) BEG indioate!! either psychiatric
unruponllivenu~ or locked-in 8yndrome
2. Mn_nvu!eive ~ tatU8 epHcpticus (seiJurea): R.b-
Ta ble 6-1 Common EEG
rt'IY1hml
sente or romplex partial sta tus
3. Bubclinkal focal abnormalities: espetially in patients too ill to be u-anBported 1.0
CT. Loo~ for e.g. PLEOs l.su ~Iocu), foclil slowing ..•
~ . specific pattern, diagnotltic for certain pathologil!'ll; e.g.:
A. periudic laterali?;ng e pileptiform dillChargeJ (PLF..D8): roay occur
.... ith any ac:ute focal cerebra l insult (e.g . herpes limple.: entephillitis
(R SE), lIbM:ell$, tu mor, emholieinfancl: .een in 85% of calleS of HSe: (on~t
2·5 d ane.. pf9Sentation), if bilat.et"sl i • • disgcll'ltie orHSe:
B. ."baeut.! adel"Ofting pDnen~ephalitil (SSPE) (paihognnmonie palt~m): penook b.lgh volUlge with 4·15 ~ IieparntiOll with Il«Ompanying body j{:riur,
no ~hange with psinfulatimulltion (differential djagnosia includes pcp
overdOlic)
C. Creutl{eldWakob diseAse b«J108f 227); myoclonjcj~rks. EEG ~ bila!.CrAI
ahArp Wave 1.1... 2 pe r iecond (~a rly - slowing; lal.l!r- triphMie). May ~
semble PLED •. but are reactive to p~lnrul Itimulation ImOtit PLED. au
not)
D. tripha.ie WAV"'" not r~ally sp""ific. MIIY beseen in he""tieentepbalnpnthy ,
post.-lInoxia, and hyponatreml9
5. obje-ctlve mea3ureofaeverity of encephalopathy ; u8ually used for anoxic enceph.
alopathy (e,g. periodic spike. with sei~uNS ind.katf! &<:;'" chance ornonnal neu _
rologic outcome , with high mortality), Nphll coml1. bunt auppresaion, and
electrDC(!rebral 1 ilente an all pOOr prognO'$ticatorl
6. differentiating h.ydrllnencephaly from severe bydrocepbll.1Ul ( _ Hy1ronf"",pll.
01.1', poge 180)
7. u a tUnical eonnrmator.l' test in the determinat ion of brain death (,sec pall~ 166)
BURST SUPPRESSION
I_Je<:tric intervals interrupted by bursts of a..~2 Hz e1~;rir.a1 activ ity tha~dimin·
iah to 1·4 H ~ prior to ~lectrical s;l~no;:l'.l . Often u~ed a8 an ~ndpoill t {or titrating fleu r(lprtr
teo:tivt drugs such as barbi turotes, etomidate... (e.g. IU page 807).
6.2.
Evoked potentials
Cli11 iCIIJ indica tiollll for !voked potential. (EPa).
1. di agcosu. : (MRI has largely replal.'ed EP. fnr these 3 indica tion,)
A. acoustic neurOma
B. "" bdinic:.a llesiolUl of multiple , dl!l"Ollill
C. brn ins!.Cro lesions
NeUROSURGERY
6. EJectrodiagnostia;
'"
2. ,nlra-operati ve U$oll bu ~Iow)
Table 6-2 Evoked pot ential waveforms
(nOle ' values may diller Irom lab 10 lab)
",."
''''
Possible- geMrtlou
M COChlear microphonic
.~"i~1 ~!\I'P5 P7
.<zl'V~2S" ,.It
I III!
II~' I V
P, cislalVllinerlll.
Pl Jlf(liltnal VIII or ooc:hIear I1\.1dOO$,
P, lower jIOI1I (1 superior olivary c0mplex).
P, mid·uwer pons.
Ps upperpoosO:- inleriorcolIiculus
IOmS
Nv (on frEp where E. ~ E.Ib"S poi01)
UESEP
~
C3'-FP---""-"" '"'
<
. ~~9_VP22 eart1 -
~f\-N~~
~
"" ~ 1"''-/
AKA EP: o:nIry 01 volley ..' 110 listal
braclial pieXIIS,
1'4" (on CvrFpz); roo! entry lone (cervical region),
N13 cerW;orneCulary~nc\loII.
N" prinarysensoryearlex,
P~ (early) motor earle.,
P~ (\al.) IPSP "reaction" to NIS
Fz-Ep
I
I II I I I
"mS
LE SEP
o.7.fPz ~ ~ r--.~
N2S-WN27 -:- I,U5uV
Cz.FPz
~
40
l5-TI2~
t
I
I
I
~12 (on ls·T,ll; luml»S¥;fal pIexvs,
POll (011 CrF.z); sensory COIle. (analogous 10 N18 i1 UE SEP, reYeIStld in
polarity !or ? reasorr),
Ng (on CvrFpz): ' doIsal column rlId~
N
t
I
~mS
..-
100 striale & pre·striale occipital C«tex.
wilh contr\bUlOnS !rom 1ha1amoixN'-
PAVER
INTRA-OPERATIVE EVOKED POTENTIALS
Also, ste p<JB<! 3 for anestbetic requi rements for inlraop.!rative SSEP monitoring.
EPs may be used for intra-operatiye monitoring (e.g. monitoring hearing during resection of acoustic neuroma$, or monitoring SSEPs during $Orne spine surgery). however,
thei r delayed npture onen mahs them ofJimited U1lefulncss in pyoiding aCUle inlrp·op.
eratiye injury. A 10% increased latencyofa major EPpeak , Or a drop in amplitude,. 50%
i$ significant and should cause the surgeon to 8..PCI1$ all variable. (retractoNl, instru·
ments .. J. lnlra ·operatiyeSSEPs may be used to localize primary senYlry corte~ in enestheti2ed patients (ao oppoBed:o using brein mapping te<:hniques in aweke patients) by
looking for phan J"I.!Venlol potentials acrou the central oukur:r'··.
EP monitoring during s pin e s urgery
SSEP 9: monitor only posterior column function. and while this correlates well with
...
6 . Ele(:uodiagnostics
NEUROSURGERY
o:>Verallaplnal tord funeliOn and ar~ a lTetted by manipulation or the .pinal cord and l~­
chemie ev~nt.l, they mal' r~in un~hanged with aome injuri" to the anterior cord,
~anscran;al m otor e voked potentillia (TCMEPa) : tran&a"anial electric .. l or
magnetic stimulat ion of O'\otor cortex and delcending motor 0::<0n8 with rerording ofmGtor pltentiuls from di8~1 ~pinal cord Or m.uscle group!! , OUl!. to thl!. large potentials, th e
acquisit ion tim" is shorter lin d feedback 10 the iurgeon ia almas! iruooediate. However ,
due to pa t ient m01li!ment from tho muscle contnlttion s. contim:oous recording: bI Uilually
not possible {except with mOn.ilOrinjl' the re1IponU over the spi nal !;Old ), U~ful for iu rgel')' iovolving the sp inal cord (tervlcal or thoracic), 110 utility filr lum bar spille surgery.
In addition to g:en~raJ EP anellthet.ic require",eolJi, n.mmmugcuhH blockade ,,,u8t mini_
n:>i~ to pennit a. 2 out of4 twitchel.
De-cending evoked potentieJ. (D£P): (form erly refelTed to by the misleotding
tern:> al oe uropnic molor eyok~ poten t ial,). Ros~al5ti!l\ula tion of w apina l corti wit.h
n<:ording ora caudal n~"rogenic response from thl! s pinall'OnI or peripheral nerve, IIr ..
rnyogeni~ r"l'lponse from a di1t.a1 mllKle. OEP. can be medial....:! primarily bl' IIIl1SOl')'
oervt'B IlIId the""fOJ"~ do not rep.....senl true motor poten lial.s. HQweV8, ;r.lwwn 10 be sensitive to s pi nlll cord chlL~gft5 and may be "...,ful wh"" TCMEPo cannot be obtained ,
ABBREVIATIONS
Abbre viationll1.l5ed below: BSAER .. brain ~tem " " di1Al1')' I!voked rO!b~: lJEILE
SF.P .. upperilowI!T ..xt .... l'Ility senso!)' evoked pot.ential: PR YER _ pe tte rn ""versal vi ·
Bual evoked response whi~h cequir"" patiP.ntcoop<!ration and visual attention as op posed
U) Ila.\h YER wh ich rna) even be done through d o....d eyelids. See aliO refe rellCf!ll'·· .
Table 6-3 Normal vulue, for evoked pOlenUals"
T~'
"'''
UESEP
LESEP
PR YER
(nole: values may dl Ne< trom lab to lab)
Pamnettfl lIINaumi -- Normal ¥8111tS --
"".
~2.511k1
Com~'
dey
I-Y pe.D: !alelq'
4.01 mS
H.pe3~ 1a1eflC,
l.\51!1S
4.63m
2.&61115
V nbsolote I~~
IH-V peaIIli!1erqo
S.1mS
6.27 m5
tfs·N'1 pealIlalMCY
9.38 m5
PuP. pe~ 1i1!!ocy
IS.62mS 2O.82mS
jlIOklrqaIion $U~ lesion belween pon$
inO coIicuII.G. oIkt" K_11e neu,oma
proklngallOn ~t:; Ie:siotI be~ IoMr
pons"& midbrain, may be seen irllo1.5
11.35111$
P.., absoMe lalerq
3720mS 44.16mS
P,oo absolule laWlCV
.3 S.D.
P,OO i!118'~)'e dfle,ence 6-10 mS
1~·eyeddll'l$'lOO is mom~"~hluil
field Slimulauon. Monocular delect so.ggesli
~ de!edif! Ul.loloplic oerve anlMor
to CIli~5m (e 0. M.S" g1i..eoma, ~pre$IOOI'Il8lifW cegeneralion). Bilale!i! de!ect
does nc)llocali.l:e.
••
IIOIm" ... Iues on _ _ ... cnliCl l "alUM
6.3.
u~
as eutaW I... aDnDImli _
Eleclromyography (EMG)
There lire two po.lrtionB 1.0 thl! EMG exam:
1. conduction lI1eI,,;Urements
2. o .. edle exam
A, ioserti01l1d actiVIty
B. activity at refit: IhouJd be I lle nl when need le Is
activity iuo3l1uieteoi
~talionary
a nd in :\Crtional
DEFINITIONS
Fibrillati on potenti"" a: following den~rvetion ofa
NEUROSURGERY
mu~rJe
6. E lectrodisgflostica
(""condnl')' La II n!!;TV"
'"
injury). individualm utcll llbe .... begin firing independently . .EarliHJ,()/\IIet 10 daY".
lOOIetime. up to 3·4 week.. after denervation. If tM nerve re<Xlye ..... it llIIIy reinnerva~
tM mu..:le. but with larger motor units N!. uiting in longer duration a nd de<:rea~ num·
bon.
F. .....,.: ~rve it . timulated. cauling or1hodromic and antidromic cond uction. Fwa"' l latency may be prolonged In rlldiculopathy (not IIIn.ili"'I).
SNAP: te nlOry nerve nction potentiall.
M YOTONIA
TheN! are . number of myot.onic condit.ion•• induding myotonic dystrophy. There i.
sustained con traction of the mu scle. Clnuic EMG IInding: ·di .... bomber" IOUnd due to
myoton ic ditcha rgu.
LUMBAR OISC OISEASE
Al.o .... pagt 292. SNAP may be normal ... the injury i. proiUmal to th. ~n body
which ruideli in the do ... al root ganglion (in the neuul foramen). Pa. upi nalmullclo! fl·
brillntiona mllY Ottu •.
Following disce<:tomy for udiculopathy:
motor poll'ntials retum fi ...t (if~rvl injury were · compl.te·, it would u.lle 1
month to return)
if lost. senlOry potenlial, retum lut or may not relum
paraspinal potentiftl. m.y no longerbeuseful because the muacll'tl are cut during
surgery
PlEXoPATHY
Reductioo of SNAP with DO paraspjDw. musele fibrillal io,,- (the donal ram i Gi t
proximally to innervate the paras pin. l•.• nd aN! involved ~ W with rootl..iorv).
MISCEt1.ANEOUS EMG PEARLS FOR NEUROSURGEONS
The short head orth e biceps femoril in the LE;I t~ Ii.... t muscle inner-lted by t~
po!rooeal division oftbe !(illic ne ..... e at or just above the poplil.e$l fOUl ju.t after the
aplil4l offfrom the sciatic ne ..... e. In cases e.g. offoot drop it is a good muscLe to
tesl to determine if there it a po!ro"",al neuropathy VI. a more proximal lesion (i.e.
above the plplit.eal fos •• ).
EMG ii not extll'JDf!'ly sensitive for radiculopathy te.g irritative radiculopathy m"ht
not be picked up). more !<) in the cervical region than in th.lumber region. However.
when positive , it i, very epecifi<:.
M ......
6.4.
References
o.-pnl_
H """_
...to ......
;' ......
'1'_
""IcIoI
_ I. M_.
~"",,,,"
8 1i" C D. (ed.l. o....t..ll u, ... _. New YOtt.
19":,. n}-ol).
'_af_'_ ..
1.
c;",toriEM.~S· Lo<"i ..
1.
J""'~"-"''''''''-''''''--''C-.
_'-'11 6, . lOO1·S<. ' 9I<
WooIM,C N.Enol _TC.O_ WE; Lo<aIiu-
148
,_ .. _ i r ' " - l ' ..... _ _ af-.-
6. ElectrodiagnOitiea
«tdnI_ ........"""bydot<a~af
. _ " " " " '.... M I I - . I .......... _ . J Nfto·
~51 ·C16-,.,..I 9'9.
a..-KH:E""'ocIp<t<ntiab .. ' liAocaI_
l r... af_ J*U) NI:IoiIIJM«I lO6: 11000-50.
""_K".£_"'..........<I-.._..
,~
int
1_",,_,...1 NE",IJMotI lO6: ' 21»·11.
'9$1.
NEUROSURGERY
'"
-"
---
..
~
-',
Also_ pag.153 for plumbi&m (lem! poilloninll frotn At.al ned bulLelli.
7 .1.
Ethanol
The acute and ch rOJ1ie errKU; of ethyl alcohol (e~h.nol , E tOU) ebuH on til, nervoua
.Yltemal1lprotean •• andarabeyondlhI8l:opIofth.i.te~t(nol.tolDl:ntion the Afl'ecb; of
EtOH QfI othar ol'la.o .ylteml). Nell1'(lmulC:war a fTKUllndude
l .cute in~""Uon: ' " ~IIIW
2. ~fTecUi of chronic. .leohol abu ae
A. We .... ;e..e·. e a e.<ph.lo p.lhy: IN ptlJ!t 151
n cerebellar degeneration: due to delL'eneratioo of PurkillJl! cells in th@cerebeUar (Orte •• pndominlUllL), ill th...nterior .uperior verm i.
C centl1ll pollllu,. my.linoJyai" _ page 17
D. llroke: incre..ed nair; of
I. Intra~,ebrl. 1 lI. marThaC': &« P"8f: 852
2. jac,h...ic slrok~
3. poaibly llMur'l'llDal SAH: &« paiJe 782
E. periphera l nevropat by: _ ~ 554
F. • ktLeUII myopathy
l . tlffCU of elcollol wilhdrawl l: u.u.aUy!letn LA hebituat.tod drinlten with cUilation
IIr r'l!duction Df eUw.hIIl intake
A. alcohol w;thdraw.l .yndromes; _ below
n. 1ot;2Url!$; up \(I33"ofpa~nt.r; h""" a generelize<l tonic_clonic !leilure 7·30
hn wr ceuatioo of drinking (!lftAlcolltJi w;lltdrowallliizul't~ . JllIII! 261)
c . delerium lamens (DTa): ue ~Iow
ACUTE INTO)(lCATlON
The primary elfKI ofElOH 0<1
the CNS 1& depresaioo of neuronal eaTa ble 7- ' Blood ethanol coI'ICantratlonr.
citabWty. impul5f! cond:.octioo •• Dd
(In noOoi' 1oo/1oIIc pa.lletl1I)
neu rolr.nlmittu releaH d.... I()ditlKl
(blood EtOKJ
CIInkll lIIlCl
elfecaon the cell memlW'ano!S . Tpble 7·
1 MI;MlI the clinical elflKlI .-0,,1«1
Ibm IIlIIOO,
....·ith Jpeocifie EtOH aHlcenll'1lUoos.
Mell.aby erred; the J~trilY of in.
pniqnlcion. ~
!!Iaication i. greater when blood.1eo,. 21.1
1feSIo"..-:I oerebt.... ~
hol leyelll al'<! .-i.ing th~n when ralline.
lion: ~ III's\.Igr!aII. ~.
In lI"Ionjuna<llcllon •• indiv idu.1a
~.1LlW
with blood elh.nolleveIJ. 21.7 rwnolII
,. totS
\ISWIlJ ,. . 110m '"""'tory C!ePlH
(tOO mgldl) are defined Allec.lly io·
I()xicated.....d II numbe~ ohutn h.ve
chenled thl. to AO maldL How ..... u.
eqn levw of 10.2 mmolll (47 mgldllllte.-u.t.ed with ItlClUted ri.kofinvol... ~ t in
mDtor vehicle lI«Idenl.l Chroni~ alcoholi.m leads to increalled I()lel'1lnctj in habituated
ind;viduals lurviv.1 with levI l, Rxc-.dinc 1000 '""til h .. beea reported.
.
...-, .,.
'.' "
".
..,
_1IIIOlI:RI:!an:
~
-
ALCOHOL WITHDRAWAL S'I' NDROME
Compen18lion for the CNS tllpraua nl elrecUI or EtOH aco::~ in mrooic alcoholi. m.
Coneequently, rebound CNS hyperactiv ity m.y rellull from f.mng EtOH level •• Clinical
!IIena of EtOH withdraw.I,,1I duaified .. mador o r minor Ithe devae 6r.tltonomic hyperKllvily lind the pr~noe(.bHnceorD"l'll difl'erenlilltel lh_ l, as well .. ,.,1)'(24_48
NEUROSURGERY
7 Neuro!OX.oology
'"
hrs) or late (> 48 hl'1l).
Signslsympt<lml include: tremuJousness, hyperreUeocia. insomnia. NN. autollomic
hyperactivity (t.a<:hycardia, s}'1It<llic HTN), agitation, myalgias, mild confusion. IfEtOH
withdrawal ~eizurel octur, they·wnd to be early (II!<' ~ 261). Percel/tual dioturbances
or frank h a llucinoais may al80 occu r early. HallucinO!lil consis~ of visual and/or auditory hallucinations with an otherwise clear sen!l(>riuUl (which distinguishes thi$ from the
hallucinations of D'l'sl. 0Ta cen occur 3·4 days after oossation of drinking (IU Ixlow).
Suppressed by benzodiuepines, resumption of drinking. Jl-adreoergic antagonists,
or ~.agonist8.
PREVEI"ITION OF ANO TREATI.AEI"IT FOR ALCOHOl. W/7HDRAWAl. SYNDROME'
Mild EtOH withdrawal io llIanag~ with a quiet, supportive environment, reorien·
tation and one·to-one contaet.lhymptoms progress, in$litut\! pharmacologic treatment.
BeozodiQzepineli
BenzodilUepines (DOls)
are the mainstay of treatment .
They reduoo autonomic hyper.
activity, and IDay prevent sejzure& and/or 0Ta. All BOZo are
effective. Initial dOles are
shown in Table 7·2 and are
higber than those used for
treating anxiety . Symptom triggered do~ing with repeated
evaluation utili~ing a standard·
iud protocol (e.g. CIWA-Ar")
may be mOre efficscious than
fixed ·dose ttchedules'. Avoid 1M
administration (erTatic absorption).
Table 7-2 BDZ doses lor EIOH withdraw sl·
.,
Adjuncti ve m e dica ti ons
Associated conditiolUl commo<IiIy as 8P1>1Q111'1ale b.l9O<I "" palienl _
monly see n in patienUl e"peri·
'lntiog alcohol withdrawal
BI"IOrI" n.lf·1i/e with 1 _ acllw rDWIt>QIilas
syndrome include dehydration,
fluid and electrolyte dislurbanc·
es, infection, pancreatiti$, and
alcoholic ketoacid"'is. and
sbouJd be treated accordingly .
Other medications lLSed for EtOH withdrawal it5elfioclude:
1. drugs useful for controlling HTN (ca ution : these agents should not be "sed alone
beceUlle they do not prevent pT<lgTe$IIion to mOre severe levels of withdrawal, and
they may roa~k symptoms of withdraw all
A. B-blockers: also !zeat most associated tochyarrbythmi 811
1. IIkru!l!!.l (Tenomtin®): reduces length of withdrawa l and BDZ requirement
2. • "void pn')r" "nolol (""ychotox;" rMctioo~)
B. a-agon>sta: do nOl use together with lI·blockers. Clonidine (SH JJOIe 5) has
been exteru.oively studied, and can be given in pat.ch fOrnl (takes _ 2 days)
2. p~enobarbital : an alwmative to BDZ.. Long acting, and help$ prophyl8.llagailut
se l ~ures
3.
badofen: a Smallsludy' fouod 10 mg PO q d X 30daya resulted in rapid reductioo
of sympt<lTOJl atle. the initial dooe and continued abstioenC8
4. "supportive" medicationa
A. thi.w:ni.o&: 100 m!" 1M q d .. 3 d (can be given IV if needed, but there is risk
ofadvene reacuon ). Rationale: high-concenLratioo glucose may precipitate
&Cut\! Wernicke's encephalopathy in patients with thiamine deficiency
B. folate 1 mg 1M, IV or PO 'I d .. 3 d
C. MgSO. 1 gm .. Ion admiSflion: helpful only ifm agnesiWlllevels are low. reo
duces sei~u re risk . Be sure renal function is nonoal before administering
D. vitamin B,~ for macrocytic anemia: 100 I'g 1M (do not give before folaw)
E. multivitamins: oi benefilon/y >fpatient is malnourished
5. seizures: ~e JXilJc 261 for indications for treatment
'"
7. Neurot<lxicology
NEUROSURGERY
A. phenytpjn (Dilantin®j: luad with 18 mglkg .. 1200 mgl70 kg rUe page 271)
6. eT.ha.nol drip: nol widely u.~d . S% BlOH in 05W, ~tart at 20 cdhr, and tilrat<! to
.. blood le".lof IOO·l5Q m~dl
OELERIUM TREMENS (DTS)
When D'l'~ occu r, they ~uaJly begin withill4 d8y~ of the ~t ofEtOH withdrawal.
and typi[8lly persist (0.1·3 days .
Signs and eympUlms indudJ,: profound disorienta tion, llgitation, t remor, imwmnia,
hallucin!>tiona, severe autonumieinaubility (taoby-cardia. H'l"N, diaplwre3w, hyperther·
mial". Mortality i8 5-1O\\' (highor in elderly). but can be reduced with tnlotment lintlud ihg troating ~ted medical problem~ and t~t.ruent Ibr aeizures).
Haloperidu] and ph~nolhia:unl>B mAy e,ont ....1 hallucinations, but can luwer the Mli.
lui'll th",shold . HTN BIId tachyarrhylhmial . h""ld be tnsted as outlinellbove under Ill ,
c..,h"l ..-itbdr8walayndrome.
WERNICKE'S ENCEPHALOPATHY ( W E )
AKA Wemicke-Konlakufl" eneephalopalhl'. ClallSic triad; em:ephalupathy (consistIng of global ""nfuaion), ophlhalmllplegia, and atula eNS; 11113 are pT1lllent in only 10·
33% ofcuu).
Due to thiomine de ficiency. Body 510",5 ofthhllninearead~ua~ only for up to - 18
daya. May M seen in:
I 0 certain BIW:~pl:ib]1! Bubset ufthi!lllljn.defici~ntaIC(lbe>l.i<:ll . Thiomln.. dencieo~
here iadue to ~ tombinal;un ufinlldequatl! iotake, reduced absorption , decreased
hepatic &wal:'l, ~nd impaired utili~ation
2. hyperemNi8 (oa jn lume pregu ancieU
3. s tarvatioD: including anor~~ia nervusa. rapId weighllo~.
4. gastroplicotion (bariat rk surgery)
6. neotOdialysis
6. can"""'
7. AIDS
8. prolOllged rv hypera.lin:..~nt&tion
Oculomotor abnormalities ..,....,ur in 96'11> and indud .., nySt"fPtlu8 (horizontal > "ertj~
cal), lateral rectu s palsy, cun,jugat.!·gllZe palsies.
Gail aLaXia i.IIseen In 87%, 8fld results frolll a oombination of pOlyneuropathy. Cl're·
t>ellard.Ysfunctiun. 8fld veatibular imwirroenL
Sy.t.erruc 8ymptomo may indu de: vomiting. fever .
M1U : May , h(IW high s iJ,'llal in 1'2WI and FLAJR images in the pa'raveDlricular (madlal]
thalamus,.the floor ofth1l4th ventricle. and pe ri aqueductal ~9y of the midbrain . These
changes may resulve with t realmeDI'. Atrophy of the mammill ary budj"," may alao be
seen. Normal MRI does not RIO the dlagnO$u .
Treatm ent
Wernicke'. entephalopothy (WE) III a medical emergency. When WE i. $ullpect.ed,
100 mg thiarnine$hould begiven 1M Dr IV (oral route ia unre/iable,sa llbow)daily for 5
daY8 . • IV glucose CIIn pr..clPltat.e acute WE in thiamine derkle"t patients, :. give thia·
mine fint.
Thiamine adJUini~trat.ion improves eye findings within hl>Urs to day,,; ataxia and
confusion improve in day~ to weeb. Many palienlll that Bumve are left. wic.h horizontal
nystagmus, ataxia, and 3Ih\ have Kurnkoff'...yndrome {AI<..... Korukorr! psytho9i,1,
a diubling memory disturbancc Invoiving retrograde and 81Iterograd~ amnesia.
7.2.
Opioids
Includes heroin (~hkh i. usuolly iTueeted rv, but the powder can M 1ID0rteQ liT'
... moked) aa "'ell a. prellcription dru~, Opioids produce small Jlllpiis (miOllIll).
Ovenloee produces:
1. rerrpirll.1Ory depll!$!ion
2. pulmonary "<lema
NI!UROSURG5RY
7.
Neuroto~icollliY
'"
3.
0;:0l1\.li
• . hypotension and bradycardia
5. ."izurea may o«u r wit h: propo:q>phe ne, m eperidille (!leme rol4t) which may .1&0
aoUM deleli um, IIf>1i the Itreetdrug combinatioll of"'1'". and blues" (.et pagt 259)
6 . r.tal overdOMl may occu r with 8ny agent, bu t I, mOTe likely with Iyntheticopioids
luch as (ent a.nyl (Sublimate'll) among "'$era unfamiliar with t heir high potency
IUver sa l 0' into:dcation "
A tQt dOH ofnalol<one (Na rclIn<t) 0.2 mg IV IIvoid. sudden complete f8verul oh ll
opioid .. frecta. If no .ignificanl reactioo OCtu", a n a dditional 1.8 mg (for 8 I()t.al do.e of2
ml) will r'fjverM the toxici ty afmon opioidl. If nHded. t he dose rna)" be rePl!ated q 2-3
minulH ... p to. to .... 1 of 10 mg. 81though even 18rg<!f doleS mly be needed with
propoxyphene, pentuoeine Or bupreoorphine (Bupren... aCI). NaioxOlW! "'ay pr1!<';piltlte
narc:olic wic.hd rawallyruptom. in opioid dep'!I\dent patient... with a.:u:iety or ~u.uon,
piloer"Ction, yawning, l oeezing, rhioorrhea, nausea, vomiting. diarrhea, abdominal
cramp!!. m....,l" spMm •... which an! uncomfortable but not lire !hr..knin,_ Clonidi ne
(Cata pr.f4) may be h~ lpfu l for &ome narcotic withd .. waJ lymplOme.
With long<! r acting opioids. especially methadone I DoJophio~). repeat dOlell of
na loxo"" may be obviated by th. UN of nalm"r,,"e (Rove.), a 10"C..din, narcotic ao·
tagOni5t which i. not appropnate for t he initial tr<!atmp.n t ofopioid OVen!Ollge.
7.3.
Cocaine
The ineNn ing use of.:oc:aine in its vanou. forme (including Crick) is resuJtinc in a
n se in theinciden... and reeornitioo ofib deletHio ... eft"ect.son thCNS . Effecu.on other
body '~tem s (tachycardia. acute myocardial infa rdion. al"thythmias, ruptureof ueend·
ing aort.a (aortic dissecuon), abruptio placenta. hyperthermia. intutinal ilOChl!mia. Iud·
de n dea th ... ) are well d()Cum~nte<! ","where, IlIId .... e not further d~-.:I here.
Cocaine is utTaete<! fromEryllu'orylOll COCCI If!avell(and other Erylhro:ttyloo ' p«ies)
and is th u ~ unrelated to opioich. It blockl the re-uptakeofnor-epinephrine by prfll)"l>8p.
uc adn!nergie n,,"'e term inal,. It ;. avaUabl" in 2 formt: roeIIine hydrochloride (h<!lt ta·
bile aod water solubl". it il usually taken PO, rv or by l1.li",,1 in l umation) and as the
highly punr.ed cocaine alkaloid (free base or crack cocaine, whic:h i. Ma t It.able but in·
&Oluble in waler Ind i. UIWlUy smok~).
Peak toxicity occul'l60-90 minutea after ingestion (except for "body packen"). 30-60
minutel after snorting. lind mi nutea after rv il\ieCtion Or smoking (frHbaae orcrack}l<'.
Ac ute pharmacologi c e ffe<:ts o r cocaine
Acute pha r maoologic eff,.., .... pertinent to the .... "'OWlI~t<!m i ..dud",
I . m~nt.al .tat....: initial CNS .timulatioa that fi ..t manifests as a M'nH orwell.beina and .upharia. Sometimes dyapharic a,;t.at ion results. ooxas...... lLy with dele·
dum. Stimulation i.lOllowed by d~ ....... iOll. Paranoia and toxic ~ychosi. may
o«ur with OV~niOllge or chronic use. Addiction may OCC\IJ'
2. pupillary dilat.ation (Illydnasi.)
3. hyperten. ion: from aw-.. ... rgi~ di.mulation
NOD· pba nn lco)ogic effects related to the ne rvous system
I . pit .. it.ry deteneration: from chronic intra.naaal use
2. Cflebral vuculiti., leu common than with amphet.ami .....
3. Hi zum' pot,ibly rel,ted to the Jocalanesthetk Pl'OP'!rtieI of cocai ne
4. cenbrov_ular a~ident (CVA. ttrok,),'
A. intra~erebral hemorrhase: _ 1"'f"Gce..,bral Mmorrlw&e. E;1,'olOtl~1 on page
'50
B. lubarachnoid iM!morrhage'" OJ: pouibly .,a mult of HTN in th<! p..-nce
ofaneuryt.ml or A\I1>II, however. sometiroH no lHion it demoMtrated on
angiOflTBphy". " Iay pouibly be due to ",rebral vaKuliti.
C. Itchemic strolee'': may mult from vasoconl t n ction
D. thrombotic s troke "
E. TIA"
6. .nterior Ipinalartery syodrome"
6. P.ft"_ of maternal rouille ..... on the fettli ne .... ou. lyatero include": microceph·
aly. di.eorde.. of neuronal migration. neu ron.l differentiation and myel ination .
... rebra! i.. {amioo. s" ba..chnoid and intraee rebral h"mol"tll . . . and l uddeo in·
'"
7. Neurotox.iooloey
NEURm,'URCERY
fant death syndrome (S IDS) in the postnatal period
TREATMENT OF TOXICITY
Most cocaine toricity i8 too short-live-(\ to be treated. Aru<iety. agitation or &ei~ure8
may be treated with IV benzodiuepines (e.lI. lorazepam. _ p4lJe 266). Refractory HTN
may be treated with nitroprusside (Mf! page 4) or phentolamine (Regitine«l. ISU fXJIJe 469).
IV Lidocaine used to treat cardiac arrhythmias may cause seizures".
7.4.
Amphetamines
Toricity is similar to thotofcocsine (1ft obowl. but longer in duration (may Iallt up
toseve ral hours ). Cerebral vasculitis Dlayoccur with prol onged abuse (Ut pogt 63)wl\ich
may lead to Ci!rebral iruorotion (u<' poge 774 ).
Eliminotion ofamphetamines requires adequote urine output. Antipsychotic drog&
such 06 haloperidol (Haldol®) should not be used bei:aWle ofrisk ofseizures.
7.5.
•.
2.
).
References
a..m... M E.Simon R P.C .... nb<'. DA . Ethanol
j 27.2(0).
Md tho...,..."", . y... m. ~ EqJ J M«I )2 •. "'1·)01.
10.
""
H.
Co«h .... P9:AI<oI>oI _ _
<. S,,·..... 'S·168_
11. ''WI.
lohr RII ;T .......... oftkohol .. "I>.Io . ...
pi .. 'i .... pa,;.., ... M.~ oOl n Proo:7'I)' 771_11.
,in _
i 2.
'W}.
•.
l.<o<M<IIb<" R,W""""T'! : S<' ..... n.~" i 'h .....
<0 ..... ' • _ _
A«h Nflo ..... ' 7.
"r"'......
Il.
SlH. I990.
}.
S.lh."" J T. Syk ... K. SCM.ide',.,." J. "QI.: /IS..
......... nI ohleoh<>l .. ;I/Id...... , 11>< oe" ..... '",i<o'
'4.
"'''''0'<- .. ;""""wol . ........... n' f.. 01e0/l<>1 "",.
(CIWA·At). B. J Addi<l 14: ,)').7. 1939.
~.
s.o~. R . M ~S"'i th
.'do.,iu<!ttUI .... n'
fco-._ If"'.
M P.R~ . M 5 ......... I»4i.
wi ....... ".. ' A' ....
JAMA 2n'
'S
""""...,dOubk·OIilOl .... roIl«I
"9·13. '994.
~"" "oC.~ ."""
F.Col'fillO E.
.,Q/, R",i<!
'OPII""""" of .'<0lI01w,IIJd,.~. ' ,y""""",, by boo
I,
9
elokn, AmJ Mod ' 12() ~ 226-9.2001.
TtalO>CII' o f o _ w~t.lrow" . M..r Le'I<.ll.
75·6. 1986.
W"_WD.Y""" ..... len.nMJ •.,.I, MR1,"
0<>1 .. "'U1Ii< ••·. <...,..'{'!IIII~7 . N.. oo\ou 611~):
NEUROSURGERY
'6.
17.
dtu"
MO'.,.O<tioM to
of _
. M«I LOIl<r lS:
4)-6.19911.
""'<leo- R D. £<>10M; C M. S,""",~w,tI R C . ., .1"
'Ttl< """"''''''.,.. """'f'I'c"ionI of <0<1 ..... s..,..
1"... .-01 n, 3,9-<,. '991.
Uc:h,<ru<l<i PJ.R ...... DB.FtId1l"WlRS: ~h'
..... I><""",hol< pu.<ip"' led 1>7 e<>< ..... .-oinJ.
A,etI_ .1 : 22' ... . ' ~ .
O},<>,k. N M. CciIo/l" A R T.lIoonow D L. <1<>1.:
Co<. ,"<-.»4oc«1 .,.,...,.,..moI N","~ A"
",...i .. f..... in , ... "",onl ~jllO<)' of 1nt/t<1anl'I
_0'Y'''''? N'"1"OW'J<'131: }'Sol6. '99' .
5th......, K .... CohonJ ... : S" _ _ b<mot·
mOl< lR"'piI''''' I»'<O<:li ... ....",; .... M<b N........
,", 705.'~(!..
l<:.i""S R.SNI! IC M.n...11 N. ""',: Co",·
bn)QI.,."" <Ompl;n,ioo, of ,... "'" oflht .. ""~.
f""" ofol~oloOl.lJ ,,",,"'ne . N En&I J Mcd 31)0 699"lO4 . ''190,
ModyC K. M.tIl" B l . M<h. l'"' H 8 •.,<>I, !'ItwoloCi< «>mpli... ,,,,,,, of <,X" .... M. Ncurolou
.11. ""'-9). '91!I.
Yolpe I J, Effoco of «x ........ "" <I>< r", ... N Eo&!
J M«I 117: )99.01)7. 1m.
7. Neurotoricology
,_,,,"n,
'.r).
'"
8.1.
General
COntciOllsnUlI hao
two romponenta: arOU8QI
Bnd conl.ent.lmpairrnenL
of ar0Wl81 ca n vary frolJ'J
mild (drowsinet5 Or som·
nole llce), to obtundation,
to nupor to coma, CO nlll
is the seVfn!st impairmen! of arouul. and;B defined Il$ the inability to
obey I'Ommands. speak, or
open the eyn to pain.
The GJosgow Coma
Scale (GCS ) is shown in
Tob~ 8-1 (note: the scole
Is inUlnded UJ asseu level
.lrttdoonsclcu&n_.
tect>nically, tnIs io • SCI'" 01
_ e •• "O(>
ma'lmpI'" ""''''PQnI~
range at I<Jt.II pants: 3 """"01) 10 ' S (nmnaI)
_ _ i$$1Ihg eye oper.1<19 ., pHI, ...... perl!>l'e<»llllimukl, (ll'le \If\'"""" associelecl 1'11111 CItIIUa! ~ may e....se eye _,e)
~ ,.., mo\OI' ,eJilO'!S4l. imp,manl 10 ~ ..,;nal <»rd lIan_11On
ofconsciouHoe!18 and ;s not
designed ror following
neurologic deficits), Some
cenleni realrd a "T" next
to the toUlI&eo", far 111'tienta whose verbal axis cannot"" Ullessed becau,", ofintuha t ion', 90% ofpatienl.s with
GCS s 8 and none with GCS~ 9 meet the above definition of (Omo. Thus. GCS " 8;1 a
generally accepted ope rati(lna.J definition of coma ,
A $CIOle for use in child ren is shown in TobIe 8·2'.
Table 8·2 Clllidren's ComB scale' (for 8gB <4 yfS)
,
same as adull Glasgow <:OmO sc:alot ,~c epl Joo _ , ,e$pQflM:'
"nge clklIlII 1l<I0I1I1 3 I_51) 10 lSI_mal)
Coma ,,"ultl! from one or Dlore or tile roUuwmC;
dysfunction ofhigb_ bl'3in~tem (eenlnll upper pons) Or midbrain
bilateral dienCli!pha lie d)'llfunctlon
dirru.se lesions in both cerebl1ll hem;&pheres (oortic.lll orsubc:nRical white matter)
PosTURING
'!'he following: term, an iMccurat.e In the Implication ofm. location of the lesion.
DE«Irticate posturing implieo a more. rO$traJ le~ion and prognosis mly bf' better.
ikcorl.icote po~lUring: CIBmliea\.b' attributed to di$inhibitiDn by removal OfCORiCO$pi·
0111 pathways above the midbrain.
'"
8. ComA
NEUROSURGERY
Overview: abnormal flCltion in UE lind cxte!\ljion in LE.
Oi!t!lU: 8low nexion of
wrist end finec<'" with edduction in th e UE_ Erlen,ion,
intern,,1 i'Otalion, ph.ntarfluion in LE.
II,.,,,,
Dece r e b,.lI t e po8turin g: Clfl&4icelly attribu~ t.odi,inhibitioo ofveslibulospinallrACI.
Imore cAudill) ~nd pUCltloe reticulAr formotion IRE) by .-emo'l;n, inhibition of medullary
RF (LrD03C!ctlon lit iot.ercollitular le~el. between vestihulllJ" and rlld nuel@i).
Overview: abnormlll utenaion in UE and LE.
Dctsil: opisthotml!ls (head and trunk exteoded), teeth clenehed. anNI extended , ...uducted lind hyperpronstfd (InternAlly rotated). wrists nexed. fingel"l nued. Loegi ClItendI!d lind ,nternally rotated, feet.plnntarflexed lind Inverted, ton phmUlrnexOO.
ETIO LOGIES O F COMA
T OXIc/METABOLIC CAUSES OF· COMA
I. elHtrolyte imbalance: ""pe<:illliy hypo- or hypematremia, hypen:a.J.,...mia, renal
failure with elevated BUN St creatinine. liver r"jlu", with elevated fI/lImonill
2. endocrine: hypOglyccmifl, nOhketotlc hypefOlimolar 8tate, DKA (diabetic Iotl.OacidO$ii , AKA diah<>tiCCOIl,a), myxedema COIllII , AdditotUILIl cn$is (hypoILdrenaliamj
3 . vll!lcula.r: va~ulititi. ore, hyperten&ive encephlllopathy IHtl JICISt 64)
4 . !.oxic;! EtO H, drug oYerdOl«! (including nllra>ties, iotTOfl:eruc polyphannsq', barbi~
tuute.), ln d ioto>(iclltlon, carbon lD(NJox.ide (CO) poisoning. cydoe-porine {CfLIlUI
ftn encepha\opetby that.l>owB white--mat~r d,,!.ngH 011 MRlt./Iftti.e often reve rsible with discOUWlufttioo of the drug )
5. infectiouslinflftmmatory: meningitis, en.cephRll tis, ~~psi. , lupulte rebriti~, Ileumu rc:oidOlli6 lUI /XJgt .',6), toxle-ahock s yndrome
8 ne-opllllltie: leptomeningeal carcinomp~i.t, rupture of Mopl8lticeysl
7 . nutritional: We,." lco's erwepltalopethy. vi' lUIlio Bit deficiency
8. Inherited ro@tabo\icdliOrderl: porphyria, la~ti~ aeidosil
9. ot"!(8n failure: Uremia, hypo" emia. bepat,ic en.,...phalapathy, Reye'& s yndrome , an oxic enc~phalopalhy (e,g. poO t. re8USCillLlion &otlll;l).rdill~ arrest), Co, oaTCQlli$
10. epileptic: st.atll.ll ('pileptklUl (including non-.(:on'lu\aiv('datWl), poSt...icl;:llat.ate'1s-pecilllly with unob6ervtd !lei~ur~)
SrAUCT1JRAL CAUSES OF COMA
I. vaS<;LLlar:
2.
A. bilateral cortical Or subcortica l jnrarcUI {e.g. with canlioembolism due w
S8E, mltrlLl &tell08 li1, A-fib, rnuraltbrombu • .. .l
B. 0«Iu810n of venelsuVplying both ce rebral hemiaphare.g (e.g. severe hHate .....
81 earotid sle n{)lli.)
C. bilateral cU"n~phallc In llirrta: wdl des<:ribe<l syndromI'. May be due to oedua ion 0( a thaJamo·perforaUlr&uppl};ng both medial thalamk a",OI or
with ·top-o~-the·hlla ila r · O«l u8ion. l n itillJly ret.embles metohDlic coma (in·
cluding diffuse I lowing 011 EEGl, patient ev<Inlually arour;e~ with apllthy ,
m('mo/,), lOll, verticai gau paresi.
inrectiQU": ab6enoo wi lh .'jJIliflcan l ''''''''' ~ R"L><!t, ."bd,,~.J e mpy""na, h,,'P"o Aim"lex e ncephalitis
3. neoplutic: primary or ro~ tlL-ilt.atic
4.
LrILU'Il I: hcmorrhILgic conl~ion5. e!lemtl, hem9tom9
belo,ul
herniation from maM effect: presumably br8in8wm
compreuion C.8uses <b'sfuru;tion of relitular activat·
ing .yalem or m~S8 in one hemispbere l:IIusing COOI~
pression of the other rnulla in bilateral heroisphen!
dysfunctiDo
increased intraerso;.l pru..;ure: rcduC<!8 CBF
aCute laterA l dhil\ of tm, hrwn : e.8. due he mlLtoma
(.ubdur1l! Dr e pldural l (...,~ Table 8.J)
(...,~
5.
6.
7
NEUROSURGERY
8, Com8
Table 8-3 Ettect olla te rshill on level of
con scl0ll8nesr
a'
>S,
P SEUDOCOMA
Diffe r e ntia l diagn.osis;
I.
2.
3.
locked-in syndrome: ventral pontine infarction
psychiot ric: oOt01OnlO, conversion ",oction
neuromu&Culor weiliest: myasthellio IP"lIvia. Guilloin·Bo:rrt
8.2.
Approach to the comatose patient
The follow;ni covers non t raumatic oomo(see Hood Irauma, paie 632 for thllt topic).
Initilll evalulltion: il>(:ludea ITH!O.!IUre:!I to protect brain (by providini CB r , 0.. lind
iluoose), assesses upper brllinatem (Cr . N. VII I), and rapidly identifies8urgica.l emergencies. Keep "peeudoooma" os II pol-lJible etiology in b8ck ofmilld.
ApPROACH TO COMATOSE" PATIE"I>IT, OUTliNE"
1. cardiova~ulllr stabilizlltio n; establish airway, ched< cil"(:ullltion (heartbea t, BP.
cllrotid pulse), CPR ifnece56sry
2. obtain blood for tests
A. STAT: eJectrolyte& (espe<:ially Nil, glu<:OSe, BUN). e BC + diff. ABC
B. others as IIppropriate: toxicology screen (serum & urine), calcium, ammOnia, IIntiepileptic drug (AEO ) levels (lfpatient is ta king ABOs)
3. IIdminister emergency supportive mediclltians
A. gluoose: lit lefUlt 2::' rol ofOll> 1VP. Due to potentillily h arm fuJ e ffect ofglu·
OO/Je in global ischemis, ifpoallible check fingerstickgluoo$t! first , ot herwise
ilucose i8given without exceplion. Wllesa it is known with cert8inty thllt Be·
rum glucose is normal
B. 118loxone INarcan®): in case ofnarootie overdose. I limp (0.4 IIIg) IVP
C. flumatenil (Romll!ieon®): i.., case ofbenzodiuepine overdose (ue page 36).
St.Ilrt with 0.2 mg rv over30 secondR. wait 30~, then give 0.3 mgover 30
sees lit I millute intervals up to a IIIg or until patient llrouge9
D. thiamine: 6()..lOO rng IVP (3'10 ofWemicke'. pre!!<lllt with coma)
4 . COre neuTO exam (aesHS8s midbrllin/upper pons. allows eme rgello!)' rnefUlures to
be Instituted rapidly. more thorough evaluation possible Ollce 8\.abilite<ll: - {see
Con MUro ~%(Im below)
::.. irhe rniation syndrome or aigns orexpandil'lg p-f088a lesion with brainstem oompression (ue Table 8·4): initillte measures to low&/" ICP (see fCP Irwl"",,,1 ""-'<l'
.urn. page 6::'::.), thee get a CT &Clln if patient bt'gins improving. otherwise
emergen cy surgery (ue fHllJe 772) . • Do tiQI do LP
'"
long tract sign$
, i
immedillte-
B.
.,.
move
".
6. Coma
NEUROSURGERY
Ol"gl.t. (LP in thilletting m~)' Iw risky. lee u,mbar puncll<~, p.gto 61 $).
seilurel if pn!lenL If sLu l u8epih!pti~", i'."6'-~, trut ... in.
d,tlIted on pa¥e 26510b18111 &merg<ln~)' BJ::G If ava.llllbl.)
8 treal metallohe abnorma lit;,.
A. reltore acid· ..... b~lllJ\ee
8. reltoN ~lecl rolylA! 1mba\" ' r:e
C. m.inl.a;n oody lempulllture
9. ob"' in o. cOll'1plelA! histo.,. ILl! poMible onee ~taobiUud
JO. admlnlat.er ~I*ifi~ Ihrlll'i ..
7.
t.n1I~III!ll~TB!I,eC
CORE NEUno EX~M (FOR COWV
A. rel (!i r ll.tory rote hod pa lttm: the moat rommon disorder in impaired ronac:IoUllnltlll
1. C h eyn ...S t oke.: breatbin, gradually CN!IiCendo.ln amplitude a.r>d thlll! ~~
trail~ off. follow.d by lin ,.pirnt.oty
L
p9U61!.and then the pIIl\.trn repeat.a.
,"
H~rpne~c phue iJ, ",uIUy. lon~r
Che ne-Slokes r,S!li'-'Ory panltln
thftn .pnetc. Uliu.lIy Ief!1l with dl~V
oopba!lc lesion. Or ...n.teral ~bral henu'pbere d),.ful>elion ('!IIf1 •• ~U;cJ. e.,..
ea.l)' Increased ICP or mt~boho .bnormahly. Rault.l fnlm anllKtea"d vMulltory ' ''I!pon,e toCO:!
2. bypene ottlatlou, usually in reapo"" 1.0 hypou:mia, m~botic !Icidof;i., .,pi...
Lion. or pulmonuyede",a. True ef1ntral neur~nic hypo""Mtilal>orr .. raN, and
",u.lly results fromdywfundion withm the poria . [fnoothe. bnunst.m algmare
present, mRyaUUe6t pli)'Chialric di5Ol"l!tr
3. du.ter bre.thi ng: penodlOf
rapid ilT1!gula. breathio" &epa.
ral.e'd by apneic lpellt. WIly IV·
pur .imillr to Cheyne-Stoket,
UI'\J' merge with
pat·
tern. of gupin, roespiratloll5.
High medulla cor lower pont~­
,iOl}. Often an 0"';nou5 eign
.. . a plleuat;o (rare): e pause It
full iD!lpiratlon, Indie.\86 poll'
tllle lesion, ~" with b .... il •• ar_
tery O«Iu,ion
-I'''''
v.nou.
,
a t .. le (Biot'. bN!athini~ no
pattem in rate ""depth of ..... pi_
raliOI\l. 58" With medulla.,. le.ion. UlUlUy pNltarminal
Alax"oc .espifaliol"$
*
B.
""1.11 (,ioe in mIn) in ambient light. and U! roeacLion to ditftlltnnsens.uallight
"'lua) and. reactive pupillindiuole to~i~n-...llIbol;c CII~ WlU! few el<a!pllona lllft
~OU/) (m.y h."", hippua). The light n!f1ex ilr the JIl(If;t uaful tiign in d181inguW1lOll metabolic from IIf\lctum toma
A. the2lllx ....J.!>boIic ca,,_ ofrued/dilated pupil: i lutethimlde toxicity. an·
ode enCf!pb.Jopalby, I ntldoolinergiat (ind..dilli: .tropi~), _ftiolUllly
with botulJlm toun poisom"l
8. narcotiCi cause 1m!>11 pupill(migaWwith I , mall ran~ ofr:onfuiction and
. Iulgiab NIW'tion to light lin "~fre oyerdon, the pupil. may be lo.m.ll
that a mqniryinr
"'Iy be needed to _ runion)
2. unequal (nOt« an aff.... nt pupiUaryde/'ecldON lUll produce InrlOCOria (... Alltrolio". in pllpillo,),dillnteler, pep 582)"
Ii liaed Ind dilaWd r,u pll: ,-uilly dUII.OOC:l.llomoto. pal.y. PIluible hemia·
lion . NPf'I'iaUy if arce. pl.lpt.I MIOci.ted with 1P'!;I.\.t. al 3rolM!..... e OOM
pelsy (eye doeviat:.ed "dowD !>nd ouI"J
B. pcnible Homar'. 'rndrome: conlIider ta.ro!.id _It>.ionldiasut lol>
3. bilater.1 pupillbnormalruu
Ii pinpoill~ with m;nl.lta. .eec:tilll1 lbucan be det.ec:uod with l>illi'lifyl ng ¥I ...:
ponline letion (.ymPl'tMtic inpu~ it 11If1; paru)'UIpllt.het.ics emerp at &d.
i"le.·Watphlll nudeu. aDd I~ "nl,lppClSed)
8 . bilateral n~ed and dilated (1 · 10 trim): . ubtoul dllm.~ to medulla or lmmeI.
,1_
NEUROSURGERY
8. Com8
'57
diate post,.anoxi~ Or hypothe rmia (core temperature < SO' F (32.2' C))
midposition (4-6 mm) and fixed: more ex.tens;ve midb".ln lesion , prosumably due to interruption ofsympatheties and pare.sympathetics
C. extraocular muscle functi on
L deviations of ocular a>:es at re!lt
A. bilateral conjugate deviation:
1. fron tal lobe lesion (frontal .::.enter fQrcontralateral gaze): looks toward
aide of dea: n.octive lesion (away from hemiparesis). Looks away from
side of /leiZllre focus (looks at jerk.ing side), may be statu s epilept icu &.
Renex eye movements (ru below ) are norm al
2. p..",tioe leaioo: eyes look ~ from lesion and tooYards he miparesi s;
caloriC!! impai red on side of lesion
3. "wrong way gaze": medial thaJamiehemorrhage. Eyes look aw .... y from
lesion and towards hemiparosi . (an exceptioo to the axiom that the
eyes look ~a destructive $upratentoriallesioo )'
4 . downward deviation: may be associated with unreactive PUpil8
(Parina ud's 8yndrome , oei1 pag~ 86). Etiologies: thalamic Qr mid brain pretecta l lesion s, metabolic coma (esp~iaJly ber bitW"ates), may
follow a llelZUro
B. unilateral outwa rd deviation On side of Iaeger pupil ([II palsy): uncal hemi·
ation
C. un ilateral inwa rd deviation: VI (abducens) nerve
C.
O.
!;k~1l!i.2n
1. III Or IV nerve/nucleus lesion
infratentorial lesion (frequenUy dorul midbrain)
2. spontaneous eye movements
A. 'windshield wiper eYell": random roving conjugate eye movements . Non·l ....
calizing. Indicates an intact 1lI nucleu s and medial longitudinal fasciculua
B. periodic alternating gaze, AKA · pin&"·pong gaze": eyes deviste side to aide
with frequencyd - 3·5 pe r seoond (pa using 2-3 &eC$ in uc h direction). Usu·
ally indicates bilateral cerebral dysfunction
C. QCulp r bobbing: repetitive rapid vertical deviation downward wiU, slow re~urn to neutral position. Pontine lesion (Ht paIJ' 588)
3. intern uclea r ophthalmoplegia UNO) : due to Ie. ion in medial longitudinal fasciculus (MLF) (fibers Cr0531ng to contraiaterallil nuc\eua are interrupted ). Eye ipsilateral to MLF lesion does not adduct on spontaneous eye movemen~ or in
response to reflex maoeuvers (e.g. calories) ( sa P<JCI' 585)
4 . rolle .. e)"l mo\fflments (maneuvers to test brainstem)
A. c>cw Qvest ibuln r enel<". AKA Ice water ca lori ea: fi rst rule-out TM perforation , then with HOll at SO', irrig8teoneear with 60-100 ml of ice water.
NB: ffl9po<lse is inhibited by neuromuscular block.i ng agents (NMBA)
I . a comato"" patient with an ~brai nstem will have tonic conjugate
eye deviation to .ide of cold stimulU$ ..... bich may be delayed up to one
minuteoT more. There will be 0.0 fast component (nyst.egtOusl (th e cortical component) even if the brainstem is intact
(NB: c>culoccpb alic renc,..s (dolJ'8 eyea) providSll similar infennation os oc~lovestibu lar relluc . but poses a greater risk to tbe spinal
cord irC-slline not cleared )
2 . no re!lpoou : symmelrical, could be spe<:iflc toxio (e.g. neuromuscuJar
block Or barbiturates), metabolic cause, brain death or pos.aibly mas. ive infratentoriallesion
3. asymme~"c : in fratentorial lesion , es pecially if ro'ponse inconsiJItent
2.
(..
A. ""ulov"'. 'ibulor ...,n~" Joliet): tho ...,'icipourl reo""" ... i. commonly "'i . und ~ ....toOd. In •
norm.! oW "",ie nt Ib..,., i•• Iow de';. ti.n towordl lhe . id. oflh. <old . timulUI .. i,b ny• ..,." • •
(which " n.., eeI ror the ,. p;d. ~i ...1 ph...) '" th. Oppooi<e di,..ct;'n (hen .. ,ho .,nemon;'
"COWS" {<o!d-<>ppooile . .... ""...... Nyotap>u . ... m be IIbHnI '" th . ... ",.,.,.. ""tI'nt
8 . oc:u.i"".pb.Uc ren"" {-doU· •• ye'" or "<Iolr. _d" ~ d. ROC porfurm if ,he .. \0 . 01 un"..u;nty
.bou t ".mCIII .. pifl . .." bility. In an n:aK ""tio-nl.lho e)"U";1I oitlMo, lD_with the hu d . 0'. if
,h. 1D0",,"'on, if;.low el1O",h and the "" ti.nt lo futatiDg on on ohjo«. tlMo .....ltI be . ontr. ~ .. i""
•• nj ",ot.e.yo .. ov."'~ o\· (c.f. ocul ..... tibuJ .. ,..II~ ~ "'·~ i.~ _ not depend on pII t;. n", 1•••1 or ....
ope"'tion ). In . oomo_. ""'ien, with a.n ",tact b,..i n. tem '" <T. ni. l Dorv... 11...... ...,11 . 1.. be oon·
' .......i • • <onjuIOt.e . ye """,.",ent (. poI;ti • • doll'•• ye..... ponst)
C. o<ulov ..,ibQIa,. ,..11..... oro o boent but o<ul_ plo oli< Ide ",. iflt.oiaec! . nlywh. a . .. tibular lnpu,"
. .. int.ern>pted, ~ -i . OlfoOp", ..ycim ",';";ty ofJobyriDth. or M.teral """""ti. ","uram..
».
'"
8. Coma
NEUROSURGERY
wilh 3rd nerve palay (herniation). UaullJIy OInjntllmed in !.OXic/meta·
boUe«>tna
4.
1IJI$l.IIrmul without IOnic deviation (i ....Y" f8ma ;n In primllry
lion) virtually di/lll(n08t ic of l'IIychopnlc wIDe
c:ontrelatualaye r.u. t.o adduct: [NO (MLF lealonl
6.
~i.
B. optoki ne tic ny ltermu, ~oc. atronal, IU!;!;"ta paychOgo nic eon,'
D. UlOI.Or: mu aele tone a nd l'1!f1exea, t8lljlOilBe W pAW. Bobinski (no'" a.ymmetries)
I. ap propriate: impJi" cortiw.pi nlll trleta lind eort.x ",tact
2.. 8.ymmuric; lupl'lItentoria l lylon (t.one Ulually IRcrenO'd). unlike ly In meUiboJic
S. incon, i.tentJv.ri.blt, HilU ~, POIytroBtnc
4. eymmatric: metaholic (""1I811J' decteJIl!f:d). Al tarixil , l!"tmor, n'yoclonu, rnft, tw
present in metabolic: coma
..
5.
I!yporene;<.ia: ooNide r myud.'lu, «Ima, nPHililly In patient
ane '1Taa.uphenoidal 'utte ry
6,
pattem.
A
p r~ ti [\1
wHIl$
_
decort.iute
po&tu.rinr; 8nM nex, lell ..,u.end: large co rtieal or ",beu rtlcaJ I&-
B. dfetrfl>l'1IU1 """tllnn,: . n . . .nd l.pcst.tnd: brainatem iDjury.t Or Mclow
lower ruidbra<n
C I~ nexed. lep nac:cid: pontine le(1JIeotum
D. Inn.llaccid. lep a ppropriate (·(r\8n·in .(h~bll'T1!l.YIldrom~): a no~i~ iIiju·
ry (poor proenCNia)
E. cilio5pi ...1 n!'f16"u (J'IIPiUary dil/ltf,upn to o'WO"'- cu t.f>toOUs.~l muJ i): ""!toll inug·
rity or lymP'thetic: pethwan
J bilaterally preMnt: mottabc>lI~
2. uailatll"'Uy ptUe1Il: poeible 3rd nerve le.si!>fl (herniati()rl ) iron.Hit orl~'1:er pu pil. Po.aibll p ....ni.Itin! Horner'. qndromf- ifon lide oI'".n>.III< pupil
3. bilateraUy a.IuIenr.: lUIlJ/I Iy nllt h.. lpful
8.3.
Herniation syndromes
Cla.ic If'Ichinr:: hu been that shiJ\l; in bnlin mue l",r::. QI\I500 by m8He1 or inintmer.nilol prasulll) throuCh rir::id openi",. in thll . kv ll (hemiatiaa) c:omp.....
other Itzvcture. oIthe CNS prodlldog theobMrved 8Ylnptoml. Th.. view hal; been
challf-nCed'. .. ith the h)'pOthuis lhat hf-mlelion may be an epi phenonllnon that !XCu"
lau in the pr_and i. notaetu.lIy thetaUSlloftheomllrvau.",.. Hp~er. Mmia tion
moder- al ill H .... e III ~ul.ppro~imation ••
ThUf- are many popible hen>i.tion ~dromH. the » vI JI)OIlc..mmon ....:
J tentral ltranlt.tn:.orilll) bemlation (_ Pl'B" 160) }
.... p ... teotori.l
2. uneal herniation 1_ pG6I161l
herniation
3. cinguJatl hf-miation: ci llCUl atll eyru. hernlal.eoll und~ rab (AKA l ubralcine
.... mia t.ionJ. U..... lly ....ymptomalicunle.. ACA k.inb and ooduducaul lng bi·
ofimpenliina: lTan"III1LOriallworniation
frolltRl infardion. UsuaUy
4. upward Of-",beJlar (we bdtN#)
}
inr.. telltori.1
hf-mintion
6. ton. mar lu.miotion 11ft. t>tlow )
~
".roII
COMA FROM 5 UPRATEHTOfilAL MASS"
CantrllJ and unul hemlll t'or. eoeh ca U_ " differtil t fOND ofroatraJ-eauda l ae' .
";orlltiol1. Cfll tra l htm,at>on , H uh. In Nqlle"ti.1 ra;tu", 01' dian«phalon . midbra in.
pon •• medulla (arf fHl6' 160). For ul\C8l herniation , 11ft' pap 161 . ' CllIu ic" l ien' ofin·
o;rellSed ICP (HTN, bradyurdia , .1te~ ,,"piralor), patUom ) lUIUlllly MIn with p-fOM.
Inionl may blabHn~ 111 alowly d~'optl\( au pflteatoria.!
mlti",:tion betWl!tn cl!tl lTal and until hl!rnill ion i. ditTi~ull .. hen dysl\.lncti!>n
ruche. Ihf- midhrai n 1,..1 gr below. Predielin. the roeatlGn a rthale4k)1I bAM<! on the
m._.
hemiat.lon ayndrome ill unreha ble.
Clinical c horacteriat iu d ifferentiati"'i u ",c.a l from ctmtrlLl h e rniation
dt\:reaH<! «In.c1ousneU«Cllr. early in «nt ... 1.... rnillthn, late in uneal
uma! herniation IYIldromll.r.JJaiy giVell riM t.o d-"w:ate poiiturina:
NeUROSURCeRY
•. c...
'"
Differential di agnosis of s up-catentori a l etiologies
L
2.
3.
4.
va8Culu: CVA, intracerebral hemorrhage, SAH
innammatory: cerebral abs<:ess,lubdural empyema, herpes simplex encephalitis
neoplastic: primary or metastatic
traumatic: epidural or subdural hematoma. depressed skull fracture
COMA FROM lNFRATENlORIAL MASS
NB: it is essential to identify patients with primary posterior fos~ IKions (lee To ·
bit 8·4, page 156) u they may require emergent surgical intervention (Iff poge 772 ).
Etiologies of infratentorial m ase
L
vascular: brainstem infarction (including basilar artery ocdusion), cerebellar in.
farction or hematoma
2. inflammatory: cerebellar absceS$, central pontine myelinolysis, brainstem encephalitis
3. neopl"sm s: primary or metaetatie
4. traumatic: epidural or subdural bematoma
HYDROCEPffALUS
lnfratentorisl masses can produce oblltructive hydrocephalU$ by campreaSing the
Sylvian aqueduct andlor 4th ventricle (Iff page 404).
UPWARO CEREBEt1.AR HERNIATION
Occasionally lOOn with p-fosla masses, may be exacerbated by ventricul ostomy.
Cerebellar vennis ascends above tentorium, c:ompreuing the midbrain, and p<I8J1ibly.,.,..
eluding SCAs - cerebellar infarction. May compress sylv-ian aqueduct - hydrocephalus .
TONSlliAR ffERNIATlON
Cerebellar tonail s 'cone" through foramen magnum. compressing medulla - respi·
ratory arrest. Usually rapidly fatal.
Otturs with eitber Supra- or infra·tentorial masses or with elevated 'CPo May be
precipitated by LP . in many cases, there may simply be pre$9ure on the brainstem with·
out actual herniation', There are also cases witb significant cerebellar herniation
through the foramen magnum with the patient remaining alert'.
8.3.1.
Central herniation
AKA tranatentorial herniaticm AKA tentorial herniation. Usually more chronic
than uncal herniation. e.g. due to tu~or. especially offrontal. parietal or occipi(allobe •.
The diencephalon is gradually forced through the tentorial incisura. The pituitary
stalk may be sheared, ",,"ulting in diabdes insipidus. PCAs may be trapped along the
open edge of the incisura. and may occlude producing cortical hjjndness (see BliJ\dnu,
from hydrocep/w.11l8, page 202). The brainstem suffers ;"chemia from compre!!5ion and
shearing of perforating arteries from basilar srtery - hemorrhages within the brainstem
(I)"...,t h .. m" ....h .. g .."')
CT or plain x-ray criteria
Downward disph.cen'ent of the pineal gland may be demonstrated '", Perimesen.
cephalic ei&terns are compressed.
DIENCEPHALIC STAGE
Early_May be due to diffuse bilateral hemisphere dysfunction (e.g. from decreased
blood flow from incN!""ed ICP) or (more likely) from bilateral diencephalic d)'$funtion
due to downward displacement. This stage warns of impending (irreve",ible) midbrain
damage but ill frequently rever$ible if the cau"" is treated .
".
8. Coma
NEUROSURGERY
COi'iio.igalf'o:iiligll1fiOMiiOml tIM"'il 'Yen w:,ugaie t!iiiT&aiiStem 11'.l:id. OSU/IRVIiCiSib\ie
i
OO!..L'S EYES and conjIJgaltl ipSiIalMaj response LO OJI~ w~tGfealctb (CWC~ ImpaJred III)galt! _ to corrcresOOn 01 SlJPllrior coIIiaJ~' lina di8!\Oellha1ic pt(Ite<:Wm (Pariodli Ii)'l'l~romeSllflpa~86)
MoIor
a-"f"pjjlopOiajilii~~liSelO r.o~6itiIe"""'iirBitiiiiil<j. iiiljiiitiil!ili (paralOnic .. '
iiS!anu). II pltVicmly hemlpar~K:conl!aralelallO lesion: ma'J I'oOfSoefl. h~ mo!lonlessness
&.JI!.a5P ,~, Ihen OECOATICA!E (rilia/Iy ~JiIltira.!.!<' ~ n~_caS:!'.5~
l
MIDBRAIN - UPPER PONS STAGE
Wh&n midbrnin s igns fully d ..... eloped (in adulu), pl"Ojj1\os is is very poor (extnme is cnemia of midbrain). Fewer than 5% ofcase:s will have a rood tf!COvery ifl"'H tm ent Ie
successfully IIndertakl'II a t this st8g~ .
Aespiii1loiip~
~
""""""'in panlinll lllmo"noge poIlPQltlI PllPis lQIIItat IIKaus- I'" 1M$0I sy""",l~ C5 ""'_IIIePllr~l­
In n~mill\ron. 1M f'II!I,.yrn~lh.tIcs ... USUAlly 10$1 , too (3nl "'''''''1,*,'11)
Ic!I Uf'OllllllS8<l.
_<OM
LOWER PONS - UPPER MEDULUoRY STAGE
ISIOW, Ifii'9Ular r~lti arid deillh: Siijhs/gasps.
!Oocasionilly /lype1)lOU I llelOlt!og
OoTaleMdityWilh~'" -
============
wl\tl apnea
OUTCOME AFTER CENTRAL HERNIATION
In a series of 153 patl"nbwith sigNlofe(!nlrai herniation (altered l..... el ofellnlicloU$IInss,ani!!OCoria orf",ed pupHs.aboQrf!Ullmol.or fiodings) 9% had good recovery. 18~ had
fun~ional out.come, 10% weI'\!! wverely diubled, Bod 6O'l> died"
Facl.ors fls&ociated .... ith II better result wera young age (eapedally age,. 17 YJ"IIJ.
anisoeoria with deteriorating Glasgow Coma Score and n<.lnflaccid motor function. Fa",.
lOra .... soeiat<>d with poor oukorneo weI'<! bilaterally fixed pupils, Wilh only 3_5% orthf!Se
patientl haYing a funct.ional recovery.
8.3.2.
Uncal herniation
Usually oc<;u,.,. in Olpidly expanding traumati. /oemat.omal. rr"'lue utly in thalateral
middle'{08'8lI Or tfimporal lobe pUHhing medioJ unn.S and hippocampal gyrus Over edge of
tentorium . 0D trapping tbird nerve and direetJ,y eornpre~Bing mi~brllin . PCA DUly be !>c.
duded In with central herniation ). For CT criteria se:B. below.
Impaired consciousoes5 ill NOT a reliable ea rly sign. Ea rHut I:OnSi9tolnt sign: llOi·
lat.erallydilatinr pupil. How~ver. it is W1likel, Illsta patient uodergoinr e8rly unca l he ...
niatioD would be completely neurologie.ally intaet ex~t for anisoc<.>ril (do not dil;mias
confusion. agitation. etc..). Onoo b",ir.u;w,o findinga app"ar, deterioration may be rapid
(deep coma may OCCUr wlth;U hounot
CT criteria"
Tentorial incisura surround~ interpeduncular and prC-pOntine cisterns and b!"8 IO'
stem. There is gteatinterpersonal variability in the amount ofgpace in the incisura .
Impending- uncal or hippocampal bemintion may be indj~ated by en<,:r08~bm~n t on
NEUROSURGERY
8. Coma
'"
lpterala sped ofsupras.allar cIstern - nMterung or normal peuLIJgoIIP I ~ hape. Once herniftt.ion OCCUMI CT Dlay "ho ..... , brail'lStem di'& pl at~ment and natten;n" coroprellSion of tont ralateral eerehral peduncle, midbrain rotatilm with sligh t i~ase of ipsilateral
s ubarachnoid spate. Alii<), ¢olltralateral hydl'Ol'ephalus may occur".
Oblitern tiol). of par8S1!ll.r a nd interpeduncula r cisre" •• ~rB as uncus and/or hippocompll. are ror~ed th ....ugh hiatus. BrainBtem c,ompres!lion - AI' elongation. Since du ral s tl'\.lcture, enhance ..... ith IV contrllBt. thl~ msy be"SEd to help del ineate tentorial
IJ'IsrgiD,S .... bell neC@$sary.
EARL Y THIRD NERVE ST.AGE
(tj:QI A eRAlHSfEI¥I FINDING, DUE TO 3AO NERVE:: COW'RESSION)
LATE THIRD NERVE STAGE
Midbrllin dysfunctioo llCCW"S almost imlJ'ledjal..Jy aJt.er symptoms extend beyond
th06edue to foc.l cerebral lesion (i.e. mayskipdiencephalicslage. d~ to lateral pressutE
on midbrnin), Troatment deJ a}'s may result ill i~versibl e damage.
From Ihi~ point ,,"wanl . the unM I synd ran... is indis lingurnru.ble mill untrnl herniation (u<! aoow).
8.4.
Hypoxic coma
MOllie eneephRlOptlthy rna)' b.
pO.) or a.nemic 1I"."tia (following e..'(du.
10 .... 0 • ....,;"
auo.i
.. (drop MyoIn
IIDnguination
or canl
iac IIrreat).
donU! i. commlmly seen.
Pat hology: Jesiona pre-dominate
in 3rd oortica l loyer (grey ma~r): Ammon'. 110m ~ 1.1110 vulnerable_Whi ta
me lter;1 u~uaJ1)' better preserved
(due to lower 0 1 requirement) .
In tht bani g.nglia (8G ); enollernie anoXil eave",]), affects globus
palHdu.; " ""mie ano..u a aITec;ts th e
caudate nucleu s and pUI8Ulen. In the
eerebeUum. Purkinje «1I~, daniel<!
nucl ei. and inferior olivea er& affected
'"
8. Coma
: '~'~'~.~'~"~~;~~~~~~'~";';'~'~'~'~'='~~~
NEUROSURGERY
Mu Ltiyariate analy"s yieLds (XIt·
come prognosticator'll shown in Tobie
8·:; &06 Table 8·6. NB: this lI.Oaly. l,
~pp1ies on.1:t to hypo,ao;..ischemie
coma'· More r~nl6tudinwnfinn
the poor prognosis of ..mrellct;ye pupils
and !ack-ormotor ..,sponse loG pain"; if
/lither orthese findi np 8M $/len within
a rew houllI lI.l'ler cs,rdillO!aTTffl tbfte
;11. 8n 8O'lI ris k ofduth Or permanent
vegetative I Ulte, 8nd if present at:1
day. these th'. r8le t(l9f 1(1100%.
Clurocortiooids lau-roids) hllY~
~n ahown tohll.Y81\O bt:neficill ~trKt
on ~ urviy.! TaU- or neurolog'iC<lL re<'(IV~<:Y rate al't.i:!r cardiac: al'TV!t!7.
Ta ble 8-6
al>b""vlat;o,u,: \Oo?iL .. ... 'lhin no""oJ Il",H••• GCS
• GlUt_ Com • .su..101''GCS-<IIO\<I<' nk .. Ie
lIN IIIOICT ""..... .J: BOM • ".-craocula< mlUC.!.:
8.5.
References
t..-loItC.J .. _
R. ... " ...""' .. of .........
PAI' ... _ _, ......... JITXU<o.I-.
,,n.....
~, ":!
11"' , 19").
>. V',_ A B. H"'Y" R Il!C""'V.o;)" ...............
.,,'''',,, I/w 1onJd.J";""" p<1IWoI I. 1'I'~roI"''''
..... ro . . y'l'R K. Wi"",,,,,, J E.on<! Povl"""""l J
T.(*") MoCro",!.II;U.N, .. v .... l\I96!pp 1,9-
,. •
,
,
,
II",," V l.aw..,C.YonIo<l M J,,,IM. ll00d <0)0.
1,<1 In <M,n. "_ loS ""''''M of 'P' 1:l<mocr"
s>Ily ..... ao"' ...... C~11<II " .... S)'>. 4: 'l-'...q).I9U.
lI.op!"" " Ii; l.Il.-ru d..,....""'., of II... ."..;" oM
1<.. ' vi COlI"' .......... ,n ~"1<n .. w;lb .......
N hJl J M... ) \ ~ . gH· I.I~ .
P-c>ri<tCM· s.... ........ opN!\o\tnelotlcol_
,;.,. •. J ""'..... No........." . 1'<)<1tio'r) XII )1J·~2.
"<"""""...,...."
•%,
a..."...-uw.2uOS V...l6oolAlltJI ..,in .., ....
",..,po, ...... ,.,.d ,..." .. 46' )6 1·), 1W9
fi",...CM """"1ni.I>&ni,....., .... ........... _.
.. pt . s.... N• • rnk>tl' " 0\ 1·11. 198-1 .
_f._.JII.Th<d....,...."'''.po<ond
<Omo F ... D.t .... P~il .... l,.,i •• l..:J 011,. \OIJO;pp«J.
." ••
•
AIII<.C M.PI<w EH . " - .... "81~ ...... <hJ ·
"',..."...., ",,_,. , "'".,Iy",. o;_fl..pd
/'I...., M,", Dis 100 n ·n.
...."'.,_.'.J
NBul/OSURGERY
'"
"
"
"
"
"
.,
n
J9U.
H.... r. c..... yI cr"""..r.. _ _ ndl ••
,,,,,,.. _1,,,,.1Il>0<l. A... J N.."or1>dIi>I6: ......
'. 1~8J.
"'odrc"'" B T. PI&> L H' FIoO<1iato>, <K<I.<t}or...
"",,",oM! ~"'ion. J'I_fIH}'
19l :!ll.,JI.I'Il1
0<b0n0 ... G: DL,.<>OOi<otda<.""", '..............1
"...,....;0:
_by
<,..j/llC1".Ilod~ IJJ, ~J-6.
I~n
5IOYn., I, o ..<-,i", .......,/11 ..... ,.,...,: FUId" "OII«><" pYldiu<1l...,."".rb, !'Itu'.... dlolor;r
14, 101·f. I!fIT.
Me"fo_' W, nf!O< J C. B_ W H. "..s; E.< ·
.....", ... <N .... r.
Otoot", ....... OIl
!~,~ _
....""'" 167·n.I'lfI/).
D f ,c..o... 1 I.S' ..... 6 K.m./J l'I«iico<o1
........... r_..,·p<\I""l\co..nl< COOI"', JAMA 253:
L<.,
1~1O-6.19t)
~EG I, .II ...
RI. S,"".. _C,.."
.1. ' S,.,.""'o<,....k"ofeotlJ'pttd~GI
__
""I<""'
" ,•.,.,.io>--«<h<",,,,..,.... u..:.. JSl,
IlIOS--ll. \991 .
,..". ...... M. ' '',/Io·T,..!! K._
v ..""",
p." ..s.
O_ialldIlUlmmlClod
_ ............
I""inl _ . " iot ...... ,", <.. d,,,,, __ J AMA
2~ ' JoI!1·JO. 1919
8. Coma
>OJ
·
~
-
"
-
~.-
'.
...
I
9.1.
Brain death in adults
MOS1Uates l<C«pllOO1efonn of "brain death" asa valid detennination of death. The
President'a Commiu;on proY'ldes the following guideline5 L:
1. the diagnoBiB ofdeath requires both ceBs8tion offunetloll IUld imlvO!rsibility of
ceuotion ofeith<!rca rdiopulmonary 8~tem orfnlin broin (including braiDilteml
2. for Bge < 5 yean. _
cUrtlll in children. pag~ 167
3. with no "eomplicatillg ::onditloDP" listed below. there 8re· ...llo eases orbraill rune·
tions returning followmg a 6 hr cessation. dDl'umented by clinical examination
and eonfinnal.ory EEcM
4. with cnnditilll18 such 8S massive intrllcerebral tumor with hemiotion Or gun!lhaL
wound to the helld , it II possible 1.0 pronounce death sooner with more certainty
than. e.g. with pclL5t ""rdiac-urTe$t anoxia Or foUowing B toma " funknown etiology
5. wheo death re8ulLi from criminal ISlIawt. or tbe .... ia the poasibility oflltigatlon
l"'I"f!arding the death. extra care must he Liken and legal counMlJ rnay beadvisable
before rooking the determination of brain dCllth
a""'n
BRAiN DEATH CRITERIA
lWcommendatlOD sL. ' :
1. !lbsenc&0I DrI_irISIem 'elIeUS
A. absen'-"!of brai"8Iem refl ca·e.:
A. liud lll4"~
t. lXular eumination:
6
BbsenI comeal relle.(eS
A. rlX~d pupila: no ....~Pllnse. to
bright light (tau: ion alter reaus,
C. absfnI OC\IIOYestIWar ~tle~
citation: H e bflow). usulIlly midD. absenI ~hallc
po!Iitiou (4·6 mID) bll ~ may VB""
E. BCseoI gag &. w.; gil IeIlel:
1.0 dilated rlngeB (9 mm) In size 1.
B. abJ;ent corneal Taflel"'I!lC
3. no r~ to d\'ep~ pain
C. abHnt lXuloc:..phalie (doll's
4, 'oi\I1~
eyes) reflu (coll lrain dicated If
C·spine not elesr edj, _ {XlB"
A. tori! temp > 32.~' C (90' F)
/58
B. SBP '" 90 rrrn t'Ig
D. ,b....moc ulovQ tibuJllrren .. '"
iccld wewr ca Jo rl ell): it1lltill6(l..
100 ml iea water into one eaddo not do ifTM perforal.ed ) wiLh HOB at 30' .
Brsin death is e~duded ifan), sya moveroent (... ~ IJ06('. r58l. Wailalleut 1
minute for responBII, and::t a min before testing the op~it' side
2. absent oropharynC .. a! ....1'1,:< (gag) to stimulation of pDJIt.erior pharynx
S. no rough TeSpOnsa 1.0 bronchial auctloning
B. a pnea leat AKA apnea c:w.Uenge: nospontan~ou~ respirations D lifter diSCOM&L:!tion
&om ventHaloT (aases_ function or ln.duJla). Sioce elevating f'aC01lncrease.ll tCP
whl~h oould prec:lpi tate h<irn.i!ttion !tnd vuomotor ;n5tability. thi~ test ahould be,.....
IGrved fa, las~and only uled when the diagnosis of brain death;5 reasonably certain.
Guidelines" ·
1. PIICO, should be:> 60 mm He wiLhou~ reapiTation$ before apnea can be attributed
10 brain death {ifpatlent d06il Dot breathe by th ill point. they WOn'l brellthe at a
,.!le.o
....
'
.I.. no<e: EEG .. J!PI "'.1\11. 10'1..... ...... ,~_ntkd """""', ..... ~ .. . pop 16:1
B. Cl M ... I-rmp. ,heli. p. thw.y. ... r ' ..... in "' ... "
C. cornul ... ~.,~. d<lO,nllO ctl:I>O.1 lnaud . ..I1 . IIa"Lul.' ....
o .... pi"''''''''' ... dtr",od u abel"",,,,,,,] or <be" ~L<C\UII""" th., po'<IdLKf
IhIon r. . ny '1LLoe$"Gn • • ' p'n>moler "'.Y ~ conn"""" 10 II .. potkn,'
'"
9. Brain deaLh
.<Wq""'" tid.1 vatu",..; If
NEUROSURGeRY
2.
3.
4,
6,
6.
C. no
high". £'aC0 2; lIot valid with aevere COPD or CH F)
t.o prevent hypoulIlia durin/: the ~t'w:il.b. tho>.da.ngerQf cardiac- 8l'ThythmI~ or
myncardilll ,,,fa rtl;on),
p~e th! te!! with 16 minutes f>fwm tilation w ~th 100$ 0,
prinr!.Q th .. le!!t, a.;ljual the ventilator W bnng!.hl! PaCO, 1< ~ O mm H~ (to
~hOrWn lh~ teat time and t l!1.L8 reduo;:e th~ n.k of":lypoKemia)
during the len. hay., p!l8IIive O2 fi()w IIdmini5!.ered at 6 Umin through either II pediPirie-oxygen cannu\anrll No. H Frencll tracheal suctioncathcter
(witb tlleslde portCO\'end with altha.lve tape)p:lped r.o the estimated 1@~1
of the carillll
etllrtinl from nOmlOCRpnea , Ule aVeJ'lIge tim" to re8ch PaCO, '" 60 mm Hg is 6
miouteM (cl9S81~ tuelling is IhIIt raC~ rises 3 mm Hglmin, but ill act.uality lJtia
nne!! widely, with an average3. 7 2: 2.:1'; or 5.1 mm flr/min ifst.8rting III
normocarbia'j, Sometimes allong os 12 minutes 1Il1I)' bee necessary
the t.<'1;t aboJrted !»"emlltu",,'y if,
the pa.t;en: blllat hu: iOCODlpatiblf! with brain deflW
significant hypoterll!ian {)<:Curs
If0 2 uturation drOPfi below 80% (on pul!MI a>dmeter)
significant cardi"e arrbytlunias IICCUT
U' patient doea not breathe, lend ABC at regular intervals and "t tM complet.ion
often rl'gardl~u ofre!l.8On far ten;ainatian.lfthe pa tle.:lt doe3 nat breatM for at
least 2 minutes!l.lhr II P/ICO. > 60 mlf) Hg is doc:ulI>en:.ed, theo the tnt i8 valid
and ill compatible with brain death (irthe patiMt is steble and ABCs resull.!o Ir~
Ilvailll.blewithina few minute8, I.h~... pnea challenge may be IIOI'Itinued whiJewaitin\! for Tl'suJt8;n aase the PaCO. 'i C 60)
i fPaCO. atllbilii:es be low 60 wm Hg and tb@pOl rem"in.adequate,tryreducing
the plIIS!!ive ~ flow rDte .ligbtly
motor function
u.
""'~::?;~~~~':'i~J;:~~~:~post uring Of seilure8 afE, intODljl8tiblfl with !hOldi.
2.
I . :'
3.
o.
I.
•
Ii
.1
3.
<.
;
;
5.
6.
E.
I.
;
II
condition i,
a single valid brain
2.
NEUROSURGERY
9. SrIOio death
'"
3.
ifan in-eversibJe condi:ion ;1 well establiJibl'li Md no clinical confll"lllat.ory tntl
...... ..ed: 12 hou",
4. ifdiagnoosU i. ulll'Utain and nO clinic.1 confirmatory ~I.t: 12·24 bour.
5. if anoDe il\lul)' ill Uw! mu~oCb~ain deaLh: 24 hou", (may be . homned if ce.N·
tion of CBF ic demonllnted)
CLINICAL COtfARMATORY TESTS
CEREBIMI.. ANGIOGfY..PH'f
Crit.lria: at.ence orinlJ"atrallial now al the level o(the carotid bifurution or eircl.
of Willi,'). f"ill.i.al o£lbe supe rior "giual . inu.
0fX\U" in a delayed (a,hlon. lnt.lroblerv<!r validity hIS not Men . welied . NO!. routin.ly used in the diAlIlllllil ortx-ain dn lh,
but IJI~ ba emplO)'ed in difficllll . ilu.tio ....
IQ..,
EEG
ell! ~ do,", III bedlitl... R.eoqui... . .,;.nced int.lrpretar Don not del.a(:t brain.
• t.lm artivity. and elec\rocerebr.l.il.nce (ECS) d ... not oelude the pouiblUly 01 .....
venibl. coma. ThuI, I I leul a:..bmu:a ~rvillon if, n!()Ommendad in cortiUDc;tlon with
ECS, U.iDg RCS . . . cliniu] Ql)nUru'lltory t.I, t . lIould be doni only in pui. nu without
drug intoxication, hypoth~ru'li. , nr . hoek.
Definition of . leetl'O«lnbral all.nee 011 EEG: no elec:triwltCfiYl t)",. 211V with
th e following rtquirelDl!nt.l!
reeord inll'r<om ..ealp or ref. rential eh,,: lrod. pair. I 10 au apan
8 1C81p .Iectrodes and eat lobe Alr-renot electrodn
int.er-elec;trodt! relilt.a"ce '" 10,000 Q (or impedance <.6.000 0 ) but o.. er JOO 0
~n.itiv;t)' 012 \,Vlmm
time oont\.Mnl.l Il.S.0.4 lee for pan. orrecotditll
no rQpOn ... 14 , timuLi :PII;n, noi&e. ligh~)
.ec:ord '" 30 mini
ri!JM!lt EEG in doubtful ~o_
q".lified t.eo;:hnologi"U. lUld el~troencepbDlor... pher with leu EEG experience
telephone lJ"an.miuion not pe.rmiuible
TRANSCflANlAl DOPPLER'
t. IIn"U peAk , in early iystole withDUt di'itoli, flow
2.
fir reterbe.ating now (indica.
tiye of tlfnificanllj Inereased ICP)
i"iultl "bllence ofdnppler ,ignal. cannot be UIIM U cri!n"1a for brnin d~ath since
10'110 of palIon II do no~hl'" temporal lS()nPtion window!
CEREBRAL FVoD/ONUCLIDE .foNGIOGRAM (CRAG)
Can b, perfo.medllt the bed"lde with a general PllJ"PO'M! Kio tillatlon camera wIth a
low enerl,)' collimator. Ma.\' not det«l minima! blood flow 1.0 thl brain. esped,l]y b.min.
l!.em, the ... fo ... i.hwu:J. obsen·lltion in cortiunction with CRAG i. ~ed un.leu
there fa • clear etiology of o"erwhehnilll br.in irtiury (11.1. lnIlSlii .. e. helllorrh'g' o.r CSW),
May be ll.O~ruJ to conlinn dini;a) brnin death in the foHowinl"u.inp;
I . where complicating conditions are pNlSent, e.g. hypotherm ia. h)'pOleJaion
(e hoci<). drug intoxication
2 . ..,veN:' racial (numB where ~u lar findlnlllQ.lY bt difficult 01 con~lnl
3. in "",tienll with "'vere COPD or eHF when apnea teating mill"! not ~vRlid
"
1.0 s honAtl th~ observation Jl'l'.riod. " pt'Ciolly wheu organ don' lion i," poIIsibUi t)'
Technique
1 acintiUation came,. fa poIilioued /iI. lin AP heAd and nKk view
2. i~ 2Q..30 mGi of99",Tc·labeled _rum albumin or perte(:blletlt.e In a .. olum.
of 0.6--1.5 mllnto a proxlmlll lV pOrt,ora ~ntr.J Une, f<lllllWed by I SO 101 NS nU lh
3. perforut H ri,l dynawle JlDage. It 2 _1>11 inteJ"Y,I~ for. 60 JieCOnd,
4. then , ooLDJII , talit IUlagas with ~OO,OOO flOunlll ill AP afld Ihll" I.tera] "I..... lit 6,
16 .. SO minute. after lnjection
s . ,f a "udy need. 1.0 be ~t.ed beeaUH or. p .."",uI no,,-dla~tJc uudy nr ..
previOWI euDl inoomplltibll. with brain death, a period of 12 houn should I.P'I~
'"
9 Brlin death
NeUROSURGERY
Findings
No uptake ill brain pllni!oohyms
1I<lUow $kulJ phenomenon- (_ FilllJ.~ 9Termination ofcarolid circulation lit
the skull bass, lind lack ofupt.ake in the
ACA and MCA dislrlbution5 lab:lent ·oan·
""labrs efTect"), There may be delayed or
faint visua!i~ation of dural venous ,;nuIIlS
even with brain desthIJdufl to oonn""tions
betwf!f!n thfle~tnocr8nia l circulMtlon arid
the vanou s system .
E
n
SSEPs
BilAteral abseocaorN20,P22 re·
sponse with median "'Il'\'a stimulation,
ATROPINE
In bra in death, an amp ofatrop,n8 ( \
Oli) sbould not sITed. the hellr! rllte due w
the absence of "a gal t,;mel it normally in·
crease the heert rate). Although atropine
in usual dOM!! doolll>Ot ""use pupilllll")'
dililtation'''u, iti, prudent to '!)Carnine the
pupils first toeliminatl! uncertainty,
9.2.
Figure 9-1 "Hollow-.kull" algn on CRAG
ISLOIIc: AP _
W<enl~ .....".. .~.er IrIjecdon)
Brain death in children
Criteria for death : ;:'ravarsibla loss ofcardiopnlmonary or enUre b""in fUnction 18f1
in adult), but the (clinically unproven) auumption that (I child'S" brain it mor<! resilient
lllSul!. in ",ore difficult determination ofb",in death , The foll.,.... ;ng guidalin.s U1! propo6ed for Pflt;enlll -< 5 yra age'"
thesa re<:olllmendat;onB are not applicable for the prelllilture.lnfant
determination of proximate cause ofllOfIla Mould be made to ~lUIur. abRonte of
~medip.ble conditions: especially toxic and metabolic disordert, sedatives, para·
Iytics, hypotharmia, hypotension (for age), and su!Vically tNlltable conditions
criteria,
A, com" and ap nea must couist: includini complete loss of ron!lciousnau, vo·
UliUllion aod volitional ael,ivity
S. absence of brainstem function
1. midp<l8ition or fuUydijllled pupils, UMeIIl"",si"" to light (RIO drug ~f·
fect.!l )
2. EOM: ab8efl~ ofsponUln80IUI, doll's eyt!8 and calorie DlQYell'H!nts of
.,~
absence of buLbar mU8Cui.aUlte movement: including oropharyngeal
lind facial rnu~cll'll; absence of corneal, gag, \lOugh , $uck, lind r!lOting
reflex
4. llhoien"" of ro~pi ... tor:v movem0at (usually tl!;lted alter other erilens
met)
5. flacci d tone aod ahoieoceof5pont.aneoua or induced movemenUi (spinal
myoclonus and spinal \lOrd I.llOvemenu, e.g. renex withdrawlare not
included)
6. examination r""ulb should remll;n clllU"leZl~with brain death
t.hrllughout observation periOd
observation period~ according to age,
A. in nawborns born at or art.er term (:> 38 wks): 7 days
B , age 7 days · 2 m(llS: 2 l!Jl3mination.s and 2 EEGtl48 hn apll.r! {repeat ualn
unnOOl!5Sary ifcerehrnl rlldionuclide IIngiDgl"Bm (C RAG) (ai .. to y;suali ZOl
cerebralllI'tl!riesJ
C. ai" 2·12 nlll~: 2 ua..rninatiofUI and 2 EEGs 24 hn apart lr"peatexam unlJ<'<.
essary if CRAG negatiw)
O. ai"" 12 mO$: if irre"ersiblt \lOndit;",n ~~iBt~, labora\.Ory tesling is nnt nee·
3,
NEUROSURGERY
9. Brain death
'"
usary, and 12 ~n observat iOfl is sufficient (undesr conditions, especially
hypoxic· i&chemic encephalopathy, are difficult to assess, and 24 hra obser·
vat ion is suggested unless electroce.-.ebral s ilence Ofl EOO or a negative
CRAG confirm dillgllosis)
confinnatory test3:
A. EEG: standard .-.equin:'ment for 10cn, electrode distance<SU!X'llt 16n may
be decreased in proportion to site of bead
B. CRAG: applicability to patient" 2 mos age unproven
9.3.
Organ and tissue donation
State and federal laws require families of individuals satisfying criteria for brain
deatb to be approacbed a bout the po$sibility of organ donation. ~'acts that may be con·
veyed to family in order to help their understanding about orglln procurement:
1. any Or allauitable oTgaJl.S may be individually specified for donation or t.o be ududed from consideration for donation
2. organ procurement may be done in such a way as not to interfere with an open
casket funeral (Le. disfigurement can be avoided)
3. families tan receive infonnation lUi t.o tha ultimate use of any recovered orgaJlll
9.3.1.
Criteria for qualification for organ donation
Ge n era l el:(l lusio n ary criteria for organ donation (modified")
l. infection
A. un~ated septicemia
B. the following infectiona or oonditiOfla: AIDS. viral hepatitis. viral encepha·
litis. Guillain ·Bam ayndrome
C. current rv drug abuse
D. activeTB
2. malignancy: brain tumors represent JlOS8ible exceptioJl.S ('ff ~kIw)
3. relativeexelusions: chronlcuntreated HTN, hypotension (desired SBP> 100 with
normal CVP)
4 . dise_ of the organs coosidered for dOJ)ation
5. anencephalic newbom~ : recent consensus is that the functioning brainstem in
these inf8J1tJ; (e.g. spontaneous respirations) di9qualilie~ them froro the diagnosis
orbrain death (furthennora, few such organs would likely oonefit others)"
G uidelines for inclus ion (some recommendations from refe rence" included)
These guidelines are constantly being revised . in part due to '".proved results with
the use of cyclosporin in recipients. In general. consultation with. a transplant coordina·
wr ia recommended to determine appropriateness of donation .
1. brain death in a prev ,ously healthy individu~1
2. organs:
A. kidneys, age> 6 roO! (because oftize). Normal blood pressure, BllN.serum
creatinine & UlA. No S I..E (because ofposllible lupus nephritis)
8. heart and beartlluolr. ageideaily" 40 years for males and "45 for females
(above these ages. a cardiac catb i8 usually performed) but up to 60 yrs may
be used depending on condition of heart and potential recipienta). Euro by
cardiologist ind ,eating 00 heart disease (cardiomyopathy, valve defect. reo
duced ejection ('-""tion. severe ASHD. SIP CASG). No roDM
C. liver: age > I ".os. Nonnal hepatic fuTlCtion (nonnal Or acceptable AST,
ALT.I..DH, bilirubin (direct , indirect & total) 8J1d nonnal dotting studiea)
wit~ no history of liver disease
D. pan cre as: age 15 - 40 yrs . No history of disbetes. Nonnal serum glucose
and oroylase
3. tissues :
A . J:lI.m9!: age" 1 yr. Neither cancer oor sepsis di5Qu"lifiea (rabiea and
CreutzfeJdWakob disease are contraindications)
B. Din: "ge 15-65 yrs. E~c1uded if cancer
C. il®l::; age 15·65 yrs . E~duded if cllncer
D. bone marr!lw: age ~ 50 yrs
'"
9. Braindeath
NEUROSURGERY
E. hgart valves: age" 55 YI"II
9.3.2.
Organ donation in patients with brain lumors
Asnong patients with a hrai,n tumor:
1. those that al1llll!t tandidnIQ fOT O'l[1Ul donotlon :
A, meta"talk tumol'll to the b ra in
B. brain tumcr~ rnat hllve been manipulated (biop.sied Or I!:lcised )
C, p/ltienl..$ with br/lin tumor" who hlV(' been 6h..."ted
2. tholle thAt m;ghtbe candida~, but eonlide.eII higl,..",k donora'" indude
p,;p"IDtitd:
A. glioblaslOtnIl rtlultifonne
B. a naplastic astrocytoma
C meduUnblBllOmp
3, unmlln;pulpted tumors that might not be considered high nsk
A , henlsngiobiastnma
B, meningioma
u.nma:.
Optimally, ifno mela!l!.ll.seSOI1l seen on CT,chest, abdomM lind pelvie) And no meu
are found /It tune oforlClin procurem~nt, a brllin bioP"Y would beperfo,m"" II..fl&t Lhe 01"
gan , aTil procured li t the same anesthetic bnd the organs would not be ~ele3Sed' until
the biopsy prove... which of the 1I1x we o:IIU!gonl!.!l applle.s ,
9.3.3.
Management after brain death for organ donation
Note: OnCe b""i n dea th 0«Un. cardiovBlIC ular instability aventll.lly ensu e., genef'/Illy within 3·5 dayo, and management with preSSOI"ll; 8 u"ually requinod. Fl uid and elKtrolyte imballlnces from 10M of hYJIothalamk regulation mun be non:r"dl ~ed.ln eQme
instanrtlS a beating·beart cadaYH can be maintbined for months".
1. ~osent: mustbeobUlined from donor'. legal guardian. NB: mUlltala<) be obtaoin<!d
from nu:dical examiner'or coroner's office foraiJ cases under their jurisdktion (in
n'IOI! t 5tPU!S. death llISulting from accident, within 24 hI"! or hospitalization , ec.t'. )
2. ~iQ:ned noU! in chart filatingd3t.e And tim .. patient pronounOO<i bTlin deBd
3 , oontact traru;ph'f]tcoon!inator 3t earHe&t pn6Iible time
4, ween from yasoJll1!BIOTI ir possible, Control hypot.enail)(l t.l)cough yolum. upan·
Irion whenever I""uibl" (after brain dealh, A1)H p.oducliof] ""a",," , pl"D!;luclng di·
abetes ;Mlpiduft with high urine oulput, thU! ~pious tlilid ad.nunist.ratIOtl i6
BntidpaU!d (,. 25().500 mUbr 1$ common). MOAt cenU!rs [,refer AVO IDING l!lI:oge-
5.
nouo ADH (vasopreain (P;lreMin®J) if J1OSs1ble . ;nett th~ ri8k of renal s hutdown
increase!. i n brain·death
A. start with(:r)'l l alloid (05 V4 NS + 20 mEq KCIIL is gtntrally a good choke
a ln ce. it repl~teS frO!t' water}, replace urine t'C for « plu. 100 cdhr mainlA>.nance
B. un c>olloid IFrP, a lbumin .,,) if unabla to rnalnlem BP by replacement
C. UIIe V"Opruso ", if 8tiU hypotensive. Start with low dl'lSll dopmrn;ne, h~
c.... a~e u p to - 10 l'gikg/min, add dobutamine ,(still hypot.enS;VD at this d!l!le
O. If UO;s still,. 300 mUhr afte r above lIleaSUri!$, U!iC ADH anlliog ' aqUfOUli
v8llo prea:l i~ (Pitretl>in®J i. prefem!d over DOA VP to a void ren8J. hutdovm )
thyroslobulin given TV convertl50me cent from anaerobic to ,,~robic rneta\lolillm
which rnay h elp .. tav~ oll'CIlrdiDY3i1Ctlla. collapse
LABORATORY EVALUATION U
Gel)er a l iDitiallabll
I.
2,
3.
serology: VORL ~r RPR, H8&\(, HIV, CMV,ABO blood group, HLA tiS8ue Lype
dtellli,t.ry. eleclrolytes. gJUCOOle, BUN , ( reatilline, cal(iulII, phOllphate, liv~r f..."I:'
t ion t.ests, U/A ( unn~ D.nD!y~i$)
hematology: c ac , PTIP1"r
to"
A, h,fb ·rlok ."...ns ".1 b< OOlI.id<rtd
For I,,·., IntUIpl&l1\O in p" i.nt • .,ho .ro "''1 t_ "" the
U.ndul l.o "ii ... h<'P.I«t\l~I.r 'M~'
NEUROSURGERY
9, Brain deaLh
".
4.
microbiology: blood, urine II l1d sputum cul t ures; sputum Gram stain
Kid ney donor
l.
2.
in addition to general labs (s« (Zbo~). check BUN & creati nine ~ q day
check electrolytes ~ q 12 hrs (m!l(liry as appropriate )
Li ver do no r
l.
in adwtion to gene ral labs ("'eabo~), check LDH, AST, ALT. bilirubin (di rect. indirect, and tota l)
Heart don or
1.
aU require an echooardiagram prior to don alioo
9.4.
References
""......... Comm,..'" roo III< s..~1 of !;lll i<ooj
,
,.
..
,.
_ " " 10 M«I"I ..: C"jdoh ... rOt'~ "1r>1II;'
~.\6; 118H•. 1981 .
Qualroy S~. 5"1><"",,"",_ or <h< .. """"''''
...,.ooI< .. y of N<"tokIcY: 1'\W;1ic<~ .. I", de.
'....,; ...1 tIftIm"""" ,~0<I0 1.. (•• mm..,. ......
"",,,,). N< ... %c 'J: lOll". 19I1S.
Wodr<h E F": 0dem>i0I~ 110>.. _
.. ""'11 •.
N...""",," 45: lool-II. I99S.
a.~ .. I EC.O .... CO. _
"l A. ,,0/ ' Tho "I'nul<>ll""he .. ' ........ ionolln'n<le;nl>. J s ....
......... 71: 191". 1939
a._I EC.Mu.l\bltmJ !'.CotHa:! $ ... <>1" .. pne.
.... ,.. I", III< _ " " , .... orl:l<>in ",.,h. .!. """,.
,/icd """"""'.J N"''''''"'I 76: 1:»9·)1. 1m .
I... 1.1': Sp;1I.I1 ..11<><. ill ~ ""-"h.
'V 1): 6,.;).2. 197).
T""""I.!.. Ro'''.!.. Boj_ ".ki '" ..... Sp;n.of ......
• f .. , <Io<1..-., i"" of 110>," dealh . ~'-''11'''' 21:
m·)(lI.I99I .
L. V«kioJ' J.
I. " GI' l.ual'll$
"In and .... """
0 Ini ....... d
J S.u ...... " 71 : ... ~ .,1. 1989«_ "pori).
II.,.",.,. '" H. 1)..... 01 ...,........, ... ""'..........
br> .. __ pou,ru, . s. ... oIoc- H' 108\1·91. 1984.
J.. ' ........ I M S. Pow"" D. S..,.-d" I." ~t" Sponu·
"""". ol<><."bu .. ""''''''''' ''
<10<1... ,,,,,, 01
h. N"",,",u,,.,,. 19. 4-;'9·80. 199 1 (Iel·
fIMioo 01 .... ... . J"'M ..
t>r.,. ""..
GI-o<"".,
"",'"rio, ..
po'"''''
.fIe,
",'
'"
9 . Brain death
Tit.""" .. ofh,..,.....",.. • . M", ........ , 36: 116-7.
,~
"
.. RI .... ,.. t-l . o.p"'" 0 E.M""n.,.lC: S"",i.a! . I·
.. ' "",Ioo&«! h1p¢O~nni • • N El>aIJ 101«1 HO: 119.
"
Goc>dm>." J M.1l«1; Ll. M<:><m B o ,conr""",.,.
011n;,.0..1I1 wIlh 1IOf" '" _
.., """,,",' "
..... wof2G4_"',"" ....... N.. """..." 16:
'91·7,19U
0"",,"" J .l'nud I. Comparison .1 .... 0l."Il111 <1".
lecliOI"""";"_J!)'<"Of)'mof ... .. ill1 ''''' IV",.
""<lion . . . .. H, J .!. ....... b Sl: I80-S. 19tI .
Oo"u ine M O. Cntu ..... E: Sy""m .. """""'" 011",i.""" ... "",inl <onl,,,,, ....... ""'"' nco
r,,«f.,.., dil.,«1 pop;Is ... nB Emo<a M«I 10: '.1-7.
1991.
Tasl Felt« foo ...
olB";n O<><h i.
Q,;1cI ... • G"idol .... roo.he dtt<",,;,u._ oft><H>
d<>,h 'ft <~ ,IcI .. " . ArdI N.... 01 ..: ,n·l. 1987 .
D..-b)o 1 M.S .. ,. K.c.."Yil; .!..<loI""ppn>o<hlO
maoa,. ... '" or tho: h<&r\btI,,,,! 0l/na ...... . otpa
"
"
"""'<-of.
•• He,.."'
"
"
"
"
"
".
,~
<I.,..
0.""""'''''''"
cIcroOt. J...........
261 :n21 ·8 . 19~9 .
She..-""", I) .!..Co""", A M .fU<o<~ "" 1.<lGt.
The ..... f .... "'"'l""taIi< ",r."I,"
A
<ri'iqu< .J"M" 161. mHlI.I'lS ~.
a.m ... ;n I M. W..."" M. Sl ......... C 1.4 . <101.:
M....... I "',n "".'" ....r "",I""tod r.al ..",; • • 1.
Qb" .. GJ _oI7~ : 4l4-7. '919
"'p. _«u'
NEUROSURGERY
10.1.
General information
~Mbrospi.nal 0 ... ;<1 (CS F) aUm;lUIlda Lhe brain lind _pinal 001<1, and !lilly functi,,m
liS II shock 9bsorber ror the CNS. ll may 11150 storYe 9n lmmunoklgical fundion BllalQious
to !..he lymphattcsYlltem'. i lcircula.tes within the subarachnoid space. between tlleanch·
noid lind the pial membranes.
CSIi' is normally" d ..... coloillfflfl fluid wit.IL
~ 7.33-7.35.
Production
80%ofCSF ;8
for-9S~ (>fCSF
produ~
in the
....
--
s"""ific gr"y,ty of 1.007 lind
II
pH of
Table 10-1 Normal CSF production yolumea and prBB8Ure
prod"ted by the
choroid plel(uSi!$, 10catA!d in both Jat.e raJ
ventriclee (acoount.&
1\
P"",,,,
IO\aI voIUIII! (
ICl(lT1;IIion ral'!
.......
I 5
25nWd
."
•
,.,,'
H OYTl
ISO (50"1. inlritcta<llal, 50% sp8laI)
_ 0.3.(.3.5 mVmin (_ 'W-150 mVd]
mean: 10 BdIIIt: i·' 5 (". 18 YSUaIy abrIcN!NIQ
roormaI:. 15 young ~uII: . 18-20
choroid plnu""s)
(em o/nlid)
lind in thl! 4th ven·
tricle. Most ofth
as me .... JI.a I" tl>lllumbir .,..OQf.ch_ opac9 ...ttII1h. 111"01 ,. I . ~.a In t~.
rest of intrllcrania 1
"'leIal GeoJbolus posiTio(I
production O«UrBin
the in t.e rst.itial
SPl>Ce'. A $l!IaU III[IOunt lI\ay also be produced by the e pendyma l lioing oflhe ventrieles.
[n the spine, itis produood primarily in the dura orthe nerve root $leeve$, T,,(Jle JO-1
show.. properties o{CSF production, volumes Ilnd PTeiSureS.
Produdion rate:: In the adult, CSF is produced (It" rote orabou~O.3 mllmin (Re Table
/o.J). In tenus thMared lnicollyrelevlUlt, this lipproximate54SQ mlt.!4hn, which mU M
that in an adult, thJ, CSF i. ·~umed over' _ 3 times every day. The rate of fonnation is
inthf"lnd~"t orthe inlrac ranial pressure!{except in the limitinK ~ when lep beeomu
sg high that ce rebral hlood now is reduced').
Absorpt ion
CSF is ~bsorbed primarily by ~rachnoid vi lli (granulations) u,alext..nd Into the duo
ral venous linuses . Other s ites o[absorption include the-choroid plellUSf:. and lymphat.iC!;. The-rat.. of Bb50rpt;on is pr8S$ure dependent".
10.2.
CSF constituents
The cornpoiiition ofCSF differs lli,htly in the ventricles wb~re the
produced compared to the lurnbar5uooruhnoid spare.
rnajori~
of it ;.;
CELLULAR COMPONENT
In norm al adult CSF, there are 0-5)ymphocyus or mononuclear cell5 per mrn~, Bnd
polys (PMNs)or RBCs. ln the absenceofRBC., S· 10 WBCs pttr mm' is sUspicious,lInd
.,. ~O WBes per mrn 3 is definitel)' abnoTmal ,
110
NEUROSURGERY
10. CerebrospinalOuid
HI
CSF CONSTITUENTS
Tab" 10-2 CSF .01111•• II, ,.." ,
_ T_ _ _ "...,.5(0)
0111 ""'" T_ s., 01 "Ce_oo.p;n.l Flulclln 0iIN_ oil"" N _ Syatem' "" ~ A. F l - . M.O,
11orCEA.AfP.&~CG .
CI'*. w. 8.~Co., I'IIiItM:IeIpI'~.P""u_w;",~
--
_tiIoIpIa<mo
NoIe: CSfPfOl_ II ........ , in~ 1ILoicI,1wI1n....-..--.
_"""CSF_ns.s . ,
~_,...oI.In
... _
Ttbl.1004
.,
hble
1~4
CSF IIndlngs In varlOUII pathologIc conditions (ad ult vllu_)" (comlnued)
_,_iono OP
. _~ ~ :
Ine C6F!irlclir9t1ll n
__ IMI tJaciII .. _
I
... . _
. I . - . , , ; t ......
_ : ~. ~nItr
...
"""9a'"
CSF
...a......*olI
_ ••pIIl~_IIWr_U/ 1II~2!h1OlIo_.
1O~_Ir1_IICI~1tom
SAt1, eIto_
~
SAH __ ".......,.,'IA _
173
t "" ....... ~""\IIICSf' .. Io!S. _rMf1I51
TRAUMATIC r AP
D itre r e DtialillS' SAlI ITom traum Ati c tap
For typi~.l findmg5 in SAM. JU ~ 784. Some f'''l!.l m
W I from 'IT lire f howo in 7b~ 10-6.
NB: ""- candl!i<>r\s.CIaI' _
b~lpful
in difrerentiatiol!
oWI\fIoCIwomil
Differentioting tr1l e le ukocytollill l'rom tTlio umatie ta p
When many RaC. a nd WBC •• "" preo.en t In t he CSF d ue 1.0 a t raumatic lap ('rn,
It may be important to eell if' lhll wa C. ar. elev.~ or 'fthey are prl..,nt in the ......
OItio 81 in ~he penphenll hlood. In non-anemic patieDia. Ihlll'1l shou ld be - 1·2
(01'
every 1000 RBC. (alII. tonec:uon'" '''': l ubt' lIct 1 wac for livery 100 RBCIf .. '>II), In the
presence of .neroi. or n Opbltal l.ukDeylolllli......1 f'i.hmlLQ'. fCN'Olul. lI • ''',oo''n in
Bq IV. I toUtrmaUolhe origi nal WBC eountlo the CSF ~the TT.
wee.
I
.
~BCC:UOIUG/I...L . WklC ar -
NEUROSURGERY
WIICB!.OOD" R8CCSI'
-
-
I!q t e. t
RHC,t.OOO
m
where wnCCSf'O~ICI"AL
K
wnc lXIun~ in ~heCSF befall!-U\e 'IT, WTJCcs., &; RaCcst''' WIIC
& RBCcounts mellllured in theCSF, Dnd WBC8I.OOI)& RBC8l..OOO" WBC & RIIC ~r mm1
in the peripheml blood ,
Estimat ing tru e Lota l CSF protei n CO l:ltel:lt with a traumati c tap
If the hemogram lind peripheral protein are. normal. then hllve ~he c~11 count alld
pro\.e.in content run an th,urne Lube, and the IXIlTection is'I.""':
• 8ubtract 1 mg per 100 ml ofpro!ein far evel")'.1000 RBC per mm'
10.3.
Artificial CSF
II numberof famlulfttiOll8 ar "artificin l" CSF have hean Pl'1)posed OVer the yell1"8 in
(lrder to mon dOlely mImic the pH. ~l1lolarlty. COt, and membr."e a~tiv" ion roncen·
tration ofCSF . In many instance$, normal B8\.iDe (NS) 118.0 he~n used in brnin Burgary.
probably without ronijequlmre. How<!ver. renewed inwrut in the su~tofanmdal CSF
haa bHn brough t about by the use of neuroendoaropy, with poeIIible reaction . to non·
phy>liologlc ",,\utioo8 when large vQlume8 Qf n uid lire exchanged . 8B <>CCIII'II during 80me
Qr th~e procedLlres . An actu'" reliction t<I NS. however. has never been prQven.
In uddition t<I.irnlllatinr the eon s tituents DfCSF. it lIIIIy alao be wen to in sllre u
physiologic temp_t .....e c>fth~.oIl1lJon".
E Uio tt's solution
AKA Solution a or ElIiCK: lin d Jasper"· II. lin
used in the pRIlL
10.4.
eJaborli~
formulillion that WAS widely
CSF fistula
AKA CSF leak. Two major J;uogrOllp.l:
1.
ijPQO~DeoLl$:
rare \,rE~tow)
2. post- procedura or poettrau.ma tie (mare I.'Ol1lmon): 67·17\\1 orcases. Including ~I.­
transaphftnoidol sUlgery snl,! poet skull b8ge s urgeI")'. Subgroups,
A. immediate
B. delayed
CSF fistula should be BLlSpected in patient1! with otorrhea or rbmorrhea Bf\u head
trsum8. orin p~tient.C wfth recurrent menillgitis .
Possible routes of egress o f CS F
I.
2.
3.
4.
5
Ii.
1.
8.
9.
10
mastoid ait ~elll \u!'e<'ia llyaf\e. p-lOesa 8Urgery.e.g. forac:oustic neuroma (ANI .
'"' PDlJt 435 )
s phenoid air cells (""perisHy po!I(..u1.n9Bphenoidal sU'l!el")')
crlbrifornl plate/ethmoidal roof(Ooor of frontal fOSS.ll)
frontal air cells
hemialion into <!lIlpty sella and then into sphenoid liir a inu.
Rlong path or mtema! earlltid artery
Roae:nmOUer'a rONa: [OClltcdjllSl JnferiQr to CQverooLl • • inll' . IMY be I"'~ by
drilling off anterior clinoid_ t.o allow 3ccesa to ophthalmic lir'tery 3Jleu1)'sms
lito or the openiog oI'lhe tran,ieD~ latpral craniopharyngeal canal
percut8<U1OuBly through a ilurgical Or traumatic wound
j>1'trou~ ridge I). intenl.al auditory .,.,..al, fLlnowing tc'mporal bone fractUle or
acoustic neuroma ,"rgery (,u pag~ 435). 'Then either :
A. rbino .... bea: throllgh middle &Dr - e ust.achian l.ubli - nasopharynx
a . o to .... b e a: via perforawd tympanic mertlhran. - ellLernal auditory ean&!
T RAUMATIC FIST\l LA
Occur in 2-3'l> of all p8tienl.! with bead ;'I.1UI")'. 6O'lb <>ccur within days oftrallmli.
95% within 3 n,onthBU, 70% (of CIl$e;I oI'CSF rhjnOlTheo It.op withIn I wk, and uSLlally
within 6 mOl in the N5t . Non·traLlmatic fQeS cease apontlllleoualy L'I only 33%.
Adut~child tati" il 10;1. 1':Ilrf! beroN ago, 2 yn. AnO!lmJ.a is.eommon in trallmatic leaks
'"
10. Carebrospinal Ouid
NEUROSURGERY
(78~),
TIIN!;n sponLln.., ... " . Moet (8Q.85%) CS F otorrhu ceases in 5-10 days_
CSP liltull oecurred in 8.9% of 101 easel of pe netrating trauma, and intreases the
infection rat. over those penetrating injuries without fistu la (50% vs. 4 .6~)". It i$ reported to occur flO't·op in up to 30'l0 of eases of .kull·ban surge.,,".
SPONTANEOUS CSF FISTULA
Nontraumatic leaks primarily occur in adul", > 30 y .... Often inald iou5. May be mil_
""ken for allergic rhinitia. Unlike traumatic leaks. these tend to be intermittent. the
...... of 1mell i. ulu.lly prtHrved, an d pneumocephalus ia Wlcommon".
Sometimu lMOCilted wit h the following"
1. Igenesi. of the noor of the anterior faua (eribrifonn plate) or middle f _
2. empty leila . yndrome: prima." or poSt tranAphenoidal ,urp." (He poet 454)
S. increased ICP andlor hydrocepbalus
4. infection of the p8ranU81.intUles
5 . tumor: including pi t ui""ry adenomas (He p4fe 438), meningioma.
6. I pe ... il tent rtmna nt of th crlniopharyngeal ClInal"
7. AVM"
8 . dehiscenteofthe footplaLl of the ."'pes(a congenital Ibnonnality) which can produce CS F rhinorrh.. via the 11lItachian tube"
P08terior fossa
1.
2.
pediatric: usually preaents with either meningitl. or hearinc lou
A. preserved labyrinthine function (hearing and b.lanee): these ulually
prtsenl with meningitil. 3 ulull rolIteaofr.. tula:
1. facial ~llJlal: oan fistulize into middle ear
2. petromastoid canru: along path of arteriallupply to 111lI<:0II8 0( Olutoid
air sinuses
3. 11yr1I's f1.-Uft! (AKA tymp.nomenillpal f15l ure): Hnka p-fous to hy.
potympanum
B. Inom alies oflab,.-ri nth (hearing IcMt ): ona of ..vera I typea of Mundini dy._
plllSillS, usually pru'!'nting with rounded. labyrintw-:hlea ~hat per mi'"
CSF to erode through ova l or round willdow into auditory eIInll
adul t: u~ually pn'senbl wit h conductive hearing loe5 with sera... err.... ion, OleningiUI rolW n follo";ng an epi.sode ofotilis media ), OTOIIreb1ll1 aba<:esa . Occurs most
commonly through middle fOll&8. May be due to arachnoid granulationl erodi ng
into lir linus compartment
Spinal
Olkn pruenta with postura l headache associated with ned .tirrnea and
Io!ndem e5S" (He pogf /78).
MENI NGITIS IN CSF FISTULA
InciderlC$ with !»'ttraumltic CSF leak: 5--1~, i~ ulealr. peniata > 7 da)'L
Menln,giti.1t more common with aponl-aneoul fistula_ Ri$k may be highe r in poiSt- neurolurg'icil CSF fistula than in porit-traumaticdue toelevatad ICP comJllOn in la ller( fon:es
CSF outward). If.ile ofl",k uoidentir.ed prior 10 a t loompted .urgical treaunen ~ 3O'lodevelop. ~rftnt leak !»'l-oJI, wilh 5--154 ofth ..... .re.eloping meningit il! bero", leak is
stopped".
Meningi til may promolo! in1lammatorychangH at the l ite of the leak. with a r ... "I1.alit oeuation ofthelealL
Pneymoc;og:al menIngitis;' the IDOIt common pathogen (83'1> Of Cll$eS1O), mortali ty
1,lower than in pn.eumoo;oc:cal meningitil without unde rlying fistula « l~ VI. 50%).
poaibly becauH thelatlo!r il frequently leen in elde rly debili""ted patients. Prognosis in
children il WOrM".
EVALUATION
Dete rmining It rbinorTh ea o r otvrThe a i . due to a CSF fia tul a
1. ~h.racteriltka orthe nuid luggesting the preeence ofCSF
A. nuid illII dear al Wiler (Wlleulnfected Or admixed with blood)
B. fluid don not ~I"'H eltcoriat ion within or outllide the nose
NEUROSURGERY
10. C.rebTOllpioal nuid
C. pati,nte with r~inorrhea describe the t.R'U as l aity
D. collect nuid and obl.llin qUBntiLa ti"8,' u<:oee (urine rlueoM detection I trip:t
may be positive even with exceu mue ... ). Teat the n" Hi abortly .ner collection to roinillliu ferme nulion. Norma! CS F' IJluc_
30 m&"lo ( .. I ... lly
lower with meningiti l) wlMreaa lacrimal "cretions and muc ... are ul "ally
< 5 m~. A negative test i. ~ he lpful , ince it ruin out CSf" (ncept in
hypoel,.:orrhacbi a), but the .. il ' 4S· 16~ chance of r.IN poaitivet". ,.-,
E. BrtrllUlafe ITln: pr,..nl in C$ f', but at..enl in t ...... u llvB. nu,,1 exudatu
and IUUrn (except for newborns and patientl with liver diNu,)" ,", The
only othe r !IOun;e i. the ,,;t ffl(lU I nu id of the eye. Dfttec~ by p. atein elec-
i.,.
t.rophores;I, . 0..5 ml needll.o be
pl.~
in aluri le conla inu, packed in dry
ie., V1d .hip~ to a lab that can p4!rlorm thilstudy
F. "ri ng ' ign": when' CSF leak i. I Ulpe<:ttd but tho nuid i, blood tinged, allow the nuid to drip onto linen (Iheet or pillowcue). A ring of b]ood with.
I.rrercooeentric rina of dear nuid (-.;I CII lled "double rint' or haloaign) luaant. the PftSenH ofCSF. As! old. but unn!1iab]", sign
2.. r.diographic ,igne of"pneumocephalul on CT or akull ~·ray
3. cinemogram; intrathecal inJectiQl"l ofradionuc:lido trlcer followed by lein tigram
or il1jection of radiopt.que cont.rasl followed by CT lean (... ~ Mlowl
4 . atl(ll mia i, pre.enl in ~ $'lo ofCS F leaka
5. followina l kull ·baM "'1lI:ery (especially involving greate r l u;>erficial p<!t.rOllal
Mrve) there may be • p8eUdo-CS F rhlnorrbea pouibly due to na8l1 hyperse·
cretioo from imbalanc:ed aUl.<)nomic regulat ion of the n" al muc:osa" i""ilaterall.<)
the , u1ll:..-y. Often accompan ied by n ..alstuffiness and ,beent ipsilaterallacrimatiQl"l, and occasionally by facial flushing
TO LOCALIZE SITE OF CSF FISTIJI.A
~ of the time, localiu tion doe. not require water·aoluble co ntrast CT cistemogr'phy (WS-CTC) (_ bel(HD)
I. CT: to RIO hydl"O<'ephah.. and obstnH:tive n""plums. Indud" thin ~ cu ta
IIlrough anterior fOMS all the way back to the tella tu",iea
A. non-contrl5t (optional), to demonstrate bony anal.<)my
8. with lV o:ontrar.: l~alr. aite is usually associated with abnormal enha"",,·
ment of aoljacent brain parenchyma (possibly from inflammation)
2. ""ater-aoluble contrut CT ciitemogT1lphy (procedure of choice); _ below
3. pla in skullll·ray (hel pful in only 21 '!&)
4. older tests (abandoned in favor of above):
A. plu.rldire<;tional tomography: S3'!& yield. better in traumatic leau
8 . radionuclide et,teroograpby (RNC): may be uaefu! in ]eau too alow or
amall to MOW up on WS-CTC. Various radioactive a~nta have been uRd,
including: ndiaiod inate<l human terum albumin (RlHSA}I-'-", and 500 (.ICi
Indium'" DP'I'A. Cotton p]edaeta a~ packed inttlnually lanterior naul
roof, posterior nan ] roof, sphenoethmoida] reee.a. ",iddle m ~atu,. and p0sterior floor of the nOli) and arw roarked 10 that their location ia known . Ra·
diotrao!! r il then iJ:Ue<:te<I int .... the.:ally Ul ually by lumbar puncture. Scans
are performed in lal.e.al, AP and posterior view . A pl"'OtOCOl .... inaln'"
DTPA is to obtain a SCIn ahortly afUr il\iec:tion. At 4 noun! post ·i l\iection,
th~ SCIOn il re~ted. and 0.5 ml of blood is drawn (to raeNure llrum activity), and Ill" pl~d&"ta are removed. The p]edaets ani then individually
placed in a welkou nl.er and a ratio;' calculated (or pledget radioactivity
..dativ. to ",rum. A ratio " 1.3 ia nonna] , and a rat io > 1.3 ,ulI"ta leak . If
no le~k , the no. can be repacked and the study repea:.ed the following
mom ,na·
Leak. into fron tal sinul will ampt.y into nllOpharyu anterior I.<) the middle
contha , unlike leak. throuah cribrirorm plate. RN C identifies the .ita in
only 5O'A-. May be milleading" with pouible contamination afU r M veral
OOUnl (rom ablorption o( rad ioilOtope into the bloodstream and accwm,l ,.
tion in the muOOP] /danda ofthe turbinatot. Patient ~itionina mly ~
COQtaroinate other pled~ta
C. intrathe<;l] (.. i" ble) dye I tudin, some luoeIII witb indiao aormine or Ouoreacein (1ft PfJII' 699) witb little or no complicatlons (II methyLene blue il
neu rol.<)";c and should not IN used, _ PQlt 599)
5. MRl : ha. litt.le to offer in Jocalilation of"CSF fi. tula 00 below)
'"
10. Cerebroepina] fluid
NEUROSURGERY
WATER-SOLUBLE CONTRAST CT CISTERNOGRAPHY
nu. te$~ i. perfQrmNl lf:
no l ite. identlfied j:1n pla in CT (with coronals)
when patient is leakinlC clinically (the. aite 15 only 5Qmetim .... identified in the absence of an active leakl
3. when m\l.ltiple bony d,,(ecu art! ident;(ied. and it i. enential to determine which
site is actively leakine
4. if a bony defect SlOen on pla;n CT does not have associa~ chan~ ofahnormal
enhaocement_o( adJacent brain parench)'IQa
Prot~u .... ofrhol~.
L
2.
Tecbnique""
Use iohe~ol lue pu.je 127, which hill! geoerally replaced metriuom ide S. 7 mt or 190220 mp] ) [njerted iOl<llumbar 8uoorechnoid space via 22 K8uKe ,piruol n~le ( or 5 ml
via CI-2 punc~u",). Patienl positioned in -70" 'l'rendelenburg _ 3 min prone with nee).
gently n""ed. in CT t.hey .rekept p[lme with head hypereKtended wi~h I> mmcoronal cuts
with 3 mm overlap (U6" 1.0 IOIJl CUtii if necessary). May n...ed provocative. maneuvers
(coron al llCIII"\8 prone {brow up) or in position o(lellk, iotratilecall8l inei.n.fu.sion (requirea
Harvard pump)'·" .)
Look for aCC\Jm ll l~tiQn ofconLrast in air sinuses. Apparentdi5conLinuity ofbone on
CT without extraV8$S8tbn of contrast ;. probably not the ~ite of leakpge (boRe_diseootinuities may be mimicked by partial Yolume ll'·f.r~ging on CT).
MRI
MRJ pro..-ides little additional informa!'!on for IOC/Ili:wtion , but it CStn RIO I>"fo""l1
mo:;.s , tumor, and elllpty3e1!~ bo!tter than CT. Both CT and MRl C"IIn RIO hydrocephalll6.
TREATMENT
AcutA!ly a~r traum8. ObuNation ia jWltilied as IIIos1 fa ....8 ceo"'losp"[ltatll!Oualy.
Propbylactic anti bioti C8: Con tro~ersial . There w;;u no differencc io !.he incidenfe Or
n)Orbidlty ofllleningltia between trtlMed o.nd untreat«! patients"', Furthermore, the ,;~k
of8~lectiug reaistaolst.ra ins sppeal"l real" and i3 thoenrorflll8ulllJy avoided .
FOR PERSISTErff POS17RAUW.rJC OR POST·OP LEAKS
NOll -s urgi ca l trea tllle llt.
I. rnellsures t.o low~r ICP;
2.
A. bed retlt ; although recumtMtncy may am eliorllte SYrQptom l, !.here i~ no other
benefit froro bed rest'"'
B. avoid atrair,ing(stoolsof\enel"l) and avoirl blowing nOlle.
C. aeet.a:u>laIOlde (260 mg PO QrD) t.o /"l!dUCf! CSF pN>dudioll
D. modest nu;d A$tridion (eaution po<It-tr;msaphenoidal becau8<!- of pouible
DI ('~l pag~ 16); 1500 mllday in odultli, 75% of rn>rintA!nRnwday in peds
If leak ptr8istli (c)ution: firs t RIO obstructiv~ hydrotephlllus with CT or MRl )
A. LP : q d to eJ'D Oower prt!$Sun! to nUr atm.osphen c or until HlA)
OR
3.
B. continuous JumblU" drn..in.age (C LOt via percutaneous catheter. Ke-ep
HOB el""al.<:d 10-15" ,."d drip ch8lllber "l shoulder le"",1 (,;4ju8t down if
leak pil .... iatli). RequIres leu mouitoring. Irpatient oeUlrioratQ with dr"in
in place: illlmedi awJy st(Jpdrainage. place patien~llat in bed ~or !light fun·
~lenburg), st.art 100% 0 •. ge~ CT or bedsideCTOEsH lible .kull x-ray\to RIO
tension poeumocephalu8 due. to drawing in orait)
lurgkal treatment in persistent cases (...-e below )
SURGICAL mEATMENT
ind ica tions ro r
8lU"gh~al
1.
CSF leak
2.
leaks
3.
inte rve n tion
h
P e trou a bone
May ptellent 1111 otorrhea or 8S rhi noIThea (via the Imstachilm tube ).
NEUROSURGERY
measures
!U r gety: UIIU_
po,.,
1.
following poat.erior {()$.'ja ~u r g1!ry: IIf'e
435 for treatmen t following aco.>ustic
neuroma eurgery
2. following mastoid fractures: may be approached via extensi,·" mastoidectomy"
Leaks thr ough c ribrifo nro
pla t~/ethmoi da1
roof
Extradura l fl pproacb: Gi! neralJy preferred by ENTlurge0n3"' . lfa frontal craoiotomy
is being performed. an intnadural approach should be used ,ince problems may M$e In
dissecting the dura olfofthe floor oftbe frontal fossa, wherein the dura almost slwllY~
tea", and then it is dilTtcult to know if an identified tear is the cause of the leak or ifit is
iatrogenic. Fluorescein dye m;"ed with CSF injected intrathecally may helpdemomtrate
the leak intraoper8tivelyICAIITION: must be diluted to red uce risk ofsei.ures, see pog~
599).
Intradural approach: Generally the procedure of choice". If the fistula site is uniden·
tified preoperatively. use II bifrontal bone nap.
General techniques of intradural approach :
Post op: lumbar drain after craniotomy is eontrove"'ial. Some reel CSF preuurt
may help enhance the seal". Ifuserl, place the drip chamber a t the level of shoulde r for
3·5 days (for precautions. $ff COOtie).
Conside r shunt (LP Or VP) if elevated ICP Or hydrO)a'!phaiua is demonstrated.
Leak s io to s pbe noid ,;null (incl uding post-tranllllp be noidai a urgery leak)
I.
2.
3.
LP BID or C!..D, as long as pressure" ISO mm H~O or CSF ¥anthochromie
A. ifleak persist$ " 3 days: repack sphenoid sinus pnd pterygoid recesses with
fat. muscle. cartilage Mdfor fascia lata (must reconstruct floor of sella,
packing alone i$ inadequate). Some recommend against muscle sin.::e it putrelles lind shrinks. Continue LP or CLO as above for 3·5 days post-op
Il if leak persists ,. 5 days: lumboperitoneal shunt (first RIO obstructive hydrocephlllus)
mOte difficult surgical approach: intracranial {intradu rall approach to medial fI9peet of middle cranial fossa
consider transnaspl..,llar injection of fibrin glue under local anesthl!$ia"
10.5.
Spontaneous intracranial hypotension
The syndrome of spont aneous intracranial hypotension is cha racterized by the fol·
lowing in the a.brwlg; of antecedent trauma or LP (or epidural injection ... "':
1. orthosta t ic headache
2. low CSF pressure
3. diffuse pachymeningeal eohancement on cerebral MRI
In most cases, the underlying etiology is thought to be II sponlan eousCSF leak from
a spinal meningeal diverticulum or dural tea r".
Clinical features
Most patients have orthostatic hel>dache. Atypical patients bave been described
withcu.t lilA , or HlA tbat i$ !)On_pOiIitional, without pa.;hymeninll:e.. l enhancement on
MRl", with dinicalaigns of encephalopathy, cervical myelopathy, Or parkinsonism".
Sinti! some plltients roay have normal intracranial preuuTe. the term ·CSF hYJlD"olemia" has beeo suggested'". MRI evidence of brain df!S<'enl oceurred in 36%"'. and reyenl!ible pi tu itary enla rgem~nt with a eonvu superior margin" may also be . een .
Subdural bematomas may occur as a result. Radioisotope ciste.oography was abnonDal
io 90%, and showed 8 leak in 40%".
Treatment
l'reatment includes:
1. bed rest
2. analgesics
3. hydration
4. epidural blood ""t.ch (EDP) for appropriate cases:"" poge 46
Outcome
Complete resolution ofHlA was pchieYed in 70%, and was higher in patients ,""ceiy.
ing EBP, and W illi lower in patients with multiple .ites ofCSF leak".
'"~
]0. Cerebrospioal fluid
NEUROSURGERY
10.6.
,.
,.
,
References
, _01_.,.._CSI'~
. _ I t T: CSF_I..;u, . .. pIIo>i< .. ~
10 ......
~
_
eo>iI, .... ....,n.... _ no .... Ur
n.-t J l ' ·191·'. I991.
E>. ... ~ _ _ '"
-
s-O.II< .... JEA
~"" Iloid. '''''N<", ' 9 U~$. 1961
....
\..cnoI ... A \I . . . . I. r; . ~(l\l . hJ.o """"'"
_ _ _.
bo1_ft~n.",
....-;,,-~""""'.,.......
'<nO.
, ).
" ...1ri........ CT c~, J J<i... __ •
•
"u .
679-91,
IknII&EA.S.... O' H~· c-F· .. b·
'. _ ....
_ ~ 01-,.....""
,~
Grilf.~
118. 1...".,.... ... 8: no. .... _ol<lMiII·
-lIy4oo<tpNIIII", ......". ,.................
..... ""'r..... ~""'- .... fIoiol porlu1...
N.......... tt 4, 9S<IOO.I990.
• u.. ..
,. Ft.,........,
I. J
1910.
••
••
00.
"
".
".
"
"
..
"
"
".
W. I , S_.I'II;'",,"IfIIIIt..
'1lC
1(; """","
lnII ................. n.",
.....,... ..... KM.W.."'_.... Jl II~ ,I"• •
Oh K. Y_ _ M.!<IoooIUT . . . . _ n.. ...,..r~
CIIOC< d ... ,r"Io' .... -,;011 0."' .. perf.....
I .... ' - O . .u,,..-,.l'I<u..........., ll: 1ll-6.
,....
Ell ... K "'C , J..I'O' H II. PII.!.iDIop<OI .. II ..... •
,i... r", ... 01 • • .....,: 51""ia of 10<" pH _";"
..... 1"'><Iic!M I9l1ooff<rood ....... burr...... itooorI ..
......i.... J N• • •_ •• 6: I.oG-Sl. 1,.9
1...0"" MC. E'I;", K ... C: a .......... of .. ... if!·
<i.ol ",,_p"'! nul6. J N....", ••• 1: ~.
19$0.
51"'.1<' MF.b_llI! 1 M:
! n•• d
r...ull.Ca.u ... ~ N...........: 1·1. 1986.
M....n. C.C.ll<rin P. Sabol D, II .t.' Of mi_ ·
.....: f._".01 ..... .,1", ....,;-<;"• ...,....""'.
AJNM1 15-.10. 19111
Mo .... .,.,y A M.C. ....... W F. !'>oltonJ D• .,al.:
O F n"ul •• <ompl;'OI i", ",,, •• 1< w ...... of ,Ire
broi. , J N.u' ....... S4: """.191 1
C¥."".""M D.S<AIo.a, I. N. ~ .. ""I
(1uOI.ho_. J N............. 80.
1994
C ........... TCC#Tt~._ . I.()oo.
...,.....,aov.Ero&lilllG M./... .).I.ipp;...,.,.R....,.
PI!;Io<k.,..... 1991. YoI. 1, Ooopr .. )1: PI' 1·7.
l'I.. k;....!<: . .... o.Ft<>D R. K-'" R 1. .. ", _ Ce~
_11'Iui<j rIIl-nocI .. . _""'.,. 01 pi<l>....,. _
1"<00...........,6: 191-1.1980.
_ W_H: C-....,...I
"',......
-=Tlo<_y
or_UK
_
of ......
aIron
.... _
f........ _
publiobed .i_
rood.
...... OIoItoryq<lllS: 1m. 1926.
SdW ...... W I. Mol'<' F B....... _ I 1. 0 ...."
Spa-. .piMI~ noi<! ~ ....s;"..
..........11o)"'*"""".J I ' I _.. "':~.
Cue....,.....
u-»,
""1«0 .......
,~.
_
... T P.-...CJ. Pftoo: ... _Io<.I"..
NEUROSURGERY
1..$_''''
~M<wrioI
1.. M_ 7l.Uf.1~ . 1 91(1
W;!Mn ~ H. .......NIr)' u.(e6\,J:_
.......,.. McGoow·HiU. Ne_ v..... ItlS.
",,_ItO ......
1)·.... G._H41: .~t) .... u.tf-..
oI .. _ _ _ .. II>t_oI,... twoop.
J~
" - . r.s...... c IJooI. n... •..,.C. .. ... Hjply
..... "; ~""""""" ot ...... l~ .. _
" __ ... -..roo-.-.-..
• • ...... CIIo
~
'CSF) ....... AcUN.. _I09: .... IO I. I99I .
OI:Io.-. : R........,.. ~.o(_ .
1'1"' ..... 1( ... ,C.m'..pI .... n"", 11>_01
r ...... <l_~
H. . '"
....71Ul·".991.
","" ...... ...,...'.. _ "ju"
.. w(do;n
'M"""br" ..... ,..,Ie>.JNno, ..... lIl: I@4J.
U111.-.. _
n.
~
.
aioI41. 1f-l', ' '1n.
",_1. WoW to! H.$<&III II D,''''' " E..........
oICSF.,.;_ ..,..n..-cr'...._
fill) N~ I6:S4-60. I "' .
1: ........., I.Sodt.... "' .II<i/Iooy<J: A~
Pf'
OP'I,Iu,,"
"'*"""" "'_
A_
bI...! >Il0l,. 50 ... No."oI" I II .... 1m.
pIII01a ....
n.
.-._Clftf.....-
AIIt.C.CiIauooo P•.,.._C lleiloeu; ... _ _
".ul......r..1 .........
.... l..-m lS4: , 229-)). ,999.
•
Cok-.. TC E.H.ruioI_ol....-."...
N.
Low;"W : ~fIoId_"<_
"
D~
- . . . . . " .. 0001
""
_
".
U.
RIMMI~
joJ..n... II J ~ 11: 1·1I. 19S0 .
TF.Geotco ED' SortrbI _ _ _ ",,,,,·
_<"'~jhJJ/i_ . I. ~
.. _
""""'rpcall«.h....... s.r:_tHH_S_W
H.ledo.). W.8.
I'Io<1I<I<lp!lol .1"' ... ..
199'.Yoll: ppI Jl·ll
Fujii T. Mi ...... S.Onod.I K... III" SioRpIo .......
MO" ofCSF , . " , _ oft.. JO"'''"'Y ""J<r)'. 50..
Ntu. oI 16: :WS·I.I986.
f;_RA.o;lI.. wP.O""I _ _
s.........
",.. brol displ>«m<m""""" .. iona_ 1oJ_ _ . Nt.roIoK) 4). 110'1-1 1. 1991.
Sr:Io ..""'.W l.T_.it J: - ....... ")'J'<IICMiooo
.. ~ ""'" _.q ..I - . , .... ....,...., '"""
. , _ ;"", • •• ,. j Nt"'-'I 91: (1'·1, XIOO
"
". ""'"
n.
19. 101-16•
«_
Clouo'SJ.)(imIS ..... M C: Sy_or-.brol
.p;n.1nu'" ~JPI>"O-' : Cli . ...1_ i","- r..•
ou_. I'1 ... ......,. ss: In l.1. :IOOO.
MoO.rI l : Spero ........ , .... t>n:oopiool r..1d 1<&1< ••
f,.,,,, io ........ ;aI ~, por..,.;.,., ...... bfoopI ... nulll
.I!,,>,'Ol<mil' F._o!w.. o r .~ . M. ro 0 •
1'>0< 10: Illl_ll . 111'99 •
... I...... tint" I.
J. lkrI...·t.- J... ~"
Pi"",,,,, .111 ......... ;" ,..1..,...."" ......... i.ol
N... ,oioU S,: It9S·7.
'"ta .....
-.
Ei<"_
". Itl_"'_"_
10. Cf:rebl"Ol'pinal nuid
,,,
.,
·
.,.
~
.
-
,
..
~
,..'
EPIDEMIOLOGY
E$tlmat.ed pre~aleMe' l -l .5'l!t.
Incidence of congenit.lll hyd rouphalus ;._ 0.9-LB/lOOO birth. (re ported range from
0.2 \.113.511000 birth.'),
FUNCTION.t.L CLASSIFICATION
Two main tunc tional s ubdivi llioDsorbydrocepbalulI (Hep)
I. ob~trud;ve (AKA lIon-conlmunicating): block prol<imol \.II the arachnoid gTIUlUlatlonil (AGJ. On CT Or MRI : enlargement or~entridell ptoltlffiSl \.II block (e.,. ob. truction ofaquwuct ofSylviua _ lateraland 3rd vMtric:ullU"enlargeme lltoutof
proportion to the 4th V61tride, ~metimetl referred to al triventocular hydrocephalUs)
2. eomm unit::"tlng IAKA non-obatruct.;vel: CSF cireulation blocked:)1 level of AO
SPECI.t.L FORMS OF HI'DROCEPH.t.LUS
1. tollditions that are n;)t actually !;rue hydrocephalus
.t.. h ydroeeph lllua e" vacuo: enlargement orthe ventricles due \.111085 ofce-rebral t.I~ue \cer<!brsl Btr"Ophyl, ... , ... aUy IS a funct ion ;)fnonnalaging, but
accelerated or !\ccentuated by olutain disease prOce&llU (e.g. Ahheimet's
disease. CreutzfeldWllkob)
8. otitic hyd~phah>s: obsolete tenu u!i«l to describe the Increll!led intraocronial pressuNi stell in patients with otitis media (see seeJdiopoli,.ic inlraen:a '
nkll "Y{lfnell~ion, pace 493)
C. external hydroc~phal .... :,.,.. poll" 181
O. hydranlmcephaly: lei! b<./aw
2. normp) preSllure hydr ouphalu8" (NPH): $ft ~ 199
3. entrapped fourth ""ntride: sn pa~ 182
4. arrested hydrtlCl'phaiu8' 1ft PrIfJ' 181
HYDFlANEN(;EPHAL Y
A pt>.Sl·ne urulation deffO:t isuptlge. 112). Total or ne...·\<It.al ab.'lence orthe C('rebrulu
(small band.!:r of cerebrum may be consi$\.I'nt wilh the diBgnosi$'), with intatt cranial
vault end men;nlleS, the intracranial cavity beinll rill.,d with CSF. 'I'l,.,r., ill. usually p ......
gr-essive matfWl"a nia , but head site may be normp! (especinlly At birth ), and, occllllional·
ty , microcephaly may oc~ur. Facial d,...morphlSm i8 TIl,"",.
MllY be due \.II II variety of causes, tbe most commonly cited is billlteral ICA infarcts
(which rfault";,, .boen"" ,,(brain ti8_ supplied hy th. anterior and middl .. "" ....1>....1 .. r·
teries with prnerv&tiollln the distribution orthe PCA). May also be due to infection (congenital Or neonatal herpe&, to""pllt8mllilis, equine viro8).
Lesa affected infants may. appe8f nonual at birth. butllJ""ll oAen hyperirritable and
retain primiti~e ~nex"" (Moto, grasp, and ste pping ",flex) beyond 6 mo. They rarely
prolfl"t!!ls beyon d spon taneo.. vowel produdion and social ~ miling. Sei~W"e!I arecomrnon .
Progr<!uive e nlargem ent "rCSF apace' mil,)' oecu' which tan milllie HVere ("maxi·
mal") hydto.;ephelu, (HC P j. l tiacrilica.l todifT.,rentist<! the two aince tnlt! HCP may be
treated by ahunting which may product! .orne re-t!1<J)Msion of the cortical mlln~le..
Many mean8 to di li tingui.'lh hydrnnencephaly lind HCPhave been descnbo>d , and j"dude:
1. E£G , $ho w.! no ~'1I1iC1llactivity ,n hydraneneephaly lmuima] HCP typically produces lin abnormal EEG, but background activity wUl bE presenl throughout the.
brain'l) and i. one of the be!;t way . to diffe .... ntiate the lwo
2 (;T). ~, MRJ Or ull1"UOund: mojo";ty of mtrlloranial space i8 occupied by CSF.
U5ually do not see front al lobE ... o. rmn~l horns of lllteral vl'ntricleB (there may
be remn.nts oftempcTII I. DCc ipiUlI Or lubfmnw corte..l. A , (nJcl ... re ton,istl ng of
'"
II Hyd""'ephalu,
NEUROSURGERY
bra iD$tem aodule (r(lundd thalamic roas$es. hypothalamu s) and medial ocelpitallobes sittingc)O the tentorium oeeupie. & midline position . urrounded byCSF.
Posterior f\lS5a structures are grossly intact. The falx is usually intact (unlike alobar hoioprosencephaly), and is not thickened, but may he. displa~ laterslly. In
Hep, some cort~aJ mantle i, usually identifiable
3. trilDsillumln a li o D of the skull: Ii hydroc<lpha[jc bead ordinarily does not IranaiJluminate unless the patient is < 9 mos old Bnd thfl cortical mantle under the
light source is < 1 em thick " ' ''~' or ifflllid displace!! the oortex inward (e.g. subdUTaI effusions). Too nOllspecific to be very helpful
4. angiOIP'''phy: in "claS$;c· cases resulting from bilate~J l eA D<:<:iusion , no flow
through supraclinoid carotids and a normal posterior circulati<.1n i, expected
Tre atment
Shunting may be pen'mne<! to control head size. but unlike the C8!;e with
hydnxeph alU8, there is no restitution of the o;:erebral mantle ,
m""im~l
E XTERNAL HYDROCEPHALUS (AKA BENIGN EXTERNAL HYDROCEPHALUS)
T Key features
• enla~ed subar8chnoid spaces over th front.al poles in the first year orlife
• ventncles are normal Or lI1inimally enlarged
, • may It.. distingui$hed froOl subdural hematoma by tbe~cortical vein sign"
• usuaUy resolves spontaneously hy 2 yealO of age
Enlarged Dubarachnoid space (usually Over the cortical sulci of the frontal poles)
seen in infancy (primarily in the first year of life) usually aOX<lmpa nied by abnormally in·
crelllling head cirrumference with n01'1lUl1 or OIildly dil ated ventricles' . There are ollen
enlarged basal eis terns and widening of the anterior interhemispheric fissure . No other
symptoms or signs should be pre:rent (a lthough there OIay be sight del ay only in motor
milestones due to the large head). Etiology is unclear, hut a defeet in CSF resorption is
postulated. External hydrocephalus (EHJ may be a variant of communicating
hydrocephalus'. No predisposing factor may be found in some cases, although EH lI1ay
he associated with SOme craniosynostoses' (especially plagiocephaly) Or it may follow in.
traventricular hemorrhage Or superior vena cava obstruction.
Diffe r e nti al diagnosis; EH is prohahlydistinct from benirn ,"bdural co!!«tiqns(or ex·
tra.axial flu id ) ofin(ancy ( Xt past 678). EH must be distinguished from symptomatic
chronic extra.axial fluid collections (or chronic subdu ral hematoma). which may be DC,
complltlied by seitures, vomi t ing. head~cht ... (sw pas~ 678) and may be th e result of
child abuse. With EH. MRI orCT may demonstrate cortical veins extending from the sur·
faceofthe brain to the inner table ofthe.ku!! counoingthrough the fluid collllCtion ("C(lr ·
tical ve in sign"), whereas th e oolle.o-tion. in suhdural hematomas compress the
s ubarachnoid space which apposes the veins to the urlace to the hrai"" ".
*
Trea tmen t: EH usuallycompen$llte$ by 12· 18 mM agewithouuhunting". Recommend:
follow serial ultrasound and/or CT to rule Out abnormal wmtricular enlargemenL Em_
phashe to parents that :his does Il21 represent cortical atrophy . Due to increased ris k for
positional molding. parents may nBOO to reposition the head w/tjle the child is Bleeping".
A shunt may rarely It.. indicated when the collections are hloo<ly (consider the pos.
sibility ofcltild abuse) or for «<metic reasons for severe macro::rania or frontsl h.o$Sing.
"ARRESTEO
HYOROC£PHAlU5~
The exact definition orthis term is not generally agreed upon, and some use the
ter m comperuoated bydrocepbalus interehangeably. M()/It clinici ans Ul!e these tenns
to refer to a situation where there is no progression or deleterious sequelae due to hydroo;:epbalus that wouJd req uire the p""",nce ora CSF shunt. Pati~nts and families should
he advised to 8~k medical attention if they develop symptoms of intracranial hyperten .
sion (decompensation): headaches. vomiting, 9t.a><ia or visual symptoms".
Arrested hydrocephalus sat isfies the following criteria in the absence ofa CSF shunt:
1. near nonnal ventricular size
2. normal bead gr<lwth ClIrva
3. continued P6ycbDmotor development
Shunt independence
The concept of becoming independent ofa shunt i$ not universally accepted" . Some
feel that shunt independence occurs mOre commonly when the HCP is due to a block at
the level ofth e arachnoid granulations (communicat ing hydrocephalu s)" , but otherR
NEUROSURGERY
II. Hydnxephalus
'"
hlVe l hown Ihat ;1 Qln occur rq:a rdleuoftha elio10gy". These p, ti""'- must be followed
dOHly .. there ar .. reporta of dellth u late .. 5 years al\.er app..en t shunt independence,
somet;me.. without warning".
Wh en to remOve a di sco nn ec ted or n on-fu nctioning s bunt?
Noc..: a dia<:onne<:ted , hullt may con t ioue to fu nction by CSt' l10w t h ro ugh a l Ube ... ·
t.aneouilibroul traCI . Reeornmendationl on whether Or not to repai r "". remove I d iKon·
ntete-<! or non·ruMtion;n, . h unt :
1. when in lIoubt. I hunt
2. lndiutionl for shunt re pai r (VI. removal)
A. marginally functioning . hWlu
B. the prese Dce of IIny .ign. Or .ymptOm, ofin~r.a.ed lCP (Yomil;ng, uPiale
palsy, IIOmet i.mel lilA .10ne ..... )
C. change. in eogn,tive fu~ljon, I atteotion span, or emoUon. 1 thanl"
O. patle nta with. aqueducullf.enOli. or .pioa binda: mosta rt! Ihuntdependent
3. beca U.!oi! of rlab al!lOC:iaud with , hWlt removal, IU'1e ". for thi. pu..-pote alone
shou ld be perfo nned only in the . ituation or. ,hu nt inft-Ction"
4. patients with a nonfun~tionin, . hunt I hould be followed dOHly with ten,1 CT••
and possibly with lienal neuropsychologiQlI eVlllualion.
ENTRAPPED FOURTH VEWTRICL E
AKA isolated fourth ventricle, al the name implies, i. a 4th ven!.riele that neither
oommunica\es with t he 3rd venlriele (through lhe Iylvian aqueduct) nor with the ~.. l
cisterns (th rough the foramina of l.u&chka or Ma~ndie ). UlJ\lally ~ with chronic
shunting of th e latera l v~ntricles, especially with poIt.-in ftel iou, hydrocephalul (especiaily funga nor in those with repeated shu nt inf«tiona. POQ ibly .. a relu)t of&dhesion.
forming frOID prolonged apposition of the ependymal lining ohne aqueduct due to the divers,,,!) "rCSF th ...... ugh the ih'~n t. The choroid plexu. of the 4th vemride tOntin ..... to
produce CSF which enlarges the ventnele when there il 4th ventricul ar outlet obItrueti on Or obstruction at Ihe level ortne 8r&Chnoid gran ulatioN!.
Present.ation may include:
1. heada che
2. lower ~rania l nerve palsi es: swallowing difficulties
3. ataxia
4. reduced le ... el oftOnsciousness
5. nauselilvomiting
6. may a lllO be aD incidental findi nl (NB : some "atypical" fwding', auch as reduced
at!entiOI) l pan , may be .... Ia ted)
T rea.tment
Motl.urteONI advOCllte shunting the vent ricle ei lher with a separate VP shunt, or
li n king into an existing .hunl. PotenUal complia t ionl ;nc:lude delayed injury UI the
brainltem by thl catheter Up " t he bra'NI!em moves in Ul i~ norma l position with.drainage ofl ha 4th ventridl. Thilln8y be avoided by bringing lhe CIIItheter inlo the 4th ven·
tricle 81 a .Iight aogle through t he cerebella r hemisphere.
A Tork.ildsell ahunt (ve ntricu lociste roal th unt ) i. an option for obstructive hyd .....
cephall.. if,t i. certain that the ar achnoid granulationa are functional (\dua lly not the
CMe with hydrocephal .... of infantile onMI).
All LP . hunt may be considered WhM the 4th ventride outleta an patent.
CTfM RI CRrrERtA OF HYOROCEPH ALUS
N uroerolll methodl h,,,. been deviMd UI attempt UI q uantitatively defilM hydrocephalus
(HCP) (mo.! date back to the N rly CT experieoce). Some ... prt!!ented here for COOlplel<!oeu. For tldioloei~ featu ..... of chronic HCP,I« f1lJ#f 184.
HydrostatiC b ydrocep hal us
Hydrottatic HCP i •• ugguted when eilher":
A. the I oU of both tempOral born. (TIt) i.", 2 mm in width tift Fi/llOre 11· 1) (i n t he abMn", of HC P. the tempo ral homl .hould be berely vi,ible). and the Iy lvian'\ interhemi. pherie fi"url' Ind cef"flbral uk; are 001 vilible
OR
'"
11. Hydrocephal us
NEUROSURGERY
~ 2 mm , IruI the ratio
~~ > 0.:1 (",hel'll PH i. the lalllest ",idth of the
6 . botll TH ar.
frontal horlU, and ID ~ tll. l1Ilemal diameter
fr1>m l.n ner· Ubl. to j"neNlble at thi. level ) (_
r-r /1 . 1)
Other foatu,," IUlge,t,ve ofb.xd..Gt~ hydroceph·
F" .
1111&:
I. t..lloonilLS of fronu l homs orrete •• 1 ventri·
de. (" Mickay Mouse" Hntric]es]lrld 3n1 V~n·
triela
:l. pfriventricuLar J.o.N deMit,)' on CT, or periyentrkuLar high lnt@n~Lt,..ign .. l em T2Wl Oil MRI
eUi!ftUIIlS trIInlepeodym,J IIb.... rpLioo Or
milP'lIt;OIl orcs!"
3. II&ed along, tht ratio
'H!<~O%
iD
4.
S.
_I
boiok,lioc:
hydroctphalul
Evan'. retio: ratio 0( PH to rnllJtimAl biparieul di~meter > 30$
tllgittal ~ml ml YI ho'" upward bowinG Qflha c:orpua ",Ua.um
40·50%
> :10"10
$~Uesl.l
ET10LOGIES OF HYDR OC EPHALU S
HCP i. either due to luboormal CSF "'lb·
sorption. Or rarely to CSf' overproduction ia.o
Tabl.11-1
HCP In 170
..vith wme choroid pie."" papilionlU; .... en
here, reablorption i. probabl)' defec:tive in
80me &5 IlOrnUll individuals ~ould probably 1001"II\e thuliglrtly el eYlted CSF production 1'lI\e
oftheMl tUIllOI'5). The etiolOjliN in onesenel of
pediatric patienls lI5hltWn in Ttlbk 11. /
congenital
!t, Chlan Type 2 malformltioo
and/or myelOmeningocele ( MM )
{ulually "'cur together)
B. C hiari Type 1 malformation: HCP mIIY occur witb 4th ¥i!ntricle out.letobI truction
C. pnma.,. aqueduclal . teno."" tUlullily p ........ t.o io infancy. taJ'l!ly;n adult-
hood )
D. uc<md ...,. Iqueduclalpiosia: due t tl ,ntrlulotrirw infec:tioo or ge,,,utU\! m~·
Mmorrhage"
E. DaDdy· Wall..,r mal formation: alrellia orfonlmina or Lughll .. &. Mar~nd.
it 1_ PflIl //01. The incidence orth~ in patient! with HCP 112.4%
P. ,..'" X·linked inhentH disorder
Kqui red
A. intKtiouI(the .....' common (3~ OrConHDlllliutinr HCP)
I . pCIoIt-lI'IfninsitiA (upec:iaUy pllt\l~nl and basal, Inc)udingTB)
tn.,.
2.
t)'AWmI6LI
8 . JIO'" .... mcnharic (2nd IDlIISt common CIIUIW! ofcorn munic:aLinG HCP)
I
pINIt·SAJ-l lMc~783)
:l. poIt-in~.v.ntticular hemBnhage ( IVB ], man)' ",ill develop laI.Il4iln\
JlCI' 2().SO" olJ'l'tienlir with la'lle IVlf d""elop perma nent Hel'
C. HCOndary to II"IIMH
I . non neilplastic: e.l, v.nuJa. malfbnnation
2. lleilpJllltic; mosl prodUCI oMlructive HCP by blockinr CS ~' palh",1IY1<,
upedaUy twoonl around aqueduct, e.l. medllJ!olllal!IOrna. A coJ!oid
()'IIte- n block CSP Ilolw It ~ (onome n ot Monro. Pituitary tumor: iU'
pl'Jltellar e~U!ruion of lumo. or upan.ion from pituitary apopleJ<y
D. pott·op: ~ ofped'atric pat.ient.o d~veJop perma nent hydrocephalUl (ra-qu iring I hunl) (ollu"'illl p-f05lle tulUO' removnl. May II<! delayed up to I yr
NEUROSURGERY
11. Uydroc:aphhw
)"
E. r>eu rosar<:(lidosis: see fJ08~ 56
F. 'const itutional ~entriculomegaly": asymptomatic. Need! no trutment
O. associated with spinal tumo .....
DIFFERENTIAL DIAGNOSIS OF HYDROCEPHALUS
For etiologie. of HCP. sefabo~. Conditions that may mimic HCP but are not due to
inadequate CSF absorption include:
I. atrophy: IIOmet im"" refef'!'fld to u "hydrOCf'phalu$ ex vacuo". Ooet not represent
altered CSF hydrodynamics, but is rather loss of brain tis.aue (set page 180)
2. bydraneru:ephaly: ~u page 180
3. developmental anomalies where the ~eotricle s appur enlarged:
A. agenesis of the corpus callosum: see page 114 (may occa~ionaJJy be associat.ed with HCP. but more often merely represents expansion of the third ven'
tricle and separation of the late ral ventricles)
B. . epto-optic dysplasia: ,~ P08~ 122
SIGNS AND SYMPTOM S OF ~ HCP
in young c hildren
1. cranium enlarges at a rate> facial growth
2. irrilability, poor head control, NN
3. fontaoelle full and bulging
4 . enlargement and engorgement ofs~alp ve i",,: due to reversal of now from intra_
cerebral sinuses due to inc ",,"sed intracranial pr""",ure"
S. Ma cew en's s ign: cracked potlOund on percussing over dilated ventricles
6. 6tb nerve (abduce ns) palsy: the long intucranial course is p08tulated to render
this nerve very sensitive 10 pressure
7. "aettjngaun sign" (upward gaze palsy): P arina ud'a syndr ome from pressure On
region of supra pineal recess
8. hype ractive renexes
9. irregular respirations with a pneic spells
10. splaying of cranial sutures (seen on plain skull ~-ray)
10 older childrenlad uJt.s with rigid c ranial v a ult
Symptomsofincreased ICP. including: papilledema. lilA. NN,gait changes. upgaze
and/or abducen s palsy. Slowly enla rging ventricles may initially be asymptomatic.
CHAONIC HCP
Features indicative of ~h.onic hydrocephalus (sa opposed 10 acute hydrocephalus):
I. beaten copper cranium (some refer to beaten silver sppurance) On plain ! kult ~_
ray". By itsel f, does not correlate with increased ICP, however wilen auociated
with ' 3 and U below, does suggest I ICP. May be seen in cranioayTlO$t08is (.....
pnge 101 fordeacription)
2. 3rd ventricle herniati ng into &ella \Been On CT or MRIJ
3. erOllion of sen a turcica (Illay he due 10.2 above) which &101eti.lnes produ""s an
em pty ""lis, ond erosion .,(the do ..."", ..,11"
4. the temporal horna may be less proll"lillent 0\) CT than in acute RCP
-5. maerocrania , by C(ln~ention. OFC greal<'r than 96th percentile.. '......
6. atrophy of ool'J)Us CStl 06um; best appreciated on sagittal MRI
7. in infaOI$
A. sutural dillBus;s
B. delayed closure of fontanelles
C. failure to tllnve or devetopmenl.81 delay
OCCIPITAL-FRONTAL CIRCUMFERENCE
Tbe oc:cipi(al _fwnlal Circumference (OFC) shou ld be followed in every growing cllild
(as partofa "wen-baby" check-up, snd especiatly in infants with doc:umented or suspected bydrocephalus (HCP)). ~ s rul e ofthU(llb, the OFC of a nonnal infant should equal
tile distance from Crown to rump .. '.... ·- . Sf!<l pog~ 9 19 for the differential diagnosis of
macroceph aly.
'"
11. Hydrocephalu8
NEUROSURGERY
Normal head (Towth: parallel. nonnal curve.a a. seen on lhe graphs on the in side
front COlVer , Or in Fi,,,re 11·2 a.nd Fill"'"' 11-3 for preemie.. Any of the followirtg may . ig·
niIY tnoatab!e conditioflt ",ch as active HCP, aubdu rt.1hematoma. or l ubdural elfulionl,
and sho... ld prom pt an evaluation of tile intracranial contenta (e .g. CT, head UIS .. J:
1. ... pwa rd deviatiollS (croQ ingc ... rvu)
2. contin ... ed llead (TOw th or more than 1.25 emlwk
s . orc approaclling 2 atandard deviatIon. (SO) above normal
4. llead g rcum ferllnce out of prOpOrtion to body length or weigllt, even if willi in nor·
mallimita for al:'8 <- FiB"'"' " ·31"'
~
I
~
I
~
•
»
V
/'
u
"»
k'
PERCENTILE
i--
,
--
H
1""1"
H
V
j,,~
"
V
I
H
1"'1"
~
/f
25'!-
"
I
I
I
/
I '~
~
n
~
H
I
"
"
H
11_2
H
JO 31 32 XI , . ~ :J& 31
.... e e KS OF a e S l AlIO ..
•
~
,
H
~
,
."
Theseconditions may al&o beseen in llie-cateh·up pll8Ml"ofbrain (TOwtll in premature infants aller Uley reCOlVer from thlli r acute medica] iIIn......., . . Colclo ·"p p",,"" 0(
/lmin 8rowth page 864). Devia l iona below the c ... ,.... or ne..d growth in the prematUnI
infanl in the neonatal period oflesa Ulan O.Scmlwk (excludIng lhe fint few weeka ofli re)
may indicate rnicrooephely (,« pagt 113).
T"",hn;qu,"c m~ ... ," eircumr.... nce arou nd rordtttad and ,,"ipul (ucludinj: ea.,)
tllree consecutive timn, and use the Ia.r:n4l. value. orc i. then plol.ted on . gra pll oraverage values as a functi:Hl or age- and followed for each individual patient. Use the
graplls on the in$id .. front cover for most cllildren and adolt!K<l' Dta. The .... ph in flBurt
11-2 11101011 the ore for premature infanta .. a fwK:tion or ee-ta tionalap up to term.
Th .. grBpli in FiB"'" 11·3 aliowl the n lationltt.ipo(lIead circum(trflnce, weillllland
length for v.riou. gestat ional agea.
11.1.
Treatment of hydrocephalus
MEDICAL
HCP nlm.in s .. lurgicaJly Lreated condition. ~tnol.mide m.y be helpful !"or temporizing <1ft btlow).
NEUROSURGERY
'"
..
"
" -l
•
• _I
•
•»
• '".,
•
" ,.",
"u
..••,
,
~
1/
b#J
J
'1.0 '
~-
11 .0
f-7
r
-~
CL
~
-
7
,
;7
~
-,=-
.. -
,
U
~
7"
. -.
- - -- - ."" - -~
.
-212130J2:Ull5
001 ' " poe
~
-
=
~
~
<0
U
,
, .1">
,,-
/c
, 7'
/'" ~ "7
7'
-
,,
~
~
/'
--
=
=
-
•
•
.,
~-
~o.
.. 2!)0.
-.~
{WIlMs ~ .- - - (/IIotII""
parium)
.2
'"
~
t
I
•~
Flgwe 11-3 Head Qlcumklrera, ~1gN and length
(_ _ I!om Journal 01 _.,11<8, ~ Go""", to< .... Cheal ~ at 1nIanI. 01 Varying 0 ...
_Age·, IIIIIleo:wISG. _ G l, ...... ""eI5 , wiIII~' .........)
Di~li c
the rapy
Ma, be lri~ in pI'MllI lun! infan\.!! wilh bloocty CSP (.. long" the.re i, no ~vide~
of&etw. hyd....,.,phalLl5) ",h ile waiting to lee it lhere will be resumption ofnOtmBI csr
.l>3olll';OIl. H_ev~r. M be" Ih i. .hould only "" colllid"red u lin ~djund to definitive
trealment or a.s 8 temporizing I'IlflaluN.
Seli5fact.wy con trol or Aep '"'11$ reported in _ ~ ofpatienu ofare <: 1 yeer who
had . .... bl" v;1;61 s;rn-, IlOrmal renal function.nd no symptoms of"l.... tood ICP (apnea ,
Ielhllf'D'. V1Imitincl u!!ina" ~ foll_i,.,...:
.eel.~ol .mide (a ce!"bo.uc anhydrase inhibitor): 25 mgl'kWday PO divid~d TID
•
II 1 day, inCrell!le 25 mgI'kNday -n day \1ntil 100 mlJl'lWday i. r1!6ched
,;multanew5ly ftort tul'ON.lnide: 1 .Wday PO divideod TID
to oaunterltC;l acid..;.
tridtrl~ (Polyctr4) 4 mlil<,dly di ..idtd QIO (.ldI rr.l it iquiul... l W 2
mEq ofbicarboalle, snd conlai ... I mEq K' .nd I II:IEq N,,')
• mtlu ure MorialtledrolYIU. and adjult dONp 10 mli " t.sin &en"n HC03
,18 mEqfL
• chlnge to Poiydlrll·KII(2 mEq K' per ml, no "'I') ifMnlm poUiaium"
cornu low. Or to iOdium bicarbonlte: ifHTU ra aodi um beoc.Gmellow
Witch fo. O!JM'l rfll)'tl imbJ,J&IlCI and Ic:fItll.Ollmid • .ul1I.rr_.... IlIlhll'2)', t&chypM I, dia"hea. perislheilu (.... tincline in It>. tincenipe)
perform weekly UIS or CT tean and Wart ".nllieul,r shunt i t progr",i... ""PI\riC\.llomeca!yoccu,..,Otherw.lt, ""inlain therapy fo. aSmo:o1h tn.I , th.n la per
dOSllIl" ovllr 2-4 _ h. Ruuma 3·4 "'(110 of t reat mtlnl .f~ye HCP occur.
•
.
,
NEURQSURG8RY
SPINAL TAPS
HCP after intraventricular hemoTTh age Illay be only tranaient Serial ups (ventricular or Lf"O) may ~."porize u.otil resorptioll resumes bu pogf 864) but!.Ps can only be
pe rformed for communicatini HCP. Hrea bsotption does not resulM wilen tile pro~in
(on tent of theCSF is < 100 mgldl, then it i. unlikely that sponta neous resorption will oc·
cu. (i.e. a sh unt will u~uany be necessary).
SURGICAL
Goals of therapy:
Nonnal sized ventricles is not the goal of therapy. GoaJs are optimum neurologic
function and a good COIIroetic result.
Options include:
1. choroid plex\!ct(ltlly: OOBCriOO<\ by Dandy ill 1918 fOf communicating
lIydroeephalus". May reduce the Tate but does not totally halt CSF production
(only a portion ofCSF is secreted by the choroid plexus, other souroes include the
ependymal lining of the ventricles and the durolsleeves ofapinal nerve roots).
Open surgery Wa! associated with a high mortality rate (possibly due to repla".,.
ment o(CSF by air). EndOllCopic choroid ple~us coagulation was originally de·
scribed in 1910 and was recently T€SUTTected"
2. eliminating the obstruction: e.g. opening 1\ stenosed sylvian aqueduct. Often high·
er morbidity and lower success rate than .iro ple CSF diversion with shunts, ex·
cept perhaps in the case of tumor
3. third ventriculo~tomy : (sec b<Jlowl
4. shunting: various shunts are described below - ventriculoperitoneal, ventriculo·
atria l, ventricuic>pleural. lumboperitoneal ...
T hird ventric ulost omy
There hu been a resurgence of inteT€St in third ventriculClStomy (TV ) with the recent incl'(!aeed use of ventriculO$copic surgery ($et! pas.. 622 for technique).
Ind icatiolla: TV may be used in p!ltients with obstructive HCP. May be an optioo In
managing shwlt infection (as a tIlean' to remOve al! hordware without subjectIng the pa·
tient to in<:Teased ICP). TV has also been propoeed 88 an optioll for patients who devel .
oped sobdoral hematomas aner shunting (the shunt is removed befoN! the TV is
perfonned). TV .,,8Y alao be indicated for slit ventricle syndrome (see fXJiIe 197).
COlltr aindiclltion.,: C<>mm"nicati"8 hydrocephalus is considered a oontraindlcation to
TV. Relative contralndication8 to TV would be the presence of any of the oondltiolls asso·
ci"ted with a low succo''IlI rat(> (su ~Iow ).
Complication s:
1.
hypothalamic uuury
2. t ransient 3rd and 6th nerve palsies
3.
uooootrollable bleeding
cardiac aTTest"
5.
traumatic ha,ilar artery aneurysm": pO$.9ibly related to thennal injury from U911
of lase. in performing TV
Succe$8 r ate: OveralllucceJ;;S rat(> is _ 56%(rangeof6l).94% for nontumoralaqueductal
stenO$is" (AqS)). Higheat maintained patency rate i5 with pnviously untreated Il(:qu i~ AqS. SUC<:e&o ,"te in inrllnt.a "",y Le po<>r beu. .. "., they mill' not hllve " n ormlllly
developed subarachnoid spllee. There is a low success rote (only _ 20%ofTVs WIll remsin
patent) if there is pre.eristing pathology including:
1. tumor
2. previous shunt
3. previou. SAH
4. previous whole brain radiation (succes.'lwith focalstere<ta<:tic radiosurgery is not
known)
5. s ignificant adheSIons v'sible when perfornting through the floor of the third ventricle at the time ofperfonnance of TV
4.
11.1.1.
See
Shunts
V~nlric!d<>r shunls
NEUROSURGERY
on page 620 for surgical insertion pointers.
11. Hydrocephalus
'"
TYPES OF SHUNTS
SHUNT TVPE 8Y CATEGORY
L
v~n lriculopentonta l
2,
vlntricu!o-atri, 1(\IA) "hunt {'~ lilkuIAr .hunn:
(VP ) ' )Hun:
A. 1II00t commonly IIStd I hllnt In mod~rn IN!
B. Ii tt rA! vtnt.ride IS t h. l.IIuol prOllimplloca tion
A. s hunu vI"triclel throughJugular vlin to,up"nor ~In~ CiV., 1O-C.1Ifl1 "ventneule-.tri.l" I hunt b6ctUlI it , hWlu the N",bral Wlilnc/~. to !.he vaKultr
.Yitem with thl eath~ter t ip in thl ,-.gion of the rilhtC4J"d1oe gtrlllm)
B. tr~ .. lmMnl of chOice w)"ln $bt!om;1UI1 SbnortIlAlit iH ... pr_nt (Utfnllvl
IIbdomlnallUl"(f!r")', pentonlli" morbid obesity, in preemw who hsW! had
NEe snd 'My nol t.>lenw VP .hun t .. .)
C, I horter ll1ngth of tubing ""ulla in lowe. d;'tal PT"@UUNllnd leu tJphon Irfect Ihln VP IhUlll
3. Torki ldGAA . huIII:
A, shun t...eo.lricle tIJ ciaw,nal,par:e
B, rarely used
C. ~ffertJ~, only In .equired ob.lrocUvt HCP. II petlenl.l with eotllenital HCP
frequently do 001 do:\velop nonoallu!)srtc:hnoid CSF pe.thwa)'J
4. m;"ceUanl!Ou,: vlriou. distal prajectilHl' u,ed hiltorie.lly 01" in Pl'tienlawho l.. vI
had l ignifiesn! problem. with tradiUonal I hunt 10000lioni (e-l. pllritonlti. with VP
shuot, SBE with vascular . hun1.l):
A. pleursl spIlee tventricu] o pleura l l hunt): not I r.rstchoiCII, buill ';shkr altemsLlve if the pe-r;tol>l!um is not sVliltble'S. Riak of ;r;ympt.>nllllic h,..
drothorax nece8IIitallnlf relocating d istal end . Recom~ only fM
peuent.s" 7 yn.1t'!
a, gall bladder
C. ureter orbladder: CIIU",", electrolyte imbala_due!.O 10..... throuch urin ..
5. Lumboperitonea' (LP) ,hunt;
A. only ror communie.rtinll HCP: pnmariiy pr;eudolulDOl' teTl!bri or
r1.&lu)s". lhIeru l in lIi tullionl with IImall " .. ntricles
B. o"er ale 2)""S. perculaJl~ul iDliertiot\ with Tvoby ne.IJe ia pre~~
6 tyIIlor llubdursl,hunt: from 1IJ1Ielwoid CYlt Or 50bdural hygram. ClIvi!)" ususlly
\0 ptriwne ul1l
csr
Djl!adyantages/con;r pi icationa of varioul ahunts
I
thOMlthat m.y occu r with lillY 1hunt:
A. ot..truction: the UlOIIt common cau'" or,hunt malrunction
• proximal: v~ntrieullr CIItheter flhe mott tommon "i~ 1
• valve ml!'Cllanilm
• distal : reported incidfflClof 12-3-4","". ~ in petito"'!a] cathel.er in
VP Ihunt 411ft below). ln atrilll CIItheter in VA . hu."1t
B. diKOnnection lit ajunr:cion, 01" break at IIny poIn t
C. u.feclion
O. hardw ..... ef"OlJlon thl'OUlh sk in, usually only in debilitated plltienlt (espedally preemies with Inlllrpd herodJ; and thin SCII lp rro m chronic " CP, who
lay on OfIe aide of head due to elonll"lt.ed cr.nium). Mil,)' a lso indicate .ilicolHI
allergy (_ belOUl)
E. KWi1U (venlricula • • hunl.lonly}: (hue il - 5.Kriskol",ri~ul"f.in the first
year aft.er pl_1Mn1 01. ,hunl which drops to - 1.1" ancr Ihe 3rd y ......
INa; this d_ nO{ IIINn th at the I hUll! 101" the caulII! or.1I of th_llri,urM) Sei~ure ritll ItqustlolUlbly hia:herwith ,","1.11 CIIth.,tertthan with
parieto-lI«i piW
F. Itt nl conduit fo.ntnlniuraJ mfllMlUftofCflrUln tu monr (e.1o medullo-
bI •• toml ) Thi, i. probably I relativlly low n&k rr
G. "licone .Ue..,... rsrelifitOtt\lrt.1 1m. May 1'fIM00bIe .h uM InfKtion WIt h
,ki n breakdown and fllnptill(lI'.nulomsl. CSF i. in,tially Iterile bu~lster
infection, mil,)' oc~u r. May requi rl f.tobrication of a ClJllOm $iJicone·free d ..
viCII.(e.lf. poI)'urethane)
1. VP lhuDt;
A. ,7'" ino;:idO!I>re inguinll hernf. {",Iny IIhuntl are il1Mrtad while pnlCIIIL~UII
"I" nali, is patenU""
B. need t.>lengthtn artMI.fI" WIth ,",wth: I1Ily bt obviltAro:! by usin, 10111 peri.
08'
NBUROSURGBRY
too"ol catheter (IOU page 621)
obstnJctio;>n of peritoneal catheter:
• may be more likely with distal ~lit openings ("alit valves") due to occlusion by omentum or by trapping debris (rom the ahuntsystem"
• by peritonelill cyst (or p8IIudoc)'!lt:r"': ""usHy lL$$OCiated with infection,
may alllo be due to reaction to talc from aurgical g loves. It may rarely
be necessary to differentiate a CSF collection from B urine collection
in patlen!..! with overdistended blpo:idel"$ that have I"\Jptl1J"ed (e.g. seeondary to neurogenic bladder). Fluid Can be aspirated percutaneously
and analyud for BUN and creatillille {which should beabsent in CS FI
• severe peritoneal adhesions: reduce surface area for CSF resorptiOIl
• malpo.'lition of catheter tip:
at time of surgery: e.g. ;n preperitoneal fat
tubillg may pull out of peritoneal cavity with growlh
D. peritoniti s from shunt iofe<:lion
E. hydrocele
F. CSF a..:ites
G. tip migratioo
• inlo acrot um"
• perforatioll of a viecua": stomach", bladder ... More common w;lh older spring- reinforced (Raimondi ) shunt tubillg
• through the diaphragm"
H. intestinal obstruction (as oppo.iled to perforation): rare
I. volvulus"
J. intestinal strangulation : occurred only in patients in whom attempt was
made to remove peritoneal tubing using traction on the catheter applied at
the cephalad incision with subsequent breakage of the lubing leaving a residual intraabdomi.nal aegment (immediate peritoneal exploration," re<.:ommended under these circumstances:r'"
K.. ov.. rehunting: more likely thao with VA shunt. Some recommend LP shunt
forcommu>licati>lg hydrocephalus (su pagt 196)
3. VA shunt:
A_ requires repeated lengtherling in growing child
B. higher risk afinfe<.:tion, oepticemia
C. pOssible retrograd .. Dow of blood illto ventricles i(valve malful)Clions (rare)
D. s huntembolUll
E. v8.I!Cular complicatiOM; perforation , thrombophlebiti s, pulmonary mie...,..
emboli may cause pulmonary hypertension" (i ncidence _ 0.3%)
4 . LP ahunt;
A. if at all possible. should not be used in growing child unless ventricular aeceSli is unavai lable (e.g. due to slit ventricles) because of:
• laminectomy in children ~auses !>COli,,"," in 14%"
• risk of progo-essive c.. rebensr tonsillar hemiation (Chiari I malfonna.
tion)" in up to 70% "fcase..... "
B. overshunling harder to control wh .. n it occurs (a special horironlsl-v.. rtical
(H -V) valve increa8e:! res;"lance when upright,..,~ ",,-I()W)
C. difficult access to prox.imsl .. nd fer r.-visienorassessment efpatency (ueLP
shunl eIJaiualion, page 622)
D. lumbar nerve root iniUltion (radiculopathy)
E. leakage orCSF around catheter
F. preuure regulatiol) i. difficult
G. bilateral 6th and even 7th cranial nerve dysfunction from overshunting
H. high incidence ofarachnoiditi. and adhe\lioJUI
c.
MISC ELLANEOUS SHUNT HARDWARE
L
tumer filter, used to pr.-vent peritoneal Or vflS<:ular S<'ediog in lumor. that may
metastasize through CSF (e.g. medulloblastoma". PNETs, ependymoma); may
eventually be<:ome oco::luded by tumor cells I!lIId need replacemenl; may be able to
radiate tumor filter to "sterili,e" it. The rak of "shunt meta" appeaJ"ll to be 10......
2. antisiphon device: prevents siphoning effect wh .." patient ill er"i!<:t
3. "horizontal_vertical valve" (H-V valve) Ulied with LPshunts to increase th .. valve
resistsnce when the patient is vertical to prevent overshunting (He page 193)
4. e>clemaUy programmable variable pressure valv""
NEUROSURGERY
11_ Hydrocephalus
'"
5. on·orrde .. k.; uad w open or oa:lud•• hun t '~8t(l\Jl
tinn of . hunt (I.g. Portlloy device)
b~
",;ng utom.l m. nipul.·
SHUNT T'l"PE BY MANUFACTUR ER
Nu.oe .........hunt . ylte.o. .... on the lIllI.ket. The fQllow;ngdeKribes the M.1ie flt fea ·
ture. or lOme commonly ulled .hunt.. Di'gr.rna Ire not 1(I1I:.le.
X·RAY "P~AAANCE OF SOME Sf/UNTS
fbe followIng figure depictt idu.linlI. x· ray
appearan~1
of IOnia <:<I)",,,nn th""u..
Agurfll 1 ... X..... y appelllince 01 common SIIunI.
P$ MECNC/tUMEDTRONIC
","'"."
125 C.tlrnona Dr.
(lop view)
GoIttIa, CA 93117 USA
(800) 826-5603
':I:":f!'W.1!!!d!'0!!1£,9O!D
Stand..rd co ntoured
valve
A li n, l. one'''' IY Dl<!:m·
brane "II... de.ign. The. ra·
dio-opaljue l/TOWhead point.
in the di.-.d.ion ornow lI«
Figurt J J·41.
Pumping tbe .... I..e
To pump Ule Ihunt in
the "forward" diNld..on. r;Tlt
occlud e the in18t pori. (1ft
Figurt J l.ff) ,.,ith p,"*ure
from IIlIe fi nger on the '"i nlet
occludet'" {pn!~entt bao:k.
..
,
_
!low
!low
(lode Yiew)
FIg"" I 1-$
PS Medio;aI-.cIatd -....:I "I~
NEUROSURGERY
nnw into the \il'ntridl! du ring the .)\,,,t step). The n whlle main:ainin& t his Pre5!lutll. (II!'ptell5 the ruervoirdome with 118/!(X)nd fin,ar. Ro!lel\se both finGers, and repea t .1'1lE! One-
way vllive reguJate8l'ihunt pfeMu re and p.... vl'nlll reflux of CSF during normal
during the rel<!lll$<l ph8~e of shunt pumping.
w;e
and
X'rpy c ba r acter iiticii
The lhree ava il able
valve pressuret an indicllt.ed by rndio-opaque dou. on
th~ .,,,,lve (allow5 x-ray identification Qr"alve preuure),
one dot :. low prell!lur~, two
dots z medium. thfSle (lotll ..
high
r;.~:r~~~~::~~M~EP~,~:t::~,..
_..
.....
STB> 1
FIgura 1HI
Pu"lf'lng!~
cl!tprllSS poolp
ctIamber
PS MedIcal vaIYe
Strata® program m able valve
The Medtronic
Strata valve is aD utemll.llya!(jUlltable
"alve thllt i. pro8Tllmmed (Ulling II
magnUjtooneoffi"e
perfof[oaoCill evel
I"P/L- ) setting!! (Filllire J J-7).
Bi!cause tile
YDlve mil)' be inad_
venently reprogrammed by
external magnet.a,
the patient must be
in formed to have the
\/lI]ve setti llg
thecked aFter an
MRI performed rOT
IIny reaSOn .
SOPHYSA USA
Sophvsa USA, Inc;,
760 WEtSI 161h 51.61dg. N.
Costa Mesa , CA 92627 USA
(949) 546·6484
www.sophysa.cgm
P o l" n .. p ....gy...... m .. bl .. vw" ..
The Polaris"V ... I,,", ial'" H lernally programma·
ble valve thai \ISe!I two attracting Sarnor iUlDCobal ll1lagne.t8 to loel< the pressureaet\ingllod
to ,.,.ilJl. inadvertent reprogramming by e.",i.
ronDlent.ally encountered magnetssl.lch at MR!
5el!onen>, oelt phon"_ headphon es ..
Available in 4 rnooels (dim-rent preasure ranges. ea~h identified by II unique nllrn·
ber ofradio-opaque dotal, each wit h 5 extemally adjustable posit ionL The ~-ray appeara nce and correBponding pr\l.'!SU'1!S lire .hown in Figu.re 11..8.
NEUROSURGERY
II. Hydroo:ephalU5
'"
NEUROCARE
Oisl<ibuted in U.S. by;
NeuroCare Graup
8401 1020d Sireel
Suite 200
PIBasanl Prairie , WI 53 158
(800) 997·4868
Heye ....SChu tte
The t.PV nlye i,
shoWn in Figun! //-9. To
pump the sh unt, o.;d u<il'o
inlet port wiLb eM fiel:er.
-Figure I I,; Heyer..sct\ulle LPV® (IGw.prollle) ya"-'e (sideYlewl
then depl'(" ~ reservoir
with anelber linger (as for
the PS Medical "alye, "'~ 000 ... ). This "alYe ma,y ~ il\iected in either djr~tjon by depres.ilW tl1e appropriate occluder while il\iecting Into ttle re!Arvoir.
,"","::",",,,;:;;:;:;,,,,,,,,,,,,,,,;;:;:;:;;;;;:;-::;;;;;;;;;:::1.""
HAK!MSHUNT
Dlslribuled by:
Inlegra N6U(OSC'Bno;es
In lhe U.S. ~
311 Enterprise Drive
PlalnsbalO. NJ 08536
(800) 654·2873
tl.!!P :I~_i!lt'9ra-ls corn
A dual ball·Yal"e
Flgu.e 11 -10 Hakim StaJl(lard M6ehsnosm
To pump
shunt. depress the indi ·
CIted portion of tl1" "IIYe. NS, Wuwt. tap be ... , liS the sHirone elastomer bousing is not
.-.elf-scaling. The ant.eehambe. Is provided for this type of 1~88.
mechlni~m .
'"
It Hydrocephalus
NEUROSURGERY
INTEGRA HORIZONTAl-VERTICAL LUMBAR VALVE
May be u!led in lumboperitoneal
shunt to increue the transmiS9ion pres·
sure ",hen the patient i~ upright 1.0 pre·
"ent o"ershunting. Markings used to
orient the de"ice during implantation:
I. an arrow On the inlet side of the
unit indicates direction of now
2. inlet tubing i. clear
3. inlet tubing has s ma lle r diameter
than outlet tubing
4. ou t let tubing is white
5. before position ing t he valve and
fastening it to the fO.6Cia with per·
Ulanent suture. t he valve shou ld
beconnected to both the subarach.
noid catheter (iD let) and the peri·
toneal catheter (outlet). The arrow
on the inlet valve should poiDt tQ.
wards the patient's feet
...
/esistance
Figure "-'1 Inlegra H-V "a"'a
HOLTER VALVE'
Distributed by:
Cadman & Shur1leN
Randolph. MA 02368
(6 17) 961-2300
A dual .lit valve
mechanism (set Figur-e , I ·
12). Usually used in COmbination with a Rickham
orSa lmon-Rickham reser·
Wli. (_ FiJluNI 11.13).
To pump the . hun:, simply depress the indicated portion
or t ~
valve.
X-ray charac te r istics
The sil astic tube bet ween the two one-way valves;$ radiolucent 1_ Figun 11.4, page 190).
SALMON-RICKHIIM RESERVOIR
Simi lar to standard Rickbam ruervoi . 8)l'cept for low·
er profile lou FiJlun 11· 13).
"·'3
FIgure
SaIIl'lOl'l-Rick·
Mm-..
11.2.
Shunt problems
Neurosurgical eva luation i5 usually requested for patients with a CSF $hunt with
variety ofsympWms. Shunt ·problema" usually involve one or more of the followi ng:
1. ~nde~hunting ($u belowl
} accounts tormostOJllVTlOO!.hunt problems
2. ",factIon (su pa~ 214)
3. overshunting: slit ventricle syndrome. subdural hematoma~ .. _(ue page 196)
4. seizures: 8U POll~ 188
5. problems ~l ated w the dilltal catheter
A. peritoneal: IIt:~ pag~ 188
B. atrial: IIt:t page 189
6. skin breakdown Over hardware: inrection Or silicone alle rgy (ue pagt 188)
NEUROSURGERY
11. Hydrocephalus
'"
TAPPING A SHUNT
indicllti(ms to Ulp a shunt or ..entricular ac~s.s device (e.g. Ommays reservoir) indude:
1. to obtain CSF' specimen
A. to evaluate ror shunt infedion
B. for cytology: e.g. in PNET to look for malignant cells in CSF
C. to remove blood: e.g. in intraventrioular henlorrhage
2. to evaluate shunt funotion
A. measuring pressu res
B. contrast studies:
I. proximal injl"'tion ofenntrast (iodinated or radio·labeled)
2. distal il\jection of enntrast
3. a8 8 tempori~ing measClre to aUow function ofa distally occlClded shunt"", ..
4 . to inject medication
A. antibiotics: for shunt infl"'tion or ventriculitis
B. chemotherapeutic (antineoplastic) agents
6 . for oathetel"!l placed wi t hin tumor o)'>lt (not a true shunt):
A. periodic withdra ... al of accumulated fluid
B. for injection of radioactive liquid (usually phospilorous) for ablation
TECHNIQUE
(For LP shunt. see LP shun' ~!JfJ1ualion. page 622).
There is a risk ofintrodudng infection with every entry into the .hunt system. With
care, this may be kept to II minimum.
I. ~h a ve area
2. povidone iodine solution prep _ 5 minutes
3. use 25 gauge butterily r>eedle or smaller (ideally a !>Oneoring ne<ldle should be
used); for routine taps, tile need le should only be introduced into shunt compo.
r>entll specifically designed to be tapped
To measure pressures
Steps are outlined in TaMe 11·2.
Table 11·2
a s hunt
neous IIow into btmertly tubing;
S-i.J.e in manometer
IN STRUCTIONS TO PATtENTS
All patients and families ofpatienta with hydrocephalus should be instTUoted reo
garding the followjng:
1. signs and symptoms of ahunt malfunction Or infection
2. not to pump the shunt unleu instructed to do SO for a specific purpo:se
3. prophylactic antibiotiC!!: for the following si t uations (mandatory in vascular
shunl.!i. somet imes recommended in other shu.ota)
A . denUlt procedures
B. instrumentation of the bladder: cy~l.O!!copy, CMG. etc.
'"
II . Hydrocephal\l.!l
NEUROSURGERY
4. in 0 growing child: th~ need for periGdicevaluation, including asses&mentofdi.r;tal
shunt length
UNDERSHUNTlNG
The sbunt malfunction rate is _ 17% during the finlt yea r of placement in the pediatric population.
May be due til one or a numbe r of the following:
1. blockage (occlusion )
A. possible causes of occlusion:
1. obstruction by choroid plexus
2. buildup of prot.e.inaceQus accretions
3. blood
4. cells (inflammotllry Or tumor)
5. secondary to infeclian
B. site of blockage
I. bloek.sgeofven tricularend (lTI(Istcommon ): UBuall,y by cbaroid ple"u",
may also be due to glialadhesioru;. intraventricular blood
2. blockage ofint.ennediate harowan! (valves. connectora, etc., tumor fil.
ters lIlay become obstru~ by tumor cells, antis ipoon devi~ may
dose due to variable overlying subcutaneoU8 tissue pressun!~)
3. blocked diltal end (U<I page 189 for VP sbunt)
C. diSC(lnnec:t:on, kinking or bn!akage of system at any point with age, silicone
elastllmera used in ca theters calcify and break down. and become man! rigid
and fragile whicb may promote subcutaneous att.chment'". Barium im·
pregnation may accelerate this process. Tube fractures often OCCur near the
davide, pn!9UJl"1ably due to tbe incn!osed motion there
Signs and ayruptom s of undersbunting
SiIWS and symptoms a~ th08e of active hydrocephalus. and include:
1. acute axDlJ>12m~ of incn!ased intracranial pre$l!ure
A. HiA
B. NN
C. diplopia
O. lethargy
E. ataxia
F. infants: apnea and/or bradycardia; irritability
C. sei~ure8: new onset, increase in frequency, Or diffICulty in control
2. acute ainI of inCn!8.'Ied int racranial pressure
A. upward gaze palsy ("setting sun sign", see Por;mwd', r:t"drorM, page 86)
B. abducen. palsy: false localizing ,ign
C. field cut, o~ blindne8g (lee RIi>ld~ss from hydroctpho/u.r. page 202)
D. papilledema (rare before age 2 yt$)
E. infants: bulging fontanelle , prominenlscaip veiD~
3. swelling around ShUDt lubing: caused by CSF dissect.ing along shll!lt tract
4. chronic chongu: before sutures close. OFC, crossing curves
EVAl.UATION OF SHUNT FOR UNDERSHUNTING
I. history and physical directed a l det.ennining pres ... n"" of above signs and symp-
tom9, al,o ascertain:
A. reasOn for initial insertion of shunt (MM, post· meningitis, etc.)
B. date of last revision and reuon for revision
C. Pn!sence of accessory hndware in system (e.g. 8Jltisiphon device. etc.)
D. for child ren: OFC. Plot on graph ofoormal curve!! (use existing cbart for
that potient ifavai lablel
E. fontsnelle tension (if open ): a soft pulsating fontanelle varying with n!spi·
rations is norllU'll, a tense bulging fontanelle suggests o~t ruct.ion , a sun ken
fontanelle may be normal Or may n!presenlovenhunting
F. abi lity ofanunl to pump and refiU
1. tautian: maye~ac<lrbat.eobstruct.ion, upeci,ll,y if shunt is occluded by
ependyma due to overshunting: controvenli.1
2. difficult to deprf!u: suggests distal occlusion
NEUROSURGERY
11. Hyd rocephalus
'"
3. slow to refill (genua!]y. any valve should refill in 15-30 &eCS): liuggellt8
proximal (vent ricular) occlusion
G. evidence ofCSP disse<:Ling a]oniliract outside "r,hunt tubing
H. in children pffsenting only with vomiting, espe<:ially those with cerebral
palsy and feeding gDslrOllt(lmy tubes, rule-out gastroesophageal cellwc
radiographic evaluation
A. "shunt leries" (plain x-rays to visualize entire shUnt' ror vP ahunt, AP &
lateral skull + "low· eXR and/or abdominal ,,-rayl
I . RIO diSCOI\l1«tion or migrat;"'l of lip by x·rays 10 visualize entire
shunt; note; a disconnected .hunt may eontinue to function by CSF
now through a fibrous USC\.; the ("l1owj"8 hardware may be radiol u.
cent and Ca n mimic disconMCtion:
8. the central silastic pan. of II Holter style valve
b. conn~tors IT & 1'" as well as straigtlt)
c. antisiphon devices
2.
d. (uroot filters
ohu.l" most recent ,,·ra)'ll available 14 compaN! for b~ak, (essential
for "complicated" shunts involving multiple veutrkular or cyst end~ or
a«essory hardw~)
8. in patients with open fontanelles, ultrasound is optimal method of evalua·
tion (especially if previous UIS available)
requi red if fontanelles dMed. may be desirable in complicated shunt
C.
systems (e.g. cyst shunt.s)
D. M.Rl: too <:(I9tly and I tow for routine shunt evaluation, shunt hardware is
difficult to see, However. may be inva luabl,! in complicated cases (may show
t r ansepe Ddy ma l a bso."t ioD ofCSF,loculation l ... )
E. ·s hunt..,·gram" ifit is still undear ifshunt ill functioDinG
I. radionuclide: see tH.low
2. x·ray: using iodinated co"tra~t..: lI"~ tH.low
3_ shunt tap: indica tions vary, generally performed if surgical exploration is consid.
ered or if infection is Itrongly auspected (see T"ppilliJ" sh unt, page 194)
4 . shWlt exploration: sometimes even aner lhorough evaluation lhe only means to
definitively prove or disprove the functioning of various s hunt components is to
operate Dnd isolate and Lest each part of the system independently. Even ""hen
infection is not suspected, CSF" and any removed hardware should be cul t ured .
2.
cr
"Sb un t-o-gram "
Procedure: ahave hairov'!r N!servoir& pN!pwith Betadine. With patientaupine tap
the shunt by iru;ertinK a 25 Kauge butterfly needle into the reservOir. Measure tJle pN!Ssure with a manometer . Patien ta with multiJlle ventricul8Tcathetera need to have each
injE-c:ted to verify its patency.
Rad i()Duclid .. "shunt-o·gram" AKA radionudide shuntogTaphy>': after tapping
the shunt, drain 2·3 roJ ofCSF and seml l rnl erCSF fo r C&S. l'1,iect radio-;sotoJle (e.g.
for VP shunt in an adult, use I roC; of-1'c (techne<;ium) pertechnetoU! (usabla !"\lnge:
0.5 to 3 mC il in l« ofOuid) while occluding distal now (by cornpressinK valve o. occlud·
ing portsl. Flush in Isotope with remaining CSF.
JJO.O\ediately iroage t.he abdomen with the gamma <:amera to .ule out direct injection
mwdistol tubing. Image the cranium to verify now intoventridea (proximal paU!ncy). If
spontaneous now into abdomen is not seen after 10 minutes t.he patient is sat up and rescalUled. Ifllow is not seen after to minuU!$, then t.he shunt is pumped. LooII: fer diffusion
of the isol4pe withill the abdemen to role out llII\!udotyst formation aroWld catheter.
X-ray "s bunl·o-gram": aner tappilllf the shunt. drain ~ I ml ofCSF and send for
C&S. Ir;je<:t e.g. iohexol (Omnipaque 180) (see palft 121) while octludinK distal lIow (by
<:(Imp.easing valve or occluding portal.
S HUNT INF ECTION
See Shun'
inr~clion
on pOKe 214 fo r evaluBtion and treat.menL
" O VERSHUNTIN O"
POSSIBLE COMPLICATIONS OF OVERSHUNTING INCLUDE"-"
l.
'"
$Iit ventrides: including slit ventricle syndrome (:ret!
II. Hydrocephalus
~fcu,)
NEUROSURGERY
intrat.anial hypotension: fU bIIloUl
subdural hematomas:"" pag~ 198
erSniO$ynoel.oeis and microxephaly; <ontrovl!l"$ial (fU pngt 199)
stl!noeis or occlusion of sylvian aqueduct
10-12... of long-term ventricular ahunt patieots wi!! develop one of the above problem ..... ithin 6.~)'l"8 of in itial I hunt ina"'. Some nperta feel that probleml relaud too"ers hllnt;na cowd be m\lIted hy IItilizina Lp , hllnl.l for communieating hy~phalll', .... d
r"erv;na ventrieular . hl,lfl!.ll foroburuetive HCP". VP s hun ts may allo be more likely to
overd rain than VA Ihll nts beelllie of the longer tllbing- INaler s iphoning e(fett.
2.
3.
4.
5.
I NTRACRANIAL HYPOTENSION
AKA low ICP . yndrome . Very rare . Symptoms limila r to thOM oflpinal HlA (poa.
turll in n.tu.e. u.l.ified by mumOOncy). Althouah uSllally not .ssociated with the fol,
IoWLnglymptoml", the" m.y occu ....; NN, lethlrgy. or neW"Ologic 8ian8 (e.g. diplopi ••
UPflIU! palay). $oml!timel the Iymptoml resemble thOll! of high ICP ncept that t hey are
relie'lfil wheo pron.ate. Mllte effects that m.y occu. indllde": tachycardia, lollS of oon.,now ......, other br. in atem deficits dlle to a roatral.hift ofth.. intracranial cont.:m ts or
to low [CPo
Etiology i, I.iphoa ina .ff«t due to thl! column ofCS P in the ShW1t tube when the
patient iI erect-. Ventricles m.y be llit·li lte (u in alit "entricle syndroml! (SVS))or may
be norm.1 in appearance. So~timel it i. OI!OI'IIIU)' todocum.."t a drop in [CP wh en iIG'
ing from .upine to ert'Ct III diagnoH thil condition. ThI!8l! patients may alro dt'Velop
Ihlln t occluaion .... d ~ the distinction from SVS bill" (..... bt-Iow).
With _hon-term Iy mpto ...... n ASO is the treatment ofclwice. However, patients
... ith Iong .. tanding over!lhunting may not IlIleratl! I!fforti to retllm intT.ventriclIlar pres·
lllre. to norm.l It'Vel .......
SLIT VENTRICLES
1.
uymptomatio::
A. . Iit "I!ntrides (totally collapsed l.tera! ventricles) may be seen on CT in 3·
8O'J:of patients .ne. ahunting"'-". most.re a.symptou>atit
B. these patienta m.y occ.as.ionaUy present with l)'Dl ptoJUlllnrelated to the
. hllnt, e.g. troe migraine
2, 51it ventriclel)'lldrome (SVS): _n in < l~ ohll shunted patil!ntl. Subtypea:
A. intennittl!nt shunt occl usion: ovel"$hllQtinglead. to ventricular c:ollap$f
(Ilit ventricles) which caulles the ependymal tioing to occlu de the inJet porta
of the vlntriclll.. catheter (by l:OIIpt.ation) prodllCing s hunt obIItrllCtion .
With ti...." many oftheH patientl develop low ventricular oompliance"'.
where t'Veo minimal dilatation results in high p","ure which prodUCl!ll
Iympt.oml. Expanaion then f'lentu.lly reopell8 the inlet porta.Uowing resumption of drainage (Mil« the intermittent Iymptoms), Symptom. may
rnembleahun t malfunction: intermittent .... ad.d..!s I,lfIrelated to pMtu.e,
onen withNN, drowsiness. irritability .nd impaired menuUon. Signa may
include6tb cranill nerve palsy. Incidence in Ihunud patientl! 2·~""""_ CT
or MRI .can. may aJao .how t'Vidl!nce oft ...... epeodym.t .bilorption o(CSF
B. totll,hWlt maUimttion (AKA nonnal volume hyd.oc:eph.lu"'): lilly occur
Ind yet ventricles remain Ili t-like if the ventricl .... c.nnot expand betau.
oI" l ubependymllgliol;'l, 0. due to the law o(Leplaee {whidlltatH th.t the
praIIU", required llIeapand .I.a.,.e container .. 1(....... thIn the pre"u'l! reo
quired to expand. Im.U container)
C. VInoU' hypertension with norm.llhWlt funttloo: may result from paTti,1
veoo ... ocdlliioo that 0«11" io 110m. conditionl (e.J..t the lev.1 of th,jug_
IIlar foramen in CrouUln', Iyndrome)_ U'lIllIy sub.idea by adllithood
3. ....... patients with IdioPfotbic intracrani.1 hyputention (ptI!udOtllrno' ce.ebri.
_ PfJIll 493) ha", .1it·Jika ventridu with COf\Iillantly ,l,vated ICP
4. intraCTInil1 bypotl!n.lon: .ymptom. onen relieved by recumbency (_ llbotoor)
EVAlUAnoN OF SLIT VENTRIClES
Th e ,hllnt v.lve fill ' .Iowly ifpUJllped whl!n thl! ventrides Ire ooll_pHd.
Monitoring CSF preesllre: eitheT via illmbsr dr.in . or with. hllttl!rOy in ... rted into
the ,hllnt re ... rvoir(wltil thil method , preU llrecan be followed during poItll.al chan ges
NEUROSURGERY
",
to look for MKali~ prn, untt when upright; possibly higher risk of infection with thi~) .
The.. patientl Ire . 110 monJtored fo r pr.U unlt spi kes, especiany dunng ,leep.
Alternatively, th eM patiwu may be evaluated by "shunt-o ·gtam" (Ht aboutl.
TREATMENT
In Iru tinr II pa tient with . Iit ventridell in imaging studies . iti, Impo rtant to aacer·
tain int.o which of the " e&tegories (8ft .. bow) th e patient fal1a. [fthe pati ent can be catego:lrited, then the '!!<ki ne treU ment li sted below should be employed. Otherwiee, it if
probably most common to initially treat the patient empirically as intracran;al hypotens ion , and then to move on 1.(1 Other method . for treatment failu reti.
Asymptom a ti c , l it ve n tr icles
Prophylactic upgrading 1.0. high er preH ure valve or ;nMrtion o( a n an!iaiphon d~
vice hul_llIel}' been abandoned . However, thia may be appropriate at the !i llM! of.hunt
revis ion wilen done for otller realOna" .
In trac r a nial h ypote n s i on
Postural lilA due to In tracrani. lllypowMion (tN tovtrslluntingl it u. ua IlYHlflim.
ited, IIoweve r, iflym pto~ PI! ... iet af't.er _ 3 da)'ll of bed . rU I ar>d an.!&uica and a trial
witll. tigllt abdomi nal binder. \.he valve should be cllecked for Jlf'OPI!r elMing pr ... u ....
Ifit ift low, ",pl.Cf! with. higt.erpreu url valve . lf il i. not low, an .nthdp ho n device
(ASD) (wllich. by itself. al$O increases Ihe ru;ll.II nce of the Iyawm) .Ione or logether
with" higher preuu re va lve may be needed" .
S li t ventricle syndro m e
Patients wi l h aympto ml ofSVS Ire actually .ulTerin, from inwrmllwnllti61t praaure.lftotaJ ,hunt malfunet i(m iI the ea ... se, then I h ... nl revilion;1 ,,,diQlted. For inter·
mittent 0«1","00, treatmeM oplions include:
1. if sy mptom. 0C<:Ur early alter , h ... m inaertion Or revi.io", in;li.1 expecta nt ntln·
.gement may be indicated "noe aym ptoml wllllpontalltomJy relOlve in I1).IIny
2. revi sion of the pro:timal.hu nl. TIIift m.y be difficult d...e to lhe Imall.;ze oflhe
ventricl es. One c.n sttempt to follow t.be e:tilting tract and '..-rl' Ioneer or
sborter length oft ... bing based on the pre-op imaging at<>dies. Some adVOC"llte the
placeme lll of. seoond ·,entrieular catheter, leavillg Ihe fintone in place
3. patienuo maY"relIipond" to either of the fonowing interveMio ... bec:.... ae the . Iighl
ventricular enl.rgement elev.tea tbe ependynlll off oflhe inlet portll:
A. val ve upgrade"o r
B. ASO insertio n"."': the procedu re ofchoice in $Orne opinio ...... Fint de·
""ribed in 1973*'
4 . l ublemporal decompression""" sometimes with dural lncisior.... Thia re.... lts in
dilal.lllion orthe wmporal hol"TU (evidence forelevated press ... re);n 1nOJIt, but not
.1l'" cll5"
5. third ventrie ... IMtorny": 1ft ~ un
P r oble o •• u o r e la ted t o s h u n tin g
For lilA ""MiSleIl! with migraine th. t are not pollural , . trial with migraine-epecifle medicationl ;. warranted ( riorina~ ... " rottre.tment ofidiopat;,ic intracran ial hypertension (pselldol ... mor cerebri ). _ ~ 497.
S UBDURAl. HEMATOMAS
M.y be d ue t.<>collapH ofbnin with leari", ofbridging vei .... ln me pre-C'T era, the
incidenc:e of , ... bd" r.l hem. to"'. (S DH) ronnation rollowlo, , bllnt ;naertion WIl5 probably ","de. . limated 11 _ I .~ However , more recent eatima t.es are 4·23'lo in adlllts, 2.85.4~ in children,.nd i' /ugher wi th lIOm>al pres.ure h)"d rocepb.l ul <:20-46'1» than wilh
"hyperte",;ve hydrocephaills" (O.4-MI» ...... The ri.k of SDH i, higher ;n the selti"ll of
lotlg.etandinC hydrooeph.l .... with I 1.1"1'1 hNd and little brain parenchyma (crani~re­
bral di'proportion) with . th ill cerebralONlntle,'s .... lIally occunl in childretl with maeroceph.ly and I'TilI ventridef on ioLtial eval .... tion. The.. patieota h"ve an "ext remely
deliCIOIe baI.nce be tween .u b\hJr.llnd intrlvelitriaJ.l' r pre,,"re'"". SOH c;an . Iso follow
. huntinc in elokr ly p'tienll who have levere bra in atrophy, The development of SOH
mly _1&0 be f.c.litated by n . tive preM ..... io the ve-ntriclea.,. relllil or .iphoningn .
". There i•• 1&0 a low ril k of epid ..... l hemalofn. following CSF ahunting" .
Ch . raelen , t i". o r lbe n uid : The colleclionl ONly be on t he . ame .,de .. the , h"nt in
32\(" on the opposite .ide in 2 1 ~,. nd bilateral in 47i1t ...
".
11. Hyd roceph.l ....
NEUROSURCERY
At the ~iltle of dillCOYery. ~he SOfu.~ u. ually . u bacute to d'ITonit. and the p~vi .
<>WIly large velltricle . ..e "" u.lly eol1apud. Only 1 of 19 c.. ~ 6howed colorl eM nuld " .
In all caSH tated. protein ...... elev.ted compared to CS F.
TREUMEWT
In dicatio n . fo r t reatn:l.en t
S mall « 1·2 Cm thick) asym ptom. tic eol lect ion. in patien t.ll with elated cra nial au·
lurn may be follo .... ed .... ith Kria l imaging. SOH wel1l Iymptoroa~ic in ~ 4 ~ of caSf!S
Clymptoml ofieo Tfl$flm ble thoee of , hunt m. lfunction). . nd the~ ~uil1l treMment.
'J'natmeotofSDH in t ll ildren .... ith open lutura h .. been ad vocated" to prevent later
sym ptom • • ndlor fU,ve lcpme nt of macTOCrania . Many . uthors .-.t(Immflnd not t rta ting
a.ymptomatic I"iolll reprd leM of 'ppu ranca'" ", wher1'as others vary their recom'
mendation. b.aed on di~flI"H criteria includinc . i:u!. appeaTllnte (chronic. acute.
ralxed ... ). ek.
Trea t.m e nt tec h niqu ee
A numberoftechniqut. lIave been detcribed . M(lft involve evacua tion of tile S DHs
by .ny of the ul ual methodt (e.g. burr hole. for ehronic ool1ections, craniotomy fOT acute
eol1ect iOOl) lOfIether with :
1. reducing thao.P""" or .hunting Ci.• . tontabli.1I alower pr1'ssur1' in the 8ubdu ral
Ip"<e th.n io the intravenlrirul. r Ipace. toUUSf! the ventricles to ra·upand and
to prevl!llt ra.a:umulation oI"thl SOH)
A. in shun t dependent c._
1. repjaci nC the ~.Ive with a bia-ller prl!llure unit (upgrading the \/IIlve)
2. inc:~ing the prl!Uure on a prognommable pl'flSllu re valve"'''
3. uling a Ponnoy device that can be turned ofT and on externally. Be
l ure that ure pTO>'ldeTl U n reliabl y open the device in an emergency
B. in non·ahu nt dependent c. _
1. .ny of the methods outlined sbove for sh unt dependent cases, or
2. temporari ly tying 01T the.hunt"
C. inse rtion or an antj-aiphon device"'
2. draio.gl or the subdur.l 6pe<e to
A. the ci!~",a magn.'"
8. to the peritoneum with a low presllure valve (or novalve"). Some authon
have the Ure-gLver rrequently pump the su bdur ..: valve
The goal iA to acb~ve a deli ... te balll...,., bet~n undershunti"ll" (producing symptoms of active hydrocep/lalua) .nd overshunting (promoting the nl.um of the SOH>. Fol_
Lowing lurw"ry the patient should be lI)()bili:u!d slowLy to p~ent recurrence of the SO H.
CRA NIOSYNOSTOSIS, MICFlOCEPHA LY
& SKULL DEFORMITlES
Also see Cronwl)'tWntotir. page 99. A number of skull chan," hav, bHo deacribed
in infants after shun ting. indudin,",,: thickening and inw ard growth of tile bone oftbe
skull base snd crani.l .... ult. decrease;n li:u! or the sell. turcica. reduction in lile of the
cranial foramina . and cnmio. ynostosis. The moat common. . kull del"o.lII ity wal dolicl!ooeph.ly from llllgittalsyno.to&is" . Microcephaly lICOOunted for ~ 6""of skul1 derormi·
ties after shunt,nc {.bou t haJfofthese had IRlgi Llal 1)'I"I05\ol1i.). Som, ofthoete ch. nget
werl reversibl e (eue pt .... hen complete I)'1IOIIlO5il WII present) ifiO\.raCl"ln iai lIypert..n ·
lion recurred.
11 .3.
Normal pressure hydrocephalus
.
I
1 Key feature s
c1.ssic triad : dementia. Ca it disturbllnce. uriMry ineontinence
• eommu nicating hydroceph alul on CT or MRI
• DOrmat prell$ ure on r~ndom LP
• symptoms remed i.bl, with CSF . hunting
Flnt d~bed io 1966". nonnll l prenure hydrocephilu l (NPI{), AKA H.kim·Adsm. syndrome.
~ originally deacnbed. the hydrocephalul ofNFH Wit considered to be jdiAAllthk.
NEUROSURGERY
11. Hydroeephlllu.
".
However. in some ca~ an etiology can be identified:
1. poat.-SAH
2. pOIt-traumatic
3. post-meningitic
•. following pntIterior fos!a .urgery
~.
tumors. including carcinomatous meningiti s
6. also seen in ~ l~$ ofpatienUl with Alzheimer's d isease (AD)
7. denciency of the arachnoid granulations
8. aqueductal stenosis may be an overlooked cause
C LI NI CAL
Age usually> 60 yrs . Slig-ht male preponderance.
C linical tri ad"
T'liad is not pathognomonic, aod may al so be seen in vascular dementia" ,
I . gait disturbance: usually precedes other symptom$. Wide based with short, shufmng step!! and ullSteadiuess on turning. Patien~ of\en fool like they are "glued
to the noor- (so-caUed "magnetic gait-) and may have difficulty initiatingsteP8 or
turns. Absence of appendicular ataxia
2 . dementis: primarily memory impairment with brndyphrenia ':slowness of
thought) and bradykinesia
3. urinary incontinence: usually un witting (NB: a patient demell led for any rell80n
Or with mnbili ty impa.i~ment may have in.:.;,ntinence)
DIAGNOSTIC PROCEDURE S
There is ill:I test nor radiographic imaging thst is pathognomonic (or NPH. Numerous diagnOllticmteria have been proposed for NPII to determille which pat ients are like·
ly to respond to a shunt procedu.re in order to avoid poteotial complications (1ft below)
and Wlnecesaary surgery without denyinl surgery to those who might possibly benefit.
None has proven to be of adequate reHabi ity. Some are presellted here for complete"':''''.
LuMBAR PUNCTURE (LP)
Normal LP opening prt'u ure (OP) should be < 180 mm H,O. The response to a single LI* (withdrawing 1~-ll0 ml CSF. or taking the OP down by ~ OM third) OT to serial
LPs may be of90me pred.ictivto value. Consider ambulatory lumbar d,.s.inage b~ below)
fOT patients who fail to improveaft.er a s ingle LP. CSF should besent for rnutine labs(_
page 616).
Patients with an initiol OP > 100 mm H 20 have a higher
respon~e
rate to shunting.
CONTINUOUS CSF PRESSURE MONITORING
Some patient,., with a normal OPon LPdemon$trnte pressure pealul > 270 mOl H20
Or recurrent B-waves". These patient/l also tend to have a higher response rate to$bunting.
AMBULATORY LUMBAR ORAI/JA GE"
Lumbar sub8 radmoid drain is pLaced with Tuohy needle. connected lhrough a drip
chambe r to a dosed drainage ayst.em. The drip chamber is placed at the level "fthe pa_
ti ent', ear when recumben t , or at the level of the shoulder when sitting or ambulating.
A properly functioning drain should pul out _ 300 mI ofCSF per day.
If symptoms of nerve root irritation develop during the drainage, the ca theter
should be withdrawn several millimeters. Daily s urveillance CSF cell COWlta: aDd cultures fihould be performed (NB: a pleocytosis of ~ 100 cel1111mm 3 is expected just with the
presence of the drain ).
A ~ day trial is recommended (mean time to improvemen t: 11 daya).
CT ANDMRI
FeatUCil8 Qn CT"" and MRI"
I . prerequisite: communicating hydrocephalus
2. features that correlate with favorable rt'sponse to shunt (thes e featUrES sugge..c.
that the hydrocephalu, ia1lll.i due to atrophy al"ne"):
11. Hydrocephalus
NEUROSURGERY
peri~ntri~ula r low denaity on CT or I'Iigtl inteluity on '{'2WI MRI: may rep!"eRnt tran.ependymal ahllorption orCSf'. May re!lolve wittl . tlunting
B. oompresaiCtn of<:On~";ty l ulei (foca/.ulea l di lation may sometimes be,eea
and may represent atypical ruervoi ... of CS f' wtl ,ctl may diminish a~r
, hunting and should not be OOfUIidered IIlItrophyt')
C. rouodiog of the frontal hom,
A.
Nthough some PIltienu improve wittl nottlan~ in ven t rides". el ioiu l improve·
ment mOlt onen aecomPllnies reduction o(ventricula r lile.
RAoIONtJCLIOE CISTERNOGRAPHY
Usefu lnes, remain& eontroveni,1. One , tudy found that the dltemogrllLll does not
increase the diarnOlt ic accu racy cl clinical and CT criteria"',
T ec hn ique: Lumhllr auh Nlchnoid iQjec:tion orradio-i$OtOpe ('g. 2.7 mCi of"""c-IYJ'PA
diluted 1.0 I cc .... ith IIII line). Cilternorrarnll are obtailltd by planar adntigra phy at 3. 6.
and 24 tin after injlC~n ( iOl~ may be obtained at 48 hn if intnventric:ular activity
i.still_n.t 24 hn, tlowever . an i.otope other than-rc-DTPA mUlt be used for , uch
del,yed Uw.ges).
Con ventio nal crit eria fo r a ~ atudy: Radioactivity i, .y~trieaUy di,tribut·
td over the COGyex.ity 24 hn .~r il\jeetion. with no intraventricular activity at any poin t.
However . up I.D 4 1'-' ofnormal, will demon, trate trllNli .. nt (up to 24 !tn. but not longer)
activity in the yentricl....
Findings that may indicat e a bette r ch ance. fo r respon se to I hU"li"if. Of the fol·
lowing. on1Y' 2 i, a reliable marur for NPH.
I. el1ly acan ('·61lts ,fter il\ilCtion~ activity in ventrides (presumed retlUJI from
obac.n.u:ted outRow). May al.o occur in DOnJIal. (_ "buw) for < 24 hn
2. I'te acan (48·72 h n ): peni'tence ofventrieular activity. Pat ient.. with this fi nd·
ing are mott likely 10 impmve with , hunting !_ 759l. ctlanee)
3. ~tained activity over ronvexity: these plltienta are Je.1ikeJy to improve
4 . quantitative c:iater rlO(Taphy
A. pIItlenta who dear oYer 5O'il>0fl.l!Yl. intracranial radioactivity within 24 tin
, re OOfUIidertd to .... ve an adequateove,.lI abo\orptlon rate, and are unlikely
to improve wittlltlunting. However others have bund no conelation of
clearan~ to shunt rt!Spon5e
S . one l tudy found thn If the ratio ofventrieuta r to t.otal intracranial actiyity
(Vfr) at 2~ tlOUrll il > 32%, there would be a responae lO ahuoting. wherea,
Vfr < 32% did DOt exclude th .. possibi lity of impmvement"
M ISCELlANEOUS
Cerebra l blood now lC BF ) measuremen t.a: Although some Iludin indiea~ other·
wile. CSF measu remenlS show no lpeel"c "ndings in NPH, and are not helpful io predicting who will respolld to shunting. However . inlnNed C 8F a~r ,tlunting ~Iates
wit h cl inieal improvement".
EEG; No specific findir.g. O<l EEC in NPH.
TREATMENT
Be(ore undertaking a surgical procedu re. , dementia workup ,hould be t:Ompleted.
VP sh unt il the procedure of choice. Lumba ,.. peri l.oneallhunta have been used. but
they tend to overahunt. In general, ule a mediym prwYrf valve" (clneing pTelllure M·
90 mm H20) to minimiu the risk of subdural hematotn"(_ ~DU!), althougtl re1Iponte
rate may be tligtler with a low·pre.. ure valve", C .. du,lIy ,I t patient up over . period 0(
l eve r. ] daya; proceed more .Iowly in patienu who develop Iow-presaure headachM. FoI·
low patientll clinically and with CT for - 6· 12 monttll.
Pat ienlll .... tlo do not improve and w~ ventricln do not eblngl . houJd be eval u·
ated for shWlt malfunctioll. rfnot obatructed. a lower preuure valve mou ld be tried .
A.
.1.,
(h¥<I.-ph. ,u, .. ~ ... uo).•,In ooBdiUo"" ,1O<h .. h1lhoi""'r'.d;... ... ,.....,. "'" tha_
of. but doH ........... Iud., rt:l:""dinc WI. ""unl (ooJ1l<.I.<n>phy io . OOID,,*, rind;"';" 1>0011.11,
1 I'1d,~idu.l. of.d•• ntt<! .... )
NEUROSURGERY
11. Hydrocephalus
'"
PoTENTIAL COMPLICA f /ONS OF SHUNnNG
Com plitoti"n ra~~ may ~ III high a~ ~ 35% {due to the froWlity Ilrthe elderly brain~' 'M.
Potentl .. 1 M1npiicotions indudalO':
L subdu ral hem~tomlls Ill" hygroma (also _ ~e 198): higher rif,k with 1_ press ure va l ~ and old.e . patieots wbll to'nd to have ",,",bra l Dtropl'ly. Usually acco01panied by h..OOo[h ... m.... t re.solv",pontanl"QOJslyorrenlllin stabl ... Appr,,~imBlely
0 ..... thl"td ",quite evacuo tion and tying ofl" orshunt (teml"'rllrily "r permanently),
Risk may he mlucW by gradual mObUiJation pll5H'P
2. s hunt in fection
3. inLropan'nchymal hemorrhage in the brain
4_ J;l"i~urell : IN pagf 188
5. delayed INlmplkatioo& H.dude: Bhu nt ob$truction or disconnection
O UTCOME
li kely symptom to 'mllrove with shunting is inconLioe~ then gait dl$and )/lsUy dementia Slack et ai ," 81"'" th e following mark~rs for gOOd and,·
dates for improvement with shun ting:
clinical i presence of thO' cla6l!ic triad" (II" PClIJ6 2(0). Al ... 77... of patienta wilh
gai t di stu rbance liS thl" prim ary sympwm imprllVed w.thsbunting. Patients with
dementia and lUI gait dilitur bllnce rarel)' respond to .u.untin g
LP: OP > 100 IIUJl H.o
iSlltope eis lemOi,.,.,.m: t,ypical NPH pattern. The n,i>:ed nr normal pat~rn has no
INlrrelation ..... ith responlle to ahunti ng
C'(\nti llU OIl$ CSF presl un recording: ,""sure> ISO mm H.,o or frequent Lund berg B wa~ea (_ pagtt 653 )
CT Or MRI: large vl!ntrides with f)auened $ulci /little atrophy l
Re!ponae is better whenlymptoms have been pruent (IIr a shllrter time.
NB: patients with suspe<'ted eo'existing Alzheim<!r'$di5ello!Sl'. (AD I mlly Ilill improve
with VJ' lhWlt.s, thUII AD ihnuld not e"elude theM! pa tien ts from shu:ltin g.... _
Smne ",sl'ondel"ll may s ubsequen t ly det.\lriorale. Shunt mstruILd;on and subdu r81
oolledioni must be ruled out before ascribing th is to the nAtural OOUr5eOflha ronditJon .
The
tu rba"~e,
11 .4.
m05~
Blindness from hydrocephalus
A rare complication of hydrocephalus and/or shunt m.lfu n~t io n. Possible ca uses include:
I . o«lusinn ofpost.eriorc. rebral ar(.eriH (p e A) CAused bydoWll",.rd IJ"Dnste ntori.1
herni ation
2. chro",[ pspill edemu causing inj ury to optic oerve at the nptic diK
3. di latation of the 3Td Yl'J'ltriele with tt1 mpn!MiOIl of optic w iasm
Orular motility Or visual field defects are ",ore common with sh'JILt malfunction
than is blindn~ l"'''. On"""'nes found 34 repMU!d c.se\l lIfpermsuenLb)iodne.s.ll in children attri but.ed to shunt malfunction with Mncomilant increased ICf»f' (thu e au thors
w"re baM<I;n. "'(" ...... 1cente r farri8u" lIy tm pa.i .... dchadren. t hua incid .." "" not ulim~t.­
ed ). Another ....ries t>f 100 pa t ienl$ with tentori al herniation (mos t from acut.. EOH
lind/or SOH) proven by CT; 48 patients opel'lloted: only 19 of 100 surv ived> 1 month \,U
were in operated group): 9 of LOOdeveloped occipita llDbe infarct (2 d,ed, 3 vegetotin
stat.., remaining 4 moderate to severe di8~bilityl'·
TYPe s OF VISUAL OlSruRBAloICE
9 ofH had pre~c:ulll~ (IIJIt..ri Dl" vil;ull path ... ay ) bJindneo.s w,th markO!1i optic
nerve atrophy {earlyl, 8nd reduced pupillary light rene~e •. S of 14 had postgeoic ul ate
(cortical) hlindneu with nonnal Light reBponMI and minimal or nO opti~ nerve at'mphy
(Dr atrophy late). 11 few pllti entl; had evideote of dam age in bolh s ite• .
Cortical hliodnelll: due Lo leti 'ol\.S po.9t.erio r to lateral gerucu)8t.. bodiea (L e B),
may also he """'" with hyV"'Oc illjuriea or trauma''', ()eao,sinnalty 8590ciated with AnIoD'Sllyndrome (denial ofYi!ual defidt) and with Ridoch'8 phenomenon (appreciation
ofmllVing obj«UI wi thout jltin:eption of stlilion.ry u.imuli).
'"
It. !1yd rocephBl us
NEUROSURGERY
PATHOPHYSIOLOGY
In patie nts wit h occipital lobe infarctio n
Ocdpitallobe infantioos (Q Ll) in PCA distribution areseen either hilaterally, Or if
unilateral are associated with other injuries to optic pathways poIIterior to LGe. The
mOl;t often cited me.:hanism is compreS!lion ofPCA .-esulting from brain herniating
downward. Alternatively. upward ce.-eheUar herniation (e .g. from ventricular puncture
in face of a p·fO$$a ma5'l ) may i,mpinge on PCA or branch"" with !,he !;arne re$ultll"'.
OLb are mOre likely with a rapid riseio ICP (doesn't allow compensatory shifUI and
collateral circulation to develop)' ''. Macular sparing is common.
Reported ca uses ofOLI include: post traumatic edema, tumor, aba~, SDH, unshunted hydrocepba lU5, and shunt malfunction"" " ' .
The occipital poles are also particularly vulnerable to diffuse hypoicia''': attested to
by case.a of conical blindneM aner cardiac arrest"'. Hyp>tension s uperimposed on compromi$ed PCA circulatioo (from berniation Or elevated ICP) may thus increase the risk
of postgeniculate blindn e"",'''''' "'.
Both coup and contre<:<>up tral110a may produee OLI. Unlike a PCAocclusion infarct,
macu.lar sparing is not expected in traumatic occipital lobe injury'''.
In pa tien ts witb prege nic ula te blindness
Elevated ICP transmitll pressu re to retioa - blood now st.asis, as well as me.:hanical
trauma to optic chiasm from enlarging third ventricle (latter more commonly thought.-esponsible for bitemporal hemianopia''', but could, ifunche.:ke<i, progress to complete visual 10&8). Also, if hypotension and anemia were present. consider the possibility of
i$Chemlc optic neuropathy" ""'.
PRESENTATION
These deficits a.-e frequency unsuspected (altered mental state and the youth of
many ofther;e patients'" makes detection difficult): an examiner mun persevere to detect homonymous hemianopsias in an obtuoded patient' ''.
Pregenitulate blindness is less often associated with depressed senaorium than is
postgeniculate (where di reet compres.sioo and vascu lar compromise of midbrain are more
likely'·').
PRooNOSIS
Conical blindness after diffuse 9noxia frequently improve~ (O<::<:88ionally to normal):
usu9lJy s lowly(we-eks to years quoted; several mos usually sdequate)"·. Many reports of
blindness after shunt malfunction....., pre·CT era, thus the presence or extent of occipital
lobe infarction not ascertained. Some optimistic outcomes reparted' ",. however. permanent blindness or severe visual handicap are also de8Cribed" ~ "; no reliable predictor
hss been identified. AB with infarcts elsewhere, youager patieata fare better"', but extenSive calcarine infarcts on CT are probably incompatible with signific8Ilt visu al rElcov·
.ry.
11.5.
Hydrocephalus and pregnancy
Patiellts with CSF ,hunt.$ may become pregnant, and there are st least 4 case reports ofpatientll developing hydrocephalus during pregnancy requiring s hunting') '.
With VP 6hunl'l, distal Rhunt problem s may be higher in pregnancy. The followillg
a.-e managernent $ugge~tioll$ modified from WiJloIJ etal." ' .
Precon ceptio n manage m e n t of patients witb s bunts
I.
2.
evaluation, ind~ding :
A. evaluation of shunt function: p.-econceptiQn baselme MRI or CT. Further
evalua tion ofsbunt pateocy ifany suspicion of malfunction . Patients with
slit ventricles may have reduced compliance and may become symptomatic
with very small changes in voll11Oe
6. assessment of medications. especiaUy allticonvul! ants
counselling, includiog:
A. genetic co~n8elling: if the HCP is due to a neural tube defect (N'I'D), then
tbere i, a 2-3~ cbance that the baby will have a NTD
6. other recommendations include early admini$tration of p.-enatal vitamins,
NEUROSURGERY
1 \. Hydrorephalus
'"
and Ivoidinlleratorenie drup and exce"'''e heat (e.g. hot-tube): """ N£urtlllu~ de{«II, Ri,lt. {aclo,.. on pare 113.
Gravid mllnage m l nl
I . dOH obMT'Y&\ion fo r sim. of increased l e p: h•• daclle, NN,le:hargy. ataxia, Mi·
utre •... C.... tion: these sim' may mim ie pre·edam!»;. (w hich mUltalllO be ruled
out). 58~ ofpatienta exhibi t . iil\1 of; nerea~ [cr, ... !lith may be due to:
A. detom~n .. lion cf pa n ial.hunl malfunction
B. shunt mllfumt;!)"
C. lOme .now .ignt ofincreltHd Ie? in ' pite ofadequ.t.e .hu M funttion, may
be due 1.0 inereal ed cerebral hydration and venous en,o~ment
D. anl. Tiemant of tumor durin, prernancy
E. cerebral "tlMU' tnromboa;': including dural sin .... thrombosis &. cortical
venou, th rombo.i.
2.
F. enceph olopathy reJa~ to di.o«ler«l aut.oregulation 1_1K>8t 64)
patient. developing symptoms of increased Ie? Ihould hve CT Or MRI
A. ifnoehlng.. from pr_n.:..ption ttudy, pu rw:turt ,hunt 10 meu .... ICP and
(UILUre CSF. Coruider radioilJOtope .hunt ...·cram
B. if aU studies are aegalive. then phy.iologie chaagN may be reapollaible.
Treatment is bed rest , nu(d .... trietioa, iltId in ....ere eua . teroi.u ... dfoT
diuret i"'l. l f symptoms do notabate, then early delivery it recommended a.
soon u fetallunK maturity ean be doeumented (aive prophylactie antibioties for 48 h .. bef~re d..!iv.. ry)
C. ifv .. ntricl ... have enla'lled and/or ahunt mal function I, d tmon.tI'a~ on
testin,. shunt revision is poI'rforO'led
I . in first two t rimute .. : VP shunt is prefen-ed (do not 11M poI'ritoneal
tl'ocar O'Ietho:)d afte r Ilrst trimester ) and i. tolerated well
2. in third trimester. VA Or venLl'ieulop]eural .hunt i. u8ed toavoid utero
ine tl'auma Or induction ofl,bor
lnt r aparlum manageme nt
prophylacticantibiotico af .. recommtDded dUMKlabor and o..livery ton!lluoe the
indden.:.. orshunt infection. Since coliform. are the most common patnog..n in
L&D. Wisoff et al . recommend aO'l picilli n 2 gm IV II 6 hrs, and xentamicin 1.5
mgl'kg rv II 8 hrs in labor a nd a 48 hrs post pa rtum'"
2. in pa tien~ without symptoms: a vagina l deliver)' is performed ifobst.etrieaUy
. ible (lower risk of forminX adhes ions or inf«tion of distal shunt). A shortened
second stage i, pre fe n"N since the inerease in CSF pressure in this Btage i, probably greater than duri", other valsaJvl maneuve.. '"
3. in tbe patien t wbo bea:omes symptomatic near term or durinKlaoor, after stabi·
li ~i.ng the patient. C-oteCtion under &:enera] anesthesia (epidurals arecontraindi·
cated wi th elevated ICP) is performed with careful nuid moni~"II (LK. PA
ca theter) and, in ..,vere cases. steroids and diuretiet
1.
re,-
11.6.
,.
,
•
,
'"
References
bo-""f"".
~",iIo" I· _ol ..
J,uu,15,,","
62,19"
$ootIoo L N • . . - D A.S<ftoI L H~J
"'. ,,11101 ~~
, _ <1.....
<ol.lwiIICt_. --.,...,. 6, ] l ••• 1910.
Uob1;aA B. F.."", B N' ~ c .........Il10.
'_""~oocq:fIal7·"'_ oI1 J .....I..... ~
,it ................. "" .......... ~
....1oIoU 1)7 11 ·91 . 1910
... ,,_ 0 I), Ntto,~ of 101-,- """ doiId·
_ .1........a..",..C~... 5prio:JI"..1oI. 1969
......... L .. . I-Io) ..IJ . Sfu_S ~ .........
...s"J"""'phoI.., N_oJ.....,._ ..
.bo<oI ••
77.
901 · 7. 1M6
_ C F- CSF dr-MI'''' '" hydOUpIooI<ft . ...III
<pot'" _ .............1
Do.6. 119-17 . 19101.
ao-t w M.a . - t J I , ,,,,,," FA n.. ......
_
....
••
..
......., »'167·7 1. 1992
~,II;W.y...u.J IW . _""J W.
S - .I..,........ _
..... .............. _
......., ... MII _
•."'. A,/NR 11; , J»,9.
'M.
h}'droccplootu.
_J_
_
_
K.... I B.Goodonoo
M. Dirra.
.....,..
0. .......
s.r.
N _ ». ~. 1M
McIoLR . Dwoo_CC. OnIorR 11..,,"' ...1.....
".
_LN
Ioc_....,
"
,m c-.-',....,...
,_IioI_""""'r"""......
"""EL. SIoUJII..rrOI
J _ ....
..,...,..""u.. ... " .....,.
--......
..-.,--.-
I I . Hydrottphalus
_ .. "" ...... _
............. ""... . J
- - . S<I. »0·' . 1911
CW-O _ _ ""h1~
.....1Ma
'lI19 (11 ~ 1·7 •
Fi_ _ .........,.....
""~)'OIr«<!*>1"
io <lulilna wi'~ _
.,...._1111 <_.)
"".
" .......,..,0.10"" ...........
a.t_HL."""""'E. _~
... _
, .10. 1064·79.
H t... .. oI : ........ "" .
1"...."'" M-V
NEUROSURGERY
".
"
"
".
"
".
".
".
".
D
".
D.
M
".
".
n.
~.
".
".
».
~
"
M.
".
N..... I S<! I, 123·6. 1982 .
1l¢I'UfG J. De wI< S ... , Sh ... ·ir<l< ~ n<k .. >I.
'u. olh)"'-'<phoJ ... J N<u ....... 19: 691·1"01.
19"13.
1lc""""R· C,. "hu"be .. ~'M_ N... •
f.1 Sd.: 221·1. 1911.
EpoIo" f : ~_i ..... _
..... '" of......, • ...,
hydr<>«p<alu,. Moooov "'....... Sci.: lOP. 1912 .
LoMoy M.Koohbutf K: V",,,... llJdiff<<t., ..
boow«. ~y""",","", h)U<>«pII.I • • and hydro«pII.
Cl". /'I.uf_1oIou 11: 191·S.
• 1•• 0.
1919.
A",",II« A L. Wolli "l_ I. Inl.... i .. hydro<.piI.
II .. : 1.o"l.l<rm raul .. or ....,icll 'II< ~ . Cblld<
B,.1n II : 111·19. 19&4.
Kill .... Rozd;llky B: Ccn&<";u l hydfOO<i>/IIl .. >0<ono1>ry .. i.... "'.~""
1m.. ~"'., ~ .. n~
.11t 11<_,• . 0 .. MI"d Child 1" ... 0"01 26: XI927.193-1 .
Kudo K. T ...... ; N. Ki<n $.<fal.: 1" .... 11'...1' " _
.. _; .. "" wi'" h yd~I ... N..... OSU<1...... 21 .
"'''''1»'
1.".....
72~l ' . I9I' .
$ohmodok K K. A.... L M. K..,., I '" Tbe "'<tl:nl
17: 66) ·78. 1911'.
TUH.G F.E •• n... J.Ct>onI W K... ~I_ Tbe ... .,ott
<oppo,.,."ium, A """"",,""' ...,_" i"""",oi,J
pmw ... <'I"na] '-'"'s<aPh>. """
l'Of>Mo "'...,. ;" , h;kbn wi.h ....;o,y ........ i•.
N... ""u'l'"l")' 19: 691·9. 1996.
SccIi"" of P<:diwic No""""'l""Y 01 ,II< A"",rico.
A."",;.,,,,,, of No" " ' ' '1Surporu . (<<I.) Pod;,,·
Ii< .................J . I" «I . •{)N1I< and SU".,. . 1'1....
Y...... 19I2.
_ T: No_InW.ad ........ : ADdOlIl<,,,,I,,,
oflb""' • . K....,.... h,,"';al.1<I< .. y"",,. 199(1.
B _ SG.II<nd> G I:G",","", Inpll. 1"..,..,<1 ;"·
!<"aI.~l oli.I"" 1 0I'''Y; ..
0$<.
J ..... Ia" 89: 8 14.2(). 1"6.
Noll>au. G: lI..d <;",.,"1.",,.,. r.... ";nj, tel .;, 111«. ,... ... Podla'f"ko '1 ' 106-1 •. 1965.
Sh; ....... S,C........, K. Ok_n E W .,,~I.: 101...,.
•tt ..... 01 "ydtouphal.J$ i. lo',IIOY· U.. of ......
ll)lomMl<
1O . _<t:<tb<oopi1W
~u",
PftIi.1r 1(17' 31-7. 1915.
K.. u..... K I... T>tttyT I .K"""" E...1'1" $orial LI'>
'".."Io ..... _ r y ......"_.,.,oI_lOI_
It><~i< ~ydn>«plulu' . r«l",ri<> 7', 7'9I'. 1m.
DMdy W E: E.>.r;rpotionof,ho 0I0000''' pluu.of,1I<
1>1<..., .. n,';'1e in oomm •• ico<i., hyd«>«j>l>al ••.
Ano S ufl6i; 569·19.19 18.
Gnlfi'" K B. bmjoom A B; The I~.,.",or .hild·
hoo<I hyd.o<><opholu, by "hoo<>jd pi" • • <O>lul .. ion
..... "",foe"lu_",i"I n ... perfu",," B, J
No ...... u'1: a: 9S· )OO. 199(1.
K.nelk. 1>1 K .... btooo' R . ..... M: ... ......·1...1........
pI"",,,,,,ot.~'bonl •••
Co..
.. pen . NftIl"OfIIf ....1 )5: 525·1. I~ .
Joj'La"VOI'. M M.
H.Klllfmonn A M. <I
1'1" T~ ....... ic b."I ........,..'" at .. , . odoo«>plc
,h,nI ... rticulo«omy' C... '0fJ0fI. N.......... f .... r
. . """• • )'<, •
.,.,.1'1...,"". ........
"""p«t<4 _
1'''''''''''
,,,,,,...,,,..,,I0I0:
,_ .J
nicu_,:
w"" , )
OJ :
1«IO ~ .1997.
J.... MfC . Cum. BG. K_ B C1' V,.,ricu·
"'un" 10< hydroc<pIo.I." " ....t.I.Io""·
,1 ..... N."''''''".. y lJ: 7S}.'. 1988 .
lame. K E. T,bbo P ... · rn ..... <l .. ico'.pplic-..
of ..... _ _ • lumbopo,joo ...1 . ..... IS . _
..
OUIlItfy I : )9,41. I~ I.
tout .. J w. Choo><IIc, I p. In.:ous«I ri.k or d, ... ,
.. "';';'Iopo"~ "''''' ..... ,''''''.,. ..-;......
.. ilh , II! .. I..,.".. 4;~.I . li" " <h. po_,J OIlho·
,," J ", ... """,,17: 412-6. 19?7 .
D", N G. Wad< M I,Tho In<ioIo:nceof ..,il.PlY 'fI<r
"ntti<ullf oII.",n; proood,rn. J N _ .. M:
19·21. 19$(>.
11«1'"' 101 S. B.umoi ... , B,C.y" J R.
ri.b QI ......, .... f<om .h,""o, in .h,idtt...;'h
lop""""
NEUROSURGERY
".
".
~
.
".
)."D"
,,<II"
"
" . .,_'1.......
".
"
".
".
..
..
M.
0),,,,,,.
'in·
i"'"
".
.....l.. ,.,. .
"
"
"
""'~ ... pOI" ...... 10.011''''''''''·1"''''''''''-1
»
,.
cf'lic Ie>ioooo. So" N<urol II): 16-'lO. 1'18).
Y."",,"~.) : Ki,., .. "'. .
.lpI>oe-rtducoq de.ice> ;. ""'. pa,lo.", willi _.
.... •..... ourt hydto<q>ll.Iu •. Ikoch I..' '" .... ~ ••
''''' ..·"h 0.11•• al .... J N<u_ .. 84: 634" I.
>I ...... M.Hl.I ..... S.
,~
"
,.
•
8o<h ... ·L. K."",lift t. SoI.,,·Ro .. C . ., ~I ' Mo·
ctuni<aI dy.I"""ion.,r ..''' ... '''P''i'''..... "'"''' '
eo""" byClk.J\t .. ionol ,Il<,l licooe f'IIbI>« ..,....
'... J NftI""""U· 9"15-ll. I998 .
F...,h II "'.S~ •• _ M' R..r;onu<llac ;..... i..
""""OII'pilylO< ,II< ...1..,.,. or "'URI P" '''''Y •
MOftOC/" NOUdI S<I" )9.42. 1m .
_ . R K. F.... E l ' Kyoiro<",holu.: o..nI .. ,.·
'f< by ..,,,,,,,,,,1,, ""' .. , .... ""OW ..... "';_0""ion>. S" f1I "'<1U"O! ),: 200-12. 1991.
Mc ~ R L.OI,.i ... : 51,'· .... ""10 .yndr<!me;
R.. ,. .. cA IS ~..... I'<oI ~ , N... , oori il: 11$024.
~.
0nJ ... , M. J.nn, P. flo"", B: E,,,,,icn«. wi,h ,he
",tI
,,"'"The
pnmaryoo,,,.1 ...,..ou • .,. ...m ",,,,,,,,. J N... ",.
• ... 1.: In·7.1991 .
Ji ........ D f. J.: w'n~ R. GoOOne!o I T: Silicon< al·
I"iY in ""nu~.lop<fi,on.. lohu." . Childs "'......
SyoI 10: 59-6.1 . 1994 .
~",",,&Ift f.GloMJ O. K.pIOn B
1.,ui ..1
hom ... oJ .. , ..n,""ulop<mo".al ohWII poo:IO<du.a
i"pod .. "", .,....n .. . S."Cynt<... Oboto< 159:
,"II).2.19S4.
Bf)"'"' M S.iJt<mer A M.T.jm l I. "aI_ AIIdom·
ow «>f>l!llic-0Ii"'" or .. nu\culop<ri_ ........
Am5u'l ).4: * '. 19IIS.
Ram Z. t,ftd]OI C.C .. ,man I.
V.nU1<ulop<ti""".1 .lMJ .. m.I!I.",,"" duo", m;I""" 01"" ,l>d .." ..1<..11<1.,. inlO III< o«<>Iu,". J ..... lalr 5u'l
n: '()4~·6. 1987.
Ru'" 0 S. Wallhl W, Abdomj",,1 <omp l ~ .. """ or
CSF.po.-;",.1t>I . h.mo. M _ "' ..... IS<! 8: n~.
'912.
M.A.t. .... J L. DeliO<l<lL.<f~I "
Go.\rio p<rf..... "'" 410< .... RI<ic"'o-.... ~
"'... . ..«Ilalt " ............ 11: 1,1-4, ,~.
~ K. B.j"'$:T~"""",I""'i< ..,q,Ifi,,"
of. _~ Iopon_ <........ f. " ' _ f....1
17. n.-6. I'll' .
$01<"". T H. 101 ....... 11 J A. B.... ~cll C E: ,""",,;,,,1
,00""lu. oo:ond.ory '0. " .. "".lop<mon..1
C''''''porI. J 1".. ......,.. 3': 9S-6.1971 .
Could .... 11 W T.LeM.y 0 R.MoComb J G: E.>.pori.
en« ",iOh Ul< .1 .. _
""I'h pe';_ ,,".m
eo, ........ J N... rnoufl 35: 41'·7, '996.
P"", • • I ) M S. Pnb'" V B S. o. .. Iopn<o' 01 pu~
"""'"'Y hypo ... _
u .... pi ...""'., or.
.Cf!fri<."""rioI """". MOJ"O 00. P'O<~'
82.19'13 .
(...... 1"1>&1 .. 0. K.1Uttti A V.D<U.J 101 .<1.01.: ........
bopc< .....1It.• ""nl: A""'''''''''''' .... >IUdJ ,n Ihe
ptdi"'i< _ Ill;oo . ,............... ,)2: 376·3).
1993 .
W."'h K. $011)110 I. S....neI R. " ~I " OIi .. l , ·maI·
I"""".",' , ,., " ....
d,_r? J "' ............ " .
604·9. 1912
<....... "... PD. Ann.".,.,DC.Onl<. I M.«aI"
T..,;II" ht«U" ... , TII< ..le n lll« 'tun ,II< ..«!'"
'"'" at,o. lumtoop<" ...... ' "'ullli........ podiolroe
_ " ' _. J _ _ " n : 56i-7l. 199• •
Poy_ T D. Pna, .'E. S. ...... T S. .. oI.: A<qu;""
o.iosi ....11_i.." lnolac_.4;"_'.
N... f ........ .,.3<I: .29·3<1 . 1994.
K... Io, L A. lluS" P. COoK ....... 1 P: s,.....,><
""' ......... 01 medullObl......,. _ ' " by ",""I.
"'1. So .. 1'1' ... 0"01), 141·5l. 19"15 .
C..... K 1I.1>I_K S; 1'r"."" ' '''IlI<~ul;.: .......
1W "0"",,,1... d"i~: A .,..,.pe<Ii •• "udy. "'....
""•..,.., n: <136-1. 1981.
MaonKS . y,-,=CP.o...GB: ... ..,u ............. p
''''.
II. Hydnxephalus
'"
.. ,i •• i.,..,. Oo.;c., ("'SO) in "'un,
""''''P~ <>I poll;'
.~2. ,98"
.. ri< ~)'<Ifpc<"""I<. ,. J 1'1.......... 6'·
"
"
"
"
.,
~.
"
••
M.
Foh. E l. 8 ....... I P: Symplomo'i< low 'n' .... n·
"", .. ,,, JI"'>Wt< '" ", ... «<1 ~ydro«pa.Iu •. J N... •
"""'IIoI.OO'·I, I!ltI.
rtoc. MorN w. SIi, .... ,id••yndr:ome C ... •
"mp 1'1 ............ 2. ()), ..... ,999.
£11,.1 M,CamteI P W.o. .. ",i.., ... M. 1",,_ ,,..
... ,.n1ric .. 1u _Uf<
~<"......,ply ,.
<~ik!f'<Il "' ''' ""'no>' •.....m.1I ",'u"",·IIy\W<.ph·
oIu,. 1'1 •• ""' . ......, S: SoI<}·S2. "..,.
Kit',n, R. Mon .... W. P<l<hm .... R:"" ,'i,·..,n,,',
<10 'ynojl(l"'" .1.... oh"n~n, In hj<!<O«p/llh' <hll.
d"n. N,.",p<1I'"'''' .): 190·•• •m .
Hydt-R.,... .. M O.R">I' H l.N.''ICII F~ R... ·
p.n,'" "I I>m''''''''y <e1l'I"«I",nl1i<l<.o: Tho .1"
...,,;d, .,"" ......... J N '.'_ ",~ , ')6·9. 1932
S.!mOtI I H: The <0(" 1"«1 "'."0<1,,, f>to ..,.O'I<f>t
."d p..... " ... SW"c 1'1,.,0( 9' 349-51 . ' 911.
"""'"'" H O.$<h.1t R R. Fo.J l, tll1i:. ..... i·.iphon
.noj ",..
ocd •• OO/l'''~ fo, .....""£ ,"h,·
d...... ploo lu,.noj
»O>Is.IIufll ... Ixi.tal .....
""..",... J Nt.,... ... l8, 119-38. l l7l
Ep><.,. F I.Floi«"', .. S. HOOhw.w C ", . .,al"
Sol:o,,,,,,,,,,1 <.. "i""om~ for <0<"",,", "'.nl .. t..
"""'ionS«"""..,..1O ,,"Oil "<",",,In. J r-I..,,..
'"""" "2:\1·3 1.,914 ,
Holn... R 0, Hoffm .. H J. Hto ojt1<~ E B; Su"' ... •
porol <Ie«>mprc>I'" f", ,... ~~· ..""",Ie . 1'tw;I"'....
oIIe, "'.ntin, '" 1tydr<>c<pI'II1;' ,h,_n. Chll<ls
""""'iI ......
"ob"'
pn"""",
"
". ,,50<,"""
.,.
M
"
A.
"
~.
".
B "'; n ~; I )1-40.lm
~.
lin<ler M. O..hll. SIoI., F H: S.t"''''~''1 <1«0,..
for "'URl .... p<ndeill ,..nui<Ie< MKh ..
....... of",,",,", S..... N... "" 19. ~l!).3. 1983
Ile<loly ". Fewe, H O. w." M... ", · S1i' _"",Ie
, , _ wilh~ , .. _if.: Thln;!,·. IUI'.c.·
<l<fi .. l.. ' ...... ""'. Ntu_~ 13:
7»-<},11lU.
1'1><. ". Eenunde. E.CotgoimoC. " oJ.: Hyd ....
<q>/I>I .. "'O ..... fIX ...'Uo; S.'liul ... _ ......... 1
..... """' of _ _ ,n, •• Ixi .... IIIe_om • . S.. ",
N........ 4S' 76-Sl. 1'196,
HOpp<.H,""hE.S ..... R_C.Il .... ,O ... <>I,
P<h<:,,,,bnl«>l I«,,,,,, .. I.. , ""'''',nl. Child, N...
S)'lIl' 91.lIn. ' !>l!7
M<OoI~ DC. "'" J l' NoS"'" i.. ,."...n;alpu ..
,.'" hydto«ph"u, '" ",.1 .. ",il~ .h ... i> aO>d /1> ....
I>,,,,,,,h,p '0 oho: """'U,,,,.,., 01 • ....,...111<"'010....
J /'1 ..., _... 40: 3n.~. 197' .
Soh" L, C"""",,,on 1'1><. A.t! ai, ~:)'<koup".lu.
"'" """"",,,,nil; Su'&>e>I ........ · .... liocolua.rn...
<>f pos..n.unti"1 "",, ...1""nl.'u"",, Su ... Nt. n>!
• ,: 81. 1996
Oit'tI<:h U..... m.."" C.Spri'); C ...." S.Ixi.,,!
,,""'''0tI'UI , . . .... ofhye,O<'phll u",nd """''''" • •
E>peri<o« wi,h • p"'".u'O<!JII .. blc .. I...
Child. No .. SI" J. 241 .... 1917
" ...."" S, Nal:ono Y. I""'",;hi T, .! ~' ,: Monqe""nl w"h.I"'>.... ~pru.......... ofIUDoIu·
",I ...... Iom .. a uoed tr)I ...n<rinIlope!i,.,.,..1
.hunl: C... "pori . S ..... r-I,..-ol lS. )31·J. 199 1
nU.,.""",h R O' S.. bdu,,1
.f.. , ... """,
rn<tIl af <hto<tic h~drQC<pIu.'u. tr)I ...,tlClJloc....
• h.n". J N<un>! NaI""" ... Ps,e/lill ' y 33, 9s.\t.
1911'l.
Po.idoff l M. F.irinl E II. Sub¢Uf" II<f'I'UIIOnIf.O<'
<um.,. I. "",","Ill' ,... «<1 hJ<lr<>«JNIo< '~ild ...
.. ,th . ............. !IOCI of tuotw;llio, pe",~ .... """,.
,",I""". J ~"''''1 '00 SSHi3. 1%J.
"",I""" 8. "'.... M H. y""", H F.<lo/. Ell",,,
<II ~ «n:b<o,pu.oI nuid
oho:
",.11 'M b... _. J "",""'"'. 31: Zn·91. 1973,
FlUllI ..... K, Sdvnitz I':
.. "'u," , .... «I hydto«pholu .. ...cta /'1, ....<101, .~:
19·101,1911,
H..",,, S.A<IInu R 0 . Tho ' l"'<i.1 <lin""" II"()i>jem
Df 'ytnplOml'l< h)'l''''''ptW''' w"h ' .........1CSF
pres."""
" los""",,,
n.
n.
".
".
N.
",a;
n
..
W.
M.
"
".
'"
"'f'I'UI'' '"'
'hun'"" ...
0-""'"'''' ""'''''''''..
11. Hydrocephalus
pre ...... J 1'1... ,0( Sd 2' )07·27. '9M .
...... "" R 0. Fi .... ,C,H.l i.. S, <fiJi.. S~""""",, ,i<
_ .. to ~)'<!""""""Io>t wj,h ·, .".".r ....,"""pi.oI
nuid p«UIm. 1'1 EnI'J Mod 211 .n·2~. 'IlM.
Th .. lJ.Gn.no! .... M, "",ubet M R. O' ...... i"
Otor"""'"u"" of ... f"",1 _I""n.no! f",,,,,,
w"~ P""S"""""' 1'1,.,0("", K: ,011),
90, '98! .
W_J H. B..,,,., 0 . 1"""," '" E. ,,<>1_ Norm.]
""' ..... ~j<!fIX.p/II'"o: 0'0;0"''' on<! PI' .......
it<'", lot >00", "'l"Y. No "'oio1J ~': 517·16.
.91 • .
S~"""" I•. Oonch 1'1 WC .S".,...IIS RJ: _ " ,
""-eo.n r.o--u.l«I ........pte<>Un: 1I:r<!~"""
",,," 1: 12\l1·2.19n.
Hu. J.lbom«r 1\ T W M. l'rt<Ii"i... 01,.. of "",.
J>O<'1'r)' .... mal """bot dtoi • .,. .. -.n.1 pre""'"
nydfo<.ph .... , N....... u""'"~ 21: 381·~1. 198!.
V... ikMI",i. J, The .yn4rom< 0( _ I........'"
hl'dtO<.pho'''. J Nt.""",... ~I ' 50 1·9. 198' .
Jook C R. Moloii B.Lo.., E R, .. <>I.: Mil rtn<lin,' 'n
""""oJ
hydroc.p...... Si,";r",."" • • tw;I
oompll;lOn "'i,h ",I." 1_. of 00"" ..... J Co",·
""1 ..... i. I T _ I I: 92HI.I9S7
S<hwuv. M. C.....1 H.C"d, C L. <I(J1, C_,·
«Ilomo,,,,,,,,,,, ... I~.,. of .",n
;n
30 ..... I'hy ...". '1"" 2. '0 II ,an, "'nn N, unll
' 1: 146·S7. '9l3.
Holool.¥ ... 1.0-.' ... E.<It '.<On M 1.«<>1.: Fo<.1
~il",,,,,.noj p.,..""it.l<oU_ of <""""' ro .......
.M "k:; ,n poo"n" "i,h nonn&l.p"'''''''' ~l'a .....
«pIl" •• J N"""""I8<1: ' . l·7.1998.
SIoe .. i. H .... O..."'"'"J O.c.o...m.nC B: v..,.
,ric.l ... " •• '~<1 ","n1inl f., "'"",ooho<_1
""' ..... hydoo«phol ... . J Ntu .... N... "", .... I'$yo
<hi"",)I, 1)).7. 1m.
v ....... I . ",,,,.uljn P. 1)0.1<, 0 " C. <I <>I_ Nor·
mo/'PO<''"~ ..,.droc<ph>1Ioo: I. <",emoVOphy , .. II
... fuI In ..10<""1 poele ... l;t. ","",1 "'« h N....
,0(.9; J66.70. 1m
0,0_,,_ G. F1 ,.. ~ , L .. <>I, It,.;;·
~
"
~
pI<I'.'"
"""Phom<"""
Be,,,,,,,,,,
_1~.I."....,....ph~""<o'T'I","d ~
".
%.
u. JO .... lltoy ..r.n...". N...... r.d;o(ot!' ZI: 1S<·
60, 1986,
......""' .... Moone" M. fI<r", ...c..,"', Pr«/ic:si ..
..l ... of.,. ...
d.~in ......... I"" ••
• ... hyd""""""I ... Mia /'I.~ ,O( SaPt ~ I I. l27·
32.1990.
T.",,,,; N. "u'"_; T. W",obIya"" T, <111/, c..
",,,,.llI<mod)'ftOmin in """"',.""" ..... b)'lrOE.. luII"''''' 13lX. itlha1'O"" ..... hoj
,..;I d,...mi< cr uud~ . J N",........,. 6, : SIO,' •
".Ii..
«plio,."
" ""
•
1I1oc~ PM.Ojo"""o R G,T""" .. "',CSFoIt!J""
fo< <i<mcn" •• ;""""i!IC .... . nd pi, di>l .........
Clln N _ .. 3l: 6n·S!, 1935.
M<Qy.m. I C. SalO'·lOu .. L. $0::""'" P B: Trea'·
",,",of _I.~ u<. n)'ll>oc<pho'", with ......
P'C' .... ' _.... plnll ~u id oh ..... ,
NftIt'IXU .... r)' IS, ~·8. 1"4 ,
81"" P M: !diopl,1H( """",,1.1"'''''''
..." 1«...1" ulll\un<in. i. (>l pool< .... J 1'1 ... <0... ... Sl, l71.7.191j(1 .
'00. Pm ...... R C. Moktl B. L. ... !; R' S"'li",J 'n:"'.
",to' of Id><>po"'"' hyd/o>«ph.l", in d<l<,'y po.
,it"" . N.... oIoe1 3S: 307·1\. 1911'.
101 . Lk! ... hO lyiC R,W"""J H.I""" ... E. R..,I,,"""
""",pll<oI"",,l" 1501t'''''''p>1le... wi," """",I
pr<>",n:
s. " N<:ural 3, 17\·'.
_m<4,.",
.,droc'ph-
"
""
hy./<o<""".r.,
CoIamlIJ •• , ai, ... "hei .... '.diou« camorttidily in
_ I ......... ..,.drn«phoI",;
.... n' """""", J 1'1...... Neu.oou'1l I'$)·,hlo'r)
68:776-31.1000
10J . Humpllay PR 0 , _ " 1 (F. R.""U R W R. Vi·
...., r..!d <1<1", .. ; ...... _ ... h)<Iro<eph.I .... J
111.,. .... 111 ... """ ...
1' . ,: ,91·7 . 19t~.
'00
Pre-.,,«:. "'"
1'$,,,......
NEUROSURGERY
,~
CM>,;010 1
.,.
•
".1\10.0.""""",u..,tw..1 O<T\II""";.;"
h~h< <~,111 ""h ..
f'I .~)oO · U6-00 .1 911
"",""'led ,""n',J
Ko,i .... I'I . K .......... K T ......., ri , tim, N..." _
~<"""-'_1"""""'""_""~_
mAIl.... , ... s... ""..... 22. 2n·6,
_of""""
Rlad P M.C"-,",, 'H · r .... .." ' _.... ,..,..
• ;. 01.......... ,"'1 r", h~pM/IR J _
....
" . 067" . 19111
107.
,~ .
._.....,..,........
I! A, I"'"'
. J E. "<Co<"';"k A Q. ..
fIt,0/10. '" .... _ ' - , .... N.....•
011 ~
..," U -t.I9U.
$000 M.TMMoS. ~A •• ,011 Oc:<:i,oitaIlotIo
Illlaoa ... . _
..,. .. """"'1 ... """';,..1'1 .......
-c<1'J I' )Ol).S.
Jo)o • • J . _~G w ...... " J. .. al_ O«¥/Uil
'M/).
". _.yoM_..,...r....... a.....o, t _ .........
l. H__
J)'. Fmltril. J
A
.... lIollo • . l " '. yol . 1
$<_ f'ubl1""
",,~g.'! .
110. Jt.-I4ItBor_ J I!. r _ C E Cotrl<aI, """1
~ i _. foI lo ..... " . "","""""",,, __
Ho)'1 W F. WIUI! F B, eon ... llIoIir4"." .ith .....
,i,1 rKo"", follow l....... III>I./.'..i. ,,,,,,,<l1l1I1..
ormI . "rtb Orb,,,,, .. 60; 1061 ·9. ,'lSI
116. Wt"lI< ..., II n .•.., dc, W_ M.M..... H C
I'fopo<.. of c«Ii<.1 ............ ,.,. ..... m.c ............
J AMA 119: 116-9. 1961
SI.." M L: I...,.",... "",,", ......,..u.1.I'Icr.MI'..
.... •• AmJOpb,hOlIllOl IGoO. 4lJ·6. 1911.
1'1• S_oq P 1,8...... "C, Sci" .... J B. .. "". 1, """"",",h)'" " , _1.,10"", or c..·
diopuln\ollll)' b,,,,,,, ,_'l' ,.........,. n, ~
I" .
,~
,~
'"
... ,. 't._•.
'"
,,,,mil; """'"
1.19111.
119.
'"
L>_lotq R. W.w. f • . V.... Ior< _ _
................... _po .......,... T. " ..
AU<! 0pII0. 0l0I61 •• " .... 1960<.
Ill. Hoyt wp y""'oIttlt.-. of ""' ....... <atIO . .. ..,
""'.. _ ... _ ~ "'"'.... ' ..,in< ...... A"'~
0,b0_601 . ..·n .w.o.
A B. M>ro_ I' .W,' .... E. ....... <...1Ira1
II ). _
NEUROSURGERY
o.-s Io1 .MotpII ~ w.s_..~ Y P-S"'"'k·..·
_
m.
_,;,;.... ""'-"'<•.J N _ _.....' . S(4.
" • . 1961
blind ...... ;•• ~_ . N•• ......,.;!o' 1107 · ~ .
191'0 .
KUII<J N. 81",11"0<1\ foUow;", 1<lII<Iri,I Joonol.. _
IuIn Nt.""" : 1116-90. 1980.
.~.
"",ie ncurop>th~ . " <011 . . of oo"JIfO"H' i ~
l I _. Nr. ... JMfIII 2U' :l9H.I91),
Loobo, ): ~ _\" '" of.i . .... ,.,..",.1.. pooIooored
b/iool .... . n <!iii""," .. 1111 hydtoc.p!lalu. or fol .... ·
lot (I)'Ofttli< ....,.I"'~ ... cu.. ..... lo" 6, 699-70).
I96J .
WiIoI'I'l H. Kn ... " K I. II_ ,' .. ,S ,.. . .. 41!
""'..-r" poIi<"" ..... c... ~ n...
"""'""•11<"""
of ....... oncI ... i<>- of ,he Ii,,,,,·
,_.N
....,...f)I..,N· t:?'J.)I. I99 I.
121. M... O F.Zt"';'i. MT. Ottio L ~ 'CS F"", ,," ...
lion ", lo .... mj obo. .. rri<aI .....,... " •. ""... h os/....,.U, J4.! •. l"ltl ,
I t. H,drocorphll u,
12.1.
General information
12.1.1.
Specific antibiotics
..,M.So",,, antibioti.,.
8~
ind uded hef1!ln to hi.hHghll'artkullln of in-.ernt. to neu..,.u,..
OR AL PE NICILLIN S
am()xicillin ... clavulanic add
(Augm en1.ini!»
\ /
\
A good PO drug for &U""rfi.ialst3pb ;nrl'JC.tiOIl8. Good
IInReT'Olric and anti..,staphy loeoccal coverage. Absorptioo is una!r~tf>d by food. Av .. ilable fonna
are lurom"rized in Tllbl~ ]2· 1.
& Adult; 250 or 500 m8
PO q 8 hr. or 875 mg BiD INB
use the apptopriaLe tablet to
aWlid uetlUive cl.vul.nll~; the
lower total dose of clavula nat.c
with the 875 mg tablet may pn;>duoe ft.w". GI , ide eO'ec\.I).
PNa: 20·40 mslkgld II.moxicilli"
d ivldl!l! q 8 hr..
P ARENTERAL CEPHALOSPORINS
Higher leoontion _,enu hive pro~~ely reduced uti-ity ag:aiJYt .tnptococci
and pen;c;Uin• • producin, S aul't'US
First gener ation ce pb aJolponn ll
~
eefll:tolin (Anee"'. Kerzol®)
\
I
DRJQ IO!FO
\,
Good for auJ1ica1 ptophylU». c:-llltVeb in h.-.i.n !.loue hne bIom documented.
Poor CSF penet•• !.ion ( !hila nllt good lOr mminciCU), Adv.ntage over otheno ~h.lo6pot­
h igher !leNm level. {80 !'&o·mll ..... ac:hievable,.00:1 h.lfli!"te {I .a h..) i. Ionger {.!low8
II 8 hr dOlin,J.
Ib: Adult: I em IV II a hnI. Peda: 0-7 days - 40 mNkrld dlvldedq 12 hno; infanl 80 mll\lild d,,,,ded II
child - 80 mef\Lgfd divido:<! q 6 hn .
[fit,:
sa..:
Third genention eephall>lIpori n .
Potency ofthne dNP are . equivalent 10 .mino,lyro.id. for: E. coli, kleb.lieUlI •
.. nd I'rou .... Onlycel\a:lidimei.itdequale for~. Cood fo r .... riou. · infecIlOu.
(..... OO",;t;.. endocarditis .ad OIteomyeliU8). 8U)11.1:f"RCT11: dian-hell (peeOOomelllb"nOLl'
coliti.). Weediordiathuu••nd may allow lu~rlnrection. {e"te~r, resJsUnt
WI
12. Infectiou
l'IEfJROSfJRQE;RY
pseudomonas. enterococcus. fungus).
,--/
cel\azidime(FortaZ®)
\
/
DRUG INf O
\
l
Good for nosocomial infectionll. One of the b!:il drugs for Pseudt:>mcfWs (J('ruginQSO
infectiolUl (large doses tole.rat.xl well), but doesn't rover staph well. Good eNS penetra·
tion .
tis) .
SIl)E EJ'T&(:TS: ra~
neutropenia with protracted
IIodmini~tration
(e.g for osteOlnyeli.
R.r Adult : 1.2 gm rvllM q 6·8 b.rs (non ·life threatening infections: I gm q 8 hrsl.
Peds: 0-4 wks - 60 mglkgfd divided q 12 h rs; child - 150 mgfkgfd divided q 8 hrs (maximum 6 gmld).
,--/
ceftriaxone (Rocephin®)
\
/
DRUG INFO
\
l
Good penetration into CSF. Useful for CNS infections involving CNR IIond for late
stage Lyme di!!ease. Long half·life allows q 12-24 hrdosing, U nlike mostcephalosp<.>rins,
excretion i9 largely de~endent on liver, therefore 8110me dosage in renllol flloilun!. May he
synergistic with aminoglycoside&. SIDE ~ may CIiouse bilillory sludging.
R.r Adult: 1·2 gm qd (may be given q 12 hrs for meningitis). Totol daily doee < 4 gm.
P eds (for meningitit): 15 mgfkgld initiol dose, then 100 mgfkgld divided q 12 hr •.
MACR OLIOES, VANCOMYCIN, CHLORAMPHENICOL
,--/
vancomyci n (Vancocin®)
\
/
DRUG INFO
\
1
Arent of choice for S. aU,""" r infections that are either methicillin resistant (if not
MRSA, better resulto are obtained with PRSP), or thot occu r in patients allergic to pen·
icillin or de rivative/:l. Multiply resistantS. llunU$ infec1iollll may require co--trellotment
with rifampin . Poor for Cram negatives. Loog half. life.
R.r Adult : start I gm rv q 8 h Tl'! for serious infection. check levels before and after
3rd dose, and aim for peaksof20-40 Jlglml (to~ic > 50; ototoxici ty and nephrotoxicity that
are usually reversible occur with peaks> 200 I-'g/ml), and troughs of 5-10 (toxic: > 10).
PO dose for !l§eudgmembraOOUB colitis: 125 mg PO QID . 7-10 days ($Orne referenc·
es re<:ommend more, but this is not necessary).
Ped s: ageO--7 days 30 mglkgld divided q 12 hra. Age> 7 days - 45 mgfkgld divided
q 8 h r5.
- 0
ch loramphenicol
(C hloromycetin®)
\ /
\
Good for: Cram ( +) and Gram (_) cocci. Excellent CSF penetration (even without in·
named meningesl. 1t i~ hard to find the oral forro in the U.S.
R.r Adult: PO: 250·750 mgq 6 h" (m ay be very difficult t.;> find in retail pharrnacie.
in the U.s_). rv: 50 mgikgld divided q 6 hI1l. Ped ,,: 0_7 days old - 25 mgfkgld PO or rv q
d . Infant - 50 mgfkgld PO or rv divided q 12 hrs. Child (for meningitis) - 100 mglkgfd
IV dividMi <1 6 hr ~.
AMINOGL YCOSIOES
When given rv, ooly amikacin has adequate CSF penetratioo (and ooly with innamed meninges). Not adequate monotherapy fOT any infectiQn. Good adjunct fOT staph
and CNR including sensiti ve pseudomonads. Poorforstrep. All are oro-and nephro-toxic,
however toxicitillll occur almOllt exclusively with longer use (> 8 days) . More rapid kill
than H-Iactams and may thus may be used initially for sepsis and then changed to a cephalosp<.>rin art..r ~ 2·3 days. Increased activity in alkaline pH. Reduced activity in acidic
pH,lIond in presence ofpusandiOT anaerobes (therefore may be pOOr for wou.od infections,
nuoroquinolones may be better here ).
J:lol!ages baaed on llIW body weight. Obtain serum l"vell! afte r 3rd dose and adjust
appropriately. Dosage, of all MUST be reduced. in renal failure.
NEUROSURGERY
12. Infections
~
gen t amicin (G arnmycin®1
\!
ORUG lM'O
\,
Ibt Ad u lt l non llal ...""1 N!lction) I V; 2 ms'kg fV lopding dOH tllen 1-1.6 mgr'kJ q 8
> ~ .,ghnl, t rough < 2). & In tril lh ecaJ - 4
It... mllin l.eoance, follow I.v,,-Is \deai red peRk
rna q 12.24 II",.
wbramyci n (Nebcin®)
\ I
\
'I'he be$l aminog lyrotide for pleullomonu (but not n good u oe l\ezid imel.
Ib: A dl.l1t (normal Tilns ' rUJ>dionl: 2 mg/k,& I V loadi ng dOile t hen 1.6-2 mlVkg I V q 8
hra maintMlnoe. For PI:' > 60, &arne do.e q 12 h rl, Follow lowet, and &dj u.t (or peak 7.S10 " glml , t n;llli h < 2. Rs 10Iro l h «:lI.l: I) mill initial d')$e, t hen 2· 4 m, q 24 h .... 1lJ< PP!dr.
6-1.5 mgIkWd divkled It 6·8 hrl.
12.1 .2.
Antibiotics for specific organisms
PSEUDOMONAS AERUGINOSA
Cef\nidlrue (Fortad>l;s the dm" OrChOH'. (1ftpa6f.209). GoodCNSpeMl.f1Ilion,
large doses tol ora u-d we ll. Amon,amioogl)'«>lldu, tobramicin illhe best an tip-
u udomonal. Aa\inoglywoidH gi •• 1J\OU .. pid ki ll and tb.refcml wll..., tM'" i, •• trona
sll~pition of poe ud omonali atMt wi lt! orit nid ime ph.. tobramidn ;n ltioUyand then atop
th e tob ro..ni om alter a reo. d oys(redutel risk Iltaminog!y<'Olidl! lllltiaty). An tip.
seudllmllllal ~ lIicillinl I re not ... effective lthe following 1Irt! B.lart.mlM lu..:eptibl.i):
ca rbe nicillin. u carcillin. ml!~locill; n , Inlocilli n. Addinl dly ulanate to ticardllin
(Timelltill ~l ,..,du o~ $WlCl'ptibility to B.lad.amalH!. Adding cipranoll8cm frV or PO) to
lU>)' IIf t h~ a1)ov" IV medieatlon~ hat. JYne rgi.Uc effec l lbul illnadeq ... te by iUlelffor
lOft· tiHue in fection,. auch 118 woond infKl.:OJ1& ).
STAPHYlOCOCCUS ... URfliS
VanOO(llyd n unti l it is dete rmmed that it i. not MRSA, then use PRSP (10.1. n,rcill io)
'I- gen!.a mici n (Ilm in.o,lyc:e.ld8 give !DOre rapid inltiallr..iU a nd are .yner(i!! lic .ga,nst
lta ph ). 5tDp the gentamicin . n.. r. few doYJ (l'ftIUCQ risk ofaminog\y<:OIIide t",u city).
For .Q[iJ trea tment of non M RSA S. DU",..., .... ound infeotionl, optioM include 2 """"Iu of:
1. AUllD"n unllll (<<e PQgt'l!P81
2. lit n illoupin (600 mB POq dh either
A, trimeth allulfa (I OS PO BIOI
B. or cll n d.m~i n
FUNGAL SUP€RINFECTlCJt>J
For tun,a1 ~up"'ri nfectio" oflhcl Gt lnct in paL;enu on "ntibioti.,. or a<UOids:
nystati n ( Mymfl tatin~)
(oral suspension )
\'--"-1__ """'_-_ _\-'--,
Ilx W a a l. ; 1 «(100.000 "1I1Le) on ellch . i6e ormoutn QJ O.
Ilx Adul l.a: itl len Aml ....llowing memanilm;, intact.. 5 ml QID ,wWland Iw, l,
low. I( comntoH Or unabl4! t.G 'wallow, 3 cc I"'r NG QI D and '2 (C onLI ..... b QID
SUPI"UEtI: in con~nlraliooof 100.000 unitalml.
~
May
fl uoonawle tDiflucan®)
"'""11.$01;
\
/
0I'l.IQ ...... 0
\.
_ nuu eorw:entral>on of phen.ytoin, l id/l¥udi""', and oralll ntLcoa.(\l·
1..,1.1, amons nth"" •. Can QU6O! live, dy.fww:tlon. which roay not be ...... enibll!.
IU Ad u lu ' (or orOphllrynreal c:andid,"ia. 200 m.r PO the fi ..ldsy li nd then 100 mil
POqd for 2 weeks. lJUpp' .IllO: tabl4!Le of~. 100 or 200 m.. Powd'!r for Itn Ll"Ip"n&ion
which Un be mind to. voIoI ..... ot3S mt 0{ ei lh.r 10 0/' ~O m"ml. AI.o.Ylli lllblfr in IV
fonn, which i. ~ry npenalve. and 1UI" .Uy not n«NUIry d". III eXteUent GI nbsorpt;.o n.
'"
1'2 InrKuonl
NSUROSURGERY
12.2.
Prophylactic antibiotics
GENERAL PRI NCIPLES'
1.
anti biotia mUlL be;o tissuea at tilDe of contamination (!hue, ",void "on-caU" a ntibiGtiu; give 60 minute. prior to il'l(:u ion)
rept.~ adm inistration y;U] in prolonged procedure.
typical infect inG organism. are usuaUy predictable. Co~erage for the.. O'llaniam,
i, IId~UBte (broadeflinG .pe<Lrum it of I)() vlIlue)
4. in low ri. k oper.tiora (e.g. carotid endarterectomy. whue infections rtlre and lei·
dom lire· threatfnin!i') may co.t mon 1.0 prevent than I(> tru t
5. prolon"ation ofantibiotic:l beyond lint poIIL-<>p day provides DO.dditional protection (may not be true;n patienta with . urgical drain,)
6. theoretical aid . .. ffeeu (alteration of patie nt', Oor •• dlPelopment of retiatant
strainl in patient or hospit.al) have not been re.li~ed wi tho",! prolonpd adminis2.
3.
tration or pre-o p Or poat.-op antibiotia
7.
factor. that incr eue rilk of ope rative wou.nd infection include;:
A. synemic f9ctors: malnutrition. reoperation , infeaion at aeeondary .ile (e.
pecially UTI when GU tract mll(lipulated), prolo"ied . dminltln t ion of an·
tib iotiC!!
B. local facton: epinepluine, dehydration, hypcWa
SPECIFIC AGENTS FOR PROPHYLAXIS
cephalos porin&:
A. ai"nts of cl!oice where skin flora (a:>8g\Ilsse (- lor ( + ) staph) are lihli""t
pathogens
B. may sa fel,. be give n even with history of mild, "....,·immediale manifuta·
tion . of PCN allergy (e.g. · rashes"). Contraindieated ifhistory of immedia te
Or acceler.ted reaction (shock, bronchospasm, urticaria)
C. eefnolin (Ance~, Kefzol®l:
d fe<tive, widely studied. therapeutic levels in brain t ...... e after systemic administratioo', longhalr'life
Dropbylactj~ d!IiI:: 1·2 gm (peds; 25 mg/l<g up to 1 gm) IV 60 min before
l u..,ery, then q 6 hr lit 24 hr& pott.op
O. lOme S. O"~Ii' IlrIIoint ""' e1'fici.o nt in B-lact8mue degrads tion of cepha.
losporina. and cefnolin is partic\llarly ...sceplible. Lowe.. infection rates
may ..... ul: .. ith cefamandoht (2 gm initiall y, and then 1 gm q 2-3 hnI intra·
operatively»
E. a umi,ynthetic peo.icillin may be more a ppropriate if good CSF penetration
is neceual'}'
2. vancomycin: allernalive if cepbalOOlporin contraindicated (incidence ofl n&phyladkrudion, i. too hilJ:h fOT routine use). Dote(empiric): I:"; mg/q (up to 1 10')
IV pre-op. tben 10 m&lka; q 8 hra for 24 bra pOOIt..op
3. penici llin s: d iudvant.llga: probably len A fe • .non.tr half-life. may prolong
bleeding ti me., N8 fcillin il probably the btlt Ipnt in thia group
1.
P ROPHYLACTlC ANTlBIOTlCS FOR SPEC.FIC NEUROSURGICAL PROCEOURES
I.
2.
carotid eodarte~lom,.: routine 11M DOt indiClOted (infection risk too low):
when riak of iofeclioo ;. high. 11M oefouoli n (•• for p ........ prophylaxis, lIHabow)
e r aoiQIoIOY: ri5k of infection tn'y be imreaNd in prolonpd or mJ.crosurgical
procedures.nd in renpera tion.. No lignifieant differellne in the .peciflc regimen
\lied was delftted in meta·anaIYI;'·, Option. include:
cefatolin (He "boo"
dindamicin (300 mglV) preoOp '" q" hn
vancomyru'l (ac obow)
scme!Kld pnt.lll1lkin (80 tng 1M) pr_p to any of the...
3. CSF . huDting procedu«'a: eft\CIOt')' haa been documented wilen the Infection
NEUROSURGERY
12. Inf«tiona
rite I. u""'''II11y hi,1I fur lO me . twllIll (e.g. _
u .ly infeetiotUl, i.1!. - fint wCIi!k pOlt-OP
A. for llentrlll LlI<!
L.
ftlec~
:I.
PLUS
I ~)
AnLibouUI1 p<III!!Iibly
redUCl!
one of the follow'!!I:
c,f"w\in (<<t llbot.,.. )
II 191 generation ctphalGllporin (e.l . «'phapiNi (Cef.dylll!)):u.
n'&/'kg {up", 1 t mll IVP intra-op ...d II hr. pD5r..<1p
I'\tJeH l1li 60 mW!t. (up to 2,1 IV 60 m in before "'.g'II!T)' and II ~
hts posl-<lp I :; dOiet Lota!
in ttBtb~J ~nUIr.nicin
4 ml( injected intolh unt
l ~ tlm.Or pJIC.
mtnl (nQ longer ",yell.hl. in U.s., bu t pl'flflro'alive./'ree pediatric gentamkin may he diI",1.ed appropnal.8ly and used )
8 , Kaiaer'. luweata no IIntibiot;':' ifinrectiCln rate J_ t< t o'iloI. Ifhi&h f>
20'10)
'"I IV)
pn:-op
very high,
... '" lrin.ethopri m 1160 rna: IV) pI .... a \.lJr.metno""nolf (800
and II 12 hI'S ~ 3 dole. poiIt-<lP INB: thJ.. Iluer infection ral-e
I
and r Hu lt.l are thul queltionable I)
ICP monitor" lIN pog, 5$0
procedurt'a involving indlionl Ih"'''1I1I 0 .... ] or ph..,.."",. ] IlIUL-oaa: Cln!.llm;·
e in ( 1.7 mlVkg TV) and cllndamicin {300 mil" IVI pre-op '" Q 8 hl'5 ponop II 2~ hn.
Cer,:ol;n & 3T(! lI"eneral;Qn eephlosporin a lll(l eff",u"e when p"en oval' 2-4 hI' jIO!.
nod pre·op
Ii. spinal surgery: r educt,;on oflnfect lon wu ~1t«J. but
not Ilawtic:aUy
IIgnifi"""t lIow inclden::e. would Tl!quire Ja~ study)
4.
6.
w"
A lringle blind pr(lllpectivf .tulb' s howed thf inridenee ofpo,."nWroIurgita( Ql>t!ra·
!.ive wound ;nf"dionS were re<ll)(:ed with eerazo]in n gm IV) plua r.ntamicin (80 "" TV)
gi ve n onehr boofo", incililo n and" 6 hrl intn-np (none pDII t-op) With ll",i fleJInt f'Nu lu
in p&r.ienta without foreign impllmta (upecially enniotomiu: no .ic'nifie.tllt difference
fill' spinol operationl, but u umben wfT'l! I mall). AU infectillM w..reSl<lph.
or ~pi.
dermidi. (maku USf ofgenlaOlirin Quetitionllble).
'JI""'"
12.3.
Meningitis
Community ,,~uire<l mening;ti~ (CAM) is gene nJly me", fu!mU:Ant lban mening;.
til following lIf!ul"Q.l urgie. , p~urel (lbe fOnDer t.end to OCCur with mo,.. virulent Ol'118ni5mlor Impoi red bo&tdefe.'ieI!l, Both Nprelelltmedieal emergent1e6,and 5hould be
treated im medililely. f oc:eol n"..... loeic 8igru; are 11I0! in IlCUle puruletlt meningiti,. ~
l.umbw punc/u", On page 6 15 (or 1 di8l"\llllion about when to perform an 12.
12.3.1.
Post-neurosurgical procedure meningitis
s.
1. 111"'11 orgllnilml : o~",~., Ent.eroba<:t.eriltl;f!lK", PseudG"""",. " p.,~IUJIOCDC'r;
2. empiric "tljbioliet: v'(,OI)"ljo"cin (to cover MR5A)~ cert.ddime lperifieally:
v..u::omyell1 (.dult) 1 em IV q 8 b ,.., (cheek leVY! beror", ...daner 3rd do.eand
3,
~.
.dJu.t acwrdingly, ~ VIIA<'O,")'I:in, page 2(9)
• ceftnidime (F orudP) \·2 guo IV q 8 hn
fCir pil!udoUlon... add genlAlIliQn (IV '" IT)
Irorll'aniacn twntout to M nOo·MRS.\ S. O~~"". change v:anCOOlycm to IV PRSP
(e., . Il8rtillin)
12.3.2.
Post craniospinal trauma meningitis
(post-traumatic meningitis)
Epidellliolo(D'
Ottur5 in 1.20«'0f P/ltienllwith moderlte to_Ill bNd inju.ri.... MoatUl _occ:ur
within 2 weeki oftnuml, 110;0u,h delayed _
hl"l bM-n ~ribtd'. 75'" or til...
hllv. delllonilrahle baaa l 8ku ll fnoetu", t_ ~ 665). lOud ~ hid obviol1l CSF rhinor·
rhu .
m
12. Infections
NEUROSURGERY
Pathoge ns
AI. eJ<pected from above. thel"l! illl bigb rateorinfectiuo with Qrgllnisl1l/i indigenous
to the nau.l eavil,Y. The most 00100100 nrganisma in a seria from G ~ we~ Gram-JlO"'Illve cocci (Slc.ph. Mm(>iilieUil. S. wameTi. S. ellhnii, S. ,pithrmldi•• and SIre.p. plleumo·
flia) IIlId Gram-negative bacllli (E. coli, KI,b,~J1o pMumoniu.,Acillf.lo/laCltrotlilroiIUJif.
Trentmeot
I. a lRO see CSF Futulo. 1'rrot",."" On pagill77
2. antibiotiea; appropriateantihiotica are M'1~t.P.d ~ on CSF JI'Inetmtlon "lid orgaoism HMitivi(iell (adapted to tbe pathogeJl8l'Ommon in the pIItient's locale; in
the above "" riel, all CnuD·negative .trains appeared ,"".isllInt to ampicillin ""d
Ihird'genel'1ltion cephlllll!porina, bU I were !en~ilj ... e t.o i roipenem and ci"rofl""a·
cin; Gram·po8it:ve ~tr.ln& werll"U ",,"sit,,'e \.0 vanCtlmydn). For emp;ri" IInlll»oll""il<'~~212
3.
~.
surgical treatment ... " ·coo.ef\lsUve treatIOent": eontrovers;.l. Some (eel that
any case ()rp08ttr"u ",ati~ CSF rhinorrhea ~hould be explored"', and th"t~9
G! ~Dtan~ou~ CUliDtion olli!n rl!pres<ml ob.u:uno.tion tly inm~ra(ed brain, $0eaJled ·sham healiog" with the pol4lntial fo, later CSF leak an!ilt>r mening;ti.'.
Othe", su p port. the notion that cessation (pDilsi bly with the Ill;s;stam:e oflun,bar
s pinal drainage) is a~teptable
eontinu e antibiotiC!! f"r I we .. k afWr CSF i, st.uilind. Ir rhln"nbea perlliau at
thiR ume, ~urgital [epa;, i5 f"8CGm1T\eJ1ded
12.3.3.
Recurrent meningitis
Patie11 \.11 ....·jlh re<:u r rent meningitiR fUUS! be evslupted for the prt':aellCe G(aboormal
eommufliclltion wilh the 1Il1t8sp",aVin\.ra<1renial compartment. Etio logil!lllndude de.,
mela;nus (eithe r !pinal or cranial, _ pa.s_ J 18), CSF r;~tula [a", ~ 174), or ne"ren,
Ulric cySt rue fX'8~ !lB).
12.3.4.
Antibiotics for specific organisms
in meningitis
RoUI.<! is IV unleu specified othe.rwi~ .
S. plllo!umOl1ilu: PeN G I1i!nd M.oice. chloramphenicol)
N. mMineilidi., PeN C (2 nd choiCO:l: chl(l1"smphenirnl)
If, j,,{1uerua :
A, no"· peniullina!e producing: ampictllin
B. penicil\in88e producing: chlGra mphenh:ol
Croup B Slrep' ampicillin
1- monGCJ'I08'e" ... : anlpicillin
S, DIU'fU'
A. ini tially before sensitivitie5 knawn, Or ifMRSA Or mu ltiply r ....;,;tant alraina
'" re!II l!tant coagulase aegative S. O"~I<' pr"-~alent o r ~us~ct«l: vnncomy,
tin .. PO rifompin" PO trimethoprim
B. once it is knGW(l that tho u3ph is nm. MRSA:
1. infanl«7dj:melhicillin
2. all oth elll: n"fcilHn
3, PC!'.' Bllng)': vancomyein Or tceJ"a!Qlin";8 both rv .. ['I')
8~robic Grem n"Maliv" rod. (CNRl
A. celtriaxone, or cefouujDle, GT monalact.llm tin order Gr p re feren ce, make .1,
teral ions b!tosed on S<'lUitivitle,)
B. if arninoglycOliide ""Iuiri!d, in traventricular theropy i. jndkal.ed atl.er t he
newhGrn ~riod
p, CU! ru lli/1(1$fl
A, cefta~id ime {Forta~) alone If ooi life threa lAlning
D.
B. more se rious infect ion. require 2 Rgenls (pminoglycOliide gives mOTe t8pid
ItiU, a nd may be w;1>(! initially for 3dllY~ and th<!T, fil.(lpped if aensilivilil'$ to
reillllidime are ateeptable):
ceftazidime + APAC .. n'gentanucin 4 mil' '112 hn ( ",~ e via intraventricu·
la r route if ven tricu.lili ll" il pre&ef1t)
NEUROSURGERY
12. Infections
OR
C. for overwhelmil\li infectiOR:
«tftnidime . tobramicin • tica'tiliiD
12.4.
Shun11nfec1ion
Ri. k orearl)' infection lIf\er .hunt . u.rgery; ~pOrted range i. 3-20'li0 pe r procedure
(typic..,ly - 7%).
Acceptable infection ,111.41 ": < ~7" (although mal\,)' published aerie. have I r'lA!
near 20"", poe.sibJy due to differel'lt patient popu lation).
Ri"k factors ror s h unt infec t ion
Meny facto .. have been bl~med; $Om, that teem to be better doc:ument.ed include:
I. youn g age of plltient" : in fD,elomening«eLe (MM ) p.tienta. wailiD, until the
child ia 2 weelul old may signifioantly lower the infection •• I.e
2. length of procedur8
3, Opell neuraJ tube deJect
Mo rbi dity of . hunt infections in c hildren
Chi ldren with shWll infectioM have. increased moruHt)' rat.e and risk ofseizull!
than those without shunt in fection. ThOIIe with myelomeningO<flle who develop ventrieu·
litia af\er shunting have a lower IQ eompared to t.no.e without infectiOll'". Mortality
r .. nges from iO_I~'h.
PATHOGENS
Over ~~O( 5taph infe<:tiQll8 QOCur within 2 ween """t.-.t>Wlt. 7~ within 2 _.
Source is often the patient', own 1Ik.i.n'". It is £5timated thllt in . ~ofopeTatiol" (or
shunt insertion the CSF is already infected (therefoll! eulwre CSF during insertion).
Early infection
Moat commonly:
I . Staph. fpidf'.rmid~ (CO/lgUlase'lIeglltive saph ): 6O-75'l&ofiDferti_ (IlI00I1 common)
2. S.ourfln
3. Gram·negative ""dll' (G NB) : 6-2~ (may CQID/! from intelltinal penOl"lltion)
In neoDatel E. ccU lind Strfp. Mrn.oiiti.!IU domiDate.
Late infec tion (> 8 mon ths alter procedure)
Risk: 2.7-31" per palieDt (typiCIIlly 6'1t). Almost aU S. fpidermidu . Tends 1.0 be internal t.YJlf. 3.~'It ofpatien u. aCCQunt for 27'1t ofinfectiollS'".
'w.te" shunt lnffttions lUay be d~ 1.0:
1. M iodo]ent inf~on due 1.0 SlOph. fp;.u,m/di.
2. aeeding ofa vuevllr Ihunt during epiaode of septio;:em ia (probably very ten)
3. ooloniution from an epilg of merungitis
PRESENTATION
NOII" peemc . yndrome: fevet. NN, letbvg)', anomia, irritability; may mimicarote
abdomen. May 11]10 present II malfunction; 29'l. ofpatienta preMntu,g.nth .t>Wlt mal.
function bad potitive euILu.ra. In neooat.. may mllnifa t lIS apneic episodes. anemia,
hepato.plenolnts. ly, and . tiffneck". S. 'pidumidi. iofectlona tend 1.0 be indolent (s lIIOl.
denn,). GNS inffttion. Uluallyeauae mOil! severe ilIne..; abdnminal fmdingo more COmmon; main clinical ma nifestation ~ fever, .... u.lly iOl.euoitt.ent and low grade. Erythem.
and tendema •• long Ihuot tubing OCCW"Ioccuionalty.
Sbun t ne pbritl, ,,: may OOI:Ur with chronic low Iev1tI infection ofa ventrieulovlllCu,
Iar , hunt ea .... in, immune complex depotition in tenal , Iomenoli, chsracteriled by proteinu.ria lind hem.tu.rill.
Blood
t e_I.II
:ilIK:: < 10K in one fourth ofahunt infectiOM. It
i,,. 20K in one third.
&liB: tately nonnalln sbu.ot InfectiolUl.
IUCI!!d cyltural" poeitive in lui than ooe thlrd of cues.
CSf; WBC i, ul uaUy oot '" lOOc:ellllmm'. Gram .taiN may be pcNIitive .
'"
12. Infections
~O'III(yie]d
NEUROSURGERY
with S. tpitWrm,dl,;. milch lower!. Protein 11 oll:"n elevatOO, glucose may below or norma\.. Rapid antigen tu tAUIHId ror«ln.muni\)' aequlred meningi!"'" ulually not "-Ipflll
folr tht OTpnl.ffil th~l w nd to cauH shunt i!lrldion • . CSf' cu ltu rea are negative in 4()1l,
of CIltH (higher culture yi eld Ir CS F' WBC count i. > 20Kl.
EVALUATION OF SHUNT FOR lN~cnON
1. hiswry and phy.ieal direcc.ed at IMunuinilli Jlre!lenoe of.hove ligns and aymptonll with emphul. on
A. hittory 11l!:!!ut!"e ofinffCuon at another lite
I . eXlIOI ure to Dlhe,.. with "iral lyudromK. includil\l fick • •blinp
2. GI ao uroe(e" . acutl gMtroenle ritia). Of\en _i,ted WIth diant.ea.
orarrhu ii II I YDlpt.om tbat "..Ilftlly elU)llIrl'I tGf, , hunt Inftctlon
S, ollt ;1 medi, C
OllICk tymp&.olC mtmbr.net)
4. lonsilliti..rpbllryn(itia
6. appendJdtil (peritoneal lnnaulmation
6. URr
7.
2.
J.
4.
Ii.
6.
~l' ilD~
VP shuntou tnow l
I)TI
8. pneumonia
B. physitlll!:UlIl to RIO mC/l;ngi. mu. I,tiffll«k. photophobi • •,)
Hrom wac COWl! wi~h liifferenti.l
. hunt tap, ,hou ld ~dcmf in Q.li4!' of.utpe<::U!d wun! inrec:t;on. Sh.¥.lIndl~'
carefully to a¥oid inltoch.eing jnfection. GNB requires different therapy In hu
highe r lUorbidity than staph. thut it .. df\llirable \.0 ict.ptilY!hue rarlll PIIuen~
:> 9O'if> of th_ had pc!IIili"" G " III·lIa i n~ CSF .mea r (oniy. few C,am 'poIiti¥e
inrectio ... hay!!. po!Iilin l"ESull.l). GNS hllYe higher protfoin . nd low1M' g1u.:.o.e, .nd
oeutrophjl~ prKom inat. in differ.mual (unpubli~bed d!ll''')
CT, UJlu.fIlly not helpful for dj~~lng mfection. Epeodymal enhan~lMnt wben
it aero,.. hi diagnostic orvenlnculhla. CT m.), de_tr.te .hun t malfunction
.lxIominal UfS or C'I': abdominal paoludOC)'it i& l uueotiWl of inr~tion
• LP; usuaUy NOT re.oommended. May be hnardo ... in obItructi¥e hydrocephalus (HCP) with a oonfunctionillJl.hunL onen does not ,;eld the PIIlhoc.n
TREATMENT
Antibioties alont! (whbout removal of8bu.nt hardware)
Although tudieat.ion of shunt infection. wi!.hout remo¥.l ofhrdwal't! has bem
"'P'lrWd""-"" ", IIUI has a lower 1ucr:etS rale than wi\.h .hUllt remov.I". mlY require
protracted treatment (up to of!> d.ys in some) • .-i6ks probb.m& 1S,0dated with dra;ninl
infected CSF into the pentoneum (reduced CSf' abso'l'ti ...., IIbdnminlll "ignohymp\.Omil
irn:l"din, '.mdemO!ll.l! to f,,/I· blown p"nlnr,i!.il'· '. ...') or vascular . )'Stem (shunt nephrit;"
18ft fHJIIt 2141. KPl-I.5 ... 1, IUld onen requ.i rel.t leut pe rliallhunt revilion al somepoint
in CMSt e.Hfi 'l'T~IItmf!nl wilh .ttlibloties witbout . huntl"l!1llOVal b then-fori! recom·
mended only in caietlwn.,re th ""t;ent:. " ~nnirn>lIy ill,;' a ptoOr .ne<theticrisk..". h ...
vMuicln !ha.lllli,101lw difficult to clllheteriM!.
wt
Removal o r IIIhu ot ha.rdwa.re
In roDllt ill5l.1ncu. durinj: the illilial tnatment "'itb anultiol;..,. !he.ahunl it ei ther
erlemllliJ.ed (i.e. lubin, II diverted . ! lIOme point di.ual to the v,mtricul.r cathtllOr .nd
conneded \.0. clOM'd ru.ln.p ')'5t.1!ml. or sometiml!ll thfc eOlire .hunt may be NlII)O\-ed.
In Ihe IIII!.I!' caM, _
ClIe.nB orCSF dnlilla,. IIIusliHI pr!1'lid.d ill ahunt dependent CB~_
ell, Ritbe r by i ..... rtion of an t>:IRmal velltrlculardrain {EVD) ...r by int.P. nnittent "eotric:III., tip. or LPa (...itb comlllunifltllll HCPl. EVD .lIo..... ~.u,. m.. nilnnnl of CSF flo.....
conl rol of ICP, .nd re~ted " mplinl for WBC derAtVllnat;oni and eu1\IIrn,ln ' ymptomatic pltiwUl or Ih_ with . ~;li",CSFcult"l't!", 'ny hlfr:lw!lrel"llmoYed Ihou ld be
cultl>~ 15 only - 6~ .. l terile on shlln! ,,,recl;orl" Skin orpni8IDI ""' rutOdioul and
m.y taka .¥Rral d.)'II to 1JrOW.
Irtherl! i. an .bdolDilUll PMUOocy.I, the nuid .hol>ld be. dJ".ined \.hl"OUlh the pentanul Q.thRte. befo.. n!OO¥inj: it.
E mpirie antibioticlil
I. IV va n comycin u.ted init iall), Ipenetr.!Joninl.oCSF .-ull.l in co....,.,nt.. tIOnl181f>
2.
3.
tha t oheN m).
PO nralllpm m." 1M added for incruted «overlge (10 mgIII"d.y PO q 12 h($)
when rulturu rl'.tum . change ¥'noDmycin to tV o.afi:illw I>nle&l p.llienl itI PeN
allergk Or colltl>'" ahow MRSA (cood pellelral;on or inflamed >II.millj"' lower
lnlticit,. thin nMlhlcillin\, Ifbact.l!ricid.lact i¥;ty i. < I·S. _pin c,)!Isi tr adding
NEUROSURCERY
12. tnf"«1.ionl
US
4.
"fampin
intl'aventncula. injection ofpreservat.iv.·free antibiotics fIIay be UlIed in a ddi tion
to TV therapy. damp EVD x 30 mioutel after injection
Trea tme nt fo r . pecif'ic o"lla ni , m ,
Poeitiv. culturu from shunt hardwa re removed at the time of ahunt r~iBion in the
abtell/>ll ofcHnical , ympl.Om a Or ' pwitive CSFcu lture may be due to contamination and
do not require treatment'·,
\ . S. Qu .. .... and S. epilk,m;di.
A. if ~n.itive (MIC s 1.0 I'g/ml): IT geM" (TV n_ftillin, Or cef/lulin, orrephalothin. Or «phapinn)
B. ifre, lltant tQ nllfcillin (i .l . MRSA), cephalothin, orOl!phapirin: PO rifampin
• PO trimethoprill>" TV &. IT vancomycin
2. F.nte. oro«U . : !VIIT ampicillin .. IT giln! (If inlrlllVallCular s hunt: add IV gent )
3. other It rept_d: either antil treptococcal or above enter«oCClll regimen
4 . ae robic GNR.; base on lu.5<:eptibilitin; both beta· IActllllllr. APAG IV &. IT iooicat5.
"
Corynebacterium . p. '" Proprlonibactenum II'. (diphth~n;lidI)
A. if PeN unsitlv.: u" ~ntel"O(OCCa l regimen above
B. if PeN re.i.t.9nt: N + IT vancomycin
Intratheca l t he rapy
Yogev" cautions agaion b..i&h levels (ClluHd neurolopc effKI. in rabbil.l]. he ' UC·
gesl.l tlriving for CSF «Incentrationl comparable 1.0 puk blood value. ('.1:. 1().12 ).'grml
for gent, or 25·30 ).'glml for amikadn ).
Subseque nt man age ment
Ooce the CSF i"terile X 3 days. continue antiblotiea an .dditiooal l o.. l 4 d.y., thfln
convert tbe £VD 1<1 a ahunt (if ao £VD was not usN. it i• • till recoounended tb.t the
shW"lt be replace with new hardware ).
12.5.
Wound infections
12.5.1.
Laminectomy wound infection
Duun in 0.9-5.. OfCII""'5"'. May range from , uperficiall<luvere deM_nt wound
infection. The ri, k i. increased with age. long term w:-roid use, obesity, and possibly DM.
lotraoperative mild hypothermia (as conunonly DccUn in the openting room) mayalao
;oerea"", thfl risk ofwound infection ( a. demon&lnIted with colorectal ruection"). MOlt
are aouse<! by S.
<I..,..,.".
M.Io.NAGEMErfl
I . culture the wound and!or lOy purulent drainage
2. aUrt the PlItiMlt empirieally on vl ocomycin plo,., a third genention cephalosporin (e.g. «f\81idime)
3. modifY anti blot;'" apprOpriately wbeo culture and s~n.ilivity resulla available
4. debride wound of.o Decrotic and devl6CUl. rUed tiuue a nd any visible suture
material (foreipl bodj~). Superlkl.l wounds may be debridNi in the oflkfl Or
tre'lment room. deep infection. (Dun be done in OR
5. . hallow defectD may be allOWfld 1.0 heal by ucond.ry intention, and tbe following
i. on. possible rectmen
A. plldo. the wound defect wilh U."lodopboJ411 gllllte
B. dre..ina:cI... nge. II leul BID (forhOlpital ized palienl3,changeq 8 hn), remove and trim ~ O.5-t" of PKking with each <iresei ng CMOge
t. while wound i. purulent. utilize 112 nrength Betadine® w e i 1.0 dry
d ...,inp
2. when purvJence sublides •• witch 1.0 nOl'll1.l u lioe wet to dry
C. aOlibiol iel, may be utefula • • n a<.ljunel to wound lrealment initiaUy,
. witch I.o oralantibiotiao a. ea r ly a . poasible. I durllion of 10-14 day. total
is probably adeqllatc ifl_ 1 wound tare i, being done
6. .arne prefer 1.0 dOH wound by primary inunlion n , il i. critic. I that there be nO
'"
12. Infection.
NEUROSURCERY
I<!llIIioo 00 the ,", ound Ibr healing to UCCur. Soma do"", over lin irrigation II)'Bl.em
antibiotic bellda. Relefltion lIu tur"" mil)' be helpful "'
7. with large def~~ orwhen bone end/or durabeoomu exposed, the\llleofa mU!!Cle
flap IQn..n perlormed by 1\ pl,,~t.c oW'Xe<ln);' probebly requlr{!d lO
8. CSF leakage requires explorat, on in the OR with wat.e.."tighldl1Tsl closure to pI'!!ven'metljngitil
01'
12.6.
Osteomyelitis of the skull
The Bkull is yeri l1!8isUlnL to Dfll.eomyelitis, aod hemaWll"'1KIIa inf""ti,;m ill t a",.
MOI't Infeo:tiOIlllIl", due to (OnllgUOU! spread (ualUllly from on inf~!ed air sinu" <xCII·
.;onally from IUIlp aOscI!lll) or to penetrating trauma (includi.:lg su rgery and r~tal fC80lp
monil(lni"). With longstanding inft!C"tion. edema and swelling in the area may becoma
viaible radiographically, and is oaHed · Polt'" puffy lu,"or".
SlIIphylocoooua 13 the moIIl common organism, with S . oure .., predominating, fol·
lowed by S. epidtrmid~. ln neanat.el, E. coli may be the iofee<ing organiam.
Trea tm eDt
AAUbiot,as alone "I'e rarely cu rative. Trutment is UBual:y 6urgical debridement of
infeclt'd skull, biling orr io{""ted t.>uo~ with rongeu ... until a n~rmal snapping fOund r~'
ploCt!B the mOre muted sound made by rongeun.ng in f~l.ed bone. In the cue of"" infected cranlOl(lmy bone flap, the flap mU9~ be removed end the edge!! of the skull rongeured
back to healthy bona. Closure oftha 1IC4lp withou~ eraniaplu\y ill perlonne<\.
Surgery ia fQllowed by at least 6·12 weeks of antibiotics'". usually IV for the first I·
2 weekll. then oraUy fOI the remainder, Until MRSA u; ruJ~d ou~. vaneomycin + It 31d gen.
ention cephal09ponn ~re used . Once MRSA is ruled out, yancomydn may be ~hallged to
e p«nicil1inue resislllniaynthetic penicillin (e.g. nilfcillln). MD&t tnatment failurll!! oc·
curred in patienta t",al~ with < 4 w"1uI ofllntib;otics fallow"'g surgery.
If there mte no ~igns ofinfetlion, a CltlnioplB!lty may be perfonned _ 6 IJlOII po!It-op.
12.7.
Cerebral abscess
EPiDEMiOL OOY
ApProJUmHtely 1500·2500 eases per year i1) Ihe U.S" wi~h a higher il\cidenee in de·
velOping eoun lril!fl. Male:r"male ratio is 1./j..3: I.
RISK FACTORS
Risk faC"tonl ioelud e: pulmonary abl)Ormalitieti (infection, AV·fiUulu .•.. ...,~ below).
congenital oYlillQtic h ea rt disealH! lie<: below), bac~rial Mdocartlitis , penettatinll head
trauma ~e below).n~ AIDS .
V ECTORS
Pria. to 1980. lhe most common SOUl"'e of (~rebl'\ll ab5c1l1l8 ,,·a. from (ontiguaus
spread. Now, IK'matoganou9 disse",inption is the moat(ommon vKtor .
HEMATOOENOUS SPRE....O
Abloeues anaing by thi! mean! are multiple in 10-50'lI0 orclilies". No source <an ~
fO\lnd in up to 25~ of rUE'!!, The che!!t ill the mostl.'Ommon cmgin:
in adult...: lung aoo<'89s (t he moat common), bronchiectu5i~ lind empyema
in children. collO genlllll cyanotic beart d iaellle (CCHD) leatjm8kd nakafab-Ke5.11 is 4·7%), especially tetralogy ofFaliot. The i.noronlllid Het and low P<h p*
vida an hypoKio::eDvironment ~uiwble for Dbicul proliferation. ThOR with rightt.o-Iel'l (venolltrio.l ) ahun"" additionally loee the fdtering effect&. of the lungs {the
brain _m8 t.e be" preferential tll.get for Lhue i.ueclion8 over (lther organll)..
5~reptoco«al otlll fiora;1 frequent. and may follow dental procedure •. Coexistiug
cOllgulation defect.. pft.en furth .... romplicat.e managementtl
pulman8ry arteriovenou. fI5IUIM: _ 50'110 of the !I! patients have O! ler-Weber ·
NE.UROSURGeRY
12. Inf<<t,003
R.,n d u llyndrome (AKA hereditary hemorrhagicte1angectesi.J, and in up toS,*,
or these patients a cerebral abscess will eventually develop
bacterial endocarditis: only ranly gives rise to brain abs«ss" . More likely to be
associated with acute endocarditis than with subacute form
dental ol"lceas
GI infections: pelvic infeetions may gain ac<leSS to the brain vi. Batson's ple~us
In patients with S<'ptic emoolil.lltion. the risk of cerebral absct'Sll formation is elevat--
ed in arell$ of previous infarction or ischemia".
CONTiGUOUS SPREAD
I. from purolent sinusitis: sprl'ads by local osteomyelitis or hy phlebitis of emissary
veins. Virtually alway. singular. Rare in inf.nts b«.allle they lack aerated paranasal and mastoid ai r C!!lls. This route b"" become less a1rnmo:l due to improved
trealm ent of sinus disease
A. middle-ear and mastoid airsinus infections- temporal lobe and cerebellar
ab.".,SII. The risk nfdeveloping a cert'brai ab$cess in an adult with active
ehronie otitis media is _1110,000 pl'r yea"" (this risk appl'ars low. but in a
30 ~ar-old with aclive ch ronic outis media the lifetime ri.k becom"s _ 1 in
200)
B. nasal sinusitis ... frontsllobe abscess
C. sphenoid sinusitis: the least common location for sinusitis. but with a high
inciden.,. ofintracronial complications due tov"nous extension to the odja·
cent cavernous SiDWI
odontogenic: rare . kI...,.,iated with a dental procedure in the pa3t 4 weeks in mOl:!t
csses". May also spread hematogenously
2.
F OLLOWING PENETRATING CRANIAL TRAUMA OR NEUROSURGICAL PROCEDUR~
Post· neurosurgical: especially with traversal ()fan air sinus. The risk ofahsce8/1 formation following civilian gunshot wounds to the brain is probably very low with th" use
of prophylactic antibiotics, except in cases with CSF I"ak not repaiN!d aurgically follow·
ing traversal of an air ainus. An abscess fnllowing penetrating trauma cannot be \.reated
by simple aspiration as with other abs«sses. Opl'n surgical debridement to remOV" for·
eign matter and devitalized tiSl<ue is requind. Abscess hll$ been reported following use
of intracranial pressurl' monitors and halo traction'N.
P ATHOGENS
1.
2.
3.
4.
5.
6.
7.
8.
9.
culturu from cerebral abscesses are sterile in up to 25% of cases
in gen....al: Streptoeoccus i$ the most frequent organism, 33·S~are anaerobic or
microaerophilic. Multiple organisms may be cultured to varying degrees. usually
in only 10-30% of eases, but can approach 80·90%, and usually i"e1udes anuerobea
(Bacteroid"s ap. oomm~ n )
wh"n secondary to fronto-ethmoidal ainusiti9'Slrep. miUeri and StrIp. o"8i.unu,
may be seen
rrom otitis media, mastoiditis, or lung ah$ess: usually multiple organisms, including ana"robic stre~., Bacteroides, Enterobacterisceae (Proteus)
post traumatic: u$uslly due toS. OUTeuS or Enterobacteriaceae
Actinomyces may be associated with a dental BOuTe"
following neurosurgical procedures: Staph. epUkrmidis and '"'TI!U, may be ~n
immunocomprom.ised hosts including transplant patients(both bone marrow and
solid organ) and AIDS: fungBi infections are mOre COmmOn than otherwise "'"Quid
be seen. Organisms include:
A. Toxoplasma gondii: xl page 232 snd pa8f' 233
B. Noca rdia asteroides: .... , po.se 223
C. Candida albiesns
D. Li~teria monocytogenes
K mycobacterium
F. AspuSiUus (umisafus of\..en from s primary pulmonary infection
infants: Cram negative;; are common because tgM fraction doesn'tcross placenta
P RESENTATION
Symptoms: none are speci fIC for abs«ss, and many are due to edoema surrounding
12. InFections
NEUROSURGERY
1M ~.ion. MOlt arc d ... e toincI1IIIMKl ICP(HlA, NN, letllafiY l. H,miplrHia a nd Mi~ ......,.
develop in ~ of~~. P'pilledema i. rare before 2)'1"1 of ",• •
NawbQm" potent .... t ... rtl and poor ,bility ofi n!an t bT1lin to ward off in fcc:tion cr .... ial en larlemlnt. Common: Milures, me.\ingiti~, irri1.llbility, incre..inl OFe, and
r.il ...... to thrive. SOme .... thol"ll SlY lJI06t ne .... b(lml .... Ith IIbscall Ire ofebrile. Tend n1M-to
do well.
EVALUATION
B LOODWORK
Pwripbeml "''Be; o.y be nonnal oron)y mildly elev.to&\! in 00·70'lI0 of CD IN ("'B... ~lly
,. JO,OOO).
Blood cult ... re.: usuallY ntgati ....
85R: may be n.onn:al (elpecia ll y in conleni1.lll cyanotic heart dlMafie ""here paly.
t)'themi.l IOWilT$ the ESR).
C ructlva p.otein (C RP): iorectiOll anywhere io Iw>dy r;aft raise the l~ve l. f>ltien tll
with brtin t!UllOr a nd olher infllmmaVlry ",nditlon (e.E. dentalet.cellOOl m.y have. and
devated CRP level . Se:lu;i ll vity \8 ~~, lpe<:irLcity i. ~ 77 ... 101 .
LuMBAR PUNCTURE (LP)
The role of LP i, ttl)' dubio .... in a~ Al t hough LP il IboormaJ in "~. there
i, no characteristic finclioe diagnolLlc of I~. The OP i, IIi\lally increaaed. a.nd the
....'13C IIOWII ,00 protein may ~ eleva!.ed . TIIeorrending o'1"anil m can rarely be identified
C5F obta'lIed by L.P (unl eN.bIC8n rnplu .... ;111.0 "'ntridu) with po$itive c... ltures
in _ 6·22..... llIe ... ia a ri.~ orb"enJtentorial herni"ion , upe<"iaUy witb l&I)lIlle~ioM.
rrom
II
fa
k
~"l'1
ifMGING
For CT findings or .,oaooo. lltaE'l1 or alJtN:ea 1ft
Sensi t ivity app/"Ollthu l ~.
lA ... kocyte scan wit h 99mTe-HMPAO (pa,bent·. own
IlnI tocced aml.einji!:ct~ ' hllA d ose Ut l ~ w ... itiv;ty and .spo!C.rJcity (sensitivity will ~ redllCl'd ir pBtienl ia
t ...~ with ataroid$ ..... ithio 48 hI'S prior to Ihe sc.an'IN.
MRJ Ip!!OClrGlilCOPY. smioo acids and !tCI!tate or I,dale ano diaJnOlltit r",. " b _.
wlow.
woCa
STAGING OF CEREBRAL ABSCESS
T"b/e 12.2 show.
the fou r "'ell recocu1ud
hlstologit II~ or ter .....
bral a~s. ami Q)~.
lates this ",ith th.
re!li!tance 10 insertiOll
of an a&pirating needle
.t the limel)(surlU)'. 11
lak"" ltl~asI2",~b to
ptIIgn:lS th roueh Ihis
matllralionpr_. and
.teroidl tend 1.0 proIoll(
;L
CT s t .. gin,
.... w «orebrili.
h llSlill'\i lar rettu".. to esr', ~'PlUle
(.t.toge 3 ) on routine 00I"I'
tlllllt a nd non-contralll. CT 'nletall.o"", th~rapeutle [lUpoN""", in d ilf"renUltin, Ih_
1""011.1(15; thlf. foll_ill-, aid. in dilli~lhin""
cerebriti" !.enclt to ba roo .... ,1I ·defined
A. ring-enhlneemlnt: usually appellts by late c:erebri tis _tap, ua .... n"lbkk
R. fu rt""r dif"l'u.ion " reont .... t inlt) c.cntr"l lumen , IlndIor laek ofdft.,. ofen·
hllneemenlon delll~ KIIn:lO-6O min n"",,r I:Ontrall infu tion
(s\.ll1l'8 2)
NEUROSURGERY
1 2. lnf~
".
capsule:
A. faint rim present on pre· contrast CT (necrotit center with edematous sur·
rounding brain t6use eollagen caps ule to be seen)
S . Uill!. ri ng enhancement AI:iO delayed IKIInl - decay of enhancement
NB: Thin rinll' ~ Dhan~m.nt bu, I.,k ofdoJ.o)'<'d do<ay co .... I. _ bottu"iLh ",,,,brill.
!'IB: Steroid. I"OdUat dOlI""" of COCI'''''' ...wonoe ...... , (... peri.Uy in _oI>ri,,")
MRl litagiDg
Table 12·3 abows
MRJ fio<lingllin cerebra l
abscess. In the cerebri.
tis stage, the margins
are iJJ defined.
.
Table 12·3 MRllfl"lding s wilh cerebral sbacell
.... -.-
,."
Tl ..
webIilis
~
, lesion
his91al
"
t:lIn!er - iso- Of hype_r...e,
<:en1&r - low signal.
C8Jl&i'1e _ ~ hyperintense, capsule .... wei delined rim,
perilesJonal Mma .... low $igrlIII perilesiortal edenIa _ iii sigIIaI
TREATMENT
"There is no single best method for treating a brain abscess." Tl"eatment usually in·
vol,·"" surgical d rainage or e:u:ision, corredion of the primary lIOurce,and long.term USe
of antibiotics (ofum IV ~ 6·8 weeks followed by oral route ~ 4·8 weeks).
SURGICAL VS. PORE MEDICAl.. MANAGEMENT
In a patient with Buspe<:ted cerebral a~. tiuue shoul d be obtained in almost ~
and to identify pathogens (prefera bly before antibiotiC'l).
eo: case to confirm diagno.su
M EDICAl. TREATMENT
In general, surgical d rainage Or excision is employed in the t reatment. Purely med·
ical treatment of eadx absuas {cerebritis stage»", is controversial. NB: pa!.hogens were
cultured from well encaPJIu la~ a~esaetl despite adequate lev.. b of appropriate antibi·
ot;"" in 6 pat ienl.l! who failed medical therapy'"'. Failu re may bedu e to poor blood supply
and acidic conditions within the abscess (which Olay inactivate antibiotics in spite ofcon·
centrations exceeding !.he MIC).
Medical therapy alon .. is more successful if:
I. treatment begun in cerebriti. stage (befnre complete enC8PJ1ulatinn), eVen thC>\lgh
ma ny of!.heS<! lesions $\Ib.sequenUy go on to become encap!lulated
2. small lesion.: diameter of abscesses successfu lly treated with antibiotics alone
were 0.8--2.5 cm (1 .7 m.. an). ThQl!e that failed were 2·6 cm 14.2 mean).
... 3 e m is 8Uggested Ill! a cutofPI, above this surgery ahould be iltl:luded
3. duratioo ofsymptontll s 2 wks loorrelates with cerebri tis stage)
4 . patients show definite clinical impr",·ement within the first week
Medical management alone con sidered if:
J. poor surgical candidate (NS : with loeal anesthesia. stereotact ic biopsy can be
done in alm06t any patient with norOlal blood dotting)
2. multiple abscesses. especially ifsmall
3. abscess in critical local ion: e .g. dominant hemisphere or brain stem'"
4 . coDcomitant meningitis/ependymitis
5. hydroc .. phalus requiring shunt that could become infected in surgery
SURGICAL TREATMENT
Indicatiorur for initial.I..IUikIU treatment include:
I . significant man efTed .. xerted by lesion on CT
2. difficulty in diagno.si. leSpe<:ially in adulla)
3. proximi ty to ventricle: indicates likelihood of intraventricular rupture which is
associated with poor outeom ......· ..
4. evidern:e of significantly increased intracrflnial pressure
5. poor neurologic conditioo (patienla responds only to pain. or does not even reo
8poO&e to pain)
6. traumat ic absce$5 associated with fOAign ma terial
7. fungal abscelS
8. multiloculated a~ess
'"
12. Infections
NEUROSURGERY
9. CT Kan. c.nnot be obtain.ed every 1·2 wee ks
SPECIFIC MAN AGEMENT
obblln blood ~ ... l: ... ~. (rarely helpful)
initiate .ntibiotic then py (p~ferDbly aner bioP8Y l pec:i<rnln obtained), n'ga rdlel5l
of whieh mod. 0( t.rutment (medical ..... surgical) is chosen (_ ~Ww )
LP: .void in moat ca_ of ee rebral abac4.u Is« pap. 219)
. nticoro ..... I.. nU: ... &eeI in n:>OIt ~a"*, recommeflded d ... ralion i. 1·2 yr1I
A NTl810TICS
I . Initiml Intibiotiu of choice (when pMhogen unkllown, . nd especi.lIy ifS. a"f'tll$
s uspeetad), make appropri.ta chlnges I I sensiti ... ities become ....ailable. lfthere
I. no history oft:ra ... ma or ne ... ros ... rgical proced ... re, then the ri. 1r. ofMRSA iiiow-:
"'anoomw:jn: «lvers MRSA. Adult: I If'" IV q 12 hr. Peds: 15 msfkg q 8 hr.
Checlr. peak &. t rough levels and acij .... t doae accordingly (_ PtIll~ 209)
PLUS
11 3rd generntion cephalOlporin (e.g. ~efotaxime (Cldoran®)
PLUS
one of the following
• metronjdnole (F1agyi®). Adult: SO nlWkJdd tota l l1l ... ally IV(divlded q
12 h rs or q 6 hrs, not t.o exce«l4 pIId ). Ped s: 10 mKlkl lV q 8 hra
OR
•
OR
2.
3.
4.
5.
6.
chlQrJlmphmiwl. Adult: I gm IV q 6 hr. Pt.": 15·U m...... g IV q 6 hr
• for pollio-traumatic abieeu, uN PO rifampill 9 mgfkgld at 1 dOH
ifcultur<! show. no staph (II i, ... sual in non·tnum.ucabtcets), cMnge nafdmn
t.o peN G (b jeb dOH): adult: 5 M Wlill TV q 6 hr: ped.: 50.000-75,000 uoiW'lr.& IV
q 6 hr
if cultu re showl only I tr<!p, may u~ PCN G (high doRl alone
ifeultures sbow staph th1lt is 1W1. MRSA and the patient is not alltrJie to penicil·
lin or nafallin. s ... bsutu1.e IlIkilli.n for the vancomycin. Ad ... lt: 2 gm IV q 4 hra.
Peds: 25 mg/kg IV q 6 hrs
C'>'/X0«>«"6 ~Qr7fUJM, M~'1Iill"6 . p., Candltla 'P.
A. amphotericin B: 0.5-1 r:nglkglday. ABJ::LCETdD (&!II p/'Iotericin B lipid com ·
ple:l) 5 mglkgld lhould be used when ~al funaion i, c:ompromised
B. or lipoaoma l amphotericin B: 3 m...... gld.y, inc:r<!Ise to 15 """,gld
in AIDS patient:s: Tru:opJ4sfIU11JOftdii is a common palhosen, and initial empiric
t.reatmen ~ with eulfadiatine .. pyrimethamine il ollen used (1ft page 233)
Duration of a ntibioti cs
rv anlibiotica f.,.. 6-8 wks boos t commonly 6 ), may then I)'C cyrn jf Lhe CT aboormalitia !!foisl (nrovaK\llarity remaml). NB: CT improvfl1leflt may Iii: behind clinical
improvement. O .. Tlltioo oflffatmeflt nlay be red ... ced;r abecef l and capsule entirely e.·
cised lurgically. Oral a:otibiolics may be used following IV course. 5-2O'I.oflbsc_ recur within 6 wee"- of dillCOlltinlliog anubiotics.
SU,ROIOS
Oe<;rta_ likelihood offibrou.t eneaps ... lalion of abscess, ;,ut may reduce penetra.
tion of antibiotica jnt.o ab.etu - . Rese .... ed for patienu with CT and clinical evidence of
deuorioration from marked mua effect.
CTSCAN
Repeat CT aftu wu" " _2 (mor<! often if patient de1.enoratee).
RecommeDded follo ...· up: a ner I (ull cou rse ofantibiot o«. CT q 2..... wlta ... ntil res·
oIution (3 .11 root mean : range 1· 11 mas). Then q 2·4 mas for 1 yr. and subsequently any·
time eNS l ymptDml occur.
Iftbe.. py it . utCUllful. CT , bollid show decrease in:
I . degreeofringe-nhance ment
2. edema
NeUROSURGERY
12. lnfectionl
'"
3.
mua effect
~.
.ile of I..ion; takes I to 4 wk, (2.(> mun). 95~ of IftiolU that will reeolve with
aIltib,otics . Ione decrease in sile b)' 1 month
SURGICAL TR EATMENT
Current methods eonsi,t of one of the follow;nl";
1. needle a.piration: the mainstay ofturg;eal t reatment. EspeeiaUy weU·.wted for
multiple or deep I"ions (He IM/ow)
2. aurgieal exciaion: pNVents recidiviam. $hort.enslenrth ortimeon antibiotiq. Retonllnend"d in traumatic ab&«M to) debride fon:ign material • .."d in (lUlIal ab_ " oo.:auH of relative antibiotic resiatance t - ~/.ow)
3. external drainlllt: eontrove"ial and mayor may not be ufed
4 . in8tiJlation of antibiot kli di rectly into the ab&Ceu: has not been utl'llPWly emea·
dous. although it may be ufed I I a Int ruort in A'~rllillu' a~
NEEDLE ASPIRATION
May be perfon:ne<lunder local e~tthe.ia if nettsaary. May be OJmbined with irrigation with antibiotic. or non:nal . ali"". Need . to be repeated in up to 70'10ofeun. May
be the only surgical inte rvention requi red, but 8Ometi.r:ne. must be followed with uci.ion
(especially with multiloculated a~"). Stereotactic drai nage may be ideal for deep
lesion~ .
P~rfo rmed
through a trajectory chosen to:
1. minimile the path length throuSh tha brain
2. avoid t raversins th~ ve ntricle!! or vital neural or vascular 1tnK:lul'flll
3. avoid t raveraing infected 8tnJ.CtUIU oUllide the intracranial compartment (in·
rected bone, paranaul . inuse&, and scalp wound.)
4. in CllSes of multiples abscesses. tertle!"':
A. the l arg~8t lesion or t he one eaUlin, the lDOIIt symJ>l.'.l<m
B. One<;! the diagnosis of abscen is confirmed
I.
anyle.sion~2.5cmdiameter
2.
lesions causing significant mllS$ effect
3. enlatgi.og lesions
C ultures
Send aapirated material for th e following:
I. ,"ains
A. Gram , tain
B. fungtlll stain
C. APB stain
2. culture
A. routine cultllre.: aerobic and anaerobic
B. (u",at (I,Iltu r" this is notonl), helpful for identi(ying (llngal infections, but
since these cultu:'eS aTe kept fOT longe r period and an)' growth that OttIIrI
will be further tbracterized. fastidious or indolent bact.erial organi$1D!I
may 80metimea be identified
C. TB culture
EXCISION
Can only be performed dllrln,the "chronic·
phase(latec.~ule.taa:e). Ab_ i. removed as
any well e"ca~ lIl .ted tumor. The length oftiroe
on Intibiotiu tan be . horUne:I to - 3 days;"
.orne"," followi", IoOUoI excision o(aIl aceessi·
ble, mattlre IbKe.. (e.I.located io poieofbrain).
Recommended for 1b8cft_ asIOCiated with (oreign body and moe t Nocorokl abeoesses (_ be·
r able 12-4 Outeomet with ",Dbr.1
a btu..
"").
O UTCOM E
In the pre-CT erl, morta6ty r""ed form ~~. With Improvement in antibiotic"
I Utpry. sod thfI improved ability to diagnOM and follow mponn ",ith CT andlor MRI.
'"
12. Infec:tiona
NEUROSURGERY
mortality rate has beeo reduced to _ 10%, but morbidity remains high with permanent
neurologic deficit or seizures in up to 50% of csses_ CUrTentout<;omes pre sbown in Tobk
12·4. A worse prognoai$ is si$OCiated with poor neurologic function, intraventricular rupture of absce!;ll, and aUnost 100% mortality with fungal a~es in transplant ro<:ipi·
enla.
12.7.1.
Some unusual organisms producing abscess
NOCARDIA
Nocardiosis is caused primarily by Nocardia oSUroitk. Cother Nocardio species . uch
as N. brosilj"I1,,, are less common), a soil-born aerobic actinomycete Ca bacteria, not a
fWlguS) that is usually i:loculated through the re$piratory tract and produces a localized
Or disseminated infe.::tioo. Hematogenous spnad frequently ~ults in cutaneous lesions
and CNS involvement.
Nocsrdiosis occurs primsrily in patients with chronic debilitating iUnesses including:
1. neoplasms: leukemia,lymphoma __ •
2. conditions requiring long-tenn corticosteroid treatment
3. Cushin!!,s diseaae
4 . Paget's disease orbone
5_ AIDS
6_ renal or cardiac organ transplant re.::ipi'!nts
The diagnos is is suspected in high _risk patient.s presentinl with .,.,ft-.tissue abSO!!~·
es and CNS lesions . CNS involvement occurs in about one-third and includes:
1. cerebral abscess: onen n'ultiloculated
2. meningitis
3, ventriculitis in patients with CS F shunt"
4. epidural spinsl cord compression from vertebral osteomyelitis'"
Diagnosis' Brain biopsy may not be needed in high-risk patients with conlirmed nocardia infection in other sites", except possibly in AIDS patient.s "'here the risk of multiple
organism infections Or i"fection plus tumOr (particularly lymphoma) is considerable.
'I'Natme n t, Usually includes trimethoprim-sulfamethox8Zole (TMP-SMZ) together
with imipenem, cenriaxone, cefuroxime or cefotaxime, Duration of treatment is at least
6 weeks , and TMP·SMZ is usually con tinued for many months because of the risk of reo
lapse or hematogenous spread ,
12.8.
Subdural empyema
ReferTed to as subdu ral abseeu prior to
1943". Subdural emp),(,ma (S DE) is a suppu_
rative infection that forma in the subdural
space, which has 00 anatomic barTier to
spread" Antibiotic peMtration into thi s spae<!
Is poor_ Distinguished rtom abscess which
fonns within brain suh!! tance, s urrounded by
tissue reaction with !'ibnn and conagen capl ule
formation. Helice, SDE tends to be mOre emergent.
SDE may be complicated bYe<!rebralabSCI''''' (seen in 20·25% of imaging studiu). cor_
tical venous thrombosia with risk of venous
infarction, or locali:t.ed cerebritis.
Ta ble 12-5 Et iologies 0 1 SDE
""",e
EPIDEMIOLOGY
"''''''1' ' ' In 8<lufts
no cases I,,,,,, OIltis ., • 'ecen1 ...,ies"
Less a)mmon than cerebrnlabsce... (ratio
ofabscess:empyema is_ 5,1). Found in 32ca5e1
in 10,000 autopsies. Male:female ratio i. 3:1.
Location: 70-80% are ove r the convexity, 10--20% are parafalcine.
NEUROSURGERY
12. Infe.::tions
ETIOLOGIES
See T(lb/~ J2·5. Most ofl.f.n OCCUr/l 011,0 TelIult of direct utens'on ~f 10(01 infe<:tion
lror ely following !;o!!ptlt(!m'a). Spf<'od ofthe infection \.0 t.h.i! intrncranlol eornpartment
may I)ttur through tt,,~ valvelfM diploi~ "ains, ofl.f. n with 8~t.ed thrombophlebitis"'.
Chroni~ otitis medi .. was tne leading """"" or SOE in the proontibiotieern, but ha..
now been il....pused by paranasal !tim.. d,seol6 especially wi!.h fronl.lllsinUll
involvemfM" (may also follow mutoid ainusi!ia), SO£: is a ror<! bu t aometimes fotal complicotion orcrania] tllletion df'IKu... · '. In fe<:tion orp~ultlg ~ubdu",1 hemlltomas
(bot h treated and untreatt-d, ill, infants and adultll) have been reporUd".
'Trauma includes compound &1<1.111 frllCtUTeS and penetrBting in,jU'ries. Other etiologiee mdud .., I>st.eomyelitis, Plleumon;a, unrelated infection in diabeli=-.
PRESENT~TION
Neuroll>gic findingS ,re5hown ;n T"b/e 12-6.
Sympt0m.5 are due w maSll ..ffect. inflammawry ;.,.
volvenlMl of thp brain and mlminges. lind throm·
bophJebitia of ~ereb ,.,.1 veins and/or venoulfolnuses,
SO£: should beauspect.et! in Ihe prel!ence. ofmeningi.·
mus + unilateral hmisphre dysfunction. Marked
tenderneS!! to percussion or presr;ure over a/fe<:\.ed air
"in u~ Is comml>ll" . ForeheaC: or eye "welli ng (from
emiuary ~pin thrombosis) C\!I.Y·occuc.
Focal neurologic deficit andlor sei~ur\lS usually
OC'Cur law.
hble 12·6 Finding_ on preaenlallon with SOe"
EVALUATION
CT: rv contTl\$l is usually helpful. CT may
,russ IIIn'e caselI (relatfld ~ early generution
_nners, failure to give. rv colltralll. pooracan
quality ... )' Ifnormal. r~~t tbeC1' at a loter
tin,. ordo an MRI ifdi nlCIII , uapicion persi8\A
Findinga: hypodl!frM! (but denser than CSF )
~o.-n. ,"";""oftr\l>lllple atlleM<l'"
creficentic or lenticular elttrucerebraJ IHlon
with dense enhancemel)t ofr:n&diel m~mbrane;
Inwa.nl displacement of gray.white interface; ve.ntriwlar dUr~rtion lind efTnoenlent ofba"l cisterns lire r:tImmOn findinga"
MRI: low signal on T1WI, high signal on T2WI. Pial epend)'ll\allin~: II non .• pecifi e MRI finding in Cr.· S infe<:t;on
LP:. pptentlaliy huardou$ (ri~k nf herniatiou). OrgauismIi are 1.JlI".ally present
only in cases originAtir.g from meningitis. Jfno maningiti., mode", .... ,tenIa pIeocyt05i. (\50-600 WBClmm'l with PMNs predominating; gluCOS<! normal; open·
ing pressure ill 1.l5uolly high" ; protein is usually ele~et.ed \ ren,ge: 75- 1 ~ mg/dl)
ORGANISMS
The causative organism "uries with !.he
'pecific lHIurce oftha infe<:t;on. SDE 8S8Odatetl
wilh . inu$iti.rr is often caused by aerobic ond
lln".,."bic .t,eptocoed (He T"bu 1.1. 1). Foll" ...·
ing trauma. Or neurO$ucgical procedures. st/l·
phylwocci Ilnd G .. m·negstive speciH
predomill~te. S lerile (:Ulture5 OCCUr in up to
Table 12-7 Qrglnl&ms In adull cases 01 SDE assoelaled witosinusili s
.""'.
TREATMENT
I . surgical dlllinllge: indkat.ed III 1\I.000t ClIl!e!l l nonsurgical managemoot hw; been
reported·l . bUUhould onJy be cOll/iidert!d with minimal neurologic inv"lvement,
limit.ed lI~tell5 ;On and rna&9 efTec~orSOE. snd early ravorable NIIPP!liHI to anubi.
otiu) usually done relstlvelyewe'llenUy
e..ly In the course, the pus tend. t<l be atore fluid lind may be more ame nable to
burr hole drainllge ; later, loculations develop which mQY n~essiulI!e ~l'tIniotomy
there has been cont roversy over the optimal su rgic~1 tre,tn'ent. Early ~ludilll:l in ·
dicated a better outeomll wilh L'l'IIJliotomy. Recent ~tudi "" show leas difference
A, ~riticaUy ill pstie.nL5 with JocsJ[~ SDE may becandidll\.e5 for bQr ... hole
]2. Infe.:tiora
NEUROSURGERY
drainage (usually inadequate if loculations are present). &peat prooed ures
may be needed, and up to 20% will later require a (:I"aniotomy
craniotomy: to debride and, if pOSsible, drain
ant ibiotiCII: .imila r to treatment for cerebral abscess
• initially: a penicillin and a thi rd·generation cephalosporin (e .g. cefotuime)
• metroniduole is added if there is a high suspicion of anaerobes
• for post--<>pSOE: substitute vancomycin for PCN (switch vancomycin to a
PCN iftllere is no staphylococcus)
• modify antibi<.>tiCII based on culture results
• duratio,,' usually 4-6 weeks
anticonvulsants: usually used prophylactically, mandatory ifseizu res OCcur
a.
2.
OUTCOMe
Set! Table 12·8 . Ne\lrologic deficita were present i.n
55% of patients at the ti me ofdi&charge". Age ~ 60 yea,.,.,
Table 12-8 Oulcome wlth
SOE
obtundati<.>n or coma at presentation, and SOE related to
surgery or t rauma carry S WOnle prognOllis". Burr-h<.>le
drainage may be associated with a worse outcome than
with craniotomy, but this may have been influenc«l by the
poorer condition of these patients. Fstal casel may have
associated venous infarction of the brain .
12.9.
Viral encephalitis
Encephaijtides lha , come to the attention of the neuro.surgoon uuaHy CaU$e imag.
ing findings that may mimic maS8lesiona. Biopsy is helpful in some instances, and
shunting for hydrocephalus may (>(X8$ionlilly be needed. Those covered in this book:
I . he~s simple~ encephalitis: Ut bdoI.U
2 multifocsl herpes varicella·zoste r virus leukoencephalitis: 1ft page 227
3. p~saive multifocalleukoencephslopathy (P1tU.): I « ptJ~ 231
12.9.1.
Herpes simplex encephalitis
.
t Key featu rel'
hemorrhagic virallmcephalitill with predilect i<.>n for temporal lobes
• definitive diagnOElili requi res brain bIOpsy
• optimal tTeatmeat: ea rly administration of rv acyclovi r
Herpes simplex encephalitis (HS E ) AKA mul ·
Ta ble 12·9 Adult
tifocal necrotiling encephalomyelitis. is caused by
the herpe'S simplex virus (HSV) type I. I t produces
an acute, often (but not always) hemorrhagic, no;.
troti~ing ellcephalit is with edema. There ill a predi .
lectio" for the temPQraland orbitorrontallobes and
limhic system .
I
E PIDEMIOLOGY"
Estimated incidence of HSE: 1 in 750,000 to 1
million persons/yr. Equally distributed between
male and females, in all races, in all ages (over33%
of cases occur in children 6 mos to 18 ynI), through.
out the year.
P RESENTATION
Ta ble 12·10 Presentation in age
< to yr.
aftered mentation
seizure
.",....
hemiparesis
!ever
papiRedema (e~cepl in age s 2 yrs)
Patien~ are often confused and disoriented at
onset, and progress to coma within days. Adult presentations are shown in ToMe 12-9,
and f<.>r pediatriC'l in Ta.ble 12·10. Other symptoms include headache.
NEUROSURGERY
12. Infections
m
DIAGNOSTIC STUDIES
DiagnOllis tan o~n be made on the basi s ofhiatory, CSF, and MRI. Treatment
should be instituted rapidly without waiting for biopsy, before the ODlet of coma.
\. CSF: leukocytosi$ (mOlltiy monos), RBC& 500- t OOOl'mm'. (NB; 3% have no pleocytosis), protein rises markedly as disease progreasea. HSV antibodie.a rna.yappear
in the CS F but takes a t least ~ 14 days and is tbus not useful for early diagnOliis
2. EEG: periodic lateralizing epileptiform discba rges (PLED,,) Itriphasic high.vol\.age discharges every few secollds) usually from the temporal lobe. EEG mBy vary
rapidly over few days (unusual in conditions mimicking HSE)
3. (''T: edema predominantly localiled in temporal lobes (poore r prognosis once
hemoJ'Thagic lesions visible). In one review, 38% of initial C'J's were normal"
(maoy wereon ea rly generation CTsulUleTsor were done within 3 days of onset).
HemoJ'Thages were appa .... nt in only 12'l>ofthe initially abnormal CTa
4. MRI: mOre sensitive than CT"", demonstrates edema as high signal on TIWI, primarily within tbe temporal lobe, with some e~tellliion ael'Olls sylvian n.ssu re
("trlllluylv ian !ign"}'l. especially suggest i"", of HSE if bilateral. Differentiate
from MCA infsrct (which msy aJ.sospan sylvisn fisaure) by typical ane risl distri·
bution of the lotter. Enhancement doeSIl't OCCur until the 2nd week
5. technetium brai n Kan: proc:ess 100000lized to temporal lobes
6. brai n bioplr)': falll<! negative. may oecu""
A. indication s: rue,...ed for QuesliGoable CIIlIe8. May nGt be necell88ry in pII.
tienla with fever, encephalopathy, compatible CSF findinp, focal neuro
findings (focal seizur e, hemiparesis, or cranial nerve pabiy). and supponing
evidence of at least one of the following: focal EEG, CT, MRI Or te<:hnetiWll
brain scan abnormality
B. should be perfonned within $. 48 hra of starting acyclovir (otherwise false
negatives may occur)
C. /Interior inferior tempOral lobe is preferred site
t. the side eh"",en for biopsy i8 the one showing maximal involvement
based on d inical information (e.g.locaLi~inguizures), EEG and/or imaging studies"
2. 10 . 10. f> mm deep specimen obtained from anterior portion of the
inferior temporal gy"" w ith NO COAGlILATION' On specimen side
(cut surface with ~II blade, then c/luteriu pial surface on rum-specimen aide)
3. 2nd specimen obtained from beneath surface spe<:imeo with fenestrat·
ed pituitary biopsy forceps
D. virus isolation i. the mOlit specific (l ()()%) and 8efUlitive (96,97%) test (or
HSE . Other nnd ings (less 8c<:u rate~. perivascular cuffing, lymphocytic infiltration, hemoJ'Thagic nocrosis, neuronophagia. intranuclear inclusions
(p~.orent;n 50%)
E. ifelectron microscopy (EM ) Or immunohiatofluorescence is available, 70%
may be diagnOli.d within ~ 3 hra Gfbiopsy
F. biopsy tissue handling
I. avoid macerating specimens (or histology
2. tiSllue (or E M: placed in glutaraldehyde
3. tissue (or permanent histology: placed in fonnalin
4. tiasue for <ulture:
It.
I>"OOl i"g: .pooci m~o ill plua:d in 8", ril~ "pe<:i "'~R oonUlin~r and
sent directly to virology lab. Iflab is dosed, tillsue may be:
i. placed in regular refrigerator (or up to 24 hrs
ii. placed in -70' C tTe.!zer for indefinite time (virus re mains
viable fGr up to 5 yn)
iii. DO NOT place in ~lar ftteur (destl'Oy!J virua)
b. cu.iwr es gener/llly uUte at least 1 weel< to become positive
c. cultures checked for 3 weeks before being declared negative
G. biopsy tesulla: of 432 brain biopsiell meeting the aoove criteria, 45'1> had
HSE, 22% had identifiable but nOll HSE pa~hology (e.g, vascular disease,
other viral in(ec~ion, adrenal leukodystrophy, bacterial infection .. .]. and
33% remained without a diagnosis"
TAEATMENT
General&upportive meaSureS: to control elevated ICP from edema. includes: elevate
12. Infections
NEUROSURGERY
HOB. flnonn't.ol. hyperv(ntillltion (dnomethasone unproven efficacy) (ab!.o aee lCP lreolnuml ""'US"''"''''. page 655). Phenytoin is u~ed for !l(!izure proph),lfLril.
Antivira.l med ica tioDs
Ganclclovir is gaining f,\Vor Ove r acyclovir_
~
acyc:lovir (Zovira:<®)
\
/
0A\b1f'l1'O
\
,
IU Adult: 30 mglkglda),. In divided q 8 hr dose. in minimum volume of 100 ml rv
Oujd over 1 hr (caution: this fluid load roay be haunlou • . especioUY$incecerebral edem~
i, al ready u8ua\1y probl~tDaticl for 14 -2J day. (tome relap!lell hav( been reporW after
only 10 dllYS of trnatmMI.)
& C h iJd r en ,. 6 J;lOIIlIge: 500 mg/m' rv q 8 Iin)l 10 day>l.
& Neon atal : 10 r.>glkg rv q 8 hn; for 10 days.
Outcome
Six month mortality following tnatment wfth aeyda-·ir wos infl uenced by-.
oge 16% under age 30. 36'11> \We T age 30)
Glllsgow coma aoore IGCS) a~time ortreatment initi ation (25% for GCS .. 10.0%
forGeS> 10)
d uration of di~el,6f! before Ulllrapy (()'j& for initiatinll' therapy within" day~. 35%
ifaner 4 days)
12.9.2.
Multifocal varicella-zoster leukoencephalitis
Ca uM!d by the herpt"s varice\la-ZOllt.er vi ruB(VZV) which i. responlible for varicdl9
herpes zoster (HZ) (shingles). ~nd po!llo-herpetic peu .... lgia ($"" fXlIJ/' 387).
VZV is" " herpelvirus that is distinct from the ,",rp'" .imp/ex~_
Symptomatic_ler -related encephalitisoccUf"6 in < 5% ofimmunooompromised pIItfeot.05 (ineiuding AIDS patients) with cuUlneQu s zoster"'. It typ1C11lJy faU"",. cul.8neous
AZ by 8 shon time (ave rage: 9 days) although ""su h8ve been reponed whre nlany
Illonth.o hllve lap •• d ft ,
ManifeBtation ~ include: alterM level ofconsciousneu. he~~ sche, phot.ophobia. m~_
ingismus. Although focal neurologic defJcits m8y occ:ur. t hese liTe UnCOmmOn.
MID m8y ~how multiple, di s'orete. round and oval lesion.'! .. ith minimol tdema (best
se<!n 00 1'2WIJ and minimal enhancement.
Unlike herpe~ .. impl"" vi rus, VZV '" difficult t.o iBolat.e in cult ure. On brain 6ioflSY.
look for multiple d",c rtleleaioDl wfthin grey and white matler_ with Cowdry type.A intranuclear inc!u$,on bodie. in oligodend roeyt.e• . astro<:ytea, and MUtOns. i nd D positive
direct fluousctlnt . ntibody telI l directed IIll"in.ot VZV.
r here is a case report ofVZ:V encephalitis tn>ated wjth IVacyciovir6"_
fcbic~npoJ{).
12.10.
Creutzfeldt-Jakob disease
1 Key feotures
• on inv aria bly fatal Mtephlliopathy choracteriud tty rapidly progressive de men tia. ataxia and myodonull
death u.8uaUy OCCUrl within I rr.0f onget of&ymptoma
3 form~ I I transmi~sible (pOs,uhly via prions), 2)"utoloroal dominant inherite<1,
3) sporadic
characteristic EEG linding: bilateral shllt'P wave (0.5-2 per sewnd)
pathology: ~t.all•• 8pongillll1.>5 without ioflamlIl/Otory ra!!ponse
Creullfeld Wakob.:Jisease (CJl) ) i. one of" k.oowo rIlJ"1'human dilll!63e$ ollSOCiated
with tronsmillSible s pongiform encephalopathy agents. slsa cs Ued prions (prot .. inaceous
infectious partlclle"). Although eometlm~ij al$O refelTed to na ' 610w viru$". these agents
conttlio 00 nucleic acid, and ara alao re3i.sta ot to proussea that inact ;vatll conveolfona l
virtlllE:$("'~ T(Jble 12-12). Priona do not provoke an isnmune respon..e.Tha prot-. r""istenl protein ailloc:iated 'with di5e1lH IS designated PrP- Or P rP'l'. and Ul lin ;.of = ofa
naturally DCt;uning prou.ss ..... ensitive protain deAignated Prf-> or Prf'C.
NEUROSURGERY
12.
lnfe~tfons
AnnulIl incidence MCJD: 0 .5-1.1:' per miU'.,o population", Over 200 poople die ur
CJO in the U.S. each year. CJD oe<:urs in 3 form" transmissible. inherited and sporadic.
Acquired prion diseases: Natu",) route ofinfocti'", i. unknown and viruleno;eappeara
low, with lack afsignificant disoomination by respintory, enteric, or lU,'J[uu\ contact.
Then> is no inrre!llled incidence in apouses (only II. single conjugal pair of cases has been
verified ). phyaieisns or laboratory wnrkers . There is no e~idence oftt'ansplatentaJ tranamission . Theonly known casesofhori~ntal transmi$$i<:In ofCJD haveoe<:UlTed iatrogen.
ically (ou below). Kuru has been transmitted via handling and ingestion of infected
brains in ritualistic Funereal can.naba/ianl practi~ among the Fore (pronounced: 'for.
ay"J lingllistic group in the eastern highlands of Papua, New Guineafl, a practke whkh
was generally abandoned in the 1950's. Kuru is a 8ubacut4! . uniformly fata.l disease in·
voJving cerebellar degeneration (the word "kuru" meatls"to tremble";n the I""a.l
language"'·").
Mtls! tltItIiatrogenically transmitted casesofCJD occur in patienb > 5-0 yrs old, and
is rare in age < 30. The incubation period can range from months to decades. The onset
of symptoJJl.!l f"Uowin!!" dired inoculation is usually f&'lter (eommon range: 16.28 moS),
but atill may b.. much !"IlgE'r(up to 30 y ......... with corneal transplant", and 4·21 yrs with
hGH transmission).
Inherited CJD: 5-15% ofeana of
CJD occur in an autosomal domiTabl e 12-11 Comp!lfison 01 VCJO 10 sporadic
nant inheritance pattern with abCJ. .
normalities in the amyloid gene"'on
chromo.oome20 with a penetrsn"'" of
0.56". Since familial CJD is domi.
nantly inherited, ana.lysis for the
PrP gene i. not indicated unl"llS
ther~ i. a history of dementia in a
. tr"
liMIt de~ relative .
Ii·
Sporadie CJD: ItI~ 90% ofcasellof
CJD. noinfectioU.9 or familial source
can be identified", and these cases
are eonsidered sporadic. 80% (l«ur
in persons 50·70 yrtI old". Sporadic
cases show no abnormality in the
PrP gene .
New varia nt CJD: C85e' of atypi_
cal CJD are we]]·reoogn i~ed . A new
variant ofCJD ( vCJD) was identified
in 10 cases ofunusuaUy young individuals (mediao age at death: 29 yrs) duriog 1994·95 io the United Kingdom".
and haa been strongly linked to the
1930s epidemic of bovine spongiform
encephalopathy (BSE), dubbed "mad
cow· disea se by the lay press. None of
the vCJD patients had periodic spikes
on EEG characteristic of claS!lic CJ D.
the dinieal CQurse was atypical (having
prominent psychiatric aymptools and
early """,ballar ataxia, 6Omewhat a imilar to kuru), and bra •.:! plaque~ .howed
unusual feature!! alao rem;n;8C<'llt of
amyloid plaques seen in kuru. A COIIIparison ofvCJD to sporadic CJD is
shown in Tablf 12· 11.
Iatrogen ic transmission o r em
Tabla 12-12 Ope/"8!lng room .Ierillzallon
procedurealor CJO"
. ,.
Fully m\edive (recomrnsncled) prOCGdurtS
autocJavlng for 1 hr at 132"C, Qr
in I N5<XiIJn hydrodde (NaOH) for I
,. steam
mr,ersle>n
hr at room
~alur 8
Partlalfy eIfective procedures
A. steam autoclll'ing II ei1he1121' C or 132' C lor
,.
c.
.
15-30mifIs, or
'm:ne!s;on in lNNaOH for ISmins. or IoMr
con<::eO~arions « O.SNl lor IIIr a1 room te~. or
Immefsion in sodium ~ (household
bleach) undiuted or up 1(1 1:I0 oiIution (0.5%) for
1 hr"
II ~ proce~res:
bOiling. UV or ior01g radiation. eIt!yIeoo oxidIr.1JIh100. loonalin. bell·propioIacIooe, cIeIer\jel"lls, qua1emary ~ compolll(ls. l~. 1IIrohcIIic
iodioe. acetor1e. pola.ssi1rn permangarnue. rQtble
.......
Described only in cases ordirec~
con tact with infected orgaN. t ir;aues or
surgical illstrumen\>i . Has been reported with: corneal transplsnts"'--, in tracerebral
EEG electrodes st.erili~ed with 70% alcohol and fonnaldehyd~ vspo r after use On a CJD
patient'"'. operations in neurosurgical O.R.s after procedures on CJD protienb,;o recipi·
~Ilts of pituitary-derivedA human growth hormone (hGm", and dural gT8.ft with cadav-
".
12. Infection s
NEUROSURGERY
eric dura mater CLyodura®J. Recommended stedli~at;on procedures for auspected CJD
tissues and contaminated materials appear in Tol>I~ 12·12.
Pa th ology
The typical fonn ofCJD produces the dassic histologic triad ofneuronalloss,lIstro.
cytic proliferation, and cytoplllsruic vacuoles in neuron! and astrocyte. (sta l u. 8pon gi.
oa'.), all in the ahsence ofan inflammatory response. There;s a predilection for cerebral
cortex Dnd basal ganglia, but all parte of the CNS may be involved . In 5·10% of cases,
these changes are accompanied by the depotition of amyloid plaques. Immun08t.aining
f!IT PrP"" Is definitive.
Prese nt a tio n
One third initiaUye:o:press vague foolingsoffatigue,
.leep disordera. or reduced appetite. Another third have
neurologic I ymptoms including memory loss. confusion,
or uncharacteristic b;.havior. The Illst third have focal
signs induding ~",beUar ataxia. aphasia , visual deficits
(ind uding cortical blindne"'l J, Or bemiparl$ia,
The typical course is ine"orable, progression of dementia, oA.en noticeably wone wook by week. with sub·
sequent rapid development ofpyramidDI trDct findings
(limb weakness and stiffness. pathologic reflexel), and
late extrapyramidal findings (tremor, rigidity, dy ... r.
thria, bradykinesia) and myocl(mu s (often stimulus trig·
gered). Clinical sign. ohporadic CJO are .hown in Tol>lt
12·13.
Supranuclear gaze palsy is an occasional finding,
also usuaJly late"' . In utly stagea, CJD may rf!Bemble
AJ,heimer's disease (SDAT). 10% of casea prellent as
ataxia withouLdementia Or myoclonus . Cases with predominantspinal cord findings may be initially mistaken
forALS.
Myoclonus subsid"" in the tenninal phase •• lind ak·
inetic mutism ensues.
DIAGNOSIS
The complete "diag·
Table 12·14 Olag nosllc cr1tena " 01 CJO"
nostic triad" (dementia.
PatllOloo;tk:aUy eonllrmed (WIth unequivQI.:aJ SI)OOgifolm d\ange$)
myoclonus and periodic
cWnicaty: requ~es bran biopsy lsee teJO
EEG D~tivity) may be abo
B. IoofICI at aulO9SY
sent in up to 25% of cas·
o...ration
1·2HlI*
Clinle.1 crlterla "~~
ea. OiagoDStic criteria
de\eoo.
riodicEEG I'!1erII dOsorOel
have been published" al
,""".~ 01 periodic
(monlhs)
shown in Tobit 12· 14. No
EEG adiYity
patienL! in their series
ciinicaIIy delW1e
with a diagnosis other
than CJD fulfilled the
OR
dinic.atf probable •
criteria for elio.ically deli· d1nieally possible
nil<> CJD.1'h .. ",,,,,t oom'
., paUenlS ..... 1I> "",mal motIIIt>oIic: I18IU$ and spinal nuid. H thOle .re
mon condition other than
eM,.......tlooUa, or "",at $)'II'[)IOmS and Iht!1 mu"",'" tigidi\y, or iTat>CJD fulfilling the criteria
oIher IIIm/1y member hair died 01 pall'lOlOgicalty"";fiII<l CJD. thert up·
for clinically probable
\llaae the degr. . 01 cet1alnly to lhe n...1'-Il"-r category
CJO was SDA'l'(especial·
Iy difficult to distinguish
in the early stoges).
There is a CSF immunoassay for the 14·3-3 brain prolein Cut btolowl.
.,
...
. ., ....
•
•
•
•
""-
•
•
•
.,"
"""
d'
,"
D ifferen tial di a gn osis
CSF examination to exdude infections $11th S8 ttrtiary syphilis or SSPE is rec(/m·
mended . Toxicity from bismuth, bromide. and lithium must be ruled·out. Myoclonus il
usually more prominent tarly in to:<.itlmetabolic disorders man in CJD, and seizurea in
CJD are usually late".
A,
W,..,;" no lonll<' . riok orCJ'D with ...... th h""'IOM;" <he U.s. . ;nee dw.ributiol> ofpit"i",,,),
derived hGH .... hlOltod in 1985 a l>d"",.,..nt hGH 10 obtained I'm.. """.. bin ... t DNA te<hnol"IY
NEUROSURGERY
12. Infections
'"
Diagnostic. teah
ImagiDg: nO cha.racteriat it CT Or MR finding. ThHf> &tudif!8 are freQuen~ly normal, but are _ntial :on OIle .... ut othe. """dilions (e.g. " e.pel-simplex enoephali.
tis. te<:ellt It..oke ... ). DiITulHI atrophy m~y be present, especially late. MRI may
ahow inerel1M!d ,ntolna;t)' on T'2W\ in al'flu typicalJy involvt!d i bllJlw ganglion,
nri,lLum) in up 10 7~ of C8aes \Mf'Ol pectively)"', Thil i. nouspKific but may
help differentiate CJIJ Freno SOAT'"
blood tc.tII: serum aauya for S ·I00 protein are 81' itlllenlit[,re and nonspecific"
thllt it CDn Dilly btt u~ed ItO an dillglll"'tiC udjunct
CSF:
A. routine lab!!: usually oon:nal, although protein may _iollally ~ el~ated
B. abnonnlli prote ins!
L abnormal protein! ( ISO" (31 ) have been identified in the CSF of pIILient.!l with CJO", but tlle I\$S~y il technitally difficult
2. prot.eins 1301131 were Identified 81 the I\lmJlJlneuronal protein 14-33, and II rl!latively aiD:lple ;mmulloasaay forthi. WRi de;;eloped for use
on n Utll .. 9550 1\1 ofCSf"I. Oeloe<:tionohhe 1<4.$-3 pTo!.!!;n 10 theCSF
has 96~ 8,,-ngi tiyit,y and ~peciticity for CJD among pati"-n!.!: with demelltta . Palfle poII;tiye. may occur in other conditio", in volv;ngexten9;y,,- neuronal dutTUtticn induding, acuc.e.CVA, ~erpeli encephalitis ,
muiti-iofilld dementia, prim a ry CNS lymphoma and rar~ly SDAT
(most case. o(SDAT tell negatiy .. ). ReqUire. CSF (cannot be done en
blood)
EEG, charaderi,tie-fioding of bit at.oral, Iytrlluetrical, periodic hi- or triph8l!ic
ftynchronou' ~harp-wB"~ comple>cel, AKA periodic IIpike., AKA p8f!udoperiodjc
.llarp·Wljve comple>Ce1 (0.~·2 per ile<"Ond) h9Y .. ~ 70% lIefIeitivi ty and 66%
a pedticilyM. They r_mble PL6Ds h "'l' page 145), hut /Ire r elponll!v,,- to no>ctou .
atimulUI (may be ahBent In familial CJD" /lnd in the recent UK variant (""e
«bow»
-
S PECT scan! may be abnormal in vCJD even when EEG i.8 normal". howllver
the findings a~ nolspecifie for vCJD
b r aill blapay: see tk-Iow
tan.mar biop.y: patianUl with variant CJD (vCJO) tUay haVil dete<:t.able le vel.
of variant type ~ of th e ahnormal prion protein {Pr pS<} in th e:. r lymphoreticuillt
!yatem, which may be accused by a 1 tm wedge-hiolMY oron~ palaline tonlil (uaing ca refu l aseptie precautions )""
Brain biopsy
Due to lacio.ofan efT""tiy~ treatmMland thepoll!l.Itilil for jatrog~nic infection in aurgery. biopsy is ltie,.".ed for c,: nea where estabH9hi "g Ille dillgna,us iJ dHmrd ;mpo~nt,
or lIB part ofa Teiiearch stu dy". or when diaJllostic testa are equi .... ocal and other pole·n ·
tially In'atable etiologies aresWipec:ted.
T rea tment a n d prognosis
Given the lack ofden>On5trated infectivity (with t;",uell other ttlan brain or CSF),
ISolation P/"l!C8ul.iOM 1UI'1l Wi gowns or moskll ace felt to be unnecess.o.ya.
There i, no known t reatJ:nenL Th~ disease;$ rapidly prog:reulve. Median su""';"al
is 5 months, ""d 80% of patients with sporndic CJO die within 1 y".. r ofdiaKJIDsis'".
12.1 1.
Neurologic manifestations of AIDS
TYPES OF NEUROLOGIC INVOLVEMENT
~0-60"" cfall patil.'nl.3 wi th Il<'qulred lmmunode.ficieney IyDcittlme (AIDS) will dt.
v.. lop ue urologic 8)'I1lptn(lll, ",ilh one third ofth_ presenting initially with th eir neurologiccD"'plainl"'·"'. Only ~ 5% cf\l3 tienb Ibat di e with AIDS hav", , no ..... al brain on
autojN>y . One study found th e CNS complication. of AIDS ahown in Tobie 12- 15.
The most common condi:io n~ producingbl C NS 185;0115 in
L tOlCopluP1osiB
2 . primary eNS lymphoma
3. progT\';I$jve muJlif_ lleukoeneephalopethy (PML)
'"
12. Infect iona
AIDS"':
NEUROSURGERY
4. cryptococcal abscess
Ii
Manifes ta tio ns of CNS tOl:opla s m osis
Ii
mass lesion (toJ:opi/lSmosis abscess): the
moslcommotllfl.'l ion ca using masseITect in
AI DS pa t ients nO·8O%of cerebral mass I.,..
sions in AIDS") (s et ~Iow for CT/M RI
findings)
2. meningoencephali t is
3. ence phalopathy
I.
CNS klxoplasmosi, occurs latt! in the course
of Ii TV infection. usually when CD4 counts are
<: 200 cells/mm'.
Primary eNS lymphoma (PCNSL)
Occurs in ~ 10'l0 of patients with AiDS".
PCNSL is aasociated with the Epstein.Bsrr vi ruB
Is« P"8t 462).
Features of PML
1.
caused by II ubiquitous polyomllvirus (II
subgroup of papova vinIll, small 'IOnenvel.
oped viruses with a closed ci rcular double
DNA·stranded genome) called "J C virusAo
(J Cv). 60-$0% of adults hav" an~ibodies to
JCY"
frequently manifests in patients with sup·
preS!!ed immune systems, induding
A. AI DS: currently the mos~ common
underlying disease associate<! with
PML
8. prior to AI DS. the most COmmOn as·
sociated diseases were ch ronic lym·
phocytic leukemia & Iympboma
C. allogr-aft recipients: dUl.' to
imm\.lIl08uppresaionl'O
D. chronic ~te roid therapy
E. PML al$Ooccurs with other malig·
nancies, aDd with auklimmune disorde ... (e.g. SLE)
CMV .1IQIIP.... fI\is oocasiona~ OOCUII
3. pathologic findings: focal myeJinlo!S$ (de.......'.c. fIt _ al .... OIIhe _ _
mye liDation . .". affect.8 white matte r) with
oj PML In AIDS: 4'11.
sparing of AXOn cylinders, aurrounded by
enlarged astrocytes and bizarre oligoden.
drogHal cells wilh eosinophilic intranuclear inclusion bodies. E M can detect the
virus . Sometimes occurs in brainstem and cerebellum
clinical findings : menta l stalu. cbanges, bH"dness. aphasia, progressive cranial
nerve. motor, or sensory deficits and ultimately coma. Saitures are rllre
5. dinicaJ cou"",: usually rapidly progreasive to death within a few month, <>cca. ;o" .. lIy 100\jj'" .urvival """,,UI"II inexplicably"'. The .... i. no GITOK:tiva t ... atm.mt.
Some promise initio.JJy with anti-retroviral thernpyS"
6. defini tive diaguosis requires brain biopsy (senaitiv;ty: 40·96%) although it is in·
frequently employed. JCV has been isolated from brain and urine. Polymerase
chain reaction (PC R) of JCV DNA from CSF habet'" reported, and iaspecifi( but
not sensitive for P ML
••
Prim a ry effec ts of AIDS infection
Neurologic involvement with infection with the Human Immunodeficiency Virus
(aside from opportunistic i" rection and tumors caUlled by the immunodeficient
statAl) includes:
I. AIDS enceph alopathy : the most common neurologic involvement, occu", in
~ 66% ofpa~ients with AI DS involving the CNS
(HrY)
\0'"
w"
II. otte. Iho Initiol. of 1M patient in who", it
r. ...1 di.."....t"td. not
""nfused wi'" Jo.kobC..... IZ ~ ldt ( 1 prion d, .....,) nO. wi.., J . ",u taw" Caoyon >i",. (.Iao Olnfu.ill&ly •• II.d JC vi .... )
II .. nKI~ · . t ....dod R!>IA oi",. \hIt ll<."CloionlUy d __ <'>«PMIi,;. in ~um .... )
NEUROSURGERY
12. Infections
'"
2. AIDS demen t ia AKA Hrv dementia compleK
3. aseptic meningitis
4. cranial neuropathies: indudi ng "Bell's palsy" (occasianally bilat.eral)
~. AIDS relat.ed myelopathy: vacua!ization ofe pinal cord (S~ M~lofXJlhy, page 902)
6. peripheral neuropathiu
Neurosyphilis
AIDS patienta can develop neurosyphilis as littlella 4 mOIl tTora infection"(unlike
tbe 1~ ·20 )'MIlisually required in non-imruunocompromised pelienta)
2. neurosyphilis can devel\lp in spite \If what W<Iuld \Itherwise be adequate treatment for early syphilis with benzathine PCN .....
3. the CDC recommend s treating patien~ having symptomatic ar asymptomatic
neurosyphilis for at le ... t 10 days with probene.:id 5-00 mg PO QID plus either
aqueous crystaUin.e PCN-G, 2.4_miltion units IV It 4 h", (tol.al of 12.24_million
uniwd), Or aqueous procaine PCN·G 2.4-mil1ion units [M q d. This 10 day rogimen should be followed by benzathine PCN 2.4·million units 1M q week II" 3
week.. . Benzathine PCN iIIl:iQI recommended initially""
1.
NEURORADIOLOG1 C FINDINGS IN AIDS
A series of200 cansecutive AIDS pa tients" with neurologic symptoms followed to
biopsy, auUlpsy, Or for 2 yrs .howed the following on inilllI..l CI':
• 81 patienta (40%) had initially normal CT. only 5% of which wen t on Ul develop
progression of neurologic abnormalities Or developed or abnormalities
75 patien ts (38%) sbowed only diffuse cerobral atrophy; 5 of these subsequently
developed focal OT findings fihown to be TO%opiasrna Bandii infection
44 patient!! (22%) had ", I focal lesion
See Tablf 12·16 for a compar·
ison Gf neuroradiologic findinp in
Ulxopla$ffiQSis, PCNSL and PML.
Tabla 12-16 Comparl 8Ofl 01 nauroradlolog lc Ie-s lons
AIDS'
'n
CTIMRI findings in t oxopl a s-
-r.
m a a b s ce8li
l. most cOmmOn findings :
large area (low density On
CT) with mild Ul made,ate
edema, ring eManCerT.ent
with rv con trast in 68"competible with abscess (of
tb~e tbat did not rioi en·
hance. many showed ~.ypo­
denae areas with less mus
effed with slight enhollCl!'
a(lb,""'a!lons: Ttm) ~ lO>CapIa.rnosI$. PCNS!. a primary
meM adj9C1!nt to lesion),
eNS !ympI\orna, PMl • P/OQ,8$Si-.. rn.J1~loc8llMlkoen·
well circumscribed
margins"
2. most commonly located in
ballo! S3n"lia. are al80 o(l.e ... . ubcortical
3. onen multiple (typically> 5 lesions") and bilateral
4. usually with little to moderate mass effect" (in BG, may compress third ventride
and sylvian aqueduct ~ausing obstructive hydrocepbalu s)
5. most patient!! with taxoplasmosis had evidence of cerebral otrophy
-"".,
CfIMRI findings in PML (ue Tabl~ 12· 16)
Note: ilie appearance of PML may differ in AIDS petienta from non-AIDS patients.
l. CT: diffuse areas oCIO".... density. MR I: bigh intensity on T2WI
2. normally inV\llvu onlJ' white matter (spares cortex). however in AIDS patient!!
gray matter involveJ1)l!nt hu bef!n reported
3. no enhancemen t (on either CT or MRI). unlike most toxoplaSlT\QlIis lesions
4. nornasseffect
5. no edema
6. lesions may be solitary On 36% ofOT. and on 13% of MRla
7. borders are usually mOre ill·defined iliaD in Ul~oplasmosis"'
12. Infections
NEUROSURGERY
CTIMRI findings in primary eNS lymphoma (PCNSL) (see To.bls 12·16)
NB: the a ppearance ofPCNSL may ditre. in AJOS patientli from nOl\-AJOS pal;tinu.
muillp le Issians with mild mus effect and edema that tend ~ rinK·enhan~ on
CT, 0. appear a~ a~as ofhypoiotensily urroun<;linlI .:ent.,,1 Hrea of high int.-naily
\largelle,ion) l.II.geu. onT2Wl MRI (unlike non-AIDS CIlllea whieh tend to en·
hanee homogeneol,l.lllyttl
2. the re 15 a greater tendency to nlul tic.. ntricity mAI DS patients than in the non·
immun oauppreasOO population ll'
1.
Imaging fil<:ommendation s
MR with gadolinium ill recommended .. the initial.creeni"g prooedure ofchoire for
AIDS pa tients with eNS "ympl.O"'1I (low~r fal!!e oegativ~ fII te \han
cr-\.
MANAGEMENT OF INTRACERE8RAL LESIONS
NeW'Olluriioal confiuiUltion it ofuon ''''lue5t.ed for biopjly in lin AIDS patient Wllh
'1u .... tionable luian(B). Tbs di~gnoslicdilem ma ill ... ually for low den!lity lesions on CT,
and in tire United Stale!! is primarily between the following:
toxopla.mOlltlr : treated with pyrimetha mine IUId 5ulfadioline(_ ~Iow)
PML: nO provon efTecti"" t~atment(anlilllt roviral the."py may helpl" l
eNS lymphoma: u~ lIally treatold with RTX (lIft-eNS lymphomtJ, page 4'61 )
1'8: tends ~ be unlikelY ucept in HaitiRD popUlation
note:: cryptoc:QCcI1S l'lno~ common tha.n P/IIL or lymphoma, but uluallY mani·
rut.! as ~rypt.oeo<:cal menjngiti~ ta nd Ml. U. ~bIa4tinr lesion}!",e p(Jge 239)
RECOMMEND.... TIONS
PML co n usually bE identified rodiogrophically. How .... er , :radiognophic imaging
alone ClInnot reliably different iate toxOpll1Sm06Ur from IYOlpflOm, o. from lOme other ~on'
t urrent condit ions (pa,tienUr with toxoplasmosis may hav. otber ,ill1 ultllneou~ dinA"'s),
Th erefore, Ihe foUuwing :r~c"'nm~ud"tiona are mads:
) , obtain b&llelin" toxoplasmo.ei s titera 00 all known AIDS patien~ i NS: :>O% oflhe.
ge nera! popu latiWl have been inrKted by 1.00;0 and b.lve poI!itive tilers by ilge 6
yean, 80·9!l"7t ""iIl be positive \;Iy middle adulthood) . 7hechaneea-of to>eo Ilrehigh.
er with seru m anUbodil'!l > 1:IGH (most are> !:258)
2. mUltiph! enlllillcingleaiun5 with baaai ganglion involvClment in a patien t Wh081!
\.nxo t\tenr eh ang~ fn)m negative to poaitive have II high pr<lbability or being '""n
3, primary eNS l)'Jllphoma (P CNS L )
A. with line.II: les ioTll, 1)'I\'Iphoma ill mONilikely than taxo
S . if pnll~ibiUty or PCNSL i, strong
I . couzilier LP (contrAindicated In prellf!nce of man effectl
•. high volume LP ro r cytology: PCNSL ClI n be d iagnbae<l in . 1025% of cases using . 10 OIl of CSF ifee f"06'" 463 for more details)
b. or send cs r for polymenl~ch.ln reaction (p e R) amplification
of viral DNA ofEp.gtein·Barr virus orJC·rirus'·' ithe age ots re"pon~lble for AIDS-related PCNSL and PML, reapeetively/
2. 50merecommend ear ly bioPByA ta identi ty PCNS L ca_ \.0 avuid deIByinr:: RTX for 3 weelus whilBllSIIe$Sinll ,..u""nRa to antibiotica'"
.. in p"u.." t .. lth p ... aible t.oxopl ... ml>&;~Ii. e. pOIIitive.tol<o titenand CT findlnr~ no~
atypica l ror \.0><0) even If other cxmditionl ha~e not been excluded:
A. empirically SUitt: pyrimetl:HlJl)iOe Waraprim®) (200 mg 1000ding dose, theu
75·100 mg/d ), sulfRdinine (75 mglkg PO loading tOile, then 25 mglk, q 6
hrs), fol k add (5-40 Ing/d, t>9U~Uy l O mg with nch da-.e of pyrime thamine)
B. if lulra a ll~'1O' dev~lops (which eommon ly occur'll). chMlge $ul(adiaO<ine to
cli nd amicir, 400-600 mg PO or 600 mg IV q 6 hni
C. a l~mativell for complete intoJu11nce:
I. lIpirllmy<:in ( Rovamycin~J S-4 gmsId (ped~: ~O'IOO mglkg/d 1l 3 ... ,..k&)
2. etovH'l UOne
O. Ule~ahould be B dinkal end radiognlphic respo!1W wi thi n 2-3 weeQ,n
E. irresponw 1¥ good, reducedoaRge afte r 6- 12 weeksto50% ..rthe abovedoaea
and maintain fl)1' Uk
F. if th~~ drugs are cont.inue<:l, it should bepo.nible to maintain control rOT re--
NEUROSURGERY
12. 1"(Kuons
mainder of patient's li fe «(u re ill not generally possible)
G. ifno response to the ra py a lterS w....k$ (80me remmmend 7· IOdays'''), then
conSider biopsy'
S. perform biopay in the following settings:
A. in patient with negative toKOtiters (note: patienl.8 oecaSlonaJly have nega·
tive titers because of anergy)
B. accessible lesion(s) atypical for toKO (i.e. non-tlnhancing. aparing basal gan_
glia, periventricular location)
C. in the presen~ of extra neura.l infections or malignancies tha t mllY involve
the CNS
D. lesion tha t <:ouid be eithe r lymphoma or toxo (e.g. single le$ion. _3. A. )
E. in patients who have lesions not inconsistent with toKO but fail to respond
to appropriate II nti· toxo medications in the recommendd time (_ a/JoLr«)
F. the role ofbiapsy for Mll.:e ohancinf,llesions is less well defined ae the diago06is does not influence therapy (mO$t are PM L or biopsies are non-diagn06tic). it may be useful only for prognostic purposes'"
G. oote: the risk of open biopsy in A.lOO patieol.8 may be higher than non·
immunocom promised patients. Stereotactic biopsy may be especially well
suited, with up \.0 96'10 effic.acy. fairly low morbidity (major risk: significant
hemorrhage, w 8% iocidence) and low mortality'oo. '01
6. stereotactic biopsy guidelines:
A. ifmultiple lesions are preaent.(hoose the mostaC<lee.9ible lesion in the least
eloquent brllin a..., a, or the lesion oot respondiog to t reatme nt
B. biopsy thecenterofnon·enhancing lesions. or the enhancing portion of ringenhancing lesions
C. recommended studies on biopsy: histology; immunoperoll..idase stain for
Toxop/(lIIma gondii; stains for TB and fungus; (ulture for TB. fungi, pyogens
PROGNOS IS
Patients wit h CNS toxo have a median survival of 446 days, whiclJ is similar tothat
with PML but longer than AI DS-related PCNSV'. Patients with eNS lymphoma in
AIDS urvive on averllge a shorter time than similarly t reated CNS lymphomll in non·
immun()Suppressed patients (S months VB. IS.5 mos). Median survival is < I month with
no treatment. CNS lymphoma in A.lOO tends to OCCUr late in t he disease, and patients
olten die of unrelated causes (e.g. Pneumocyslu carinii pneumonia)"'.
12.12.
Lyme disease ~ neurologic manifestations
Lyme diseue ( lJ) ) is a complex multisystem disease caused by various species of
Borrelia spirochetes (io North Americ.a: Bar~/ia bU'1ldDlferi) tranllmitted t.o humans by
the tJCC<ks scapu/ari$ or pacifo;us ticks (the Americsn dog tic k is not involved). It W8l!l
fi rst ~gni~ed in Lyme, Connecticu t in 1975, lind i$ nOw the most CommOn arth ropodborne infection in the U.S"OI.
C LINICAL FINDINGS
The..., s..., S clinical stages wlmh can averlap oroe<:ur sepa rately.
Stage 1 (early localized d isease, erythe ma migrans and nu·li ke Illness)
Systemic signsofinfection usuaUy begin with a flu_like illnen withio days w weeks
ofinfettion, sympwms indude: fever, chills, malaise, fatigue Or lethargy, backa.c:he, head·
ache. arthralgia, and myalgia. Regional or genernliwd lymphadenopathy may occur.
The hallmark ofLD is erythema c bJ"on;eum .... Igl-ana (ECM) (classically II "bullseye ra8h~) which begin! 3·S0 days slter the tick bite, and <>CCurll in 60·75'10 of patients.
EC M usually begins in the thigh, inguina! region, or axilla. lind consi~ b: ofan e"panding
macular rash with bright...,d borden and central dearing aod induration that usually
flldes without ~arTing in S·4 w~ks. Within 30 days of the tick bite, spi rochetes may be
demonstrated in a.c:eUu lar spinal fluid.
Stage 2 (early d isseminated disease)
Several weeks w months alter infection. untreated patienta develop more serious or12. Infections
NEUROSURGERY
gan involvement. Cardiac and neurologk involvement IIl.,- oc:rur. M3nj("~ttllion5 in_
dude :
I . cnrdiac: oe<:urs in 8~. Conduc lion deftl':'ts (ususlly A-V blocll. ,renerally brief and
mild) and Ol.,YOperiClirditi~
2. Mu lar: panopbtbal",i~is. i""h"",ic optic atrophy, and inte",titial kerntitis OCcur
rarely
3_ neurologic: OCcurS in 10-1$" ofpahents with atag" 2 dise ...&
A. the clinical triad Clf neurologic mlInife.stationa of Lyme diseaae i~ 'Qof:
• cT>lnilil n"urWI (especilllly thpt mi",jelLing Bell'. ""IllY: Lyme diaell""
is the mOSI common cause ofbi I8tunl ·Be Il'~ pal,y " in endemic areaa)
meningilis
radiculopathy
B. other po!l.!libl" neU{ologic involvement includes: encephaliti,. mye litis. pt>ripherol niul';t1.
Neurlliogic findlnp are frequ~nll, migratllry, and _ 60% IIfpat illfll.l have multiple
neurologic [email protected]. In Europe. 81llUlwlOrth', 6yndNwe (chroruc Iymphocytk meningili., peripharpl neuropalhy, and rodiculopillhy) is tbe Il)0l<1 common
m ~nifelltotillo. o'ld primarily affecUl th l< periphenl nervou~ aYlle,o' •. Ne uroiogieaympJ.omll usually ""'lIlve gradually.
Shlge S (late d iseaae)
Anhriti~ and chro~ ic neurologicsyndrOIll<!' "'~y ~ur i" thiH etage. Arthralgia.. are
COm mOn in 813ge I, bul trullarlhn·'i8 Ulmllily doe .. nllt begin for mon/.h lo yealll" after in·
fection, lind i8 S""n in _ ~ o(n.._ '''. When arthritia O«UnI. it may affect the kDee
(89%), hip (9'JI». shou lder (9'1o),lInld~ (7%)an<llor elbow l2'Xo) '" Neurolob"C involveme nt
indudHl""
L cnrephll.lopathl'
2. enccphalomyelili"'"
3. pen pheral neurCopath,..
4 . lI13xla
5. dementia
6. sleep dillorder
7. n euTOlllIyeh iatric d isease and fatigull syndromes
DIAGNOSIS
There i, no leSl indicative of aClive
in faction . The $pl r~hele i~ dimeult to
culture from iufecled human s . DiagnOllil
.. eel$)' if a hiRJ.ory of travel to endem ic
a n""" tick bile, e nd EC M a re identilil.'d .
Thblf 12· 17 sllowl the CDC cri teria for
chegnosi s.
Table 12-17
d lagno,ls
oj
"
Serology
It take.. 7- 10 da}'1 Fram mitial infee..
to develnp alltibodies lo B. burgdor.
hut it lakes _ 2·3 wlul before
IInt.!bodiel elln reliably bedetuted in un·
•...,0 ..." potien!.lo ("'libi~ti ... ~n reduc ..
(FA . Immuno/l"",_ antibody
the iromWle rl!llponu.!"". If the lif'llt ae·
,",un le8t is negative, it s hould boo repeat."""'" fn<dOJlosliolle:at. fI&UtI)Iogie 01 ce«lt.<:
ed in 4_6 ween if the clialeal tuspldon of
LD ia I lrong (seTOC<lnvers;on from ncg~ live til pIIsitive is lIupport;ve of B. bU'7ldor(eri infection). "'alse pCIBitivl)l! tan occur with
oilier borreli.1 and trPponemallnfectionll (e.g . ..yphilis, however, VORL lest will differentil~ the twol.
Enzyme-linked iromunosorbenl eBllay (£LISA) del.ettll fgM or IgG. Antibodi"" loB.
bU'7ldorf~r;' iathe u~uBI l:e!!tmethod . lgM illelevnted Bcutely, and!gG ~du ..Uy rile. a.od
il elevated in almO!lt 1111 petients Ilt 4-6 weekB and if UIIual!y !tighe'lt in plI tlenta with
&rthriti9'oo. Western blo't !lIpy help identify fai:Je..polIiUve ELlSA re~ult.s (more .ll(!ruriuve
and Jpe<:ifie than ELISA, however, l"I!IIulta may vary betwe.!!n labs). Amplification B.
tmrlJdorf~ri DNA by pol)'TllerlOS8 thain ruction (PCR) yjeld~ a more very I18n~ilive test
~iOll
r~rl,
or
NEUROSURGERY
12.
I nfed;on~
lhIIt may Mvttaicnilicant faloe
dud organisml.
polIiti~es.
and can be poeitive even if th e DNA is from
CSF
Elevated CSP IgO antibody liter. to 8 . burgdorfui may Ottur with neurologic
invol"'rt>eflt'''. CSF findinll in lat41 dioe..e are usually wmpatible .... illl aseptic meninriu" OIit«lon,1 band, and increased ratio of IsO to albumin may occur''''.
TREATMENT m.'" 'If
Antibiotic therapy i, more effective early in !be illne...
12.13.
Parasitic infections of the eNS
Th .. followinl it a list of lOme of the many p.o.raaitk infectiolll that involve the neTyousayitero. Thoae that poteotillity invol~e neurosurgical int41rvention have _ daggerCf).
1. cysti«rcosi.,: lee Nfu'WY'lk~rr:o.i. below
2. toxoplu roOllist : msy Ottu r .. , ronlen;t,1 TORCH infection. or in t.he adult u.su.lIy with AIDS (1M NfuroloRk mani(ufC.tion. 0( AiDS. pal" 230). Toroplcuma
gond;; i. an oblilate int racellul. r proto_n thtt il ubiquitous butdoe. ooteau"
c1inkal infection except in immunocompromiaed hOllt41. Histologic feature.: necro.i, containinl2-3 run tachyz.oitelllcytblll
3. echi nocoo:cust: He pogt 238
<I. amebiasi.t
5. ..,histoeQmi.. i,
I poruitk inf«tion. "Lib. d""~r .... t"-Ib.' .... _ ... lihl,IOU. ....1ve .. U/WU.tIkaI.ueolioa
N EUROCYSTICERCOSIS
CysticerCOollis is the mwt wmmon parasitic infection involvinl the CNS"'_It ;'
caused by C,,'iotrcu, ctUuw-. the larv, I . t.age of the pork t,,,,,wonn TClfn", fOlium,
which has a marked predilection for neW'al tiuue. Cyaliceroosi. iI endemic in atu. 01
Me!<ico. Eastern Europe. Asia. Central.nd Sou\.b Ameriea. MIl Mric • • The incidence of
oeu.rocysticercosis(enCYltmento(]arva in the brain) rosy rncb ,,'lit in lOme are..'''. The
incubation period varies between monllu! to tiecadea, but 83'9lo of o:aae. ahow . ympto ....
within 7 yeanl ofuposure.
LiFE CYCLE OF
T.
sotlUM
'nlere are 3 stages to the life cycle: 1...... (or onoosphere), embryo.nd adulL. T. MIlium can infect m.n in two different way.: .. the adult worm or 81 the larva.
Infect ion with the a duJt worm (para!lit ie infeetion)
TIll' type of infection results from etting undercooked infes ted (meuly) pork. The
e~ted embryo it rel<!'ued in the . mall bow..!.nd can then rosture into an _dulL "..
~groented adult worm attaches by meanloflo ..... auckera and two I'Owlofhookleu to the
.... all of the .mall in~ltine wht:re it absorbs food directly throuKb il>! cuticle. Man i. the
only known perm.n,nt hoel for the adult t.lpewonn. for which ihe human GJ Inct iI the
.ole hl bit.lL Proglotu.a {Ol.ture aegmenta. each cont.t.ining repn>ductive organ.) produce tIP which are liberaUy eJU:reted in the feon.
Infeetion with the larva
00:::"'"
".. dileaH ~~
wheo _nimala or humana become an iOUlnuediate
oo.t for the larval.tage by ;"&aU", viable un produced by the proglottid. In the
dL>Odenum of man alld pil, the Ibell of \.be ov. diuolves and the thu.sly hitched larvae
burrow throop th. Im,lI bowel Will to enler thl lyD'\phatics Or .y.lemiccin,:ulation and
lain aeee.. to:
brain: atiro.ted to be involved in 60-92% ofcaset of CYBticel'COllis
.kelettl mu.de
.,.
' Uhcutaneoul tiMue
The IlIOIIt roromon routeJ ofinplltion ofviable egp I re :
1. food (Ulually veletablea) Or water contaminated with egp from human f/!Ceil
12. Infection.
NEUROSURGERY
f<l<8I.o,.1 autoinoculation LU a n indiyidual ha. baring th~ adult ronu 0( tile tapeworm due 10 l.~k orgood unitary habits Or facilities
aUlOlnfection by re~nt penatalait of grllvid prolllo!tiw. from the inteitlRe into
the ltomllch (a theore!i"i pO!I~ib; lity IhM is unproven)
2
3
OnOll In the ti&aueofthe iotlitrmedilll')' hOllt. Ibe Ill/"Ya
d~velop
I cyst waU in
~ :2
mrmU., and miliUM. in _ " month. to lin embryo . Many 6Dlbl'}'Oll d •• wi thin 5-7 yno , the~
somelilM!! caldfy. ln
th~ emhryo.li .. dunnoll! in the mu..cJe, ·wailing'" to be eatet\
af't40r 'l'hich tbe tyde repHts.
pra..
TYPEs OF NEUROLOGIC INVOlVEMENT
Involvemen t of thlapinal cord and periphenl "uYel ie rare.
"""0 type. of CYlts tend to develop in the br. in''":
I eyati". rc:uI cel lule •• e: ~l\Illir. round or ova.llhi/l·wa]~ cyst, flU>Ilnl in "Ie
from . 3 to ZQ m.m tel.<lioK to fonu.o th" pH renchyma or nll'f'OW , ubA rllchnoid
.,,0;1
2.
I paNS. Thb cY'! OXInlalnl \I loo leJl; (h"d), il u. uall)r .ta~,
prod1.>Cfll only
mild iunllmmlltion durin, t be active ph. .e
cyat'lle r cua nllclt1,,~ua: larcer (4- 12 em), ~W. aetivoely prodlM:;ne g-r.pe-lik"
duster. in tho! banl . ub.rachuoid 'P"~ Ind produc.. 'nte" .e innammltion,
Ther<!! are no lar-..uin tlludqs\&, 'l'heKCYIIII u. uaUy dq:ene rate in 2-!1 yea"" ill
which the ClIpsule thiekeu. alld thl elear
eonte"ta are 11191.0. by. whitllh
~I which unde'l:~ calcium depo$W<In with «InCOmitanlsh.rinJo:ap of the c,..t
,,.t
l.ocation ofth ... cy,\& te"d$ to fall in to \ of 4 JITOUpl:
\, meni"e.al: {ou.d U! 27-!I6~ofta.ea with n ... ur~1 InvOlvmlenL Cy.tI.r. .dhl""nl
or {r""noat;ne and are Iocatad ei ther tn.:
• dorlQlat<emJ auN.rtlthnoid If»I~ u8ually C RUIII""'r type, uull"l mini ,
mal.ymplomt
• ba!.llubarachnQ,d apa", : u.uBlly the e apa"dint C norm"'u, (0= prO.
ducLng arachnoiditis and libro&i, eompl1llin, a d..-ouic nlenln,itia with hypoglYCOrThachia. Can obstntct foram",a ofLuachka and Ma,HMi,e
p.ooucin, h~phal u. , or ean c:lu.e enlnlpment of ball I e""'rna- cra·
nial neuro;»<thie. (including visual rlisturb.nc::ej. EIlnmely high mortahty
with this bnn
2, ""re nchym.l: found ieo 3(1.63-.; focal or general''f<!d ... i-w.urs O«u"' in ~ 50'10 of
tMH (up to 92\10 in IhHIIfIleried
3 , ventricular: found in 12.!8"J-, poIIibly lIaini", aecea ,-iii IhI! eh oroid plel<ut. ....
dIlIKIII.~ O!" frw I1GBt;n, cysts occur, c:I" block CS F flow and r.UM. bydroo!ph.
ah.. w,th intenailtent ;ntraeranial hyperten.ion {8nu.'• ..,ndromd
4. mixed lesioo.: fGund in _ 2~
CLINICAL
Pre5el.tation:aeiZllre., ~ign.o ofel~.ted ICP.1'ocaJ defidb related to the lcabon or
tll a <:).. t, Ind alte," m! IItal .tatul a re tbe!DOel tllrl)lOOn find ,np . SymplDma lillY'''''
be prodo..ooed by the imu, ullologic tHet;on to the ;Ilreatation. Cracial nerve paltiet can 00wr with basallracbno,dit is, Subc:utan~ nodul... may 10mHimH be fell.
LtBoRATORY EVALUATION
Mikl periphenJ _inophilia CIOn o<cur. but i. incoosis tent and thu s wlf~1iabl ....
CSY may be IIGrfOlll. t:o.ioophiLI are IftIO in 12-~orClUet and ,uaf:llt. po .... itic
i,,{mion , Pn:I~n may be flevDud.
StoGl: !eM Ihln 33"1tof ClIMI bIIve T toI'um OVII on the ltoI)l
& rology
CYlliten:oai. IlIlliborly lite ... delenwDII!'d by I::USA Ire ~ 1I.idered . ignltltant.t1'601 in lerum , and 1'8 <II the CRF; checki n, (or tite ... ..... ~ir_' thP!ll! lhnlllhold& in the
auum prodU~I' tal \hI t i. ltIClte Mllsihve and >II the CS F ill nlCll'e specH;" for cy5tia;r.
co.iI, FI'" lI.,auve rata Ira hither In case. without nwningit:il 0. with leu sentitive
IUU, Tha "",wer flUyme-linJo:ed im munoell'Ctrvtranaftlr blot i. _ 100'10 lpeci fic and hiKt.ly
alLboulh MI\I.ti ¥lt)' il l..- in eaMI with a "'lita!')' (:)'lIt,
se.,.iuve"·,
R.4OcGAAPl-/IC EVALIJATK»I
Sol\..tip"l .......,. mllY . how .,.ldfit.ltJ,gnt In lUbc:utllroeoU1 n«lulu. a nd in thigh
and lbou lde r muadH,
S hlll · rn' tbow caleifieationa iu 1 3' 1 ~ of ellllea with """urOl.")'~tiCl!r<:OI!is. May be
NEUROSUHGERY
12. lnft'Ctiolil
linille or multiple . Ut uaUy ein:ular or oval in ,hllpe.
cr
The follo .... inll findings on C'f' bave been defUibed (modified' ''' "' J:
I. rio, arthanein, cytUl of veriou t t izea representin, livu., cystiee",i. Little inflam·
mateT)' fe.ponae(edemal occurs IS lon, IS I. tve i, alive. C her. ct.criatic findin, it
sm,ll (e 2.5 em) low detllity cyaUl with eccentric punctate high density that may
represent tbe Beolel(
2. low den t ity .... ith ring eohancement.een as an int.crTl.>elfiate l tage between living
cylt end e.leified ranUlant rl!pn!8entu.g int.rmedi. t. l tage in granuloma forml.
UOIl . Resultant inflammateT)' readion can c.ule edeme. Ind b n l arachnoiditis
u. cyat$ loca ted in hull suba rachnoid apace . Onen rin, I nh.ndn,
3. intraparenchYll'lal punctatol CIIldficationt (graouloml ) IOmetimel .... ith. but u. ually without l urroWlding eohancemonl. leen with dead par.litel
4. hydrOOllphalu l . Sometimes with intraventricular cYl ll which mtly bl ilcM tense
with CSF on plain CT'" and may requirecontru t CTvl ntricu:'l phy'" or MRI
to be demonurated
TREATMENT
S teroidll
May temporarily relieve ~YlI'lptoma. and may help dec:reue edeme th.t tend. to (IC.
cur initially during treatment with antihelminlic drugs (I., . delUllmeUuuor>e 16 mgld iniofacute
tially, lubsequeot.ly tapered'- ,. Steroids .hould probably be reserved for _
deterioration during therapy' ''.
Anlibelmintic drugs
CoruC06teroids should be u$Bd (if poasible •• tart 2-3 d befOl"ll! treatment., continue
during therapy). Any c)'llticen:oc:idal dn.>g may caUBfl irreversibl.. danage whe-n \11M to
treat ocular or spinal CYl ta, even with corticosteroid \1M.
PraziquanU!1 (Biltricide®) il an IltItihelmintic with ac:tivity agai ... t.U known species ofsc:hi9lO3om ..... Given .... 50 mgftg divided in 3 doees (.. """ (\oft. for pediatri ... ) for
15 daYI . (.here ia a l ignificant reductioo in Bymptom. and in number ofty.ta seen on
CT' ''. Also dn.>, ofchoioe fo r intntio.al.tage infestation.
.
A1bendazole (Zenl@latI) 15 mglkg per day divided in 2·3 dOBeS, taken with a (Itty
meal to enhance absorption (.am .. dose ror pediatrics). given ror 3 month . ... "I"!.
Niclosamide (NiclocidelS.nd others) may be given orally to trea~ adult tapewOnn.l
in the Gl tract (not@: pruiquantel is drug ofchoieel. R.x I gro (2 tableta) chewed PO . ...
peated io I hour (total ~ 2 gm;.
Intra ve ntricular disease: The,e is no COnHtlluS 00 the efficacy ofmedicall.reallm'nt
for intraventritu lar cysta'·.
5u.rge ry
SufKeT)' may IOmeti "'" be n_
al")' to establish the diagnosi •. Stereotactic biopsy
may be weil l uited for lOme casel. es pecially wilh deep l...iII....
CSF diversion i. nec: ...... ry ror patient.. with ' YlI'lptomatic hydrocephalus. although
tubin, may become obstructed by jp1lnWomltelJ& innammatoT)' d.. b"s....
SurgeT)' mtly be indica ted ror lpinal ."..Ia"· and for intraventricular c)'IIla whim
may be Ie.. respons ive te med ica l therapy. The latter may IIOmItimes be dult with ul in,
ltereotactiC IA!C:hniqufll andlor endoscopic inatrurnentation''' .
Contact.
Both .. uenta with cy. t icercosis end their personal contact.. Ihould be K Tftned for
tapewo rm infection ai~ a l il"l(le d _ ofnidOlllllide or praziquantelwm l liminate the
tapeworm '-. CION conlld.l of persont with tapew(Wml ahou lei h.ve acreerung by medical
hi l toT)' I nd H rologic ~ti.n1I for cy.ticerentis; if lUu " tive of cy.ticercosi, a lI<!urologic
.,UIII and CT or MRI t hould be done.
ECHINOCOCCOSIS
AKA hydal id (cyll ) d ifUM. Ca uHd by Incysted la rv.e ofth l!oc tapeworm &hi·
nococc:u. grntUdOIO in endemic are• • (Uruguay, .... ua tr. li. , New Zea land ... ). The dot!: i.
the prim' ry definiti ve hnIItofilil ad ult won:a . lnterme<liate bolla for the l. rvll.tage in·
clude . heep and ""'0. O¥a are u Crl!ted in dOC f_
and contaminate herbage e.ten by
eheep. After ingatioll , the Im!)T)'OI hatch end the pa11II,i te burrow. through th duoden.l w.ll t<l pin hematoee_ . c:caa to multiple o rg.tII (liver. lunp, heart, bone, blllin).
138
12. lnfectioRf
NEUROSURGERY
Oog:t Nt these infested orgal13 arKI the par8Bite enter! the intestine where it remailUl.
Man it infected ei the r by uting food cont.llm;nll.\.e<! with ova, or hy direct contact
with infected dop. eNS involvement occurs in only ~ 3%. Produces eerehral CYSI8 that
Ire confi ned to the wh ite matter. Primary CfatAa re ulua lly B(lli tary, MC(\nda rycYlto (e.g.
from embo liUltion from (/IO rdi •• Cyl.ll8 that ruptu re or fl"(lm h. t.rogenk Olpture nrcerebral
cylt.t) are uaualty multiple. The CT den.i!), of the cyst illimil8r to CSf', it doea not enhanee (. )though rilo enhancement may oa;:ur lf t bere is an inflammatory Te8Ction), and
there i. litt!e I UlTOundins edema . It cont.ain'lIerminating para sitic particles called "hy.
datid sa nd" eon to ioing _ 400,000 aeoleca.lml. The <:ylt e nlarg<ll slowly (ra tes of _ I em
per YNr a re quoted, but thi. i. variable and may be hiehe r in ch ildren ), and lISual1ydoea
not present until qui te :arge with lindinga ofincreaHd ICP, ae1ZUrH, or focal delicit. Pa!ient.l often have eoI lnQphllia and may have positive serologic teJItl for hydatid disease.
Trea tm en t
TTeatmen t i~ . urg"k.l remova l of the intac!cysl. Every effort mUI! be made to avoid
",pturing these cyst.l d l.lring remova l, or else the fQOl_ may oont.am in ate the a<lj.afltnt
ti guu with ]'I<IQible rtcurrenceof lUultiple cytt.a or allergic rtao;:tion. May uM acijunctive
medical trutment with ~lbenda"lOle (Zentel®) 400 mg PO BID (pediatric dose: l.5
mJo1k&ld ) . 28 dllYl, Ll. ken with a flilty meal. repeated .. nKeEnry'''.
12.14.
Fungal infections of the eNS
Mo. t are moedk~lI~ treated conditiolUl l hat do nO! require neutollurrlcal inte",ention . They tend to pre se nt eit he r wilh chronic meninciti. Of" brain a~••. Some oft...
more com mon onn indude
1. crypw:occosis:.t />l,low
A. cryptococcoma (mucinous pseudocyst)
B. cryptocottal meningitia
2. candidiasil: i. n_the most common fungal infection oft.he eNS, but is rarely diagnosed before .utopay. Very rate in healthy individu...ts
3. aspergillosis! may be IISsociated with cerebral absceu in organ tranlptanl pe.
tient.ll (supagr218)
4. coccidiomycosis: caused by the d imorphic ru ngu$ CoccidWUk. immili • • En~n;lic
in 80uth weBtem U.S •• Muico, and Central Alnerica . U.ually presenta .. meningitis. with rare repo>ta of parenchymallesKlM '"
S. mucormycosis (phycomycoa:is): U5uaUy occura in diabetics ~ ptJgt 586)
CRVP"TOCOCCAL INVOlVEMENT OF THE CNS
CNS involvemeol i. diagnosed more frequenO,y in living patient.ll thin Iny othe r
fungal distill<!. Octura in healthy o r immuoocompromised patient..
1. cryptOCO«:Om. (mucinoua paeudocY5t): a parench}'IN1 cotleetion which 0<:CUf$ al.
n'ost excl ulive\y in AIDS petientl. Noenhancement oflhe ltlion or the meninges.
U.ually3·10 mm in diameter and are frequently located in lhe bQal ganglia(due
to .pread by llIlIIlI penoretotl)
2. cryptocOCClI meningir;':
A. occurs in 4-&1. of pelientl with AIDS""
B. ca n llao o«ur withoul AIDS: IIOlli variety can in~eet the bnlin ofimmunOcompe~nl hottl'"
C. may be auocilted with increaHd ICPiwith or w:thoul hyd rocephalul on
en,deereaaed viaull acuily, andlor cranial nerve deficits
D. I.te dettrio ration it> t.he IbMoc:e ot"documented in feetion may respond 10
deeadron ' IRJ q 6 hf$ tran.itiooed 10 prednieon, 2S mg p.o. q d''''
Tr-eatme n t
1.
2.
antifunlalagenl$ (e.g. flucon awle , In orl.llria.ole or amphotericin B)"·
A. petieOt.l "ith H[V require lifelong trellment
B. non-H [V petienta have aliroited treatmenl COUrN
manapmen t of inlrao;:ranial hypertelUlion UC HT) (with or without hyd roce phalu.): contrOversial. OptiorUJ''"::
A. ifinitial openinl preuure COp) on LP ia WNL Cc 20 cm) Ihen a repelt LP
in 2 weeu ill rc<ommended to ....... cu/lute! llalul . nd to re~vll l OP
NEUROSURGERY
12. InfeetiolUl
'"
B. f(lr doeument..d ICH'f. initifl.! manogement is daily LPs. drain ing enough
CSFIO redu<:e ICPby~. Daily Lf>. may beiuepended when prt'5SUre~ "'"
ncmnaJ for Rverru tOMe~ut.ive dllY'
C. c"aH with p"r~;"'U!nt IC HT Or th""" with visual deteriorat.i<,ln in ~pite ,,[Beriall.J'~ may be ,,:ulnaged .... iUl:
I . lumbar drain: temporizing. Drain 10" height of. 10 em ofCS F
2. ""rmonentahunL: !>eilher di ...... minntion ofinf""Uon tJu-uugh the distal sbullt nOr ~~tion ofa nidus ofinfection ",frndo'1 to m~ical
therapy hlU been deliCribed ""
D. iumbo""ritoneDI shunt
b. VPor VAHh unt'''''·
12.15.
Spine infections
Spine inf~tiol\ll may be divided inlO the following major ClltegOries:
I. Vilrtebral os~myeliti~ ("pondy)iti,l: «f! PIJ6~ 243
A. pyogenic
B. non pyogenic. gt"IUlulornatou,
1. tuberculou •• pondyl;ti!
2. bn",ellO!!is
3. nsper gillOli5
4. \)lut0n'\y005i~
5. c.occidiomycosi.
6. inf""Iion with Cotldida trop;/:aU"
2. discitis : i~ pnge 245. u~ually 1U8odated with vertebral O/iW!olnyeHU. (spon dyiQdiscitis)
A. spontB""" ....
B. polt-ope rat!ywpo l t·proc:edure
3. epidural abscess {fte bi!loml
~ . aubdural empY"1I'B
5. m£ningiti!
6. apinal cord Bfmess
MR)uperi,nce uggeat.lhal pa~ients with in fectinus spon liylitis will dlOVelop an
B850ciu.ted e pidural a~us ifWltreated. and thn epidural empyema i8 u n usuwl ,n the
ahsell«! ofvertebral ost.omyeli lill'''. Thul . Ihe diseovery of one of these ronditions
Ihauld pTalDp t a aea.",h fo r the ot her.
12.15.1.
Spinal epidural abscess
, Key feature.;
should be eon~;dered in "pelieat wi t h back pIIin, fe~er, Rnd 8"pine tendern","
major ri5 k factol1l; diobetell , IV drug abuse. throni~ rena! foil ...... alcoha1iam
mllY pr-odu«! p~.i .. ~ m"jf.!opalb.y. ,ometimes with precipi\DuS det.o.riorotioo.
therefore ellriy su rgery is rt!C<lnunended eye n if 00 neuro deficit
fev .. r,sweat. or rigal1l are common. but norma l WBC IlIId U!n>penUure CIIn OCCUr
dllSJlital pres£ntat ion oh skin boil (furuncle) DCCUI1l in only - IS~
EPIDEMIOLOGY
Incid ente: 0.2-1 .2 per I O.GOOhospital ftdmiesionumnuo liy'''. po~!libly pn the ~'''.
Average age: 57.5:t 16.6 ye;)rs'·'.
Thoracle level ill the mos t commOn site (_ ~). follow~d by lumbar (351'» then .cervical ( 15%)"J, 82')1> ~re pOl:l, rior loUIe cord. and 1$'11> Interiorlnone1tl!ries''', SEA may
span &oro I to 13 levels"' ,
Spinal ,pidurlll abscen (S EAl is ollen u~inted with vertebroJ o$teomyelitis (In
one fl(!riea of40 cases. OIteomyelitis Otturr~ in all cases of anteriar SEA. in 85"" af elT'
cum fe renLial SEA. a nd no CaSl'S or poste rior SEA) and ;nl.ef\Oerl.eb,.,.1 di.<cit is
CO-MORBID CONDITIONS
Chroniedi5easu pssocillted with compromised immunily were identified In 65'1'0 of
12, Infections
NeUROSURGERY
40 ca.u"·. MlOCiated eogdition. ig~luded dill~tet n'ellitua (32\1», IV drug abuae( IS<J,),
chronie ren"l failure 112,-,», alcoholism I I~J, and the following in only 1 or 2 pa.tienta:
cance r, recurrent UTI. Pott', disease, and positivity for HIV . Chronic . teroid use and ~
cent .pinal procedure or trauma (e,g. GSW) a~ . 1110 ri sk factors''',
CliNiCAL F&'TURES
U.u.Uy p~senta with e~eruciating pai n localized over Ipine. tender to percuasion.
RII d icular .ymptoU'll follow with . ubilequent di,tallXlrd findin"" often beginnill( with
oowel/bl.dder diUurbance, abdominal distelllion. weaknns ~"ing to perl· and
quad.ripll!gia . Average tiD'le i.3 d"yl!'roD'l bIIck JIIIin to root . ymptom. ; 4.5 day. from root
pain to weakne ..; 24 h.. from we,lulea. to parapltgia.
Fever. sWUtl Or rigol'l .... eomn>Qn. but .re not alwaY' pretent"'.
A furuncle may be identified in 15%.
Patil!nta D'lay be enoeph,lopathie. Tbi. may range from mild to severe and m.y fur·
ther delay diagn03i •. Meningilmul with . positive Kemig'. lim may occ:ur.
Patientl with posl-operative SEA may demonstrate lurpr .. ingly few ligna Or .ymptoms (i nduding lack or teukocytolis, 1.. offeverJ nide from loul pain''',
*
Pathophysiology o r spinal cord dy.function
Nthough soroe rod l ympt.Oms may be due to mec hanical comp~..ion (i ndudinr
that due to vertebral body eollapse). th i. i. not alWIYl found '''. A vascu lar mech.ni.m
ha s also been postulated. and vanoUi eombination. of arteri.l aDd ~nous pathology
have been described'" (one autopay series . hawed liull! arteri.1 eompromiae, but did
ahow venous compreQi on .nd thrombo. is, thrombophlebiti. of epidural veins. and
venoW! infarction.nd edema of the spinal cord'''). o..:uionally, there m.y be ;n f« l ion
of the spinal eoro itself, possibly by extenlion through Ihe roeIl.iTIIH.
Differen ti al diagnosia
SEA should be con3idered in any patient with b&c:ltache, k;vl!r,lnd .p;n.
tendemeas''', AJso see Diffrrl!fllial di06f1()$js, M~lopalh)' on plge 902.
Differential diagnOllili
I. meningitis
2. acute tra nsveru myel itis (pa ralysis is usually more rapid, radioeraPhioc atudie.
art: nonnal)
3. intervl!rte:bral disc herniation
4 . spin.l cord lumor.
f'>. post-op SEA may appear simi la r to pHudomeningocele'"
SOURCE SITE OF INFECTION
hl!mato(enoul spread is the most common lIOurft ( 2~ of cases) either to the
epidural ' paCl! or to the vertebr8 with extension tol!pidural space. Reponed foc:i
include:
A. akin infections (mOllt common): furonde may be bund m 15'Ao of cases
B. parenters] injections, especi ally with IV dNg .00M'"
C. bIIete:riall!ndoearditis
D. lITl
E. ~.pirat.ory infection (including otitis media. 'muaitis, Or pneumoni.)
F. pharyniNl or deotal ab",,",
direct extellIion from.:
A. decubitua ulcl!r
B. psoa' abloe.n: peoas O1ajor muacle .ttaches to ttan.verse PrDCelSeJ. ~rle­
bral bodieJ (VB) . nd in tl!rvl!rtebral diaQ ofapinalcolwnn .tartingfrom the
inferior m.rgin ofTl2 VB, e~tendill( to the uppe~ pa rt of 1.5 VB
C. peoel ratinr t rauma, including: abdominll wound., neck wound., GSW
D. pllllrynre.1 in fectiont
E. mediastinitis
F, pyeloneph:itls with perinephric abKeQ
followi", . pin al ~uru (3 ore ofthne pIltitnta h.d readily identified perio·
perative infectiQIlI of periodonta, UTI, or AV. r;, tula ''')
A. open prootduru: Hpecially lumbll r diIotetomy linc:idl!no:e'" _ 0.67'1»
B, t:loeed prooedU'H: e.g. epidural catheter inae rtion for 'pin al epidural
anesthesi."'·!», lumbar p"nctu ... ' .....
• hiWlry ofrecen t back trauma is common (in u p to 3Q9l.)
no IOlIrct un be identified in up to so-. of patienll in l ome 'eriel'"
NEUROSURGERY
12. lofections
".
ORGANISMS
Operative cultures are most useful in iden tifYing the responsible organism, lhese
cultures may be nega tive (polISibLy more common in patie,,1.$ previously on antibiotics)
and in tbese Catell blood cultures may be positive. No organism mlly be identified in 2950% of cases.
I. S taph. aunluS: the most com mon Qrxan ism (cultured in > 50<lt) possibly due to
its propellllity to form abscesses, its ubiqui ty. and its ability w infect normal and
immunocomprornised hoo;ts (these faclll help explain why many SEA arise from
skin foci)
2. aerobic & aMerobit SlreplOCOCtu8: second most COmmOn
3. E.coli
4. PK udo1JW1WS aeruginosa
5. Diplococcus pn~umon"'t
6. &rralia null"CelC<!M
7. Enurubacter
8. chro"ic infectio"s:
A. TB is the most common of these. and although it h95 become less widespread in the U.s. it is still responsible for 2&% of eases of S EA'''', it is usu·
ally associated with vertebral ost«lmye!itis (Pott's disease) (see
1"ubtl"Culous wrtebrol O!Ileomyt/iJi.:, page 245)
B. fungal: nyptoooccosis, aspergillosis, bruC<!lIosis
C. parasitic: EchinCCOCCU8
9. multiple organisms in ~ 10'1>
10. allllerobe. cultu red in _ 8%
DIAGNOSTIC TESTS
CBC: leukocytosis common in acuu group (average wnC. 16,1001mm3), but usuaUy norenal in chronic (ave. "'DC .. 9.8O<Vmm3 ) ,,, .
ES R elevated in most", usually> 30'''.
LP: performed eautioualy in suspected cases at a level dista"t to the clinically su8·
pected siu (C l.2 puncture may be needed to do myelogram ) \Vith constant .. spira tion
while approaching thecal l ac to detect pus (danger of transmitting infection tosubarachnoid space); ifpus is encountered, stop advancing, se"d the fluid for culture, and abort
the procedu re. CSF protein & WJ3C uSlllllly elevated; glucose normal (indicative of parameningetll infection). 5 of 19 cases grew organisms ident.ieal to abscess.
Bl ood c ult ........: may be helpful in identifying organism in some cases.
Allergy batt ery: (e.g. mu.mps and Candida) to assess immune .ysum.
RADIOGRAPHIC STUDIES
Plain film s; Usually normal Wlless the r", i. osteomyelitis of m:ljsC<!ct v"'rtebral bodies
(mo.... common in infections a"terior to dura ). Look for lytic l<'!$ions, deminerslization,
and ~\loping of end plates (may tske 4·6 weeki! afulr onset of infection).
MRJ, Imaging study of choice. Diffe .... ntiates other conditio", (especiaUy transverse myelitis or spinal cord infarction) better t han myelolCT, and does,,'t require LP.
Typical findings: TIW I - bypo- or iso·lnun${! epidural mass, vertebral ost«lmyeliti. shows up as reduced signal in bar>e. T2W1 - high intensity epidural mDSS that often
e""~noe ~ ",,; Ih gadolinium (3 p"Ulrnl of.nha"".",."t: I ) d.no. ho,n08.n..,., •. 2) inhomogene<tus wit h seattered areas of sparse Or 0-0 uptake, a"d 3) thin peri pheral
enhancement'"') but may show minimal enha"cement in the acute stege when comprised
primarily of pus with little granulation tiuue. Vertebrlll 09teomyeliti!l shows up DS in_
creased signal in bone, associ.'lted discitis produces increased signal in disc and 1088 of
intranuclear deft. Unenhanced MRI may miss some SEA"', g3dopentetll.udimeglumine
e""ancement may slightly increase sensitivity..•.
Myelo gram: Usually show. findings ofextJ"adurBI compression (e.g. "paintbrusb ap.
pea rllnC<!" when complete block is present). In the event of complete block, C 1·2 puncture
is needed to delineate upper extent (unless post-myelographic CT shows dye above the
lesion). See cautions above regarding LP.
cr Bea n: Intraspinal gas has been described on plain CT' ''. Post-myelograpbic CT is
more 5eruoitive.
TREATMENT
Early surgical evacustiorl combined with antibiotiC8 is the treal.ment of choice. AI-
'"
12. Infectio""
NEUROSURGERY
though the.r. ate teporu of patienla managed with antibiotial alone'" '''' J:
immobi1i:uo t ioro' '', ",pid and irnversible det.erioration has oc<:l!rred e~en in pIItienti
tr. .ted with apPf'Opriale ao ubiotiQ wbo were initially neurologically intact''',''', 86% of
thou wbo det.erior1lt«! were initia lly treated it with arHibiotic. alone''', Therefore it;8
recommended that I>OlIIursical management be reserved for !.he following plItienti
(reference'" modified"';:
L thoM with "rohi':liti~ operative ris k factors
2. i.nvolvement of lUI ext.el'lSivtl length of the .pinal canal
3. oomp lete Pl' rll lys i. for> 3 doy,
Sur,ery
Go.b are u l.oblis hin, diagnQl;' and causative o rganism, drainage of pus and debri.
dementofJTllnulation tluue, and oony stablHution ifneeeal3ry. MoslSEAare posterior
todura and are app/'OlOched with. e.xtena ive laminectomy. For posteriorly located SEA and
no l8\Iidence of vertebral Oftoeom~li li l. instability will u~lIally not follow simple laminectomy and appropriate po.ttope rati~ antibiotiu'M,
Specir,c ant ibiotics
If organis m and .our« unkoown , S. 010"", mos t likely. Empiric antibiotics:
I . 3rd generation cepha lOllporin. e.g. cefot.axime (Clafora"')
PLUS
2. vancomycin: until methicillin rel il:tant S. 0""'" (l'IfRSA) ean be ruled out. Once
MRSA i, ru led out , witc h to syn thetic penicillin (e.g. n.fdllin or oueillin)
PLUS
3. rifa nlllin PO
Modify antibiotie& bated 010 cultu re ..... u!~ or knowledr of 800m! (e., . IV drug
abUlle.. have s higber incidence ofCram·neptive organiarm).
Du ration of t r ea tme n t
For SEA, 3·4 week. oflV antibiotiQ followed by" weelUl of oral ... tibioticl .... ua.lly
suffices. 6·8 weeg of IV antibiOlict are l uggftlted if there is documented concomitant
vertcbTIII OOIIt.eomyeli til:'" (although .orne argue that o.t.eomytlitil is pTflent I"'thoJoci·
<:ally in mostcasese"en ifnotd emons trated radiographieally, and therefore the resbould
be DO treatment difference Iletween th_ gTOUPI'''). Serial ESRa may.1soo ruid. dura·
tion (fllilure to reduce suggesUI raidua l infection"'). Immobilitation for at leut 8 weeu
during antibiotic therapy i, ..-mmended.
Ou",,,,,,
Fatal in 4·31% '""(tbe higher end of the range tend, to be in older patinlll a nd U!
tboee paraly<ted before surgery"'). PatienUl with HYeN neurolosic deficit rarely ialprove,
even with l<Urgical inte.,.-ftltlon within ().12 h .. o£Ollset of paralysi s, althoup" f.w_
fll!$ have "'own a chance for some recovery with treatment within 36 hra of".rlllyai" ...
.., Reveraal ofparalyais ofeaudel spinal eonj s.:ognlenta if present for more than a f. w
houra is rare (exoeption: Pott's di~...., has sow. retu rn). MorteLi ty il ul ually due to oriS'
ina l focus o£ infection or as a oompiieation of l'Hidul!.1 pa.raplegia (• .S' pulmona ry embolism).
12.15.2.
Vertebral osteomyelitis
f or differential disgnOOllia, 8ft D"'t'u(li~ k,ion, o{llw "P'M. p81'1939. Often aseoeilted with diacitil, wh i: h may be grouped together under th e tena,porrdylodi«it~ , VO
h .. fut ures s imi lllr to lpina l epidural ab.eess (SEA) (su pu.ge 240).
Vertebnl body eol1a p$<! aDd kyphotic deronnity is common with poaoible retropul •
• ion of necrotic bone and diSC' fragrnenlll againn the spioal cord Or cauda equina.
EplOEMlOLOOY
VelUbral o.t.eomyeli L;1 (VO) compri," 2-4% of all C&SM of OOllt.eo myeliti s'·'. Inti·
denCCl il 1:250,000 i" gene ... 1 pOpulation. I"el dence appears to be ri,iDg. Male:femal. ra·
t;on i, 2:1. The lumbar fpine il the moeteommon l ite, followed by thoracic. cervical and
sacrum ''',
Risk factor. :
I, IVd rugabuH '·
N£UROSURG£RY
12. InfectiollB
2. diabete$ ~llitu8: sU$Ceptible to un""ual bacterial infections and even fungal osteomyelitis
3. hemodialysis: II diagnostic challenge since radiogTaphic changes o[osteomyelitis
can occur even in the absen~ of infection (see 1Jf!'lrucli~ le.io"" o{the 'pine ,
psge 939 )
4. illlmunosupprusion
A. AIDS
.8. chronic oortioosteroid use
C. ethanol abuse
5. infectious endoenrditi£
6. following spinal su rg'l.."'Y or invu;ve diagnostic or therapeutic procedures
7. may OCCu r in elderly patient.. with no other identifiable risk !"aetors'"
Complications that my IIttru&:
1. s pi nal epidural absce ....
2. 6ubdural ebscess
3. meningitis
4 . bony instebility
5. progressive neurologic impairment
6. un ique toCl!rvicalspine involvement: pharyngeal abacells
7. unique to tha."dc spine involvement: mediastinitis
CLINICAL
Signslsymptom.· localiZ@dpain (90%), fever (52~, with rever spike. and chilli being
rare), weigh t lOS!!. paraspinal muscle spasm, radicular symptoms (5()·93'70) or myelopa·
th y. VO somet;mN produces few systemicei'fecta (e.g. wac end/or ESR may be normal).
~ 17% ofpetients with VO heve neurologic symptom s. The risk ofpe ralyais mey be high·
er in the older patient, in cervical VO (vs. tboracic or lumbor). in tbose with DM or rbeumatoid orthritill, and in those with VOdue to S. aureu. "' . NeurolOgIC finding>lare
UllCO mmOn initially, which mllY deley tbe diagnosis"'. Sensory inval"vement is less COm·
mon than motor and long-tract Signs because compression is primarily anterior.
SOURCE OF INFECTION
Sou~s of spontaneous VO: UTI (the mos~ oommon ), respiratory trnc~, so ft.ti""ues
(e.g. skin boils , IV drug abuse ... ), dental 110r&, blunt tralUl"la to th~ spine. In 37%of ceses
a ""u~ is never identified ""
Potentie l routesofspr~ad: arterial , spinal epidural ,..,nous plexus (Bateon·s plexus).
or by direct extension (e.g. foDowing surgery). Spontaneous spondylod isciti1 in adult..
usually involves bone primarily. and once infection i8 esteb1iahed in the subchondral
space. spread ill to the adjacent disc and thence to the adja~ent VB"'.
EVALI.JATION
Imaging
A comparison of the sensitivi.
ties and specificities of various im·
aging modalities is shown in Tabk
Table 12-18 Accuracy of various imag ing modalities for venebfal osteomyelitis''''
,
12·18.
Pia ;" .. -ray: <:hangM !.:Ike
from 2-8 weeks from the onset of in·
fection to develop. Earliest changes
are loss of cortical endplate margins
and loss of disc spece height.
Bone &can with technet.ilUl"l
~m.HOP: may be positive within I·
2. days of infection. False positive increesed uptake way be due to degenerative changea,
recent su rgery or fracture.
MRI: TIWI sbowsoonO llent low signal from the vertebral bodies and intervertebral
disc space. T2W1 shows inCTe8sed intenai~y from the involved VB and disc space' ....
Laboratories
WBC: elevated in only ....3$%{rnrely:> 12,OO()), 8$$OCiated with poor prognosis.
ESR: elevated;n almost all. Usually:> 40 mmlhr. Mean: 85.
CRP: may be mOre sens itive than ESR, and mey tend to normalize !DOre quickly
with appropriate treatment''''.
12. Infections
NEUROSURGERY
Cultureslbiopsy
Culture: blood (positive in ~ 50%), urine and any focal s uppurative process.
An att.empt atdirectculture &vm the invGlved site shGuld be made. ld .. aHy. cultures
shGuld be dGn .. before antibiolics are st&rted. iffeasible, percutao<'Ous biopsy with CTor
fluGroscopic guidance as required is optima l. The yield of needle biopsy cultures ranges
from 60·90%. Open biGPsy is more seJl.'litiv... but morbidity is higher. CUllur" sbould in·
clude: aerobic and anaerobic. fungal and 'l'B.
Organisml:l
1. as in SEA, the !:lost commGn causative organism is Stcphylocoeeus
2. E. coli is a d.l.9t8llt aeeond
aureU8
3. organi6ms 8!lSQ("iate<i with SGme primary infection sites"':
A. rv drug abusers: p ... ",damtJna& aeruginOS<J i . COmmOn
B. urinory tr" ct Infect.IGna: E. coli & Prot~(J.8 $PP. are common
C. reapira tory tract ;nfecl ians: Strtptocoeeu. pMum"ni"..
D. alcohol abuse: Klebs~lIa p""umonia~
E. endocardi tia:
I. acu i.e endocarditia: Staph. au",,,.
2. subacute endocarditis: StrtptOCfJC("$ . pp.
4 . unusual organi~ms include: nocardia (S« pQJJe 223)
5. pyugenic infections are uw:I.x polymicrobial « 2.5%)
'l'ubereulous vertebral osteomyelili"
AKA tuberculGUS spondylitis, AKA Pott'a d ia"u". More common in third world
countries. Is usually symptomntic for many month s. Us ually arrect.s more than one level.
The most commGn levels involved are the lower thoracic and upper lumbar levels. Has a
predilection for the venebra( body, sparing the pojIterior elements. Psoas abscess II com·
mon (the psoas major muscle attaches to t he bGdiea and intervenebral discs from '1'12LS). Sclerosisofthe involved vertebral body may occur. Definitive diagnosis requires the
identi6cation of acid fast bacilli On culture Or Gram stain of biopsy Olaterial (may be done
percu!.8neou$lyl.
Neurologic de6cit develops in 10-47% of patien ts''', and may be due to medullary
and radicular innammation in mostCIISes . The infection i~lfrarely extends i.nto the spi·
nal canal"', however, epidu ral granulation tissue or fibrollis Or a kyphotic bony deformity
may cause cord wmpression ''I.
The rule of surgical debridement and fu sion witb TB is ~ontroversial, and good results may be obtained with either medical treatment or surgery. Surgery may be mOre
appropriate when de6nite cord oompreslliGn iii documented or for complications such as
abscess Gr sinus formatiGn ''''.
TREATMENT
90% of cases can be managed non·su rgically
with antibiotica and immobiliution. Characteristics of potential candidates for non ·s urgical treat·
ment are li sted in Tablr 12·19. For de!.8ils, see
T~tlrn!nt. page 242, for spinal epidural absceSli .
The incidence of treatment failure is increased
when parente ral antibiotica are given for < 4
weeks"'. Recommendations: rv antibiotics for at
le .. t 6 w""ko (longer if ESR " ot "'''nnali~ing) folIl)wed by 6-8 weeka of 0191 agents''"'.
12.15.3.
Table 12· 19 Candldalealo r nonsurgIcal treatment In pyogenic
apontaneoua apondylodllcitta''"'
orgaih$tll iclentifltd
antOJtic 5efISitivi1y
single cisc space invoIvernl1f1t wiIh iii·
lie YEo JIvoIvement
minimal Of no ne<KoIogic delicil
miJ'lmat« no $pi'Ial insIatlftv
Oiscitis
An uncommon primary infection o{the nucleus pu..lPOSU8 with ~ndary involvement of cal1,ilaginous endplate and vertebral body (VB) . May occur following a number
of procedures (see EpidAlmiology, page 249) Or may be "spontaneous' (the latter being
mare common). Often a benign. self-limited disease. Similar to vertebral osteomyelitis,
el<cept osteomyeliti s primarily involves the VB and spreads secondarily to the disc space.
Features a nd manage ..... ent commGn to spon!.8nwus and pG$toperative discitis are dia·
cussed in the "gene.a.l" section below, followed by sect ions describing chancte riaties
unique to each (see SfKJII/OdtM/J.$ discW , . page 248 or Pos!"ptlroU,", diuW$ on page 249).
NEUROSURGERY
12. Infections
us
"1&ny tadiogrephk fe~~ures o{gpOlldylodi.dtia lind Ulmar (met.astati"ond primary) are ,imihu·. but t umors tareJy invoJvetlle dill: !<pIce ..... hereos mOil infec_
tions ""gill in. Dr beror~ too Jong. i"volvlI the ru"" SI""'e.
OISCfTlS IN GENERAL
CUNICAL
).
lympt.onl8:
A. pain Ithe "rimary symptom)
I. local pain. moderate t.o (.,·ere. nacerbated by vlrtu9.lly any motion of
the spine. U&U~\ly w..1I1ooaliz.ed t.o th"I"Vi!) of involvement
2. radiating to 8bdomenlj,. hip. leg. scrolu.m, groin , o. perineum
a. radicular symptoma: in SOO;;'... t.o 93'ii,w depel'lding on till! .erieli
B. fever and chill, 1<I<IIy 30-50'iC.:sre febrila l
2. ligna:
A. temlaroea
B. paravertebral muscle 8p88m
C. limitati()fl oflllovement
RAOIOGAAPHIC EVALUATION
A characterial;" IlIdiograpbic finding tbat helps diBtmgtU yh infertioo fronl n"~t.a·
Italic dileaS4! is that destruction ofthe diK sps«!! is tlJghly suggeltive ofinfeclio n, wher&lUI in generaJ. 1lIml!r d~ IWl. cross the dio<: !~~ (911 Diff~f'Ulliati~ (oc/'mr, page 939).
PlAIN X-RAYS
U$ually nOl helpful for early diagnosi•. Sequence of chang>!Kon plain film$:
• earUelILchange9: int.enpe.ce na rrowing wIth lOme dtmjneraliu~jon of tile VB.
NQt Been < 2·4 .... k$ following onBet ofcllnil....1 symptoITt$, nOr later than 8 ""lui
sdertlllia (eburnation) ofadjaeent cortical margin! wilh in.rea-' den";ty oradja.
cent areM of VB repTl!5enting new bone fOml8tion, slarling"·12 week.9 following
onset or clime.1 symptoms
irregulari ty oflhe IIdja<ent ven.ebnll endplate~ .... ith Ippong of the pediclu (ea ·
~ept for tuben:uloail;. which may involve the pedicle:aJ
in 50'10 O f CBH~ . the infe:tion remaiof confined to the di.~ Spacf. in the other 50%
it IpreadB to adjacent VB
a late finding is wideni llg (ballooning) of the disc ipace with lrQ6ion of the VB
dn:umfenmtial bone (ormation ma.y Iud to f!Jruberant ipu r formation between
VBI 6·8 monLhs into COII",e ofillnes.
aponLaneoUll fiulon ofllle VB moy oc<"Ur
MRI
Demon.trate$ involvem.mt ofdise 8paCi! ond ofve •. M"RI ""n RIO I"'nlvertebrnl or
epidural spinal abscelll but i8 poor in aneuing bony flllion. All aellliil ive II. radionudide
bone KIln. Characteri~1.ie 6.ttdiog: dec-reul'd Bignal from the di!!C ancl ldjlll:el\~portiOf1 of
VBH on T1Wl . and lntrelllled si,gnal !\'lIm these ~tnJcture. on T2W!_Charilctenstk nnd_
ing"l mayoctur 3--5 day! aft.ero:lut oflympluma. MRI al.., rul".-outothercaus"'" ofpo!!t0" pain lepidural ab8tess, recurnmtiruidua.J di.K herniation ... !,
The u-fad ofgpdolinium
enhancement ahow" in Tobie
Table 12·211 ~dollnium en hanoen"lenll n di,enl,
12·20 i.strongly Buggestlve of
L.ocalioll or gadolinium
NumNr (01.1 or NUlIlber (out 01
di$citi. (lome aaymptomalic
InhBI>te"",""
1 ~Ilenlt with
15 pBlltI1lt
patients may ha~e some of
wUhoul dlKIIls)
dlaellla)
thell@finding1l,buttheyrarely
ver!eblalbone millfOW
7
h.veaIlP".
CT
,.
• "'"
,
7
,
7
MlIY a1lo RIO paraverteI>ral or epidurol'P1nolabacen. and il better for aueS8inll bony fllaion . With the addition of wllter IOlublli
tntrath eocel enn trast. ~Lao a9~~ iJle spinol tanal for colnpromi.se.
pOI$IefIOI" aMU£us hbrosus
12 rnfection9
"
NEUROSURGeRY
Dia gnos tic c rite ria
ThrH bas.icd\lwges on CT'· Of all 3 are present, pathognaJTlOllic for discitis; ifonly
the lot 2 are present , then only 87% specific for discit'.):
1. end plate fragmentation
2, paravertebral soft-tissue _e ll ing with oblituatioll of fat planes
3. paravertebral a~88
SPINE POL YTOMOGRAMS
For P<l'IUlperative d,,,dtis (P OD): performed through level of previous discecUlmy.
Otherwise, eent.er tom0I.'Tam S on painfulleve!.
SCINTIGRAMS
Very sensitive for disciti. and vertebral 05teomyelitia (85% sensitivity), but may be
negative in up t(I 85% of patients with Pott's disease. UI5e$ either tedl.lletium·99 (abnor·
mal as early as 7 days following onset of clinical symptoms) or gallium-67 (abnormal
within 14 days). A positive scan shows focal increased uptake in a<ijaeent elldplat.e., aod
may be differentiated from osteomyeli tis whicb will involve ooly one end plate. A positive
8caO is not specific for io:lfection, and may also occur with neoplasms. fractm-es. and de·
gene rative changes.
L ABORATORY STUDIES
ES R. [n III1n .immuoocomprom.ised patients, ESR will be elevated in nlmOB! all cases
with an average of6O mmlhr (although it ean rarely o«ur. a normal ESR should call tbe
diagnosis into ques t ion!. Interpreting ESa may be more problematic in post-<>p discitis
(su ~ 249). ESR rna)' be useful to follow as an indicator of response to treatment.
C r ea ct;ve protein : Su C·rea.ctilJf' prolein on page 249.
is o~n nonna!. and rarely is elevated above 12.000.
WBC : Peripher al
PPD: Applied to help R'O POtt'l disease (see Tubflrculmu; wr1~bral OIloomyeliti$:, page
245). may be negative in 14% of casea'''.
C ultu",s: An attempt t hould be made to obtaill direct cult urn from the involved disc
~pace. These may be obtained per<:utaneously with CT or otber radiographic guidanCf!
(reported up to 60'1> positive culture rate; if available, s lIudeotome provide.. a higher
yield than e.g. Craig needle biopsy), or from intra-operative speci men (NB: surgery for
open biopSy alone is usually not indicated). Staining for TB must be done in all cases.
Blood cultures may be positive in. 50'1> or cases. alld are helpful in guidillg choice
ofantimierobialageDt ",hOlD positive.
wac
PATHOGENS
Staphylococcus aUl"('ur is the most common organism when direet cultures are obtained, followed by S . orbu8 and S . epid.ermidis (S. epidermidit.a the most common
pathogen in PODJ. Gram negative organisnu may also be found, illduding E. coli and
Proteua species. Enteric nora ;D POSl-OP disc itis may due to undetec:ted brP.acb of the an·
terior lon/litudi.nal li~ment with bowel ~ rforat'on .
PHuOOm<>fl(U Ot rugillOlO may be more common in IV druil abusers.
H . flu is common in juvenile diadtis c,,,,, below).
Tuber<:uloU8 spondyliti s (Pott's disease) may al80 occ ur.
TREATMENT
Outcome;s generally good, and antibiolics l.Ogether with immobiliut ion are ade.
quate treatment in . 75% of uses. Oc.:asionslly su rgery i. required. Also see Mar.agt ·
menl, page 250 under postoperative disciti . for other aspects of management.
IMMOB!LlZA TiON
Probably dOl'/! not sITed filial ou\come, but generally aITorcls earlier pain relief, and
may allow return to activity at an earlier time.
Most patienta are started on strict bed rest, alld are fitted for a plaatic-typoe body
jacket in which they are allowed toambulate, and in which they remain tor 6·8 weeks on
NEUROSURGERY
12. Infections
'"
the average. Alternative fomm IIf ;mrnllblhJat,on indUlle ~pica COlit (provide. better immobilization) and a ooraet·type b".~.
ANTIBIOTICS
CUmlnt thinking is that mllflt p8tienu should receive antibilltitll. gu.ided by the reo
s uIts ofth'" direct eultures ""hln positive. In the 4 0-5~ ofcaaes ""b ~re no orgllnilnn is
'solated. i;)roll.d spo:ctrum ontiblntic511.hould be uaed.
Two alternat ive tn8tment 1'111115 suggested:
1. treat with IV II.ntibiotie~ for ao .. rbitrary-period Of time. Ilsually . 4·6 w~ks. f.,l_
lowed with 0",1 antibi~tics for an additional 4.6 weeks
2. treat with IV antibioti~1 uuti! the ESR nnnn9!itU, then change 10 PO
SURGERY
Reqlli~ in only _ 25~ "r casea. Oebrideme,a lJIoy ~ dnn .. throllgh the previolls
ill.mlnedomy sit... Ikwever. if lilere has be.>:n significant bone loll!! and Inatability, then
an anterior d~tomy and (uII.10n through II retroperitoneal apPl"'IIAI:h !My be rnquired.
SUrg<'1)" is reserved for;
t .Iit\Ultion~ wh e~the diagnosil iauncert.Bin. especially when neoplasm is _ s trong
con~ide'8tion (CT gu.idt><i n""'\l" bi"P$y may hell! he",)
2. dec<lmpress(nn nf neural.tNctures. upeci.lly with associated .pinAl epidll ral ab·
$~a IIr compression by re~ctivl'-g-rjHlulot; on tlUlle. A8<:ending numbne~$, ...... ekIlea, or OlUn of neuTogenie blodder herald cauda equina I)'lKirome
3. dra;n~ge of a55(lciated abllC"'I&, upecially septat.e<!ab.ceues Wat lIIig11.~ be recs(.
titl"llnt to CT KUided percu(aMOlls needling
4. raNlly, to fuse an Ill\$table spine. PoorlY 'endor&ed (n tbe face of active infection.
el~i~lIy since. mllSt 10 on to BPIlnl.alle<>Us fusinn
Approac hes
anterior diacectomy and cOl"('(!Ctomy remov.. the offend ing infected lisliue. wilh
using Wile crf!4lt (or. in th thorade . et:ion. /I p<l5terolll~ero( approacb.
with the &tNI mad& f,om the re&e<:wd rib if large enougb)
2. PQllerio. laminectomy lDay be odequllte for emel"\lt!nl decompress,on. bu~ d"""
nOlllll(lW "<!<leIS to the aite of palh(llogy in Oilrvical or thorack regioDs
I.
Ht.ruljt"f8n.
SPONTANEOUS DLSCmS
No I1!C<'nt history of lIu .gery or in:ltrumentatlon. Higher incidence of n~urologie def·
icits and I'IIdieu1op>lthy r.h,n with pot;toperal;ve disciti, (POOl.
'two di..!!tinct type!!:
I, j llyen ile: more romll'OO : age ll~uulJy "" 20 yrs ("~ belQ1~ )
:l. adult: uSllally OCCUMI in aUlCeptible p3l;enl.a (diabetic •• IV dl:Ug abusen)
JUVENILE D/scmS
Aile lIIuully"" 20}ln, with p peak between 2·3 yeal1l. Probably due to lbe preaenee
nfprimordial [.....ting arteri~ lhal nourish I.he nucleua puJpo, us lind which involuu al
_ 20-30 Y'" age. Lwnhpr . pin .. i. <no ... ""<nmcnly i"",,/ve<l Ihan th"".,;c<I.oerviCIII. Cnm·
WIlO prese.otation; . eful8 l towalkorlltand pro~(ng to ",rugl to sitUl youug-children .
Back pain is mosl. CtllDmOO in children :> 9 )'rs ace Low grade- fever may\)Ol presenL ESR
Is uSllally 2·3 II nonnal . WBC i3 ~mel;mes elevated. H. fI .. Is a lJIore Ctlmmonly IM!f!n
pathol!"1m in W. grllUp .
In mo.gt tMef, there is c:wnple1.e resolu!.ioCi in 9·22 w~kP.with<lu l re<:urrenoe.in lon,tenn follow·up sludie6' '''''~''. Surgery is ",served for the rare ease ~hat progresses in
apite of an tibiotics. f<lr IIpir\81 in.tability. 0. for recu.rent ""Be••
MOtit authors reserve .ntihio:,.:>; fur patlent.!l with'''' '· -'' ~
L pw;il ive clli lures (blood cultllres or bioplycullUT"Sl
2. elevaW<! WBC oount. IlOn$titutiollll] ~ynlptom •• Or hIgh feye r
3. poarresp<'lMe to re$t Or immobllir.a tion
( . neu,..,logie ~quelae (~el)" f'II",'
Antibiotic. should be. given flIT a toblllf4·6 weeks. Start with rv ant lbiotiC$. and
when clinical symptom) Improve convert to PO for the remainder of therapy.
u.
1.2. lofectioll8
NEUROSURGER Y
POSTOPER ATIVE DISCITlS
Unless otherwise .peeified, the following
identified retrospectively at Duke''''.
i~
based on a "eries of27 p<.l!I1.-<,Ip cues
EPIDEMIOt..OGY
Indden"" after IUr:>bar di~lOmy' '': 0.2-4% (realistic utimate iR probably at the
lower end ofthia range ). May lllao OCCur after l.P. myelogram. tervical lamineclOmy, lumbar sympathectomy, cilemonucleolysis'''. discography (U t paIJe 296). Fusions lind othe r
proOl!durea. Very rare after ACDF. Risk factors include: advall(»d age. obe~i ty, immu nosuppression. syatemic infection at the time oflurgery.
PA THQPHYSIOLOGY
There is Klme controversy as to whether 80me cases of p<.l!It-op di""iti, ~ not
infectious'''. an autoimmune pr0ces8 ha" been implicated in some of these so-called
"avascular" Or "chemicsl" or "aseptic' diseilis case$. These cases are less OOmmon than
infectious ones. ESR and CRP abnormalities may be Ie$! proMunud in th""'" patients,
and biopsy of the disc spa"" fail. to gnow organism, or show signs of infection (infiltrat'!s
of Iymphocyteto or PMNS) on miCTQ!!OOpy'''.
In septic ellSes, various mechanisms for infection have been propo6ed: diTect inocu·
lotion at the time of,urgery , infection following aseptic necror;:is of disc material..
CUNICAL
1.
int'!rvai from ope ration to onset of symptoms: 3 days to 8 mos (most commonly 1·
4 wks post-op. usually al\.er an initisl period of pain relief and ,ecO"ery from SW"
gery). 80% present by 3 wks
2. symptoms,
A. moderate to (usually) severe back pain at the site of operation was the most
common symptom. uacerbated by virtually any motion of the spine. often
accompanied by paras pinal muacle SpDBmB. Back pain is uaually out of proportion to the findings
B. fever (> 3S· C in 9 patients: literature reports only 30-50% are febrile) and
chill s
C. pain radiating t(l hip, leg, scrotum, gnoin, abdomtn Or perineum (t1"\.le sciatica is uncommon)
3. signs: all had para"ertebral muscle !pasm and limited range of motion of the
spine. 13 were virtually immobiliud by pain. Poiut tendemes>lover infected spine
occurred in 9, upressible pus in 2 (literature repor\.8 0-8%). No new neurologic
deficits were no~ . Only 10-12% have MSociated wound in fection '"
4. lab findings:
ES.R: 261'27 had ESR > 20 mmlhr (60 .. ave .: > 40 in 17 pa tients; > 100 in 5
patients; the si ngle patient -: 20 was On steroids). ESR ;ncrf!S/!ea .. fter un·
oomplicated discectomy. P':'alOng at 2-5 days, and can fluctuate for 3-6
w~k.oi bef\lre normalizing'· '. An elevated ESR that never decreases after
surgery i. a strong indicat(lr of discitUi
C-reactive protein (C RP)'"': aD acute phase prot~in synthesized by hepato·
cyteg that may be a mOre specific indieatorofpos1.-<,lp infection than ESR because of rapid decompoSnion. [n the absence of disci tis, CRP peak.oi - 2-3
days pos1.-<,lp (to 46 :t 21 mgIL after lumbar microdisceet(lmy, 92:t 47 mgll.
after conventional lumbar discectomy. 70:t 23 mgIL after anterior lumbar
fusion. and 173:t 39 O1gIL a!\ar PUF), and return. to normal values of -: 10
mgIL (" I mgldlJ between 5·14 days post op
lYJX;:; ele"ated > 10,000 in only 8127 (Iit'! ratu'e: 18-30%)
RADIOGRAPHIC EVALUATION
Also, see Rodiogrcphic ellOluol«m, page 246 under Discill, in general .
In postoperative discitis (POD), the average time from surgery to changes on plai n
x-ray is 3 mos (range: 1·8 mosl. Changes are detectable earlier on polytomograms l3 wks
to 2 mos) . "verage time from first chaoge t(lspinal fusion : 2 yrs .
NEUROSURGERY
12. Infections
'"
PATHOGENS
5« T".b/, 12.21 . Most st ... din report S. ".... .
Table 12·:ZI Culture rll. ult.
Ole most commonl)' identified organism.
l""OUnling for - 6O'i\o ol"positiw. cultU~I''', fol.
lowed b)'other'Ulph .pecies. Also reported : Gram·
.,.,g. tiV(! orgln;'m, (indudini £. ~j), S!"P uM.
daM. St"pt(}'tOCC'" .peeiu anatrob.., TB Ind fun·
",ul I I
••
Blood cultur.. were. potitiV(! in 2 of6 (boOl S.
0."",,,,).
For culture tec:hniqllH, IN /xIQW.
MANAGEMENT
L admitting I.be (in .ddition to routine): ESR, C·rll.ctivlI pratei n,
2.
esc. blood c... l·
turn
1n.lguics. mutele re lUll nt.l (e.g. dinepam (V.llum(1J) 10 rna PO TID)
3.
'ntibioti~
IV IllItibiotia for Hi wks(or until ESRdecrealle,l, then PO for 1·6 mG$(typicsll)' 6 weeks)
most , tart with . nti .$laphyloeocc.lantibiotic. (initisl ",mpiric th"'rapy: vanoomycin .. PO rif.mpinhnd I broed .pectrum antibiatk(e.g. ""box), mod·
ifY bal<!d on 8Inativitiu i(poII;t;ve (ultuns.rt obUlined
4 . .ctivity rntriction (one. 0( Ole. fallowing used. usually untilsignHlcant pain reHeO:
. plnal immobilintion wiOl s pia c.1t ar plastic body jacket
, trict bed rat
activi ty with con.et
5. SOlllllluthGn recomlllend steroid therapy initially to ..~ilt pain relief
6. cuitu,n: performed if radiographlsuspicious. usu,lIy performed utili~ing percu·
u,neou. CT-ruided tecilnique
A. , ilel
1. disc aJpirllion if evidence ofdisc space involvement
2. ne«lling ofparaspinal m.ss if pUllent
S. send cultures for the following:
1.
7.
sUlins
I . Gram stain
b. fung.1 sUin
c. AFBsuin
2 . t;ulture
I. routine culturn: aerobic and anaerobic
b. fungal culture: OIi, is not only helpful for fungu.!, but .ince thue
cultures are kept lOr loncer period and '"Y growth that occur.
will be furth~r charaeterized, fll.8tidious or indolent bacterial or·
ganisms may sometinwl be identified
c. TB culture
3 pati~nt.l in Duk~ series und",rwent anterior discectomy and (u.ian s ne.r unsue·
~lJIrul medical therapy
""'COM'
9 p8tienb developed bon;, bridging in 12·18 rooa; 10 d.vltloped bony r",ion in 18-24
~.
All potienb eventuaUy becnrnoe pain freoe (or Iignil\cantly ImprOVe). Thi. i. not the
in aU .erin, where lKlIlle n!port 6O'ltl were pain free It FlU. IIlhe ... found ,light welt
pain in mo.t patient.l, and yetothe ... report Iflvereduooic LaPin 75'.4". 67-88'" return
to OIelr previa", work. and 12·2':;'" received diaability pltllliGn; 01_ n ... mbers art .imi·
lar to the outcome fram dilc ':.II"Iery in general.
Na difference io outcomoe wU found for the variGul activit)' reltrictionl.pecined, 1\)1 •
.:.opt for earlier plin relief with first two typt1i lilted .t.ov..
taM
12. Infections
NEUROSURGERY
12.16.
,.
References
,,"i.., A II. A""mlC.w;., prop!lyw.i, ...w,...,..",
, r..&1 J
,. K.",,,,II.
of
Mod lU, 11,9·31. 1986.
F.."", PT. W'UO>Jo;WI>,Un, C.M<\..o., .. 11. l.: Poo_
.. "',.,. of .. r<;II; •. mrll>::;I Ilt!, ..... «f.<O\," '.'0
"".". tni.,;'..." . "".' OS. 'ltty II: 141.7 . 1913.
OS.CI ...... OC.llu,u j P. "'Q/'
«~Io>P<>'in.
~
mphrlOC<l<.oI "«UJ
". ,," ." y)"
£1><_ M I. e:.m-.. OIl S/>ek<..,.,. A." aI.' PIi,
""'I)' "00."
F"'." "
I"
...
",
"",,,.1 _04 ,.f"",on .. JAIII ... 263: 961-6.
'.
,.
•
,.
••
•.
,m
11.,,«, F <l: Eff..:.<y of P"'P>yl ... ,• ...,lIto.. ,,,, for
",".,,,,amy: A ......· .....1 ... . Noo' ...... '1' JS:
..;.0·92.1994.
YOU", R F. Lo"' .. rP M:
"";"00'"
prop/Iyl..i, r... pcc .. ntion of Il0l1''''''''''''' .... m",.,,,aI io fecoLon. J N _U'Ii16: J()]·S . In1,
B.t .... l. T_If.S.S>k<I!ariou p, "4/' ""''''''U·
mali< meni","i" B..... iolQu. h)'<lroc<phalu,. ond
<.""om< . N.... ........., JS: <n·l. IW<.
Et;.m.' M S M. Foy I' M: _ ·".....,11"' OFf,,,u·
1... 111< co .. foe .... ",at ",poir. II, J N",,_'lI~ '
"",Lope.."..
.1Hl. 1990.
u ..... w ' C... t.<><p; .... nu", " , i _. in,_
lie'" i.~ •. C~. N..."",", ,12: lll·Sl. 1966.
Horwi .. N H. I.... yC S: Com...." .. HoI .. ,I. " ."
"""
......... " ....;"li""_ 1Io<"'rioIot.7.
hydroctpt.ol., • .,.j <NI<QmI: . _
..... , lS: all>. 19'JoO,
V",.. R' Ce"l>A>Ito;1!Il n.i<l.hu .. ,nf.<1i"n., A
.i<w, Pt<I .. " l nlo<' Di> o. Ill·'. 1985
A""", ... i lot. lI.i<Mn<l; A. C. .. t>ro>po ..1 nulll
,hu .. ,.f........ i. <hi!cl"n, A "1>11 of Ih< !O ........
•'''~ be,...".., tl'II: "iolOU"I," hydroc<""' .... 'S<
.. 1M: ,im< of"'un' »I>o< ....... ond ",1«""" Child.
N.",S)'" l. 106-9. J9I7.
M,Lon< O. C.~"",w"'i D. ~ .. mo"<1i A," 41.. Ce.·
uoJ "''''''''' .~ ... '" i........ ... O.. i,;n.a {"'lOt i.
lIIe '00<1101<"1« of '~,Id ... wi,h ntydom,",ntoe<l<.
P..Ji.,C'b 10, 331-42, 1~ll .
A"",bor A L. Weillns' .. I: lnl.." k hyclroc:eph.
,10 •. L.ooI ·....., ="1" of '.'1""1, ....",,. Cbllcb
8 ..", II: 117·2\1. 19801.
O'Brien M. P..... A. 0.", B: Iot.n" .... ", of "" ...
""" ... ohu", 'nfec:' ........ CblIMB .. I.~: JOot·9.
...
"
...
".
,m
Woi<JS L. Md .....inR L: Shun'· .. ~odl_
ulonep'OI'''''' N.."""" ... y 1: 1.j6..~> '97,
s."""" of PM;',,,,, N.u"""",oty "I<too: A.....,"...
"'''''''''ion ofNewol"""ol S........... (<<I,) P.dl...
,10 "'''''*''&<1')' , I.. «1 .. 0 _ "'" Sua",," , N.w
York.l9fl..
Fra .... p T, M<:l.ouno II L. T,....,.,.."., ofCSf .... 1II
,.f_ ..... ""'" ;"".","'" pl., .... , ar."l;Mo"" , ....
py. J r<.... _" 00: llO-OO. 191".
I ...... H~. W.... ~l W. Wil .... II D,""'': .....!p«•
"" .. ndomi...:! _~ c( ,hefoP1 In <."'IH<>Sj> ....
noid """III ,"fecoOon. _ ' l t T y 7: 0S9.f>l.
1910.
s.: ..boI: P. Co<tnn. 0 0, K.,,10 J R W: The ,,~ .
nif"' ...... oIl1ooc"riolo, ... lIy poII~i" .... riallo~..i"'..w "".., _""'" i.1h< _""" 01 Olher
• itn. or.huo, "'f«,ion. J /'I' ''''''''''IlO. 611·1J.
,~.
W.
".
n.
St-d"".n A.O, ... "'~ MS .SoIomon M p, ., 0/,
M"'lemen, of inf«l«Ibm;no<"'my""",lIIIs.
N"""""pry lS' )(11·9, 199'.
Ku", A.S... I<,O 1, /..enI.atdt R. I'<,oof"'OIl .. ""'.
~nn"l0 Ifthoc< ,he
01 ......,,,,,,1.
w""tIII •• 1"", ... ond """',n "",p;"lito"... N En"
J M«I J14' l109-U. J9\lI5,
Ootn.."" P 0.<:>"''''' 11. H>l'InJ: Pri""'J'lo<co ..
or ,.r"""", .p, .... 1""",till •. N... , ........., 16: 7<l1.
9,'990.
NeUROSURGERY
in<""'"""
'W,
«_ . ..-..«>n<..,..
....I9Il.
N.".. D"._..",OO, R""' .... dI: ... loplnl ""
"",,,,,,,1>I>«< .. . J
010/ 1(1.1 :
"6&-n.I990.
HoU;" S ". H.y .... i H.O ..... S W: 1"'''''QlliO, .b""'... of ocIo"oscni< Gri,i • . On! SU'I ll, 177·
91.1961 •
Wittwm F II. Nolml 0 K. McGoI!&nn K M. 8";.
.boc:eso; A .... «ImPli,"ion 01 bolo .'4<. A,,~
"",.M..J IIlf>o.hit 7l: 49()..1, I~l .
On",,,",, I A. IIlro<hb<rJ II, 11,,"..... 11 K: 9'hnT,,·
1Ie...... th~I""""I<..."., .... ' ... kol:ooyte """ ,
"",pilI "'" C·""" .. p<O!<i" koc" ,n ,.. d,rr.. •
ell'IOI di,,_i,oltnin .1»«"" •. J N.u'''"P'I77.
JJl·6.199:I.
F,;':t. p. No]"", P 8 : 8ro/0 oil",.... In u.',aI
" ..""'. 'j'>Um i" f.. tiomdi .......nd ,htnPI.
R"", K L.(..J J. MIIWI DoH .,.,... ... York , 1991:
ppoOil.91.
B,,,, R H.&."..... 0 R: Ctini<oI ...",.oI"hu",".
b<..n . bo« ......... iol CT
of, ... «W .... iofu ..... J _
....... , S9:972-3'1. 1911 .
H..... """ II S. B,..dI: A I. OsIaIw>itn 1 L: lou"",,·
n'ol . u"""' .. '~4ilUl<. J A JI.I" 111: I~2- 7. 1911 .
Block p. C .. ybo 1 J R. Chu>o<too: P: "'... "''''''' of
tn," .1>«<.. b,- .~".m"atl~ adm'oi ..<RO<l ",,'Ola·
k., J N....""'. aJl. l'O.l-g. 1'173.
R""""'um 1>1 L.lloff I T.No<man O."QI.: " ....
ope"';,.. _ _ OJ ... "' ..... _ . "' ....... «1
",,,,·n.k pOI ....... J 1'1 . ......... S2, 11l·~. ' 910.
R.dl< A. Zerbi D. :z..cc...11o M. Of 1'1.: B",...',,"
.1»«..
1»11, b,N "'""'~'i<",lI : 7.2-6. 1991 .
ui<l..,." S M.O<;"', fH.Oli.; A: In"' .... n<~I ..
"""." 01. "",,,len' bnin . _ , C..... pon
10...",.......,)6: 11!l-9l. 199$.
S'opbono' S: s.~ _""'" ofb .. ,,, .1»«...
N.............. ' n: 724-)(1. I~ .
Hotl""' .. O. V;il<"",,, J..Q. I.cbl""" II : """m'"
. _: A ... ~.Il, u_1< 1<.... . Appi
N""""" YIlot~ 16&-71.J917.
Ro ...blum M L.llofO T. /'IOnn>ol O. ,,"'.: 0. .
, ...1«1 morul.it"1 I<om In •• ob>< ..... .;""<0<\, .....
orcr, J 1'1" """"'349: 6:lS·f>II. 1971
II)"", E. BlOpI'tj' B P.""IC" L V, :-.'""an/j, ",_I
""""": N,w
in ~",no.i" """"...... ,.
ond pI",""'".J N _ .'1<0.0, ... ' . 1'1101.1" ' 1'1:
I031"S.1919.
Lar,.
""'1<"'" ..
..
.."
..
..
"-
~.
...
...
°
1<''''
,....,«1 ",," ..
•.
".
of *,.".1., in~
",om, a",,,""mo:nil>idi •
OJ>dboo<lo~ol"'in_ ... ·J_ ' I~m·
'"
.,
mod".,
0 ....,. 0 : a.m:",
of III<
~.
"
".
".
"",.. ,<me", of mul'ipic Imin ObI' • ....,
A comt.;nod ' "Il""loO<l
_ h . /'IN ' '''
"
"
".
...
Im~,od
"'I<. y)6: 16-86. I99S.
T...,,;'" M. K.p"'. M. V.. ~ S. "4/ .. CutTCOI
_ ..... of Ini" .bK<u in ~i<". with , ..,.ni.
.., ,y.""'i< bNIo d'oease. N......... , J • ., 01: 12709.1991 .
Kon«< M C. H... R 0 : NourolOf" «><npl"'"'''''''of
l.f«,,'" 'ncIo<"'hti •. N~" : 101'·.10.
"
"
-,040. "'""",
..""".ffeu1 """""""". r OIl .." IUd.,. I~ ,so..
I. I'ISI>.
Bull'" E.l.ch ..... 11. II w- Ost<omyt)i,i, of tho:
>1;.11 SUrK N.....01 II: 16l·~. 1979.
M"""I" A N. M .m~WnT LOb&no WG.<lD/.:
"
"
" 1'<"""'"'
".
0(;.1«10<1.."""
m.199oI .
L",,"'ky J L. _ I I P,EiJ>oIm S E: Pah<tol ....
,oomy.lj,;.1'>l cpidu ..... 1>0<.." A <l<1'rod ,.",.",.
Infections
mod"'.,"",,,,,,.
""""'pl'
'"
"
~.
"",.d I. 5., J 'OJ. Po'<f><. J M. 1'.......1<»IeOm,_
"",.of,,", ,,"'" ","hop'''''''' '!>iN1 ,"'" romp..._
oioo· A 00<c
", lS4.6.I9S4
S, SlOW" A H, I.. ,o< ... iol ..
1»'<.... """;,. mO<W£<m<rI< A,...,,,,of 'I><I,,.,.
'." "';'h eom"""". S.. w Su .. ' IUo 1~9-61. 2001
KubOl C S.Ado"" R 0 - Subllu",'cmp),<m"
66: 18"2.194)
s,,""'''''.
_
N...,..,.~ r .... ,
.."
...
B,,'.
Dill 5 M. CObb:> C G. M<DonaId C K: Subd''"' <m·
pycmt: An,ly.i.of)l <a ... tnd ".lew. Clin I.f
1);0 10 ' 11J.S6.I99S .
J>«>I><M P L. r.m><l T w. s.ubd.""<"'91'''''
«>m1ll"";"C ", ...
In i.I..... ' ImJ)H>"td P<'OIi-
,n,,,,,
"",... I'I "'roIotJ' )1 :
"
"
"
"
•
"
"
".
"
w.
".
"
~.
..
"
.
,,1_ .. _...,.'0.,. ..,........"""'.
m
~.
"
N<.""
",,,tn<1I,
_«,"'"
m~.!987
s.:"""h G. C.""h. I. Tb"", ... . ., ~I. ' Tho ."..j) di """,io.,III< 'f!'•• itnpl., ...... "..." ~ '" MRI.
Nou, oIOU 37' 119·1). 1987
Whi,l<y R •. Sooos S_J. Dol io R. " "L Ado"";,,.
II><npy 01 t><woy.1"O'<'<l h"""", ~ ...
p'" ''''''pI>aH,;''' ro-ui«>ll ,no'"'''' of . 1I,,1l' ond
i.f. .. ",., _ .....oll'l>ORti ... ..,..1..1_yorofnJtl J M«I797' lS~. 19n.
s.: .. ,iKMJ.M""' ...... R B.IIo<wl;.1 M,,,"": II .. ,.
biopoy for ""'pII&l~". C~ . ,.. .." .... ,~ )): ~l ·
602.1936.
WIt"",, R J.e_cc. ""fon:I C ".<lM_: 0;" ....
Ih .. m;",'" 1I<1V<, . implu ",,,,ph. liti l; 0;'1""''''
~""""
J A.\l "162: n .·9 .
"'''''''''iII<
,m. .•nd""""'....
e • ...,..k M A. rw;"J.e..,-"" .. DR. n"'.: M.I·
"ro<o1 i<."",""q>h>I ~ i<.-d b) ......11.·_
.i"" in •• hild " .,h I,ul."",,: SU«fl>foi 'lUI ... ",
""h O<J'.lovlr !'«Ii." Inf"", Oio J 12. .002-6.
'9\13.
B,I'n«R W.hm... ' O. M,I,;I<><oI ....,<I.
I. ·...... ' ..... , ","k"""p"",iti> 'mtpo"ny ~mote
fromll<fp."""', ... .. N.~ roI 9 nl-66. I981
lohn_ ~T.C;t>bIC I·C..,,"r.Id '·lal..,di .....
."d "Ill'" ' ''''''''''ito. !flO.~,f"",, ",.. phoIOpo·
'h .... N Etl&1J ,'.1'" 119. 1994·2000. '991
c.jd"",~ DC: Ull«>ll"'", ....... iN>n .... ,1I< on·
I "' .... dl.. ppo&"not oH<>nt.Sd<t>« I~ . 94l-60.
1977.
KIi....... R. T I>< " .... blJ o ~ """, nLoI •. A po ...... . ,
K<OII ~ ' oft u"',<onn lbo(o, . .... ",oil «>", dh._ .
Pl •• ,mT,ad<. No" Y"'k. 1m.
_ . ..... ) G.U"IC lC .1't!nt<tt F, "., · T,,,,. ·
mi ...... ofC"-",d.Id,·).k",, ~; ......i, • <_,I
"""'1'1 ... . J No . roI N.. _"". l'Sy,hlo..,. 6);
.JU.9O.IWI.
110100 11 . """ " " S B; I."",; .... h.l .... ""ood •• •
..... N"'I'OIoo'40: 1120-7.1990.
J M. 8..,..., p. Coldf"" L C. ,,"', F, .. i1i,l
e"""feld,-Jokob d, ......
200 ...... ,on)
"'". """"","k.. pOl.y. JA.\lA 268: 201 l-S. 1992.
W,II RC,Z."'I,,' W,e""""" SN . • ' 0/.: A """
vo,;"" ofC,.""I<I", ·J•• "" di>oeo)c in ,I>< UII
r.. ..... )017' 9l1·S .I9%.
Ho"".
6<",,,,,
«odon
12_
Infe~tjo"s
Duffy 1'. ""oIf I.C"~o.G . •.,ill._ Pou,bIe "''''''' '"
PO""" '~'",,"''''' orc.... .r.kI'·I""o~d"" .... N
~J U ... 2\IO-691·].1'lJ4.
""""",IIi C. S.. ",ri«I J, II..",,,,,,,,,, G,,, III"
o..~ of ><code ...1p<r>On·lO- p<non ".."m""""
ofc",""r.kI1·'III;Obdil.eM< by, ....", 1.0_ L
47!·9.19n
F,odki. J E.
L B. Mill. J L ", <>/,
c ....,r.1d1·Jombd;_ in ,,""ilO<)' JfO"'Ih hot·
moo>< ",cip"'" in Ih< U•.;!«I St. ... . JAMA 26~ :
ScfIont>o,,,,,
1l8O-4. 1991 .
"
n.
1\0,,,
..
"
190-). 1931 .
MUI'Jli. A J.CooO";. W I. AmO:dJ J<. " .. ,., 1.uoo, ..
~"I'nf<<<kmo in ><1,1" and <M"r<tI A.. h
Ot.I..y . ~ H.... N «k s.. , ~ ,, ~, 14;4 _~ . 1989.
COIf,. S R.
M I . Tnu,lI 1.<101.' S.b<I ...1
........ ""lO<ill<d ""~ ~'IOi'i.'''''''_ J lion.
J.la 'S''1I71)'''' 1l31..r.l.1981 .
W'i,brt. ~ S.t>ci."le""'r<""· Clio",,1 ooo! ..... pu«d ... ...,p>p/oi< <'(In<1 .. ;on,. Ar<lt
OJ.
oW1-:iOO. I93<i.
Mou"" H W.Ito"jI, R A P.E""'''''''A. "./: N.",·
' ''1",.1
of •• ~",I .mpyema: C.,., IepOll . J 101 ... , .",,'1: 6l : 121·)0. I98S.
Wilk,n' R H. R.np<!WY S 5.1.,1> ). N..".·
,"1'Xfry . Mc(;""'·Hill . N<w Yor'r:.19lI.l .
N<illEW. LIIl<,. R.Torn • .,k T A.".,: M'&fI<Ii<
,.,.,. ..... imoC''''''''
lOII\OVIp/ly
", • ..,i., of II<rpoo .. mpk. ''''pbl;'i •• J ro-.., .....
...... 61 '
"
"".ral.",·
~.
"
".
n."" •
Itooenl><'1 R N. WII;", C L. S...... P, " .'.' """"'"
'_;..luo><Ili"l".......
.,.j"' ..... «>o>U .. ;·
n_
ffOM ""10",, "i'h<lO<"""' ........
C",,,,.f''''.Jok<>b di..- AM N......
' loU·7. lm,
B....... P. Cit>bl C I. Am). J L. ,,~I.. Cl>emk,' <Ii,.
inl«,..", of C", ... foktt·l.kob .im. N EotiI J ,'.1'"
J06' '179-12. 1911.
/I..,..., P.C.. "",. f,e.... i&"< P." 01" em",r.",,·
lok",,<li...,.: CI,ok" ".1,.,;. 01. _>«"'i~ ,. ·
...,0( 130 ",_,_,i<,lIy .. ';ford c,,,,. A".
591 -602. 1986
fink .... ""'" M,S.utlnt A. Zen-I.~. I , MR im.,·
~oIa.. 'itI.Id,-hl."'d ;","" . Rod"*'D 199.
79).1,1'196,
Cern H·J, He.ke, H. e<rvos·s.",,,, I.
C.. L<Zf.IdI·I ... .., di ....... Con'<I ...... of MRI ..d
""",opot'l>:>loJic f,ndi." N•• ~ l'. 1481·1.
.,...';.1,
....1>«,,'"
N<."" w,
..
" ,
"
".
"
W
".
"
"
..
"
...
".
o.
Ono M. Wiltl•• S I. S<h .. , E. ,, 1'1.: D>o.-i. 01
e", ... f< Id,·. okobdi .. _ b,- ....... ",meo' ",Sloo
~olo "'N." """.".:I,h", « .. -<:on'tOl"";1 B,
M«IJ )16: ,77-8, .I 'I9! .
H"" ...... MC. M.""C R.A ..... ' DM . .,,,,_: ... I>,.".,..... 1pt".";n, in'" ..,"' ......pi .., noid 01 "..ito ..
wim CI<,,,f""'-I.k.ob d;o,."" ro- E.JI J M... l" :
Z79-U.I9$6,
H. i<h C.llonOO)' II .CiI»>C l.tlQI.: Tbe 1. ·3-3
"""tin in .... t>fO:Ip; .., o.id ... mut...- for
' ..........ibl ••
..,..,ph%pI>loi<> t'i E<tJtl
J M«I ))S: 9'l4-JO. 19%.
S,.;nhof!' II J. Rllc k.. S. H< .... ~ C. ".1_, At""
..'" ond «lilbi"'Y of P<' od",.1t>rp wave tornp ... ·
to ,. C... "f.Id'-I...., d ... .. A.-.h ro-.., .... ' l'
'6Z·6.19%.
<It: Si!>-. R, p,,'moo I. Hll<lloy 0, ,,"' : Sin; k pi><>"'" emi ..... """'PO'''' ,,,,,,,,,,,,,,,y ,1\ lite .... "' ,f,·
• .. ;.", of""w ....... C..... f.,d'·Jok"" d; ...... :
Cow r<p:trt>. a , Mod J )16: '9l .... 1991 ,
Hill A f . S""envorth R I.J";o<' S ... D/' In .... 'I.·
'''''' of ,&Ii ••" C"."I.I<I·/lkobdiou", .od a<1I<t
<II ....... wi" ,.,...il ~<l9IY .. mpk ••
I.. ..... ' 3Sl: Ill·9. 19II'J.
Le.T R M. B........ " Of. R"",."',,,, M L: N• ...,..
101",,1 m"if"", ,,,,,, 01111< O<Q.I,.,j i""'"'"""'ft·
, .. ncr .roo:l ...... 1"105): E'I>«"""" UC5f "'"
,. ... w of ,II< I;, ....... . J N......... <& f>!. 47!-95 •
I98S .
.~i_ D M. r."hOlI M: ~"""I it """if.... •
''''''oIlflV 'Df<C'l "",_ A ~. ' n ~ 101«1 121: 769·
SS.I994 ,
11<" .. ) R, K. ..ovtl' B. Po>t J O.,,"'_ l'roI .... ,""
","~;ro<. 1 ~""'''''''''''Iopo' ~ y ....,., ..... w;'" h••
",,0 ; m"mnodcr";"'1 .;"" ;n f«lion: A ... "w of
lite Ii".."". wi'~ • «pori of ..,,_ ""' •. A... 10'
l<,oM«I107' 71-17, 'W1.
Cin.:~10 S F. ROK."'''''' M l; U.. of cr .... MR
i""Ci .. ","i" ;,,,. i'" inn<t:Ooi.llnion>..., 10<10;.
no< ,he """" for biopI.r ; .... 105
J r«U, ...
tI,.".
""."form
1Itt"''' """"
"" . n
710·2<. 1990.
PO'''''',
o..i.- R E. Cnffi n 0 5; l'roI"' .... m,,'olo<.o1
1e .... """'.ph.lopothy ;n ... ,05 J AMA J6.i: 7~·ll.
'"'
In. WC_H. II W A; M.,......,"" "'"o( . ...... ond
I"r«,ooo •. e ... " ... p
<& ll) (9); 110.1'193 .
'~Nl I
N<.,.....
NEUROSURGERY
".
o.mtle'L M .J<."'. _ ",/w"",~_"
f"O,~,·,i
1.lfoc<>! '"'_~""""~1
~.
M a ndtll, d o ",,", aod ..." ... " po-lfIOipl<s ond
ptxti« or I. r<fll _ d.Is<......1.1 ...... 11 (; L wi
11<..." J E. 1«1'.1. O'Lu'th,I II...;.;.... _ .
York .411> «Ii,..... «I., 199~. Vol ~'PI' loIIX)-6.
Knopp !. B.Up"" . 8.S .... d..,.. '" \...,<>1: ""'"
,.
... ....
,...w
,"'..i..... hifOCOI l<oI<o<oc< pN.k>pOll>" C~ ' i<.1
and '''''OlI''p!'IOc 1< ...... ... . " "" .,01 )7- ).4.1·9.
,m .
8<"",
". 1'«0"'<),"
J ~.M .');. L: PlOIoot<4 •• ,..", 1...:1 po~;.1
AIDS_i.ooed II'''!=''' muU ,f<I<&I
N• ..,.._ ).8. 10000S. 1991
~.
Ell .. B. "'"""in I,Qok! R. nul., lJ ,.." "' .. i1 ....
of ... ,00·''-'&1<6 p,_,i., muM.foa) ieul oo.·
coopI1,IoPl'hy ",i,n combi_ ,.,i""",.i,al ""'rapy.
Ufl<t'
ISO. 1997.
JoM. D R. T...... , M. f"<l<n",,,, 0 :
in
,iI< .. ,.,,1
or "".I(lO)pl"WIi, byc.on<.""" in·
"',h lhe "".... ;m",_(", .. "", .. N •. /'I
En" J Mtd ll~: 1$69-92.19'1
~.
L.l.ho"S .... Hoo. E w .~ ..,,·7.. ""'rS ...... ~I'
In .....,.,of, ... "...""I....--..yu.mbjl ..poM_
pollidum : 1"'9lic",.,... 1"..6,,,,,,,,,,, IN! ""........
A.n l ., Mtd 109: 8,'-6l. 19n.
Ctn .... "'" one ... eon..", 11.""""""""" .. ..,..1"..
di_inl IN! " ..,r", .ypIoili, ,. HI V.,.f«otd po.
,iem, MMWR 37· 60().2, I98S
le.y It. M. ~ .... bIOOm S,
L V· " '.ro,ldiolo@icr."".nl" n ... lDS, ....... "'wol 200 <.0"".
AJ/'IR 7· &33-'1.1986
J..... ilIO. H.... IWO I R. t(.nn«ly C, "DI, "'Co
q.iml i-mmoncder",,<o"y
M.J1I<1i<: "' •.
onaJICO pou.m. of ",.i •• n"""'·. ",.", .. oh
polholot;ic """"I""", . Arob I'i.u .... 4}: 731-6.
1988.
Sodl« M.
N S.OO:lIwd II C: M• ..,".... of
i.'".,,«bnI ",.... 1. p.';"n" ... ilb HIV, ... f<1'f<I'poc'i .. ,tlIdy .,un d"""uion of di_i<: pn>b" .... QJ:\Itd 91: 20'-".1993 .
Scbwtilioof., B w. H....li.k J R.1'I><>o. 0 .... <1111"
I'ri".,.,., 1.,,..,,,.i,1 o;S lymphoma: Mil. .... nile ..
Ill .... AJI'<R 10. 12S-9. 1919.
'00 s., Y T. fl«lo"'" J H. Ooo>i. II. L: ""mar)' « n...1
11"'f'1>ooN 10 "",,",m) i.. _
(10:.
r><ie""'.y""'''''''' ... <li.",, 10"" po'hoioJ.,,1
.. "", ... ... _20; ~nI9~ .
C; roq", p. S,.,."i.1 M. VIIO L. ".1,. Epr.tei.·!h,,."", OS ........
1n.id from pot"n" .,',h
AIOS-"Io,"" "-'""'1 ly""""",o 01 ,... "'.. ".. . Of."". 'y>l.m, Laa.<<l l-<2: ·l 98-'O I. 1991,
102. Cohn 1 .... Modi'" M C.C...... W. <lDI.: Ev. I...
"o.ol.iI< pOl"y 01 """,i", ,........ , of •• ..,..:ocd
""o~",."n«pho' i'" in """' ... ..-i,h ,,,. ...
qui"" immoO<Joler""ncy.y""""",.A",J Mt<! 16;
Sll·J.I989.
10l, o..~ 1 E T, C,nNie 0 L. Dn-n"". J. Tho rol< 01
U<fOO<l<1k: ~1op'Y ,. ,.. ""OIl'''''''' or "IV·",',,·
"" 100:.1 In•• k:,io,\I, """ ..... '1"' 1 J(k 8l}·9.
",u k""_ p"'Jcpo I ~I .
"
,.'=
fue,'"
"'1"","""
"'''Of)'
"
...
Po"""
"
.,oolrorno,
.
",no!;
"
"". "",,1[""">01"1> 0(
46: m.S.I990.
C,.,.,.
..to""''"••
,m.
,~
,~
1.<', II. M. R.....11 E. y""lbl..... M. .. DI_ Tho . m_
cocYof im., •. &u.(Ied .",_""i.ln.n biofrI1 i.
,..,.ro""",.lIy .,"'_"' ocqui..., ......... no<Io:r..
<ie"'y.y,..), ..... ~ ... " /'I..., ..." ..yJO. IJ16.
90.1991 .
.'1icoloro ... . GoIo:<o M. )';0' 0. F., .. DI.; Comj>u"".
Owl '00"001 ...... y """
' .... OIOC"" br",. tuopoy; ' """.
'''_p«>m,,<d MoJ ... IOS puicnt •.
/'I •• ,.. <S: 261-n , 1997.
Noc_ I I. s... ..... e: L,,,,,diseaJ<. Ad v I., MN
00: 69·117.1995.
!'t"h... , ... R, 5,..", ... C: The "iad 01 ""'toIoJi<:
...,,".."' .... oI Ly.... d •..,.,.· M."''''~i1.'"''''1
......nri ••• "" ,.""",1""••,,;.;.. i'i....-olOU l', ,<7·Sl.
I98S.
I'Khn<,'" R _Duray P. SK.,.· C.""'I .. " ..,.., 'YO-
01.'.... '" "'-._ ,.oded
Sot,.
' ''.
'00.
''''
NEUROSURGERY
Coo,,,,':
",cU"i<.,!"".",.
"
Ill . M".!:..... II; LA : Cu",", .. " .. oIloborao.ooy diolllO.... for Lymo di-. • . Am J Mod 98 ($-0"'). 1G-2S.
199}.
I!' . Will« !I.SChe..... C. l'rr:ao:·M."'" V.".." 1." .. 1>"", I PfWLI<1'" 01'1"'<'('" .. uibod ... . I ""'p I>ctT<I.. ~ i. poo ......... ;,n Iymphocy''''
"",tunl'>'Id".I;li . ( !I"' n,.. nh ~
J I ..
f, .. Ok 1}1: JOoI·ro . 1986.
II}. H... il ......... u.l H.C",. 1>1 ... <>1, 1"""",.,,10""lin t\:InDtm.I li, ... ln "'n:b<o>pOn,1 ~" id or-.! blood
ov<r ,,'" «>.or><: of 1,"'f'I>o<:Y'''' ....... ~"'"l""
n""'h~ 'y1Idromo) . ..... i'i ..."' 1O: 1)7·~}.
'f""""'"
.
la ••
"
116. T,..,,,,,,,. d Ly .... _
117.
li S.
119.
,».
Il l .
Ill.
.... Mod lo" ... XI: 65-6.
1988.
S/a", "' C: L, ... "' ....... /'I Ene! J Mtd Ill . 58696 . 1919 .
Sot.lo I . F....,obedo F. Rodri' .....corbol • • " .1 ·
T..... py of I'" .",nym.o' ln" ",.'~i1 .,i,n
pruiqo.nl<l, I'i Ene! J .\It<! )I~; 1001·1. 1'$-1.
$oI<101.Goe'''',. V. ROJIIio ~ /'1'0""',.""""",,,
A ,.. .. ,1 .... ro<rioo._""O<\i ••• "" ""'i...
for .... .. ",h 10"". M<d lOS: 441_S.198}.
l.<t>I..." R. K.... \u t( F. M. I....... D, ..,111 · 1<...•
""'1"'''''KOOil: S""""I and """,,,,", ....."'own'
wilb pn.<;q,.o ... I. i'i ......... ~y II, .19-n .1 9 ~
wi l_ M. B..,... II. T.F,o«IJ .... <r~I ' Clo.al
• ••1.. , ... of tho ')'$Iioc<toO>i. , •• ".,.·" . l td ;m_
m."""Iot" ........ I.. blOl ,n ~u ...... illl ..."",,,.
,.....-a>W.. J Int..-. Dis 1/,1. 1«17·9. '99 1.
Elum •• 0 11. : C,.,k",,",•. I. I""IP"I oll.rt<·
...... uod Inn."'''' .. ''''''.r .... . .. ' ,..I .. ' ......
.»0.... , C"",P"1t<I "'_rapby.
hucloo. "'OC. " I< .... _._ 11. . ... """-,.,,,,.,
Yorl.193<o . pp 10J-12.
M""..., I. R"",rio J ", C. PmtdeIC • .,DI · mq·
..... of i..
",,1 .y~"'er"o ...
t>y .""'_ri« < l _.....y ,.,"' _ " ..... ,,.. " "".1...........:0 .-...I,.m, J 1'«....... 55. 9007.
SI. 1'/1' ,
L I .D-otoI<i. W R.l« C-S ... DI.: So.q;.
,II _,.,.,,,"'"' '" lJU,,,,,", of i.,,,,,.,,i<:.ltr
.,.. ... KOOi1' An '''\1'i1 010' , ..... J /'1'"""""&
60' 000-1.1984
Wood 1 H: Cornmon' on __ o.n.. J R.n .1" I'r"i·
_ , (py,&>:I"""""ol", """') In 0<,1.. """ .. ,I
",,'««oM8 1'i... """'I"',ll. 9S·6. 1938
Soc, lo J. P"noroo P. Eo.<ob«Io F.<rDl. Shon """ ...
01 alb<"" ...... iI<rapyl", "u""'Y"_ •. Al<k
I'l<00''' ~" 11 )(}.J. 1938
Mt<l I...... J1' 99·
Ilrul"'" ~."i<:
"'''-'''I.,''''
"""""'. 'f"'''
'"
1..,,,,,, di...... .. ",b ro•• ,o!
S,«tt" C, Soh<><o R T. Toylor '" Th«lmico' '''0"
1uI>O"Of l..l"" ... ~i' .. , M.I ..... /01'" I01 ' 7)~
31.I\lS7.
110.
for 0; ......
Lymed i...... - CorI_ri<," . .'.lMWR )7, '·). I9M.
III. 5 ,!'IILH: l , ... di..... OV"U""""'.s:C_"""
ou",. !loop Prort ll , U·S. 19% (edi",,;. ,).
Ill. W...... in A. Buj'" I) I. L,.... diH<>,,: A"'.' .... .,
I'IYSI. .. J Mtd.I9t9.ppS66,~ .
'1 ).
no.
12J.
,.
111.
"""."i,,"Ior ."" " ...
..."",:.0 ...
in("',......
'08. '9\lS,
' 2& , Coli, IIO.Corioo:i CO ..... o<I\Io:Io H R.<loI · T",,,·
..... of
''''''1 ... ywku ...... .
C"'"I .... p I'l<00' ....,.21 (1 1)' 1·1. '999.
Mo:C""" itl C F, l« C-S. Hoo<lt:n I; C,.,,,. «,,,i.
..,..... ... t<tJ _
l9; ~}<'9. 1911,~
C....... I", 0; ..... Con,"'" locally ""l",«d ......
""''''''''f""js. ~IMWR 'I : 1.... '99'2.
Ill. 101 ......1E. Mileldo,l E N. ""modi J • .., #/, Coo,,","
""""'ymi<: 1lnO•• """'..: C... .. pon . J /'I.u",·
..... 110:140-1. 1_•
1)1 . Clw<l S L.
M .... I.r..:, .... .. ;!to ..,.,.JlNXO<'
"". _Iomuon . .. ,... 0«1"''''' imm.n«Ief",irn<y
N !;o, l J ~I 'd l ll : 7</'1·9, ' 989.
".
pi'"'''' "''''' .•'''.....
S."""
'ynd''''''''_
12. Infection.
m.
"
'"
'"
t..>oS.~ w.l«C ....... u .. tmlJ i.lan:I .....
A ,omp"i""" ofM><""k""
"""'.C""''''' < r y _.1 m<ni.,.i •. Q J M.d
",", l41·~l. ZOO,
, _ M. M,R""" ,. Afeh<r /; Sl<roid "'.,.,.,,,,,
,... de ...i<nrio1o i. <lJ'P1O<'«<~' nnfo-""'~ • •• n·
.,~ t<''';; """i.",,, 1'1'.<0100" 6l: 71)". 2004.
Sao! M S, ......... o1y WO.CIw<IO A. ,,01. c.....".ri_ of amphDlori<'. a ... ~Ir n._1e In II,.
of""'1< A'OS·."",.. ,,,,, <rypIO<>O<eOl
mrnin,i" •. Tho NlOl mJ'CO'" <lWy ..... P _ tbt
AIDS ,"okal ' rial'I""'P. :>I E .~J M"" )26 m .
8),9. I'm .
o.M'", OW.A""''''''', II w. ,-<.. I, 8 H." 01..
EIovar«!~I<b""", .. , n.od ""' ...... '0 "., .....
"hlr " , , _ . 1 m<n' .. i" •• nd ooqoi .. d
""ro:;"fIC)'
A'" J Mtd 91 Of: 161-11.
1991 .
""" M K. H""",.. "", O~.Be .... " I E. T... ,"" ..
o(hrJ.ot<pIo ..... ~ "'c.,pIO<OC<oI m<ni. ·
' "" by ... 01 ,hu."., . Cli" (~I.. ' Pi.< 2' (}); 629·
""_it ""'"'''£"'''
'JUl"",.,
,,,,,,,.no-
.'nOIO.....
'"
'".
33.(~ .
HO(hMC. Tolly P W.OoOof"'1 E W. lIsto(<< .. Iloood _ " i. ".,,,.,, "';~I ""'lui ....
,_ _ roc_, .ynd""". "~h <~pto<o<"'l
"",",.~i", >rid _,,,,11at>1e ,.'n":r,, ...1hyp' .....
.ioo1. J 1'1........ "'41 . IllO·} . 1991
Uri"" PC.Uon,c I...C"",,, W N. "Q/" U.. of
......,..,u'-ri __., .Ir •• " 10 ,.....""",,"oI'. blt
~""' .. , hy",,"".""" i. ".,,,.,, who 1II'«l)'l>
Iry<kl>«ph.llu, Clio
1.'«1 DIo ).4 (11); EM·8.l'Xl2.
Cohill 0 W: ).IO('Iioo1.of,'" "',.. COOlOmp~.
' '''''' 1 IS: I·,. 1993
B"., A $. OJ<m,,,. ~ G. S..·"". M N. <I 01, Spl.. ,
,p01utll .10«.. . 1'1 EntJ J M<4 1113: '63-1. 1975.
N...
E S. Ril_i O. S",""ifcwd H.... ,"
Sp,,,"I,pi~'nIl
A ",pan 0( <j) " ... "'" 1<,,,, ... Su,,,N<~ 18: 12-S-31. 1991 .
0.,-,...- ~ L. H""", .. 8i. U~" cl",i"" .pOd ...1
-...., lS<OSe$ ond ,.,jc.,. oflloc ~"'''U" , It••
I...", [)is g. 2!6·~.19S7
eo".,. WT.k.""" 8 L.A",,,,·H.,..,,, S.<101.:
Spi ... <fHd_1 oboa.I: Cli.... , ".......... ......... • t<", .... ..-I""O<o<n<.s... lN--.I ~Ji . ), )600.1,:
d"",,";""lll.200.S,
HI •• in 101 L.I"min<ki H I .Roo.I S. <1<>/' Spr",,1
<pidufll oblCUl: A "'n·],<&! ",,"pcdl". 1'1........
........1 27. 177-1<. 1990.
sp...,..... R,FonoIlt.().F.ib<IM.<lQ/. ""'"",
• .-.; ..... pr • • 1<"'d .... c~· cmo, CI;."" ..d <Om.
""I<d......,..,phy I. ... ~ . Spill< Iii; 1106-9. 1991.
B.ow .... I. 101<)<" R. i'yOp.I< lof......... ohll<
opi ... ... iof ...
Ill. 296-lOS . I900I .
Ru.ocU N A. v"'&h&n R, M<><k) T,.. SpirW <pidu.
,II ;"f«,ioo1. COft J N. .. 01 Sri 6. lZS·a, 1979.
Hc" ...... A'" N""nJ!I<fCIolo.. ,prnolcpo<lw.l ;.1«·
110... 1'1 t:.w J 101 ... 1)9: "S·SO.I""" .
K"ppel B S. Tll<:h ........ ].M..,' .... i JR . .,,,,.,
Epidu ... 'pi.al Ww'" '" 1",,,,,,,,,,,,,,,,, abo.·
• " . At<h "..ouoI . ,. 1131 ·7.1988.
AOdeI·Mapl II A. K",b HIM . Sp'.'I.pid"",1 >b"""... ~ .. . pi"'"
A " ....... 1< .."'''''''' .
1'1... ,,,". ,,,, ,, 17: ) 10).1. 1990.
Loorit: D I. f.;m:y H 8 : Epidur>l ........ /011""',"1
"".. I ... >Ih«i •. ,."..."" ""01,S7: 1' ,·). 1971
S''''''l W E, E!>Olu ..
i• ..., wi,h <podol .
... 0.. 0.:«" ..,100: A r= ."".. , ltcpo~ 0(,..., 0•• •
..... ,,~ MOr4d1y d<l'ytd """" ..,,_.
broop,""
..
,.
,
""".",.. "".,.Jitj ....,,""",
101.
1<2.
1<1 .
'" .
'4).
,~
141.
,...
'0.
,
lSI .
ba""
.\000<,,,
,.pocc.S."",
'i<'"
,.
,.
,ro.
'"
IS).
,.1I«<>< ......
'"
",. °
,~
'"
12. lnfe.:t'ollS
'n'I>J:'.'
s_.
,w.
F S. Oilloo W P. S,inol ... Ol.nJ oboa ..:
E.. ,..."" ... "h«>l>ltlll..._
M~ 'mos' ",.
AJNR 153: 1011·9). 1991.
K...... , H.C)!, Y I' .Loe$ H: ,.' ..... ,.. , .. r. A CT
nodi'l of<piolonl abote>• . A./R lSI : 1111·S. 19U
'-<,. D. '-<00" F. Yi .... C, .. uI, 0<0<.......:1 """'.
~~, f,- x.,., ,*,.,n., 09' .. I.piof ... , oNe ...
""1 """'''''''''' _ . . . , . O<od _"'Iit:., ,... ,"'<fI' 10"""'" pot", .... A",,!'In'" 17: )50-,.
""
,-
'"
"'_< """,.,.,.!
'M
V.rner E F.MU>lw:rO 101 , Spinol cpidom .-...:. .. ,
M«l Clift Nonh Am~: 175-I\oI.198S.
C"li.. 0 D.O-.. O J.Mcwr., ... " M.Chot!Ji".
,""""". I. "".. I.""",") ob.,,..,, A "'lI<I" 01 29
...... N.u .....""• ., 27, Id~·9:!.I990 .
1'<,.;.. C [.I..yoch 'C: Spi,.,1 """,.nIl .\rO«-Oi: ... "
""y... of 14 <...,. 5<0", ..... roI 63 S.P!" I: Sl6-
'''.
'0.
'"
•. =
Sc_O.I.",- H, no.b . ..... .p;n.I.
....Ub • . . . t _,O"'''' ... S''''non.1''ew YorI. .
19'11.
W.I<I,or<' f A. V. .. , H: o.o_<litio:T1><paor
N htJJ Moll J(l3: ;00·71).1980.
Hoi ...... R S. 8,"'-1;0 R: o,_]'<I~"" ha-c1n "".
""". A.A In,..,. M'" ?S' 691--6. 19'1 1.
CMoill D w . Lovc L C. Ro<lo.i .. G It:
__ ,...I;'I.of oho: "trw: I. "" cl<letl" J No._fll
14: 878.16. 1991 •
Ei.mon, fl._I ..... H H.Scw..Pl. .. "'.: i'yoJI<.it: lind I....,"" ... ",bnd """""',-.:"'" w~~ plnly.".
J _Join, SUQ6' .... 1~29 . 1981.
a..a. 0 R. 8 .....·Za...""ill 101 B: CT 01 ~ y. .lC
'fl;"" inl«1_ N<IlI"Ondioiou 11. 111 ·7. 198'.
Sopoco F L. M""..,."..n. J z:' 1'y_.it: "".... "
o.....m]'<l~il: R<pon 0( ow. ...... rod ",.it:w of
II.. 1I,..onr,. . ~", ' ofo<' Di> I: 1S4.76. 19'19.
S~ .((l S. F.""",, 101 0.11"""'-.. C H: M«IkoI
."" .......1 "'"",,"'0' 01 PI",." it: .". """P)'<>""""'11odi.. ~", Parll. C.o'""P N... .....,CJ:
26 (191: ) .~. lOO4
Mollie MT.F.,,'itI 0 H.PJOino Ow ...... ,: vrn ..
bIOI """"",)<1.'0: A.... ' ..... ' "''''I MR Itodiololl' 1)1: 15J.t\6.I98S.
R.. " S .... N<lIU.Sc.,.,'WO." 0"
m.....,",," of,_it:."" Iu,"b .. y<n.lnI
oWel,,"'rod d, ..
A""" .. 0143 ""'"
....'i .... 'U,,"'II ~ ",:>,tdl>"''''''' 1'1 .... ...,.... ,
38, 9:!6-1l. 1996.
Shl() S.fo~linv 101 0. B"",,!>ou,C H: M.,jiool
..,d ."",col " ' _..... dp~.it: "'" ~
,..oo4y!o<li.<:i"~ Pw: II, C""'rrnp ~ ....
.... ,26(10): I·S.2000 .
Itothrnur R H.So- F A.(.....~ Tl>o 0f>In< 3nI
«I .• W.8. SOUndc".I'hiIod!IpI1io. 1m.
Ki"';"' W s ... , ,toINrcol<hlJaf,M>I..II • ...J,pi"'.
I" Nc .... """'. E<to-'ard o\rmld. London. l~. Vol .
I:W,7SoSJ .
""" ...... R..."",h Coo",,1
Pon~ "" Thbo,_
""to<.. 01,10< Spi.. ,Coo,,,,~""
.. ,1 ....... .,,00.:_0.:"'" ;" ,II< or"tnolo!ooy ""u·
..... 0'." ...... ' .ut.:.. uro..., R<,.I,. AI (/om: , . ... of
..
'0.
, o!I:<.
'w.
111 .
'"
I Jl.
114.
Pyop'''' ,...
".1<
17'.
176•
"i. ," ""oJ,,,
'"
111,
A~,..,90)--6.1991 .
Be ....... I. WOld ER . M<y« j D." .t.. Epido..1
......, ... "'" v.... bro'_m)'<,iti. 100Iowi ", .. " ..
IIwnbar_",,. •. Podlalries n " 7SoSO. 198)
R.. 1... 101<0.-."" I M .Millt'C A.«<>I.: SOfJ'<a1
""...... , oftbt _ _ .p;.. l cpidurol ....
ICUI, S. ", N,.<OI 37. 17<·9. 19n
K.. r..... D M. Kop! ... j G. Lio",_ 'II: 1.1«<.,.,
POll M' 0.5><0.00'""'" ~ M.t! oI.; Oo4oli.i·
.",.. nIwI«<I Mil ,•• "',,' nf«''''.J C.... p ~, .......
.... T"""'J' , •. 72'·9. '9!'0.
POll M' O.Qoon«. Il M. M,,,... I... B M." "'.
Spi'" ,.1«1;,,0' E,·aI ...", ... "h M~
Onol
i.,,",,,,,,,",, .Ill,,,,,.nd. Rodioloc1'<fl; 76S·1 ' .
162. Moml'Ol*nlT I . lto><p, H. """",,' a T... oI ..
S _ u « O"< .. "",.. of,pi"'<J>~ ,.fo<,ioo1 •. J 1oIn ..... ,'" 2(18·10. 19t'I,
11.0"'1"" WC ....."'" NO.£I .. """ P W. M..... 'it:
01>< "",.",...,i«_... ",
o(;pin"<pO<!",.I._, . S ~ ... N_J<l : ~.ll.
"""""0:
'R
i. ",i.," .pid.ri! .......... . Nturolo&l' »:
8"·~.'95().
' S1.
,~.
,~.
"".""",.;<.'
""«>-
,<11"
"'0<1<,",
"'.. .,,"""'_
NEUROSURGERY
..,<><I, .. Komo,J _J.oi~1 s.,'1 7SB; 100·1.
1991.
l SI. SoUl • .., C I. 5,,",,,,,,,,,,
_ , n", .....
J",\I"
~
E' o;.k ....«';O"'.owI
l"' :65~·S. l !164 .
M ol, ~ G M. M<C"""ocI P: M.... ;C ....... or.pin<
""" I.......... lnl di'" 'P"" mf..,;o. CO . ..... p
Nt .......... 10: ' .(;.19&1
Ill. K. "",Hll S.loc h "" JW .J<f.miolllo. .,t>I" i')'<>.. " .. ;~r« , ,,,,,, oc<u~poimorily
Inl d ...... J 80.. Join' SUfi ~l B . 693·1". ''713
, •• . _ .So.o..;.oO.DiNTS,n.ol.: "-of><'"
t,.., d,, ~ "" : Do~,,,,""h;'l . .. MM ,,,..,,°1(,od·
'"I'
1
dill< !pO«<Il..., ...
R..s .. ,"l!)' 11"76)..11.1992 .
IS~ . Kop«k y K K.Gilmot II. l.5<0" 1 .... ~141 .. p;,f.l1.
ofcr '. ~i",..,.;.or .....i,. "'.........,.....,.11
~1-«> . 19a5 .
186. Wf...,1 M. w•• ",,~. HNlkt E H: Tul>o"," ",",
112.
I. I.,.".,.,"...
j,
f""" _ ... ,.,.""",>1, ..
NEUROSURGERY
spon<I)'l;';'''''''k'. J _
JoI •• s..,,61 ... : JOOS·
II. I'/I~ .
I. ~' J,"I' C E. Willie" III .GoIla II ... . ., Ill" """.
.....-..t
1tlle.,....I'1.........
,u'l"l'J' I}; 371-6. 193).
188. 1.." ... E.l'lidoenV ... Il . Il...... LG: """"""' ..
pOI/OI><f>lti .. di"'~i ..... ",'_ I~ ...... yof 'I'
U1U . ... ct.
S<aJod 61: lOS·,. 1m.
IS'). o.....Z L .Sc ~ ;_ 1 S.O,/T".., II. H.IIIII" In"Mf'
Ubnf d"k·.po<:< ;.f«,'" .1'Ie« h)'...".,.;. ;np:.
'ion • .o.JNII6: 5H. 19a5.
190. Fouquot B.Coup.!" P.lo" ;'" F.,,~I" o.",iti..(I ..
I.","" d. ", ....J<>')'. !'<"u.nor -0"'1";'; - ,,'" -.. p''''· ' ...-.Splno 17: JS6-I. 1m
191 Th<1_ U . b...... S,Qu""" ....",orC.""""..
l"<I«i. 1e..I, oncI'<ylt..o<)1< "",i_.",... _ of·
." 'pulS! ,",£<,} . SpI ... 11' 0100-0 , 1m.
117 .
"I'<'", ......
on"""
12. l nre<:tions
d'" ........
13.1 .
Seizure classification
Dellnition of II .;el lU",: an abnormtll p$ro~yamal cerebral n~uron81 dischaTge that
reauiu; in plu ralion of seMation. motor (undion, behavior or t<>n~jouaneu. Seizu~
Olay be cJa!lSified by type, etiology. and by "pilepti~ ayndromes.
C lass ificatio n o f mllj or se izure
1.
typ{!. '~
primal")' ge n e ralized: bilaterally symmetrical and synch ronous involving both
""rebral hemispllerea 'I the onHI, no 100:111 onset. ~n9dou.ne&IIOS I from the
lta rt. Repre$<'T1ta _ '10% !If all5llilurE!st
A. generaliled Wni~-cl(lnk (GTC) (nee: grllnd.mlliaeizuret, ~Ilerali~ &eei.
zun! that evol"". from IDnic to donic motor activity . Thi, iSlllpecific type
lind dOef tiQl' include plIrtial Hillires thai g<:neralize ~~darily
B. donit &eizun!II: fairly symmetric, bilateral synchronous semirhythmic jerk·
ing or the UE & LE, usually with elbow I'!u.iOI1 and kilO'" exlwaion
C. tonic seiures: sudden allstained increased tone with" ~haraeU!riatie guttural cry or gn.,"~ fI.S air is foreed th rough adduc~ vocal cords
o. ab6enCf! ( n~: petit·mlll 'J'Iisure): impai red conaciOllll1'leSS wi th mild or no
motor involvam~nl (_ ~Iow)
l. typical a~nte'!l
2. a typical ah&"",cea : more heterogeneous with mor~ variable EEG p.~t­
!.I'.m then typical o\lsenct'. Sei~u ..... may Il18 tlonger
E . my~)onic seixUTes: .hocklike body je rks( I or more in su~"fon) with gen·
eralized EEG dilOChprges
F. 1I!'miesei~u re6(AKA ut ~tic $eizu,ret; or "drop attacks").: s udden brieflossof
lone that may l'8 un falls
2. partial Inee f~allei •. ure): implies nne hemisph ere involved Ht nnlel. Abou157'i
of all sei2uretl. A new onlle.l of partial se;:ure repreent.! II a!Nclura) leiion ulllil
proven (otherwise
A. simple panial.eilu,.. (no impairment oroon.dousneul
I . with motor signs (including Jacksonian )
2 . with stlnliOry . ymptomli (5peda) sens<>ry or .omatoienaory)
3. with ~utooomic signa or SymptolliS
~.
with psychic symptom. (disturbance of higher cerebral func tion l
8. ~mpleJ< pArtial .eizu re (many used to be. dasaified lie psychomotor&eizure,
often attributed t o temporallo-l.w but the)" elIn arise from any cortica) area):
auy nlUl rntion ofconaciO\lsn~S8. usually LOC ora utomal;smR (inc1udinglip
smQclti ng. ch ewing. Or picltirlg ..... ith the linge"' ) ..... ith s " tonomic eUrA (US".
aUy nn epig8l!ltric rl.ing s.ensationl
I. .im ple. panial 01l6et followed by impllinnen t of eonsciousnel!Jl (may
hBve p .... monitory aura )
B. without 8u tomlll;sms
b. with autolliatiams
2. with impairment orconsciousnesa Nt onsn
a. without automatiSml (impairment ofoon>IC;Ouane&1 only)
b. with automatismll
c. partJ~l6eixure ",ith secondary gE"rlcralization
I. .imple pIlnial evolving to li:en~ ralized
2. complu partial evolving to generalized
3 . simple partial evo],'; ng to compl"" panial evol~ine to generslized
3. unclassified epileptic 6('izures ; ~ 3% ofal1.se'tures
ClaSllificlltioD by et io logy (an d so me e pil e ptic ..yndrome9)
Thi5 liat t. nnt " lllnclu$;ve
( ~rererenc:e'·ll.
13. Seizures
NEUROSURGERY
s ymptomllotic {AKA 'secondary1: seiwres of known etiology (e .g. CVA, tumor .. )
A. temporal lobe epilepBies:
1. mesiallemporal .der(lsis: fI'" bfolow
2. id io pathi c (AKA 'primary"): no Wlderlyingeause. Includes:
A. juvenile myoclonic epilepsy: Me IH:low
3. c ryptogeni c : Seizures presumed to be Bymptomatic but. with unknown etiology
A. West syndrome OnfantHe spasms. BJitz·Nick·Sala3m Krampfe): sl!e below
B. Lennox·Gastaut "yndrome: """ bfolow
~ . special syndromes: . ituatico-related seizures
A. febrile seizures: u" p<J&t 264
B. seizures occurring only with acut1l metabolic Or to~;c event: e.g. alcohol
I.
KEY dist inc tions (having thera peutic implications)
In generalized tonic-don;c seizures, primary generalized
generalization (o ften_le..., l On!let may not be observed)"
In ,ta rjllg spells: abJlence VB_ complex partial..
V3.
pa rt ial with serondary
EPILEPSY
~: '~.~";-~'~~~~~'~'~_~.;.~'~"~m~-
leriu-d by recurrent ( 2 01 more). unprovoked
A disorder, not a . 'ogle disease. Characseizures.
••
ABSENCE SEIZURE
Fonnerly called petit-mal sei~ure. Impaired conaciouSJIe8s with mild or no motor involvement (automatislIU occur more
commonly .... ith bursl.8lasting > 7 secs).l:'ill
post-ictal Ccnfusjon. Aura rare_ May be induced by hyperven tilation x 2-3 mins. EEG
shows spike and wave at exaotly 3 pe r sec_
ond.
,.
UNCINATE SEIZURES
Obsolete term : ' u"cal fol.8". SeilUre50riginati"i in the inferior medial temporal lob<:-.
us ually in the hippocamp91 region . May pr(l.
duce olfaotol')' halluc'''ations (kakosmi a or cacosmia: ~he perception ofbad odors where
none eKistl.
,,
M ESIAL TEMPORAL SCLEROSlS'"
'the most comma" cause of intractable
lempo rallobe epileptly_Specific pathologic basiA: hippoeampal aclerosi~ (ceU IOS8 in hippoc_
ampus on "ne side). Characteristics are shown
in Table 13 -1_For differential diagnosis , Ut
pog~ 938.
Adult seizures are ini t ially responsive to
medicallherapy but become more varied and
refractory_ and may respond to seizure our·
gary.
JUVENILE MYOCLONIC EPILEPSY'
Sometime!! called bilateral myoclonus_510% ofcase~ of epilepsy. An idiopathic gener-
epilep.y $yndr ome with age-related on_
$et ron5isting of3 seizure types:
t. myoclo,,;cjerita: predominantly after
waking
Z. generalized toni~-donic seizures
3. absellcc
EEG -. poJyllpike discharges. Strong
family history (IIQ me atudiu showing lin kage
to the HI..A region on the short arm of chromOllOme 6). M08t responsive to depakene .
ali~ed
NEUROSURGERY
13_ Seizures
WEST SYNDROME
Thi. term II being used JeM frequently as it appe.... ootto be. homogeneous , roup.
C]"s.iCIIlly _seizure di sorder th ,u u",'ally appeart in r.rttyur of life, and fIOI:I, i,ts of,.,..
(urTen t , ,ron nexion and occasiona lly e~ten.ion of the trunk and limbt.(maslive myoclo(lua, AKA infantile spum a, AKA salum "ilUTti. AKAjacklO1ife apa,m.). Seizure. tend
todiminlah with aile, often aMting by ~ Y"'. Ulually .uocialN with mental retllrd.tion.
501\ may develop eomplex -parti.l seizurN. lome orllle relt may devel~ I..cll1lox-Ga.U"t
.yndrome (Ut bt:low). All .uoclattd bra in IHion may be fouod in lome.
EEG - the mlljonty ,how either intenda! hyp..rrhythmi . (hIlP.piketwave plu.
slow wave re,embling mu.de artifact) or modified hYPIIllrrhythmi. It OfOMe point.
Ulually d ra matic 'UpOn.. ohei.u rel and EEC findinp to ACTH orcorticotteroida,
LENNC)X-GASTAUT SYNDROME
Rare eondition that begintln ~hildhood u atonic "i,uru{"dropalUtC:Iui "). O~ de·
velops inw wnic sei~ures wi l h menUlI retanlation . SeizU"'II~ ofttn polymorphic, diffi ·
cult to treat medk& lIy, aod mllly OCeu r D.I ofttn a, 60 per dilly. May al", preMnl with
SlatUI epilepticus. Approximately.sO'Jl of palient.s hay. reduced sei,ul'e"l wi!.h v.lproic
acid. Corpus callosotomy may reducelh. number of.tonic seizurft.
7000'5 PARA{. Y515
A post-iclal phenomena in which there i. perti.l or tot.] pIIr.ly.i. ulually in ......
inyolv~ in a partisl sei,u~. More COmmOn in pati" nls with ,tructu ral lesion, u!.he
source of !.he seilure. The pllre lyai. uluaUy resolvel.lowlyove r . period of.n hour or 10.
Thought \.(l be due to depletion of ""uron, In !.he wake oIthe exten. ive electrical disch.llrJ·
ell of a .. hun. Other limilar phenomena indude post-itt.al aphuia.nd hemlanop.i • .
13.1.1.
Factors that lower the seizure threshold
Factors that lower !.he seizure !.hreshold li.e. make iteu i"r to provoke a .... iture) in
in dividual. with or without II prior seizure hiawry include many itema li.ted under £Ii.
ologier of New onset Huun, (5ft boolow) aa well U:
L sleep deprivation
2. hyperventilation
3. photic stimulation (in some)
4. infeclion; aY' t.emic (fellrile 8I"i1U,,". sec ~ 2(4), CNS ..
5. metabolic disturbances: electrolyte imbalance (especially profound hypoglyce·
mia ), pH disturbance (especially alkalllOlli,), drugs ... (sn bool()&:J)
6. had Ino urn.: dosed head i!\iul')', penetrating t rauma (_ page 260)
7 . cerebral ilChemilll: CVA 15ft bt:low)
8. "k.indlina": II concept th.t repeated seitu r" may facilitate !.he developmentoflater leilu"'l
13.2.
Special types of seizures
13.2.1.
New on set seizures
n.e 1Igf! .djulte(! i.M.i!1tntt ofne... onlel se11UTft in RochnUr, :'>linne.ata wu 44
per 100.000 penon yean'.
E tl oloai"' In ~tienta pretet>tifl( wltb a firtHi ...... ltu re. etiologiell incl1.lde
(modified'):
]. following IWurolOJic luult: .i!.her acutely HA. < I week) or remotely I> I week •
• nd ulually < 3 ~ from illfull)
A. cenbrcrvQCu lar .ecidenI ICVA. or I tl'Ol<e): 4.2'" had. leilUre wi thin 14
dllY' of a CVA. IUak incnNed with MYerily of , t rok.'·
8. heed trau.rna: cksed head i!\iul")', penetrat;na trauma Uft ptJIft 260)
C. CNS inr~tion: meningiiQ. ce",bra] .b_n•• ubdural empyem&
O. febrile .ilUra: _ po,. 264
13. s..i1UI'ft
NEUROSURGBRY
E. birtb 8!iphyxi<l
underlying eNS abnormBlity
A. conpnit.al eNS abnor()"lRlilieil
B. deg!!n!!rative CNS disea5l!
C. CNS tUnlOr. me13sl<ltie or primW")'
O. hydrnc:epb"iu l
E . AVM
3. acoWi SYltemie metabolic diaturbionoo
A. electrolyte di3l!rd~rG: Im!mill. hyponatremia, hypaglycemia tt!$peeially p_
Cound hypogl)'t"elDiaJ, hypel"ClOicellli3
B. drug mlaled, lncluding:
I , alcohol.withdrawal : JUprJgt 261
2. roeaine toxicity: _pagt 152
:I. opio;oid s (narcotical. principally a&aociatM with the following:
a . propoxyphene (DarVllnill)
b, rneperidin('.(Qemero)®l: nlB.Y alw c~use d~leri\lm
~,
the Itree! drug comhination -rsand blues" (pentawcil).8 \Tal·
wlnill) • the a ntihis tamine tripelennamine)
4 phenothi a1ine antltmeti<5
5 _ with administution of nu!ouenil (Romlllic:onill) 10 lTelll beuzooiaz·
epiru= (BDZ) In"erdose(especially wben BOZs al"l! taken with olhers!!i·
~lIre lowering drugs luch as Iricycli~ anlidep re ilSanLs or eocai ne
6. ph,m~ydidine (PCP): originally u!red D.$ an (UlimallTllnqll ilizer
7. cycl""JXIrine: elln affect Mg" leveL.
C. eclam/lSia
4. idiopathic
2.
In 166 ~ patients presenting loan e.mergency depar1.Olent with either a chief
romplai nt of, OT a discha rge diagnosis ofll first·timll5l!izure'! ;
1. no were found 1.0 e~tllall)' hive either 8 ,"""UHent seiz ure or " non ·ida! event
2. of the 51! p3ti""ts actually thuught til hve had a 1in;t.-\imeseizul"I!
A. 71 % were fabrile eelruru
B. 21 '10 were idiopathic
C. 7% wltre "sYn:lptomalk" (hyponatremia, meningitIs. drull intoxiClitiun .>.)
In II prospeetive ~tudy of244 patientf with II ne"·~D.~et unprovuked Hi!ure, /IDly
2770 had further ~ei%,," a d uMng follow-up"- ". Recum!nt Hi zUJ eI wera more common In
",th
a family $l!"i~u .. lU! tllry. ~ pikl!:-and- .. ave!llln EEG, or . hist.ory ofa eNS
poIuentf
insul~ (eVA. head iojw:y •.. ). No p•.tfenneizur.... rree for 3 yeaMi h ad a recurrentt'oFollow·
ing a second seilure . the risk offurLher seirurM W84 high.
EVALUATION
Ad ul ts
A new-oosel &fIlilllre in an w1Jd.I in the absen ce of obvious cause (e. g. olcQhol with ·
drawal) ~hllu ld llrompt a search for an u.nderlying bull/ the OnMlt ofldiupat hir ooituru.
i.e. ~pileJ.lIY, i. most common bero"! or durinsad ole8cence) . A C1' or MRt (withnul a nd
wilb e nhance!oent) ohoold be perfnnned. A sY"t~mi<:."orkup "iIo uld he doo", to identify
the pre.en~(lrany faCIQTS tis1.i!d previou aly (~tt abo"'). IfaU this ii" negative, then o.n
MRI s h,",ld be per;o""w ifnot already done. Ifth." I' nerst;v •• 1&0. a ~PI'at s tudy (CT
or MRI ) s hould be done in - 6 month a and ftl I lU,d PQ6IIibJy 2 yea" to Tule-<>ut a tumor
.. Mch rolShl not he e vilienl nn the initiai u udy.
Pedi a t r ics
Amonr pediatMe patienlll with Ii.Mlt-t;me 8eizul"U. laboratory and rlldiologic evalu·
BtionB were "fl.en «ISlIy and not helpful". A detailed history and phyllioa l ~lWJn wert'.
more helpful.
MANAGEMENr
•
MpnllgemenLofan aduJt with ~he n\!W OIIMt oridiojlSlhic: l e'z\lr1l.0 e. nn abo"""al •
•ty fouod nn CT or MRI , 00 eviden«! nfdrug wi t hdrawal) la oolltl"OYeraial. 10 one s tudy.
an EEG WILf perfo""ed. which ifnnrrnBI wa~ followed by 8 sleep deprived EEG with the
foUowlng o-beervntioM" :
I . there. ill IUbotand91 interohl<l!rver variation in interpret.ing SlIth EEGa
2 ifboth EEGs were normsl , the 2-yr Tf!(:\lrren~ Tille-of lIl'izures was 12%
3. if oneorboth EEGs showed epllepti~dilcha'1res. Ihe 2· )':" recurrence r~(t,waa 113%
NEUROSURGERY
13.
Sei~ure.'l
'"
4. the prelence of nonepileptic abnormalities in one Or bot b EEGI had a 41% 2.yr
recur~nc. rIta
the I"«urrence rat. with focal epileptic dillChargea(8 7%)waa Ilightly higher than
for generaliled epil.pt>C: diachargl!8 (78'J\,)
The.:onclu.ion ia thit BEe. thu.obt ained hlva moderate predictive value. and may
be factored into the deci.ion of whe!he r or not to t realluch sei!ur" with AED •.
5.
.
I
13.2.2.
Posttraumatic seizures
1 Key pointa
2 categori": ear ly (,. 7 dayl) and lote (> 7 day") alle r head trauma
• anti.:onvu laanta (AED.) may be ulled to prevent u.cll pasttraumatie .ehurea
(PT5) in patien" a t high riak for Ailurea (fH ~:Itt)
• prophyl actic AEDI do NOT reduce the frequency of late PTS
• diacontinueAEo. aller 1 week except for caAI meeting.peci roc criteria t.... ,..Itt)
Postt ra umatic aeilurH (PTS I are ollen divide-<! (arbi t rarilY) in to: udy (occu mng
within I week of injury) a nd late (thernller)" . The~ m~ bejuttilication for a1.hi n:l eat. gory: "immediate". i.e. wi th in minute. to In hour or.o.
Ear ly PTS
(:0;
7 day. a fte r he ad t r a uma )
30% incidence in IeVere heed injury ("leve.e" defined .. : ux: > 24 hra, amnHi.
> 24 h.-s, focal neurodelieit, documented oontuaion, or in t rlcuni. l hematoma).nd
in mild to moderat.e injuri... O«un in 2.6% of children < 15 yr. Ig' with Mid injury
cauI;ng at least bri efLOC or amnesia".
F..arly PTS may precipitate .dverse evenu . . .. rNult of .I.vation oftCP, .It.e .. tio ...
in BP, ch.nge. in oxygenation, .nd U«Aa neurolranamitt.er r.leale".
-I"
Late o o set PTS (> 7 d a y s afte r bead lra\lma l
Estimated incidene.. 10·13'1> within 2 Y"' aner · signif,c.n t" head trauma (includ..
LOC > 2 mini, GCS < 8 on admiuion , epidura l hemat.om •... ) for alL.ge ftO<J(»"" ' . ReL.
ative ri . k: 3.6 times control pIl pulation. Incidence in.leYt!ll! head injury» moderat.e >
mild".
The incidence of early PTS i. higher in children than adulu, but lat.e "';&urea are
much Ie.. frequent in children (in children who have PI'S, 94.adevelop them within 2~
h ... oftha injury"). Most patieou who have not had a seizure within 3 yr. ofpenetrltinc
head injury will not develop leizures"'. Risk of lat.e PTS in children don not appear related to the occurrence of earl,. PTS (in adulta: only true for mild injunea). Riak of devel·
oping late PTS mly be higher after repeated head injurie •.
PeDe trating tra uma
The incidence ofPl'S;1 higher herewith penet ra t ing head injuries than with closed
head injuri" (occura in ~ ofpenet rating trauma C86e5 follo.... ed 15 )""Sf').
T AEATMENT
A prosPfICI.ivedouble blind . tudy ofpal~nlS at high risk ofPTS(exduding penetratinc trau ma llbowed a 731110 reduction ofriskofu.w PI'S byadministerinc 20 mglkg load·
ingdoseofPHTwilhin Z. hraonnjury and mainlaininghigh lhe .... pel::tic level.; but aner
1 wef:k there wn no benelit in continuing the dT\1g {bued on in"'ntion to treat)2". Car·
bamazepine (T~to~) hn also been ahown to be effective in mucing the risk of urly
PTS, . nd yalproic acid i, currently bei"i Itudied '·.
PhenytOin ha . advene cognitive effectl when given long''''= as prophyluia
&(ail\.lt~.
TAEArMENr CWIOELINES
Bated on .vailabla inforTl\.ltion It« obouel it appeara that:
I . no treatDlent lIudied effectiyely impede. epilep~nes;1
2. in hilh·ri,k patienta!He' Toblf 13·2), AEOS mUCH the incidence ofurl:t PTS
3. however. no .. tudy h.. ,hown thlt reducing early PTS lmpro-.·es outcome
4. on« epi!e!»y h .. developed , continued AED. re<lucea recurnnce mlUr"
The following •• e ther.ro... offered II &\IidelinN.
NEUROSURGERY
I ni tiat ion o f AEDII
AEDs may beCOnBidered for ~hortterm U$~ Table 13·2 H igh r isk criteria for PTS
e!~ially if a «izure could be detrimental A .
I . 8ClJ1lI subl::u13l, epidural. 01 intracerebral
Early posttraumatic seizures were effectively
reduced when phenyt<'lm wD8 u&l'd for 2 ... eekl!
2. ope!"K1epte$sed skul ltaClWfI wilh pllfe ....
following head injury ,.-ith no significant in·
dl)fnal lnjury
creased mk ofadvel"M effecta".
3. seizura wilrin !he flrsI2' In aIIer injloll
Option: begin AEDa (usuaUy phenytOin or , . Glasgow Coma Seale score ( 10
oarhamazepine) within 24 htll of injury in the
S. p&ne\Iatlng brain;,jury
presence of any of the high risk criteria shown
6. "'15I0I'l of Ii:p~icant alcohol abuse
in Table 13·2 (modified' .. ' .. ... .. ). When using
7. • COIIicaI (tlamor!hagic) CO'11usion on CT
PH1', load with 20 mglkg and maintain high
therapeutic levels (s« page 271). Swit.ch 1.0 phenobarbital if PH1' not t<'llera~.
--
~~ri1~:
~iij;.~~;i·;::~::'::::~:i~".":h'::r'~Il:owin~
~
following head trauma )
':~~~~~;~:~~;:;!\~f.1~:r~~;::i~;'~\~",~:~::;:,,,,
after 1 week (aee obo~):
mOJl of therapeutic AF.D levels
A~·
2. for
i _ 6-12
B. recommend EEG to rule-out pre!len~ofa seizure focus before discontinuing
AEDs (predictive value) for the following:
I. repeated seizures
2. pre8ence of high risk criteria shown in Tobie 13-2.
13.2.3.
Alcohol withdrawal seizures
Al90. see Alcohol wilil.drawol syrnJT"f)rM, page 149. The withdrawal syndrome may
begin hours after t he EtOH peak (8U page 150 for prevention and treatment). Ethanol
withdn wal sei~u res are da9.5ically 5*n in up 1.0 83% of habituated drink"," within 7·30
hour! ofwSl5atioo or reductionofethanoJ inta ke. They typicalll' coosistofl·6 tonic-clonic
geoeralized ~;~ ures without fowhty within a 6 hour period" . Sei~u""5 us ually octur be·
fore delerium develops. Tbey may a l90 occur during inl.oxication (without withdrawal!.
The sei~u re risk penista for 48 htll (risk of deleriurn treTD.ens (DT. ) con t in""" be.
yond t hat ), thUll a single loading dose of PHT is frequently adequate for prophylaxis.
H ow~ver, ,ince mOllt EtOH withdrawal ""izures Dre single, brief, and self·limited, PHT
has 1121. been shown to be of benefit in UIlcoroplicated cases and is thua .IIjJ,!ally not jndj.
~. Chlordiazepoxide (l.ibrium®) or other benzodiazepinea adminiBtered during
detoxification reduces th~ risk withdrawal seizures" (....e pogo 150).
Eval u ation
The follOw ing patients should have a CT lI(an of the brain, and should be admi tted
for fwther evaluatioD as well as for observation for additiona l sei7,ures or for rrr.:
1. those with their first EtO H wi thdrawal .... izure
2. lh""" with fOCllI findi ngs
3. those having mOre than 6 seizures ill 6 hrs
4. those with evid ence of traum a
Other causes of seitun! ahould al90 be considered, e.g. a febrile patient may require
an LP to RIO men ingitJ.s.
Treatm e n t
A briefsingie ""i~"re may not warTant t rea tment. except as outlined below. A sei.
zure that cont inu"ll bel'ond 3-4 minutes may be treated with d iazepam o r lorntepam,
with fl.lJ"t.her meaSureS used as in stat us epilepticu! 18<'t page 264) if seizurea perSist.
Loading with phenytoin ( 18 m&fkg" 1200 mgl70 kg,""",, pa£e 271) and long·tenn treatment is indicated for:
I . a history of previous alcohol withdrawa l seizures
2. reculTent seizures after admission
A. •• ~,.Iy . ..1,u reI OIly . I"".,. rcp . • <><1 OIay ad.e_ly . ff«'l>!ooc! P"-U,"" Ind ""Yl" n deh.e<y .
• nd ""'Y'"Oroen o,b. r injuri • • (e ... . pin. 1cord injury in t ho .."i",or e n u .. labl. oetvi .. r . pinel"
NEUROSURGERY
13. Seizures
'"
3. history of a prior sei zure disorder unrelated to alC<lhol
4. presence of other risk factors for seiz ...... e (e.g. aubdural hematoma )
13.2.4.
Nonepileptic seizures
AKA pseudoseizures (although IIOme
prefer oot to UM: thi s tenn since it may con·
note voluntary feigning of seizures), with the
term psychogenic I!<!izures being preferred for
nonepileptic eei,ures (NES) ....jth a psycho·
logic etiology {psychogenic se;,u«", are real
even13 and may not be under \"olunlary con·
troll"".
In a major medical referral center. 20%
of patienta with intractable seIzure. have
NES. Up to 5O%ofthese may have legitimate
seizures at $Orne timeaa well". The hazard of
NES is that patient.ll may end up needlessly
tak.ing AEDa, whicb in some ClOseS may wors·
en NES . Posaible etiologies orNES are given
i..o TobIe 13·3. Most NES are p"ychogenic.
Table 13-3 Olfferentlal dlagnOll1 01
nonepUeptle seizures"
c.
o.
c
,
...
,"'"
G.
DIFFERENTIATING NES FROM EPILEPTIC
SEIZURES
Distinguisbing between epileptic seizures (ES) and NES is a common clinical di ·
lemma. There are unusual ~ei~uru that may
fool experU". S<lme frontallobeaod temporal
lobe complex partial seizun!S may produce bi_
UrTe behaviors that do not correspond to
eiQllic ES findings WId may not produce dis·
cernible abnonnalities with scalp-electrode
EEG {and therefore may be mtsdiagn05ed
even with video-EEG monitoring, although
this is more lik.ely with partial seizures than
witb generalized ). A multidisciplinary team
approach may be required.
,
B.
c.
D.
H.istOI")': Attelllpt to documen t: prodromal
symptoOlS. precipitating factors, tiroe and en·
vironment ofSz, mode and duration of pro>
gT"ession, ictal and polItictal even\.6, frequency
llI\d stereotypy of manifestations. Determine
ifpatient has history of psychiatric condi·
tions , WId ifthey are acquainted with individuals who have ES.
Suggestive ofpos$ible NES: mulUple or
variahle oei.u .... typea (whereu ES ill. "3""lIy
ste!"eQtypical), fluctuating level of OOTl$Ciousness. denial of correlat ion ofS. with stress.
Psycbological testing: May help. Differences occur in ES a nd NES on the Minnesota
Multiphasic Personality Inventory (MMPI) scales in
ria, aed schiz.ophrenia".
,
bypochondriasi~,
•..
depres.9ion hyste·
Tabk 13·4 COlltra$\.6 some features of true $l!izuTe!l VlI. NES. and Toblf 13·5 lis13
some features often associated with NES. however, nocharscteristics s re defInitively diagnostic ofNES since a number of them mpy also occur with ES.
1.
2.
3.
""
Ifany two of the following are demonstrsted, 96% of time this will be NES :
out-of·phase clonic UE movement
out-of·pbase clonic LE movement
no vocalization or vocaJiution at start of event
Features COmmon to both true seizurfs and NES: verbal unresponsiveness. rarityot
13. Seizures
NEUROSURGERY
au"'matiam •• nd whole-body f1.ttidi ty. rarity of urinary inc:olItine.-.
Pro lacti n le vels after eei zUl"elll
Tran.ient ele"al.ioa, in hum811
aerum prolactin (lIS P ) leve l' Ottu r
followi ng 80110 of general ized mo"' •.
45'11 of compleJC pa rtial , ond only
15'1. of simple partia l .eilures" .
Peak level l are reached in 15·20
minu,," •• nd gradually retu rn to
baseline over the lublequent hou~
" . It hu been I UgcHt.ed that d raw.
in, . serum prolactin Ievellhor1Jy
I fler I q Ueliition.ble _ilure may be
helpful in dilferent iltil'lj' NES
(wh ich may hive elevated cortisol
levell but normal HSP level .... ).
"
....
.....
.....
,,.
F'I!~
Epilepllc HIlu,.
cIenie UE movemenl
'"
---- ............
...
OOA..oI·~
0
dorJie----cE"""_
0
,,
I!M 01 ~llJ'
.-
"'.
...,
....
6(l'4"epilep!lccr(
!ilde-lO-siQe
NEUROSURGERY
'ES
'"
""
SO.
,
.....
.
so.
~
.--0
mic: 01 donie: It$- .....~""
ga\1911'9. 'eIdin;.
.....,..
"ilOty JruSde
!riIltIJi
Repetitive seilUres an Issoci·
eted with progreslively I maller HSP
elev.tions" •• nd no riM followl IbHnalaeilures or IUtUS e pilepticu.
(whether tOIlvuiJive or IbRnoe)"".
Greater than twofGJd HSP elevuion$
con! iBtently foHow aeilllTft th.t pro-duoe intense widespread high frequency mesial temporal lobe
di scharges: whereas .uc h elevation s
do not OCCur in sei lW't1 not involving
t hese limbic I tructUTK<O.
Furthermore. the ... may be high.
ItT bawl!ne HSP level. In C.MS with
n,htoilided inte.xUI EOO discharges
c:ompared to t.hOH with kn-lided".
I nd the pr esence of ~ych<lpatholOC'
may s/feet pooitirtal HS P elev.tion....
",,",,,ro. e. the ,,~nal of HSP
peolul may be BtI"onll:ly indicative of
troe seilures. but the abaenal mlly be
due to. variety of com plu
phenomen.··. The over. lI c1.&Sifica·
tion accuracy io _ 7~
,.
Table 13-4 Faat ,... 01 ES a NES'"
...
--..
,
8'fo (sIooo. 1ow am- 36%!'IIOIerl. hi£tI
pMude)
.mplitllde)
nble 1W Fealuru often as.aoeliled wUh
NES"
13. Seitures
Febrile seizures
13.2.5.
DefiDiti o o'"
IetIIie
~,--
~r.1n irIIIms 01 e/IIIOren a$SCIdII:eQ with I"'e' I'Iliii no dtl'lI'II!d taU58
_ ~nIId by IItUIe IMRiiogle ~
NIMH
rll"ducln
cumo
~'-1)
.0IIIIWIsiCln NIHIl; Iongii'""... 15 rnmtes.1S lOCi crll'AJll!plll {mole 1hII~
_~ptr~oIlew!)
...""'"
n'IOfe ""'" _
fpiscde 01 \e'N .~- wI!h
semw.
EpidemioloJY"
febril.l'On¥ullion. I~ th, moel ronllllDnlype of •• jure. E~dudlllg chi ldren with
pr. w.tm, Mut'Ol",", nr dev.lopmenllllibnormilitlu, Ihe pre¥lle~e of reb rile ..i·
LIIrn;' _ 2.7<rt (I"II nse: 2·$" ill U.S. (hild"n llied 6 ~·6 yrI). The risk for developing
epil.pt'y .fter I simp!. febrile ",bul'll iII - \ .., I nd for I comple>: febril. "",ilure i. 6""(9'.1.
for pl"Olo~ teilUl1!, 2!Mo Ibr i'oo:el wtlurel. An underl)'ln, nNroloPU16r developmen.
t.l1.bMnn.lity or. r.ml", I'Il.tory of epilep.y inc~ the ri,k of developing e9iltplly.
T rt'.Rtm e nt
In ollliludy, the IQ in !.he ,",up t",.led with phenobllrb.ital Wle 8.4 painu lower
(95"ronndCl~ lnW'rY'U lhlP! the plaeebo /!:TOup,.nd t~rt remRinad •• iKDific,nt dlf·
ioeyenllllOnlhs .notrdilCOntlnuing ~ oinIlI"'. fUrlhnmo.e. there WIH no.ignif·
kant radIKtion in AilUrei in the phenobarbital group. And yet. noc-th~r drull' l"IIally
. ppeal"l well ... il<P;d to lre.ti"" thi, enlity: earblmnepinl and phenyt.oin II ppes. ineff""
Live, vllprOl-\e mlY be ,!fen!"e b ... t h..... n OUl rilb in the<:Z yr. sgecroup. Given the
low i.>cidena! (1$) orhavin, c{dvUe ~ZJJ'" (i.l . • pilejnY) ~' ali!Julk febril. seizu.e
and the raelthal AEo. pmbllbly do not p""ventlhil ~velopmenl, thue ialltll.! ... pporl
I"or p1l!5<1ibingllflticonvul'lInUl in these tun. "". re(:Urn"1lCI rtlle.offebri1e seizure- in
drild ..;m WIU, I hi.cory of one or n\Oft! febril. HizUI"!! can be mlt>C:ed by administering
diaz&pam 3.3 mglkg PO q 8 h ... dunn&. rebriillepiaode ltemp >38.1 "C).nd continuing
until 24 hN
th e r. .....r lu\)sided"
f_"""
.n...
13.3.
Status epilepticus
Derio!tion: More than 30 min ... t" onUtontin~ se.z ... re aeu"';ty , or (:&) multiple se..
~uros
without full _ery oftonscioulneK
beI."Weetl
H1"luree"
Types of atatu s e pile pli c u 5
gene ra lized SliltU.
clHlvulsive, geMTIliud conv ... lei_ toni~lonic statu. epileptu:Ul lSE) i. lbe moe!
frequent type". A medical .""''VIllCy
I.
2.
lIh$ence"
3. 8etcUldllrily ge ne"li;u,d: accounts fOf _ 75'1> ofgenerelized SE
4. myoclonit
~. ltonie (drop lIl .... ck): Npeeiaily in l#.nllOl(-G ......... t Iyndrome (In" ~ 2581
partlaIIUlt .... (""","Lly relllled t.o In /IIlllwmic abnormill ty)
1. simple (AKA e pil e pl)' pl rt l.li, cont ln u RII.)
2. compJu A: mo.!. often from frocllllllobe foo:ua. Urpnt t~.tnwnl" r.q ... ,red
3. .;econd. rily leneraliu-d
Ep id e miology
Incidenc. il _ 100,000 Ciau/yNr In the U.S. Most ea_ ooeur 1n)'O\itIII ehildtcm
(amon« ehlldNn, 7S'Ao were < $ 'J"I"I old" ), th e nlllt n_t a rrtcted rrOJp il pauenla over
Ige 60 yr!. In " 5O'Jo OrCl\it'Il, SE t. the !)flUent'. lil"$t aei . ... reM.
EUo lo gl ea
1. febrrle ¥ellUl'll': ' rorr.nwn pT~iplUto.in youn« I"'tlenlil. o5-&'lIo IIf palrenla pre-
13. Se;z". ..
NltUROSURG£Rt'
teoling with S[ ha~ a hi¥tory of prior febrile M'izures
2. ~erebrovJ;lJculu accideot.t: the m Olll~ commonly identified c8uIIe in the elderly
3. e NS infection : in children, mo.! Ire bacterial , the rnOtit <:ommoo Qrgan is rn . were
H. irl/llO(lnZll and S. pfU!~moni~
~.
8.
9.
10.
idiopathic: aCCOIInU for ~ one-thin:! (io cbi ldren , usu a ll y aasocia(.ed with fewr)
epiJepiI)I! i. plft",nt Or il .ublleq .. ,",n tly di agno»ed in _ 5[)%ofpatienu presenting
with SE. About 1(We of .d ult.. ultimately diagnosed as having epiJepll)/ will
pruent in SE
lubtherapeutlc !\EO, in patient with D known a",iure dilJ(lrder
electrolyu imbalance: hyponatremia (moct common in children, usually due to
w.~r [ntollie.lion"), hypoglycemia. hypocalcemia, uremi a
d rug intoxication (elpeelatil' cocaine)
. Icohol withd rawal
traumatic brain injury
II.
aoo~il
5.
6.
7.
12. tumor
In children < I yt age, 7S'JIO had In I~UU eau1le: 289& were te<"Ondlry to CNS ,n fee:'
tion , 309& due to electro~yte d i80rders, 199& 6IlI«ilted with fevu". In adul1.l, I Un.octu ... 1
lelion ,I more lik ely. In an Idult, t.ll e m08t common ~au.. ofSE I, lubthe'lpeutic AEO
level s in I patient with. known leinore di80rder.
FeHtures
MOlt common eauae iI. patient with I known .eizu... dilOrder hlvin, low ABO!ev·
ell for IIny ...,llIOn (noo-c(lmplilO.te, inte",ummt infection prevlnting PO inLllke of medl).
One out of .ix patieoUi pre_enting with I flNt timl ..izure will pretent in l1.I tUI epilept icu. (SE) . In IDO$t inatances. SE il' manifest.at;on of In !lCU!,.e inault to the lH".in .
MO$t Clse1l of convulsive .ta tU I in adul1.lI1.lrt • • partia l telzur. t~t ,ene,.IiM.
Morbidity a nd mortality from S E
Mean durat ion ofSE in patientl without neurolocic lequelae i.I I.e; hrs (therefore,
proceed to pentobarbital anH theaia before _ I hour oCSE). &nnt mortality; < lD-IN
(only - 29& of deaths .re directly a ttributable to SE 0. i1.l eomplieat ionl: the rat.re due
to the underlying procea producing the SEl. Mortality in lowu t .moo p t children
(_ 6'Ao"), patien1.l with SE retaled to subtbe rlpeutic AEo., and pl t ientl with unprovoked SE>O. The high..t mortality occur. in elderly patien1.land th_ with SE .-ulting
from a noxia Or CVA". 19& of patientl die during the epi.ooe i~lf.
Morbidity and mortality is due to":
1 . CNS injury from repetitive electric di K hargea: irreversible ch.... ges begin to IJ)'
pea. in neurona .ner IS little as 20 minutft of convul,ive activity. <:'11 d... th i,
vlry common afto. r 60 mina
2. ly51emic at rtali from the se izu relcard iac:, retpil'3tory, ""nal, metabolic)
3. CNS damage by the acute inault that provoko:d the SE
13.3.1.
General treatment measures for status epllepticus
Treatment i. directed .tltabilizing the patie nt, stopping the IIIizure. and identify.
ing the Clu.se (deurmilOin, if there". n ac:ute iruult to the brain) and if possible liso
t .... ting the unde r1,; n, prote:U. Although SF; ill defioo:d fOl" sehu,""" lasting". 30 mins ,
IggTeMive lo ticonv"laan l therapy i. indicated for any sei zul'fllasting:> 10 mins. Treat,
m~ntoften mult be inlti.led prior to the avsilsbi lity oftatl to confino the diagnOlli$.
CPR ifneeded
.Uend .i ....... y: onlli ...... ly Iffe6lible. Ot by n .... 1~.nnula or bag·v alve· mask. Con·
l ide, intubation if respirations compromised or if aeiture pel"8i8t1!". 30 min
IV (2 if pouible: 1 for pM-nytoin (PHT) (Oi lanti~), not neeeMary iffOlphenytoln is
.~.lI'ble): IU.rt wit h NS
monitor: EKG,. frequent blood p reasu, e check.
bloodwork: electrolyt.es (including glucose), Mg", C ... , phi nytoin level, ABG. SE due
to elKttolyte imballnce reapondl more read ily to eorrection than to AEOs"
,f CNS infection it. m~r eon,id... t;on, p.erform I..P forCSF a naly ai.(eapeciaiJ), in
f, bri le childrtn) unl ... contrli ndicl led . wec pleocytOll i. u p to 80 ~ 10'/1. can occu ,
following S E (benill'll ~tictll pleocylOolil). and th_ pltien Wllhould be truted with
a ntibiotics IIntil ,nfKtion can be ruled out by neestiv, cultu rea
NEUROSURGERY
13. Sebu rea
US
~ew
rueds for unknown pstient:
glucose:
A. for adults: thiamine &0· 100 mg IV should precede gluCOIie bolus (in tllS~ of
thiamine deficiency, e.g. in EtOH abuse ]. NB: CIIn precip;t./Ite Wernicke's
entephal opathy in akvholic patienl.$ (Uf pag<! 151)
B. iffingerstick ghu:ose can be ObUlined immediately and it s hows hypoglyce·
mia, Or ifno fingerstiek glucO$f! can be done, give 25-50 ml of 050 IV push
for adulls (2 mVkg of25% glucose for peds), Be aure blood has been sent for
definitive Rerum g lucose first
2. naloxone (Narcan®) 0.4 mg IVP (in case ofnarcotics)
3. :t bicarbonate to counte r acidosis ( 1·2 amps depending on lengt.h of seizu re I
administer .p~dfic ant iconv ul$1lnts for seiwres lasti ng:> 10 millS (""" ""low)
EEG monitor if possible
if paralytics sre used (e.g. to intubate), use short aeti ng agents and be aware that
muscle paralysis alone may $lOP visible seilu re man ifel;tations, but does not stop the
electrical seizure activity in the brain, which Can lead to permanent damage
1.
13.3.2.
Medications for generalized convulsive status
epilepticus
Table 13·6 shows a summary of
medications for 8t8tus epilepticuJI
that are outlined in further detail be- Table 13-6 Summary of medications for 6tatul
eplleptlcusln average size Il.l!.Y.!t
low (modifIed management scheme"·
(see IMIo< ~tails)
..... ). Items below in boxes are(on8~·
A. lorazepam (Ativan ) 4 mg IV slowly OVer 2
ered treatment of rnoice. · Peds· reo
mlM, may repeal ancr 5 mini
fel"$ to patients" 16 )'fa of age. Dru gs
should be given IV (do not use 1M
B. simultaneously loa with phenytoin'
rou te). If IV aroeS!! is impossible, di·
1200 mg ifnot slready On phenytoin
uepam solution (not suppository]
500 mg if on phenytoin (check levell
can be given rectally.
C. phenobarbital rv (@<I00IOg/mi n) until sei.
zures stop (up to 1400 mgl (watch BP)
Protoc o l
L
D. ifseilures continue> 30 miM, intubaUl and
begin pentobarbital (Ut tut)
"",,",m...., rat, tor pMnytOin IV i. $0 mcPnIn ; t", lot·
p/"ItnyIOin
~ ~ t5()
mg PEImIn
1_~2'2)
diazepam (Valium®) 0.2 mglk,g (10 mg aversge adult dose) IV @Smg/min,
repeat ,fineffective q 5 mins up to 3 additional d08e$. Pfds: 0.2·0.5
mglkgldose with max 6 mg if < 5 )'fS, max 10 mg if .. 5 y/1!.
Diazepam should routinely be followed by phenytoin to pnvent recurrenee.
Rectal dOile is 0.5 mglkg of diazepam solution up to 20 mg max, and is usu'
ally absorbed in ~]O mins
OR
2.
in pediatric patients with freq uent seizures or prophylaxis of reb rile sei.
zures and no IV al:Ce!;S, vaJproic acid is well absorbed ....,tally, a nd is admi n·
istered at 20 mgfkg d iluted in water or vegetable oil"
simultaneously W with phenytoin (Dilantifi®) (P HT ) as fol!ows (do not won)'
about acutely overoosing, follow dosing.rJlJ.tl, monitor BP for hypotension and
EKG for arrhythrniaa). Conven t ional phenytoin must be given only in NS to pre·
ven t precipitation. ~r giving the following loading dose, start on maintenan~'1
(lfffpagt 271)
'"
13. Seizures
NEUROSURGERY
3.
for 70 kC adult) (use 15 mg/kl for elderly pat.ien~). maximum rau tor
phenytOio < 50 mglmin (max rate for rOllphenyt(l' n ia 150 rna PE/min),
P~.: 20 mgI'II.g, ral.e < 1·3 mw'klVmin
B. ifoo fliT and ...... nt levI' i. known: a rule ofthu.mb il (ivinS 0.74 mglka:
to an adult .... i.es the Iflvel by ~ 1 .. glm]
C. if Oil PHT and 1eVi!1 Im known: -, ... It: (ivI500 mtO < 5(1 m"mln
pnxeed to each :oIlowin,ltep iC seiturft continue:
A.
PHT.dditional ~or5 mg!ka O< 60 mg/min up to_ toul of SO mglkg
8
either"
.<
phe~~~~I,:_ up to 20 m~ ~~. ( 1400 lTIJ fw 70 kg) (start in uaing
100 '"&'min vntil ..ituret atop), takes 15·20 min to work, ""atd!
BP (e myocardia l depres .. nt).
Ped.: 6·10 <n&:IkaIdo.e q 20-30 min to mUIOU130-40 mglkg.
Phenobarbital may be pn!fernd to PHT in pauanu with PHT hyperMn.itivity. card,,,,, eonductioll abnonnaJity, and in neon.WiII aDd
younr children. Maintenance phenobarbital therapy should be inlU_
tut.ed with 24 hOll" of tht 1000dini do$e (xc~ 275 )
OR
diat.~ eva1iutr4) drip: 100 III( diazepAm io 600 ml D5W. 40
mVmm (_ Icvl!! ofO.Z-O.& ""'mlJ. Ra,..ly u~ , levels hard to dleck
C . Prtp8r.! to init.iata reneral anuthelia, lidoc:.ine may be med to temporill!
a.ihown hert (ulually oDlitted )
lidocallle 2-3 mslkg IVP .25-60 mg/min, ifeR'eetive follow with drip
o(51).IOO mg in 250 cc D5W . 1-2 DIg/rain
D. ifeei,urel continue > 30 mInutes. intubate and i,...t.ituu."generalllIle$th...
ti a" by any of th.e following:
pent0b3r?~ta : load witb 15 mWVJf (range: 5-20 n:gr).g) IV at a rate of25
mg/mln , tbe .. place on "'Iinttnance IUrting It 2.5 mgIkghr, follow EtG
and t.itrat.e while maintaining burilluppression..··' hometimes up to 3
m8/kglhrl. Monitor SP. i/hypoteR.lion OCCUl"lllgive fluid. and dopamine<utpog, 662 lOr addit.ional meuu res IUch as PA eath.eted. For bmokthrough
sei~urell, Jive additional SO mg pent.<lbarbiul and iner-ease maintenalJ(:l!
rate by 0.5 m8/kglh
OR
benzo(liazepinu:
high-d06e IV loraupam {He ~I"",l
or midatolam (VO'~): adult: 5·10 mgbol u. at < 4 ""'min. followed
by 0 .05-0.4 Dl8/kgrhr drip. DaLa is limited, and use . hould bI rel tricted to refractory SE"
OR
call anesthetiologist to ioit.iate
general inhalat.ion anO'.thO'!ia: isoflurane (Foran/!4D) i, the pref...reo;I
agent (M avoid enflurane (Ethrane®),$UpafJt 1). NS : this requirtttn
&neath'!'"ia machine and usually tran. port lei the O.R... and eannot be
mainuined indefinitely. Rar.!ly. neuromuscular junction blodung
agenta are required (NS : paralyzing thO' pat.ient and thu. halt.ing the
motor activity without slelppin, the epilO'ptk: act.ivil), i. in!ufficient a.
continued oeizure act.ivlty in It&elf ia harm ful , . . ~ 265 )
OR
propofolanellthellia: Dau. i,limited. and use Ihould be rest.rict.ed to
refroctory SE". May have weak intrinsic e pileptogenic pro]M!rtiM
Efficacy
Diazepam .IeIp. "izuret within 3 n'i.n.t in 33111>. within 5 min. in So-.. PHT .topol.el·
2urel in 30$ aner ~OO 109 has been given. 63~ ofgeneraliud lonic'clonic SE r espond to
benwdiuepine • PHT. PHT is . Iower to control . U.lul than d,azepam, but lutllonger.
Lor ne pam
Not FDA approved for seiwrH (m.y , t.ill be used U ·off .... bel· indleat.ion ). Among
"- ... in.1>o>th phtnoborbi"ta1 on<! • bonood" .. pine (•.•. di • ..,.m ) I. di_"',od b«. u.. oI i ....... tod
rilk 01 '""1» "'10,), dep....i...
NEUROSURGERY
'"
benzoc!iazepines.lora,.epam (LZP) is preferred (diazepam (DZP ) ~istribute5 rapidly
in fatty ti" ues~, and sei~ure. may recur within 10·20 minutcll), but ~a\lses longer sedation. LZP aborts SE in 97% of cases, " •. 68% for OZI"". Abo. leSli respiratory depre.osion
than with OZP. As with all benu.>diazepines:
1. respiratory depression and hypoumsi on are exacerbated when used with other
depressants (including barbitu rates ... )
2. effectiveness in SE is reduced by prior maintenance on other benzodiuepines
(e ,g. dona>.epam), but.s not affected by the presence of other anticonvulsants
3. tachyphylaxis may deVl;!lop 10 that .ubsequent d<)$eS are less effecti"e'"
High-dose IV lorazepam:
LZP may also be a leSll toxic alternati"e to
Table 13-7
pentobarbital bUT1:lt supp re""ion «"na" because.
among other things_ LZ P does not produce systemic hypotension (this may beartifactual since
in this study_ bUNtsuppression was MI an endpoint with LZ P 88 it ill with most barbiturnte
protocols). It may be given as II contin uou s infu_
sion Of as frequent intcnnittent boluses. The
continuous infUSion protocol used by LIIba"" is
shown in Table 13·7.
,
,,
Me di ca tio n s to a vo id in .statu s ep ile pti_
ou,
I.
2.
nareotice
phenothiazine.' includ ing promethazine
(Phenergan®)
3. neuromuscular blocking agentli in the
ab.sence of AEO thempy : seizures may
con ti nue and cause neurologic injury but
would not be clinically evident (.f('t page
""
13.3.3.
Miscellaneous status epilepticus
MYOCLONIC STATUS
Treatment: valproic acid (drug of choiC<)l. Place NO, give 20 mglkg per NO loading
dose. Maintenance: 40 mglkgld divided (.f('e ptJIJc 274).
Can add lornepam (Ativ.n®) Or c10nazepam (KlcInGpin®) to help with acutccontrol.
ABSENCE STATUS EPILEPT/CUS
Almost always responds co diazepam
13.4.
Antiepileptic drugs
The gGBI GfllJltiepileptic drugs (AEDs) is seizure contrGI (a contentiGus term, U!Ually taken 8.R red uction of seizure frequeocy and se"erity to the point to pennit the patient to live a nonn.r lifestyle withGu( epilepsy-related limitations) ... ith minimal or no
drug toxicity. _ 75% of epileptics ca n achieve satisfactory sei zure control with medical
therapY" .
13.4.1.
Classifi cation of AEOs
AEDs tan be grouped as sho wn in Table 13-8.
13. Seizures
NEUROSURGERY
Tabr.13-B ClassltJca lion at AEDs
OIfl., "OM. • .g. le, CN"""""",") FOil. .1'.M1c.>1"'" _ a ' In p'."" ,.,.,
IM.,_ let ..... <Jr8typ8S ~_ IlOl ~
p<QYe<j irrdl<:a""'S .-e ., _ . oII~or..J
II.bIIt. , lOtbOns: II.BS . aD,""""". a(Ij "'adj~e ll!erap\< . CP ", comp!e. po!InIAi, GTe .
gMtrit~ed lct>k>-elOnic, PHT ", ~fl'rIOIn. Sz . "",.~"'. "tlttU¥"' .Ial"" ~p~
onmediale ' .... a .. oooage 10111>
13.4.2.
Choice of antiepileptlc drug
Autie pileptic drugs (AED ) for various seil;U r e type»
8o!dfa~ drup 8~ druC of choice (DOC).
I.
prima ry gtl neraJiUld
A. G'I'C (gene ralized I.oni.,...,lonic),
1. val prole acid (VA): if no evidence cf foc.lity sollie I tudiel fthow fewer
.idi! effecta and belter control than PHT (5<!~ poge21~)
2. CII rb" rnaupin~ rte pogt 273
3. phanytoin (PI-tT); Off pas. 27/
4. phenobarbital (PB): Mr past 275
S. primidone (PRM): 6« PfJIJ~ 275
B. ~b~""e:
NEUR OSURGERY
13.
Sti%u r~
'"
1.
2.
etholux imide
val proie acid (VA)
3. cJonazepllm
4. methsuximide: I a page 276
C. myoclonic _ benzodiazepines
D. (.Onic or atonic :
1. benzodiazepines
2. (eJoomate:!Ie;> po.8~ 276
3.
2.
vigabe.trio,seefHllIe279
portial (aimple Or complex , with Or without secondary generalization)" (VA may
compare fav"nhly with CBZ for secondarily GTC, but is less tiredive forcompiex
partial se izures"):
A. carbamuep ine (CBZ)
most eHeetive, leaS! slde efteets
B. phenytoin (PHT)
C. phenobarbital (PB)
D. p!imidone (PRM)
3.
I
slightly less elfeclive. more slde eHects
se<Xlnd line drugs for anJ of the above seizure types:
A. valprOllte
B. lamotrigineA: lMe p~t 278
C. topiramate': _ pllf;e 279
13.4.3.
Anticonvulsant pharmacology..
G ENERAL GUIDELINES
Monother a p y versu s polyth e rapy
1. in~rease a given medication until !!eiuTes are controlled or side elTeets he<XIme in2.
3.
tolerahle(do notrely$Olelyon theTal)eutic levels, wh.ich is only the ran8fin which
most pa.lients have seizu re control without side effect$)
try tno!lQtherapy with a dlfferent drugs befwe resorting to two drugs together.
8O'l& of epileptics can be colltrolled on monotherapy, however, failure of monotherapy indicates an 8O'l&chan~ that the seizures will not he controllahle phermae<>logically . Only. 109'0 hellefit significantly fTom the addition of. second drog".
When> 2 AED. are requ.i.red, conaider nonepileptic seizures
fXJ8~ 262)
",ben first evaluating patients on multiple drugs, withdraw the most sedating
ones first (usually barbiturates MId donnepam)
<-
Gf!nerally, dosing intervals should be less than One half-life. Withoutl08ding dose,
it takee about 5 half-liyes to reach steady $tate,
Many AEDs affect liver fu nction tests (LFTI), however, only rarely do the drugs
caUBeenough hepllticdysfunction to walTll.ntd iscontinua!.ion . Guideline: discontinue an
AEO if the GeT exceeds twice normal.
SPECIFIC ANTICONVULSANTS
Table 13-11 AbbrellraUon.
AED .. antie~~I_~ptic drog; ADS . ab5en~; EC '" enteric cooted; DIV '" divided;
DOC "drug of choice: GTe" generalized tonic-.:lonic seizure; SIC-P ", s imple or complex partial.
P h annaoolUnetioa: Unless otherwise specified, numbers are given for.onL dosing
form. t m m half· life; tp£.oU( " time to peak serom level; tss .. time to steady state (approximately 5 ~ tm); I OIC" time to discontinue (re<:ommended withdrawal period OVer
which drug should be tapered); n-IDF " minimum dosing frequency. "Therapeutic levelis the average therapeutic range.
A. • ffi!<t.iv. for monr tl'P"" ofVnoroli..d
'10
~.u,..,.,
13. Seizure,
""t •.-enal rnA opprovod fa, Uti. ,ndi"'''n
NeUROSURGERY
~
phenytoin (PHT) (Dilan tin®l
___~_oo_._ro_
\~-,-I
_ \
-"-~
INDICA TIONS
GTC, SlCP, occasi(lRally in ABS.
PHARMACOKINETICS
Phannacokinetics a~ complicated; at low concentrations, ltir>etics are 1st order
(elimination proporti(lRal tQ concentration), metabolism saturates near the therapeutic
leYel resulting in uro-orde r kinetics (e limination at a constant rate). ~ 90% ofl<lt.al d rug
is protein boun d . OralbioBvailability is _ 90% wherl'3e TV bioBvoiJability;s _ 95%; this
small difference may bto significant when patient.s are nea r limit1l of therapeutic rang<)
(due to ulO-orde r kinetics).
Ivt
' tii£.t.K- - _.-
!"!',~~ __.J10(~•. suspenso<:w1
~'!~'~"~3c
. . ,..
-~, ,"~\range.
~140hrs)t
<>[$
j,egularcapsules; 1.:"3h'5
extende<l_~~SII~:
4-12 hrs
IherapoeubC _
u """,sured in _laba: l().20jI9ImI (NB. ~ Is lIMo Ila PHT Ihal is "'" impcrlarll !Nliel)':
9>1$ 1$ USUAlly _ , .,. 0/ 1O~ PHl. !/Iu. IMr"l*'tic 1," P HT l""otIS ... ,·2 /IgII'm: $Orl'WIl8bs at. able to
rneaWr. j,,", PHl dired",).
pn~ oe~. on ... rum """'*'lIrltlOn and melat>olic IIIIOlndoction
I'I:! lot
Ren a l fa il u r e: dosage adjustment not needed . lIowever, serum protein binding
may be altered in urem ia which can obfuscate interpretation ofserum phe nytoin le~18.
F:q 13·1 may be used to convert. serum PHT concentration in a uremic patient C (obse rved), to the expected PHT level in non uremic patients C (nonuremic).
C (nonu'~mic)..
C (obse,",,~d)
0.1 ~
.lburnin
Eq 13·1
.. O.J
ORAL DOSE
Rx Adult, u3ual maintenance dO!!e= 3O{I ·600 mgld divided BID orTID (MDF z q d ,
for single daily dosing, either t he phe oytoin-sodiWD ca]lfiulel Or the extended release
fnrm should be used). O ral ~ dose, 300 mg PO Q 4 h" uotil 17 mgtkg are given .
Ped e: oral maintenance; 4-7 mglkgld (MD F .. BID). StlPPI.IJW: (oral forffill ): 100 mg tabJets
of phenytoin·sodium ($Odium·salt); 30 &: 100 mg KapsealS® (utended release); 50 mg
chewable lofatabS® (phenytoin·add); oral sUlipension 125 mgl5·ml in 8 oz (240 ml) bottl .... or individualS ml unit dose p3cks; pediatric suspension 30 mgf5· ml. P henytek® 200
&: 300 mg cap!lule• .
Dos a g e c bang es
Because ofzero-order kineti<:8. at near · therapeutic
Table 13-10 G ... I~lIne" or
levela a small dosage change can caw.e large level chang- chang ing p henytO in dosage
tIJ. Although (ompu\.er models are ne«.ssary for a high
Presen1Ie~1 eMnge 10 mak,
degree of accu racy, the dnaing cha nge guidelines in Table
(mold)
/3-10 or the nomogram in Figure
may be u~ as a
l00mwday
quick approximation .
GJ abaorption of phenytoin suspen sioo Or capsules
S.
5O~day
may be decreased by up to 70% when given with ns""llU·
tric feedings ofOsmolyte® or Jsocal®"· " , and the suspen 6ion h as been reported to have e rratic absorption .
Hold NG feeding for 2 111"3 before and I hour a~r phenytoin dose.
,:i.,"
"
>.
PARENTERAL DOSE
Phenytoin is a nesative iDotropl' and Can cause hypo\.ension.
Conventional phe nytoin may be given slow fVP or by TV drip (Ut below) . The 1M
route should NOT be used (unreliable absorption, crystalliza t;nn and sterile ab!ICe&&es
may develop). TV rnlUlt be given ,lowly to reduce risk ofarrhythmia~ and hypotension,
viz. Adult: < SO rnglmi.n , Ped s: < 1·3 wg/kglmin . The ooiycorr,pRtible solution is NS, in·
ject at s i\.e neares t vein to avoid precipitation.
Rx ~. Adult: 18 mWki s low TV. Peds: 2Q rnglkg slow TV.
NEUROSURGERY
18. Seizures
no
R;c m~'l.«. Adult 200·500 mg/d (MDF = q d). Most adulu have therapeutic
levels on 100 mg 1'0 TID. Ped s: 4·7 mg/kgld (MDF ~ BID).
Drip loading method :
Requires cardiac monitoring. and SP check q 5 minutes.
R;c Add SOO mg P HT to SO ml NS to yield 10 mg/ml , run at 2 mUmin (20 mg/min)
long enough to give 18 mglkg (for 70 kg patie nt: 120(1 mg over 60 mins). For more rapid
administration, up to 40 mglmin may be usOO , Or use foophenyt(lin (_ b.!/ow). Decrease
rate ifhypou-nsion occurs.
Dlr&ellonl for ullng nomogram
"
"
"
I ""
• ,~
30
~
~
,
""
draw line connec:r.ing serum
~ 00 line A with currenl
flDseon me B
B. marl< point whete lhis I'im il·
lefSeCIS line C
c. (;I)tIIl«;I poirIt 00 C 10 Ihe desired serum level on A
O. read new dosage 00 lire 8
.
.,
I
600
500
'SO
3SO
9 B
~
(SSWIIIIIS Sleady state)
300
,SO
""
6
'SO
.
5 -
,.,
-
R.p«odocw
r""", ""'' '11<"''
~ M,",itori " 8··l"r<4ict;"~
Phony'oin Dooc • " R<Yil«ll'lo-
3
A
50
B
C
~m·.R.mbe<kB ....I.\loI. t.
W. l2S·J). 1979. ",th p<m,. .. ion
FIgure 13-1 Nomogram 101 adlushng phenyIoin dose
F OBpb e nytoin
sodium injection
Foephenyt(lin sodium (FOS) ifl.iection (Cerebyx®) is II newer formulation for admin.
istering IV phenytoin. and is indicated for sbort term use (0: 5 days) when the enteral
route i. not usable. It i8 completely converted in vivo to phenytoin by organ and blood
phosphatases with a conversion half·life of 10 minutes . Product labeling is given in terms
of phenytoin equivalents (PE,. Safety in pediatric patients has not been established. SUPpuw: SO mg PElml in 2 & 10 ml vials (l00 mg PE and 500 mg PE respectively).
Advantages of FOS (over conventional IV phenytoin ):
I. leu venOIL!l irritation (due to lower pH ora.6·9 compared to 12 for phenytoin) resulting In 1~B8 pain and rv extra vall88 ti Qn
2. FOS is wster soluble and therefore may be infused with dextrose or saline
3. tolerated by 1M injoction (1M route should UOJ. be usOO for atlt tus epilepticu.)
4. dQell not come cotnbine<\ with propylene glycoL (which can caU8e cardiac arrhythmias sndlor hypotension itself)
S. th e maximum admini.tration rate it 3 X as fast (i.e. 150 mg PElmin)
S!DE EFFECTS OF PHENYTOiN
May interfere with cogni tive function. May produce SLB·li ke ~yndrome, hepati~
granulomas. megaloblastic anemia. oe rebellar degeneration (c hronic doses), hirsutism,
gingival hypertrophy, hemorrhage in newborn ifmother on PHT, tmae epidermal nectol·
Y8is (St.even8.John90n varian c.). PHT antagoniU8 vitamin D - osteomalacia and rickets.
Most hypersensitivity reactions occur within 2 monthsofiniliating therapy" . In e58'" of
tnaculopspulsr erythematous ruh, the drug may be stopped and the patient may be reo
challenged; often the ruh will not recur the second time. ~ (fetal hydantoin
8yndrome'").
Sign s of phenytoin to~icity may develop at concentrstions above 20 I'g/ml (toxicity
l 3. Seizurea
NEUROSURGERY
is more common at levels> 30 pglml) and inc lude nystagmus (may a lso ocCU r at therap'!Iltic levelsl, diplopia, ataxia, aSlerixis, slurred spee<:h, confusion, and CNS depre.\!~ion.
Drug-drug inte ractions; Ouo~etine (ProzaC®) results in elevated phenytoin levela
(ave: 161~ above baseline)". Phenytoin may impair the efficacy of; CQrticosleroids. war_
rllrin, digoxin. doxycycline, estrogens. rurosemide. oral contra<eptivel, quinidine.
rifllmpin. theophylline, vitamin D.
~carbamazePine (CBZ) (Tegretol®) \c~/,---
__~_"'_~
___\,,-,
INDICA TIONS
Partial seizures with Or without secondary generalization. Trigeminal neuralgia .
An rv form fo r use in e.g. status epilepticu$ is in developmen t.
Dos.
&: ora l route . Ad ult ra nge: 600'2QOO mgld . Ped. : 20-30 mgl'kgld. MO P .. BID.
Before starti ng, cl>eck: CBC &. platelet count (consider retku )ocyle count) & Mrum
Pe. Package insert &ay. · recl"leck at frequent inte rvals, perha!'S q week I( 3 mos, then q
month I( 3 yrs."
Do not sur!. CBZ (or diseont inue it if patient already on CBZ) if: WBC < 4K . RBC
< 3 x 10'. Hct < 32%. platelets < lOO K. reticulocyte. < 0.3%, Pe > ISO pg%.
SUrt Inw and increment slowly: 200 mg PO q d I( I wk. BID I( 1 wk, 'I'ID It 1 wk . ..u
an inpatient, d(>Sage changes lI"lay be made every 3 days, munitoring for signs of side ef·
fects. As. an outpatient, changes should be made unly _ weekI)', with levels after each
change.
SlIPPLtEo: oral fonn . Scored tabs 200 mg. Chewable scored tabs 100 mg. Su~pension
100 tnglS-ml. IV form' Dot ava ilable in t he U.s. at the time oftNs writing. Carbohy_
dra te (exte nded releu1! CBZ): 200 & 300 mg tablets.
Caveats with oral fonns: oral abso'lltion i$erra ti~, and smaJJermorefrequent dose$
are preferred". Oral suspension is ab~rbed more readily , and also lit should JJ.l!l be ad ministered simulta neously with othe r liquid medicinal agents as it may resull in the precipitation ofa rubbery, orange mass. lit May aggravate hyponatremia by SlAD H·Jike
effect.
PHARMACOKINETICS
l,l'i (ha~.fiIe)
single do:l$e: 20-55 '""
alte! cIIIoruc therapy: 10-30 h's (&duIts),
~.~ ~~ (peds)
may be mi_rng """"'" lhe _
""'tabOide Clllbem<l.Zepine-1 0.1 ' -epcx;,je moy c.ouse 10XOcity and musl
beassayed_al~
ISS ""'y :Ml.eq"",,,Uy!oI due 10 auooin(luClion wt.O(:h plateau. $I . ·6 wks
eBZ induce$ hepa tic enzymes that res ult in increased metabolism ofitliClf(autoin_
duction) as well as other drugs over a period of 3·4 weeka.
H
$IOE EFFECTS
lit Drug-drug interaction; caution, propoxyphene (Darvon®), dmetidine. erytlUomycin and isoniazid may cause dramatic elevation ofCBZ levels due to inhibition ofhepBtic
cytochrome oxidallO! t hat degrades CBZ"'. Side effects include:
1. dtowsiness and GI upset: minimized by IIl0w dose esca lation
2. relative leukope nia in many: usually dou not require disconti nuing drug
3. t ransient diplopia
4. auwa
S. 1e$ll effe<:t on cognitive fu nct ion than PH'I'
6. hematoiogicaitoltitily: rare . May be serious - agranUlocytosis & a plastic anemia
1. St.evens.Johnaon syndrome
8. SLAO H
9. hepatitis (occasionally fatal) reported
NeUROSURGERY
13. Seizure!
~
oxc:arbazepine (Trileptal®)
\c.,../,::,--:-~--::"":.,--"'__\-'~
Ver, . imi.a . efficacy profile 10 carbamueplnlP. with Ih~roUowing differe neu:
I thare il no lIutoi oducl ;on (C. P~ 50 i. not involvM In ,,, at.ftbulilln) and Ih enl! rore
m;rumal dmg-d' ''11 ;nkrlldiofll
2. fI<I bll'lOd !.tIling if ~ulr1!d ';1'1«:
A. lhl,.. ia no Ii..., «Iudt)'
B. lite,.. i. nn hematoLogic wx ici l.)'
C. there i. no netd 14 check drug 1, ,,,,,1,
3. do.i nl iI BID
• . ki r>elic. ... Iinea r
!i. mOllle" pelllli..e
005E
R.r. tUrti ng d_
for ptIIin con t rol iI 1)() ms PO BID, fo r ",~urat It i, 300 mg PO
810. Muimwn dOle 2400 mlP'day lOUt . !Jt..'I'I'UM: \50, 300 &.600 1111 Kored ta ble"., 300
ms/5 m! anol UlptllIlIion.
~
•• 1"",..
\,-~/
,-_ _""'_"_'_ _
\>-..,
A•• ilabl. . . valpmic .dd IDepa\umfl'ill) and dinlproex sodium ([)@pakote\lll),
"""'nom
Effective in primary GTC. Abo uw l\.o\ in ASS with GTC, jllvenile myoc]onicepilep..y, and PIInial ~izu r. (not FDA appf'O'led for 1Mtel'). AJiCI FDA IPPI"O""'" for migr.>ine
propbylu iL Note; 1e"1"" GI upset and shOf'\ halrlife ~kl " .Iproit acid much leas useful
than Oe~kot<llll (di "a1prou sodium),
DosE
Adult rang'" 600-3000 meld. Ped. TIlIIJr. 15-60 mw1<gfd . MOP ", q d.
Rx Suu't a~ 15 m&'kgfd, i rocremMl al I \\Ik in~rvals by 5-10 mclkgld. Max recom·
mended &dul ~ dose; 60 mi/'kg/ol. Ir daily dOH" 250 mg iuequired , it should be divided.
9U1'f"UIW- Oral; UI*UlilS 250 "'I. Syrup 250 mgl5-ml. Depakold(enleric _ud) tabs:
12!i. 250.& 500 "", 5prinkle ClIp5u lesl25 me. IV: Depacon®for I V• •!\i..:tion 500 mg/5
mt vial.
SlOE EFFFCts
s..rious ,ideeff.,w ..... I"IU"8.. f'Mq1:ll1ilil hal ~n
repo~
F.UllU.er failure IuIII
occurred especially if IIge < 2 ynand in combination \\I,th other AEDs. Tbtppntc 1_
Conlroindil:ali..". btlow), Oro....mna ~lI'mpOr..,.), minimal coenlt.ve dt6~ita, NN (mln1roJ1ed with Depil kotl'),livet dy. f"oetion, h~ramm_mia (tven w.thout l i~rdy:lfulK'
tion), weight lain , mild hairlou.l.remOl' (dose related. l imila rto ~ip !'amma] tremor:
If'eo<er. and vlliproic lleid i. 1'Molutl'ly ntcuNf)', tbe tnulor m1l,)l be lrutftl with beta
blllCkeno/. May ;,Hetfen witb platelet fllnction, ealltion with aufJef)' on theK pII t;en".
COloffRAINDICATIONS
" Pregnancy: CIU_ n""1111 tu be def.,1.1 (NTO) in _ 1· 2110 of,.l1l n"", Sinee II cOl"rtl,tlon bet\\lO!en ptllk VA l,vl lI .nd Ih' ri, k orNTOs h .. been fouod, ir VA mll. l 11ft
wwd , -.>me ol'''-peru recommt:nd dtangi nalmm BI.o w TID d.:..in" " Pltiol'nts s 2yrs 'I'!
(n. k of hepel.OlmrJcityl,
la , ~jlUIU
NEUROSURGeRY
\ I
phenobarbital
\
INDICA T/ONS
Uled u .Uemllt;Vi! in GTC a nd partl.ll nol DOC). Had b,e.en DOC fill' febrile tel·
ures, dub.ioUIIlH!neCil" . About 41 en'clive I.-' PHT, but very &&datinl' AI.'IQ lI~ed fll~ sUo·
I", "pilllpl;(U' (Me Pf18t 2611,
DoSE
&1m" do8e PO, TV, or 1M. MDP . q d" " . Start .Iowly 1.0 minim it. tedation .
Nor AduJt lOlldini: 20 m"" ~ IV (.dmini,ter at rate < 100 ,""min), Ma.iuk:
.nlIJltt; 3()'250 mgld (ullulillyd;vidM BID·TID) Pcdlll!adin&; 1!>·2{j mg/llg. 1!'I..wt.tlW1r/l!
2·61t1i/'kg/d (uIU$1I)' divided BID}. 8U1"I...:0: Uoba 15 ml, 30 mi, 60 mil. 100 mr. Mi.w;ir '20
mKf5.-mt
PHARMACOKINeTICS
~~
l (pHiI""') ISIH!1f5lll.)
1m
(h.itII-ife)
iiiilf5C1 (fBI'9&: SO::160 tnf IN rnr:f:'6
(~)
f&:2raiYi1/i11, IiQ F
'!!
PIds:~':7onca
~
11M!
&:a-..¥{,ecII.a 1s.30 iijmI
iDe
up 10 3OdI'I!)
- 25,;,perWMll}
_
Phel'lobllrbital i& II potent induee. ofhepahe In:qmu that rfletaboli .. ollier.u:o..
SIDE EFFECTS
Coen ,live impairment (mill' be . ubtle .nd ltUIy oull ... 1 ..tmintstn.tioo ofo.e drug by
It leul several m(lnlhr'), o.ua Rvmd in ~!; &&dlhOn: pa..-wal hypuac:tlV;ty I~
dllUy In ped!l; may CIlUM! Mmorrhage m newborn ifmother
primidone (Mysoline®)
~
on phenobarb.tal.
\ I
\
IND~T/ONS
Sime a! phenobartJital (not DOC). NB: when II&ed in combination therlp"lowda.es{50·125 mg/dayl ma,lld d $igniliant6\lin"'\I! conlTollOthe pnInllry AED with rew,ide
elfec:"'.
DosE
R.r Adult: 2S().lOOO mgId P ed.: tli-30 Inf/kgld; MUf' '" BID.
Start.L 121i meld II" I wk . and inc. , !owl, to "'(Iid -u.tion. SUl'I'UEIr. (()f1I1 oru,l:
lOOTed t.I~ &0 rug. 250 mil:; IUlpelUlion 2IiO mg/5· ... I.
PHARMACOKINETICS
Mtllbolilell include pho!nyletbylmllonomide (PEMA) and ph .. noba rbital Thln!fore
alwly! dltc::!..Pt'enob.ttlit.t.1 1....I.t ..ml ti.,.. .. Primldon",.C"'~'~I.",. ."".... -_ _
1117
+~.
WAIl
IIsIS
""IiiC" IIifiiIiIO*IiViI
/!IIIt·We)
1PNt1Mal(tltadr1lall} (~) (jqIrIj
j
~: Cmlli"
ciIfWt!I D/lIfICIbIibltII: 500 1!iC M
11"-5111
SlOE EFFECTS
S.me .. ph<llnoM.bilAtl , plu~:
1 ~1ii3D1IiYI
~.
""" . . . IJI'TiibIi: H5
~
dIMd ~ If)-'O I
oflibido. rare ..."crocylit: .nemill.
ethosuximide (Zaroo tin®)
\ I
\
INDICA rlONS
OOCinABS
NEUROSURGERY
13. SeiturN
'"
DosE
Rx
Adul ~:
~p .... lel 2~
500-1llOO mWd. POO l : 1().<40 mglkgld ; MDr . q d. SuPPU£D: oraJ only;
mg; 'YTV P ~O mW5.m l.
Its
Therapeutic Ia'IIII
(SItIft1 "'t.)
(IiVII'i)
acOt: uplOf4Oii)'l 4().1!):1
ptds: up 10 1 dal'
SiDe EFFECTS
NN; lethargy; hiC<:'Ough.; HI... ; ra~ly : eotinophilil, leukopi!ni •• erytheml multi·
forme. S tev'M·JohnSOn syndrome, SI.E·lllca Iyndrome . Toxi c level. - pl)'1:hotic ~hav·
jor.
methsuximide (Cetontin®)
\ /
. ,,.,
""",
\
INOICA TIONS
l "di~llt.ed
for ab$~nce seiz,,~. refractory to other drop.
DosE
Rx optimum dOM! must be de~rmined by trial , Start with 300 "" PO q d, ine~'M
by 300 mg lit weekly intervall PRN to a maximum 0(1200 mgld. Suppuro: ISO&: 300 rnl
cap$ule.,
,-/
felbamate (Felbatol®)
\
/
tRJOlNFQ
\
,
• CAlITlON: Due to an unllC<:eptilbly high nlU "f '))Iut;" llnem;1I and nepoltk fail.
felbamate (FBM) 5h ..... Jd nol ~ ~ e~cept in those cin:u1n6tanca w~n the ben·
efit clearly outweighs the risk; then., hematologic con.ultation;. recommended by the
manufacturer. ~e Sick t!ful. below (also for drug.<,lrug interacti.ons).
~.
rBM i. efficacioUII {or monotherapy IUId adjunctive lherapy lOr pIlrti.l .eizW'ft
(complex and HOOndary gene. a1intion). and reduces the r~uency of atonic.nd GTC
",izures in ~nno,,·Gastaul syndrome.
PHAflMACOKINEnCS
"~)
I 20-23 fA
I1(pe·kleYebj
....
1·31n·
DosE
R.r. CAUTION I « QI>oot.
hbl.I3-11 Effect ollelbemale on olller AEO level.a
Felbamale ia~ 10 be used as I
lint-liM! drug. Palientor
cu"dian . hould sign informed
content rele'l\!. S\.IIrt with
l200mwddivided 8ID. TID.or
QID, and deerUI\! o!.her AEDS
by one third . IncruM relbama\.ll biwHkly in 600 m, inue.
rMnU to ulual doN of 16003600 mWd (m ...: 45 mg/l<gId ). Slow down ina.!menUo and/or reduoe other AEOt further
if,ide etf\!Cu ~me ~en. Admini.l.er at upper end ofr."(\! when used .. monothe r.
apy. 9uPPuu>: (onol only) 400 &: 600 "" acored lIbleu; .u_pension 600 mg/5-m l.
SlOE EFFECTS
Felbamat8 has bHcn auoc:iated with aplastic anemia (ulually diacovered afte r
~30
...·ks 'ftherapy) in _ 2·5 caSOl' per million person, per yr, , nd hep3lic raau", (..-me falal.
nt«IIIiUlling b..eline and serial I..I"I'1 every ]-2 wki). Other .ide effeda: inaomnia. anore",;a, NN, IVA. Felbamate i. a potent tn\!Ulbolic inhibitor. thus it i. necellaryto redUCf!
'"
13. Seizure.
NEUROSURGERY
the dQ~1! or phenytoIn, vllipronle Or C8rb8maz .. p;n~ wlln \l&ed w.11I relbamllte '" (see 'rabi,
/3 · / J! (geoeral rule: drop dOlle by ooe l hirdl
\ I
leveliraceLam (KeppraQ9)
\
INOICATIONS
AdjUnctive therapy for part ial 0080\ Sz. in &dults.
DOSE
IU st.art. with. 600 mg PO BlD. [ntroment by 1000 mgld II 2 w«kI P"RN 10 II maxi·
mum IIf3000 mgfd.
SIIT'Pu ao: 250. 600 & 750 ms Salrl!d rdm-<:Ollied Ulbl .
SlOE EFFfX:TS
Somnolence and ratigue in 15'>\-. Dininr.ss [0 Sot-.
\ !
clonazepam (lGonopin®)
\
A \lenzodiucpme derhr~liVL'.
INOICA TIONS
•
tilI.~ I r<!COmmended drug for l<!i1.UMlt (SI!f! btlew ).
lIRed for mJOClonie, awoic, Dnd absent(! &eizur~s (in pbs" .. """ leas "lfacl lve Iloilo valproale Or ethosuximide. and tol~ranC\: m~y deve!o-p).
Nl1: clona2epam u~uaUy work$ very wQII for $evenl mortlns, and thcrt tendg to ""eomo l"55 ~rrC'Ctive. l~aV\ng ol\ly th .. ~~'CIatingflrr~'(!to . Aillo, many casu have been ...,port..
ed or patien ts having sclwres dunng withdraw"l, induding AlII!U!I epilcplicU!I (even in
p$tiento with no hi~tory Of&l.II.luS). Thus. may nef'd to taper th)$ drug Over 3·6 month!! .
DoSE
1U Adult: IIUlrt eL I .!i mgld OIVTID, incrclIIIC. by 0.5-1 mg '13 d. u6ual dosage
range is 1·12 mgld (max 20 109/d); MOF ~ 'I d . Pew.: Bt.arlat 0.01·0.03 mglkgld OIV BID
or11D. irn:rea9e.byO.2S-0.6 mglltwd q 3 d; u9U111 dDMge. range,~ 0.01·0.02 mg/kgld; MnF
'" 'I d, suP!'uHu: <IJ'el onl:.'; S«)rcd !.lib,: 0.5 mg, 1 mg, 2 mg.
PHARMACOKINCTICS
1'<1
tss
I!'WI
(hIIII-liIe) (pNk Mis) (siOOtly (.late)
, ~""T,!1n
,
-
TlierIlQellllc level
lQ(
(1lisoonIkot]
(PI¥rnI)
~"i:"4:.aa~3-6~:
-O.lI"i3=O.on-
CAUTlON. ~awal""U/"""~' _"""1tbove
SIDE EFFECTS
Ataxia: drowl incU; behavior d>llnR"C!.
\ I
zonisftmide (Zonegran®)
\
INOICA TlONS
AJijunctiVl! therapy for JWlrtlaJ Sl in ndulu..
~
\ !
acelazol8l11ide (D iamoX®)
DfIUOItlFO
\
,
Tho anli~pilcptie errC'Cl mfty Ire e.iUu:r due to dln:.d iMibltfon ofCNS carboni~ 1111hydraS\! (.J~ l1!duces CSF production) o r due. to thc ~ light CNS acidosis that T1!sull!l.
INDICA noNS
CentrkephaHe cpileps;~'S (ebsence, non focal
NEUROSURGERY
&ei~u r"g).
13. & ilurea
Best ,"""u)u. are in ab<sen~
m
aeizuru : how_ r benefit h""ellKl b!!en obllcrved In GTC. myocloni,jerk.
SIOEEF~CJS
Do no~ UII in fi"'t lrime$:er of prfllUan cy 11I111y
btl ~rll~nk). n,e diu r.tic ~fTect
Ul ullU ,,!nallo... t>fHCO~ which mllY lead to lW .ddotic I\.III.!! with lon,-I.!!nn Ihe •• py , A
aulfonamld., Ih,,,,fo", eny typi~lI.l reAClion \0 \hI , clll61 mlly OC'C ur (anaphylaxii, fevi!r,
ruh. Stevens.JohnlIOn syndrome, \o~;c ~pi di':rmal n8Croly~il .. ,l. P. . . thui": medica·
tion should be. diMOntlnufld.
DosE
Rx Adult; 8·30 I1Ilt1'kgfd In divided dOJt!alma.x I amid, hiKher dlllla donot Il1Ijlf'OVI
control). When given with another lIED, theluggelted lurtingdOlllll250 mgoocedaily.
lin d thi! ilJTld uolly Inere.aeC.. 8IJ1'PULD: t.ableu 125. 2SO",.. Dilmo:~ ilf!qudalll ..... au.·
tainl'd reJea'e 500 I1Igcapolulet. Ste rile cryodeN;csted powd~r ;,alllO ..... il.ble in 600 mg
viala for p...... nle •• 1 frv) use.
,---/
gabapentin (N eurontin®)
I
\
IlfIUOII'FQ
\
,
Although developed w be. GABA .coru&t, ildoes nllt inlll rlol:t.t .ny known GASA
Em""cioul far pril1lary generaliuod sellUl"e1 and P/lrtlallei.uru (with 0. with·
out ~onclal')' generalization). Ineffective for 'WoeI1C<l ..i IU~. Very low incidtnoe 0(
know n tide·effect..o.. No known dr uc interadiona (probably beqr, UiIe it i, ..... nlllly excrel<ld).
~ptor.
DosE
It:.: Adult; 300 11111: PO II( 1 day 1; 300 Illg BID day 2; 300 o:o,gTID dayS; thell irw:rea..
rapidly up l.o u.ual doIIe. of ~ 800-1800 m&" per day. 00$eI of 1800-3600 .... y be netdi!!l
in intracLabln pati~nt.s. no.a~ mUlt be redured;n ""l~ta with ~.I intufficiOlney III'"
011 dialrs\;!, 8m'I'um: 100. 800."00 109 Cllpeulu.
PHARMACOKINETICS
Gabapelltin i. no~ l1Ietaboli~d •• nd 9a~ile~creled unchanged renallywi\h pla.ln.
du rance direetly Ptllpnrtiona~ to crntinine deal"lllnct:". Ooea nat affect ~patic micrn&om.1 "nlymeB, and doe.. not .ffect fUelJlbohsm llrother AEU.. Ant.acid. decUQe bioavailablUtv by _ 20%. thererore <'ive ,abe"""t;n > 211,..
the anl.ldd"
ilin: ~
'"""'¥W --I1r$ ="- nw-~
.ne.
llhaII-lilel
$-,IVi'
(pNk __j
(s1llldy$IIII6J
f.3fiiS
f.laiys _
. .........
SIDE EFFECTS
Somnolence. diulnea., . Iui l, raligl)l!, nystagmus; IU redu.:. .1'-.....,-2-8 weeb of
drug lhenpy. lncre.1ed appetil.e.. Nat known to be terat.llp.n>c.
,---/
laffiot rigine
(Lamit:ta~)
\
I
~ I!*O
\
,
A.ntleonyultant effect .... y t,. dw.1.o prayn.ptic. inhibition ofllu tUUlte relealJe".
E1fiCicioua.1 .dlu!)I:Uyt thenpy for pnrtiallCizuretl (with 01" without seoond.ry
gener.hJ.aUnnla nd .... nnox·O.. taul IyridroOle. Pnlim;ruory daUl I"'llBul it mly IllIo be
us.ru!
In .~ltRct (/)r refractlit)' lellenl lized KizUIU. or n IIIOllIIthe .. py for newly di.",~ part ial or ¥t'nl!flj li Uld aeizum .... Alia fDA Ipp«I¥ed for bipolar clillllm r.
a.
SlOE EFFECrS
Somnol.noe, d.iazlllQl:, diplopi • • II Serio..- .... b" requirillC hOll~itaJiElltion and di.
cnnunuation O(WOIpy hllye been reported I,...h ....,ally bt!gi1Ul2 week. afte r inili.ling
therapy and lilly t,. HVete and potenUllly lire-tb,,,,t'!lung, inclw\lnC Stewcna·JohlUOn
l)'I1drome lmore of, concern " 'ith ~muJtaneou. UM o1valp. oale),'rod 'Irely. tolUf epi·
deMl"l.1 necTOlyllia ITEN )). lncideru:. or'icni1kanlep;dennal rNction may bot dec:reBted
by. alow ramping-u p lI( dataCe, MIY increaH MilU'" (requenQ' in severe myoclonic epileplly orin/"allcy"". Metabolilm or lamolri"ne ;1 arrec:t.ed by Q\her ABO..
13. SeI1.U,et
NEUROSURGERY
DosE
Rx Adu lt : In aduJta receiving enzyme-inducing ABOs (PET. caz, or phenobarbi tal). start. wjth 5(1 mg PDq d lI 2 ",lui, then 50 mg BID 1 2 WQ, then I b.l' 100 mgldq "'...,1<
until the UlIual maintenance dose of2oo· 700 m(id (divided 'nt.:- 2 dose,) is reached. For
patients on .... lproic acid (VA) oJone, the maintenance dO&e Will! 1(1()-2oo mgld (divided
into 2 dOlI". ), Rnd VA level. drop by _ 25'1> wilhin II faw weeks ofsLilrtinlllamolrigina.
Por patien ts on both enQrne-inducing AEDs.a.rul VA. the starting dO&<! iii 25 mg PO qod
• '2 \liD, then 25 IIlK qd • 2 \Ilks. then I by 25-5{lIllg/d q j-2 Wk3 up to a maintenance of
100-150 mgld (divided into '2 do&e.). Instruct pati"ots that f8~h. rever ()r Iymphadenopath .... may herald .. serious reaction and !.halll phYllidan .hould be contacted immi!djately,
Ped~: not indicated fbr Ulie in patients < 16 yrs old due to high(!r inciden<'e of potentially
life-th reatening rash in the ped iatric populat io n". S\II'Pt.II:U. 25, 100, lfi.O &. 200 mg tablets. 2. 5 & 25 mg chewable dispe1'8iblc tabJ~ts,
PHARMACOKINETICS'"
ilPW.
llotl
j(pta~ 1eYeIII)
(hIIII·li!ej
~iv!.'
1I.5-5r..s
naw·I~';s <t1OI!&nI(llO _
_
1ss
1staad1 stale)
4·1 dayi
~ IiVii!
niifiiIililiiIi
IS 1>15 II)' f'HT .".,. CBZ, _
•• VIIIproo<
or'()r.asea ~ 10 5'i 1'111
\ !
vignbaLrin
\
INDIO. nONS
EtTective in treuting pEll"I.iaJ
DoSE
R."
Adul ~;
,-/
sei~t1res. Le5~
aa far
ge"emli~ ~i~"r".
1.500..;>000 mgfd .
wpiramatfl (Topama¥®)
\!
DflIJO fIFO
\
1
Mal' block vo!tage-serlJiiuv ... sodium channels- and enh~nce GABA activity at GABi\\
reeeptors and attenuate !;Om'" gJut.amate r..ceptor~"
IND~TIONS"
All 8n (lml Bdjuru:t to (llher drop in t .... at ing refl'8cl.Ijry plll'tiHI ~ ... i~U""8.
DOSE
Rx Adul t.: start .... ith 50 mgld and increlile ~Iowly up to 20().400 mgld", with no
s'gmficllnt ben~fit noted al dQS.a~a > 600 mgld i '. SIII"''''" ;II: 25. 100, &: 200 mg !.!llls
PHARMACOi<INITICS
30'16 il md8boli~~d in !.he liver. the I'tiIt ill excret.e<i "ncha nKed in the "rine.
-'" --TI'iiI~
{han.i1e)
(~SIale)
!ill - l (9-251irs
5-1 days
~
estabiStIeii
SIDE- EFFECTS
May in«re8JIe phenytoin concentration by up to 25%. Level s oftopirllmateare reduced by other AEDs Cphl'a.ytoin. carbamaze pine, valproic IIcid and possibly olheral.
Cognitive ill1p,&irmenll ..... ord fmding difficulty . problems ... jth C<)n""ntrllti,;m •.. ),
weigtn loss. dininess. ataxia . diplopia. pareathesias, nervousness .nd conrU~;Of\ ba ~
been troubleMIme. ~ I.S'A\- incidence of renol stones ..... hich WI"ally pan lpo ntaneously"
Otigohidrosis (redoced eweatingJ pnd hype.rthenn.ia. prima r ily in child ...m in Iluodution with el~Y8t.ed enviroomenl8l te.n'peT~tU1'8S and/or Yigol'O\.Is plly sicsl a.divity
NEUROSURGERY
13. &iZUTes
'"
~
tiagabinc (G!lbitril®)
\
I
OfIUO~O
\
,
A GABA ... pt/lke inhibitor, with eogni~iye problems ora sim ilar l'T equl!ncy to thet
witll topirsmate"".
Ri' Ad u lt, sla .... willl ~ mgld , ,,,creaM wukb by 4·8 mg to II maximum of32-56 mg
(divid....J BIO to QID). SU'I'PlJtD: 4, 12, 16 Ie 20 mg teblel.5.
13.4.3.1.
Most
se!%U~
Withdrawal 01 antiepileptlc drugs
recurrences d/)vejop during the r;ru6 montha aile. AED withdrawal" ,
INDICATIONS FOR AED Wlm!1RAWAl
Then! is no agreemel'\l on bow long a patient should be seiru re-frel! befQI"<! with.
drawal of lIntiC<loyuluRUI, nOt i. there agrllement on Lhe progTl0<5tie _allle of EEGt lind
on the but time IMriod ~er whicll to withdraw AEDa .
The FoLlow;n!!:;" based aD a study of92 patient!! w;UJ jd joDithil: epi leJl'lY, who had
bt!en rreeofsei~urea for two )'Par.... Gt.neraliwLion, e.g. til polIltrnumatic stizu.es, may
not be appro pri ate. Taper WQ3 by I "llJ\it" Q 2 W"ka (when! a unit UI deflnoo till 200 rng
for CBZ or valproie acid. or 100 mg for PHT). Follow-u p: IMAn ~ 26 11I0B (r lrlgf: 6-62).
3) pa~ientJi (8491,) reIDp>led. wiUl Ule 8V1!rsgt' lime to I"I!lapse beL~g 8 m(>ll (ranh"': i·
36). Usi ng act~rill l me thods. t he rigk for ncummce i. 5.9 \IIJmonth for 3 month •. then
2..7'WmonLh for 3 mon th!. then O.SlI<Imonth for 3 months. Fa.d.onl found to affect the likelihood of rel~p$e include:
i . ",,;wre Iyl"': 37"" rel"1"'1I rale for g:~nerIlJizl'd seizur",, : i6% fo?r«lmpiu or ~imple
partial; 54'1 for oompln part;"1 witb sec:ondary generalhalion
2. num ber of oelzl1UlI bl!fol't'_
w nLrollluained : thOllt' with
'"' 100 seizure! b~fore C\ln·
trol hlld slawt;cally lIignificaM higher ~Iapse rate
3. the number of drugs thai
hlld to bo1 Lried before 5i",le
drug therapy t~S9r~uy
contro lled seizuret: 29% if
llIldrug worked. 40% if 8
change to a 2nd drug "'as
needed.Wld 80% ifa cl>ange
to II 3rd drug WIlS required
~.
EW cias. (Ie<! Thl>le J3.12 j: cl81~ ~ had wo rst progn08;1 for reiap!ll!. Epileptiform
discharges on EEG se rv" to di/ICoursge AED withdrawal"'
In" larger random;~ed ewdy·. the.m06t ;'<lporUlat factors identified to prfldicLfreedom from recurr~nL seizu "-'"II were:
I . longe r seiz ure-free period
Table 13-13 Recommend ed AED withdrawal Umea
2. useofoni)·<Jne AED ('.....
multiple AEDft)
3. !lei~ull" ol.iler than to .. rc·c!on ie seizures
Wl r HDRAWAL TIMES
'I'he rerummended withdrawal times in TQilh: J3- J3
shO\lld be used (01)1 118 gu ide.
lin....
13.4.3.2.
Pregnancy and antlepUeptic drugs
W01)1 en of thildl;)e"ring potenti al with
ing pregnancy"".
""
1.3. Se izu'l!li
epile~ ahou l d
und e'l'l "",unuling rqnrd -
NEUROSURGERY
BIRTH CONTROL
AED~ that induce liver micro~o",al cytOChrome p.!>,>
enzymes (su Table 13- /01 ) increase the failure rate of"ral
oontrateptive~ up to fourfold". Patientll desiring to uSe
BCPa should employ barrier contraceptive me8lu res un_
til ovulation i, consistently suppressed, and they should
watch for breakthrough bleeding which may iodicate a
need for a change in the hormone dosag ..... Noo-oral hor.
monal contraceptives (e.g. levooorgel lrel implant (Nar ·
plaot®» circumventll first paM liver degradation but
should combined with a barrier method because afde<:lin·
ing effe<:tiveness with time .
Te b le13-14 Et1eetol AEDs
On liver cy1oc hrome p. 50 "
COMPUCATIONS DURING PREGNANCY
Women with epilepsy have mOre complications with pregnancy than mothers ... ith·
out epilepsy. but,. 90% of pregnancies have a favorable outcome".
There is an increalile in the number of gravid seizuTe$ in
_ 17%( reported range: 17-30%)0(epilepticwon,en, which may Table 13-15 Changel
be due to noncompliance or to changes of free drug levels of
In Ires AED level s d urAED~ during pregnancy t.:Hoe To1:tl~ 13· 15). l solalfd seizures
Ing pregnancY'"
can oceasionally be deleterious. but usually cause no problem.
Drug
Chlnge
Statu, epilepticus pose. serious ruk to mother and fetus during pregnancy and should be treated aggressively .
There is 01." a slightly increased risk of toxemia (HTN of
pregnancy) and fetal loss.
BIRTH DEFECTS
The incidence of fetal malformations in offspring of pnient.s with a known seizure
disorder is . 4·5%. or approximately double tha~oftM- general population*'. The degree
to which this is due to the use of AEDs vs. genetic and environmental fact.o.s is unknown.
All AEDs have tbe potential to eftuse deleterious "ffe<:t.s on the infanL Polytherapy is as·
sociated witb an increased risk over monotherapy in a more than additive manner.
Generally. the risk of seizures (witb possible concomitant maternal and fetal by·
pollia and acidO'ilis) is felt l.Oou t weigb the teratogenic risk of most AEDs, but this must
be evaluated on a cllse.by-case M sia. Oc<:a.iooally patienUl n,ay be weaned off AEDs.
S pecific drugs
Carbamazepine (CBZ) produced an increased incidence of "minor" malformations
(but notof "major" malformation s) in one studY" (t his study m'y bave had methodologic
prable",,). and may increase the inddenceofneuraJ tube defects {NTD)*'. In utero exposure to phenyl.(lin may lead to tbe fetal hydantoin syndrom .....·" and a child with an tQ
lower by ~ 10 points"'. Phenobarbital produced tbe highest incidence of major malforma_
tions (9.1%) in one prospective studt" and wa.o slw associated ... ith mOllt of the increllse
in fetal death or anomalies in anotb"r . tudy". Volproote (VA) causes the bighest incidence of mD (1-2%"), which can bedetected with a mniocentesis and allow an abortion
ifdesired. TID dOlling may reduce the risk ofNTD (see poge 274). Benzodiuepines given
ahortty before delivery ~an produce the "noppy infant syndrome''''''. Similar e(Tect./! may
QC<:ur ... itb other seda ting AEDs l uch lUI phenobarbit.aL
Dru g r ecomm e nd a tion s
A general consensus is that (or most Wamen of cbildbearing potentia! who require
AEDs. that monotherapy with the lowest dOlle o{CaZ tha t is effective is the method af
choice if the seizu.re disorder is Te$ponsive to itt". tfineffective, then monothe rapy with
valproic acid (with TID dosing) is currently tbe recommended Se<:ond choice. Folate supplementa tion (a fter confirming oonnal B" levels, lee poge 904/.i>ould be used in all .
13.5.
Seizure surgery
20% ofpatienta rontinue I.Q have seizures even with AED •. Many of the" patients
may be candidates for .urgie81 proceduTe$ to control their , eizures'.
NI';UROSUROERY
13. Seizure/l
'"
INDICATI ONS
Seizure diaorder must ~ s~ere, medkally refractory with I13ti. fa cl.ory tri,la ofto1uable medication for It least ~ 1 yea r, and disabling 1.0 the patient. Med italty n!h-actory i. ul ually con.idered two attem ptaofhigh .dolle monotherapy with two di , tinrt AEOa,
end one attempt at polythuapy ,
The thlll. ¥tneral categoriH ofpatienta . uilable fOT .ei~ulllaurgery h", . ...:
I. pa rtiBl ltiz u.e.
A. te mporal origi n: th e larpal gf')\Ip of surgical undidatea (HJ)KiaJly me, iaJ
temporal epilepsy whlell iI ofie n medically Illmdory)
B. ex tratempor. l orifin
2. seconde rily generalized It;Iu.ea: e,g, Lennox-Cntaut
3. unilate ral , multi focal epilep. y afloOClated wit h infantile hemipl egia . yndrome
E VALUATION
All patients ,1I0uld undel'll'l Imaging atooy to ru le out neopla. m, AVM. etc. Nonin·
"asi"e techniques aUow locali ution in the majority of cl _ .
N ONINVASIVE TECHNIQUES
MRI
Tile imaging modal ity of choice. E~tremely good for detectinghippoc.ampaluymmetry ormesial te mporal sderosia t hat may produce f;Omplex partial..,iwrtl (CPS) ....
CATSCAN
A $e izu .... focus may enhanze with IV contrast I hortly following a seizure. Subtle enhancement may be present on the . ide of the focus on interietal CT kiln ....
VloEO-EEG MONITORING
Most cente.. periOTUl pre-openoti"e long-tenu inp. tient ,'ideo-~EG monitoring t.o
correlate the c1inicaUy diaabli ng ""ilUre with appropriate elN:triuol abnormali ties and
possi bly to identify the sei~ure focus.
PET SCAN (POSfT1'ION EMISSION TC»/OGRAPHrJ
lnterictal PET sc. n uoing nuori nl!· 18 deoxyglu ..... (IIFOG) shows hxlmmetabolism
lat(lra li zed to thel id.oftempol'8llo~ focus in 70'11>oI'pstimts ... ith med ically refractory
CPS (dOH not t how actu , 1 W of origin). u""rul whl!n MRI and EEC uonnot localize.
SPEcr SCAN ($INOI.£ PHOTON EMISSION TC)t,f()OIW'HYJ
U~ t.o demonstrate increased blood now during a Itilure to help localize lite of on·
!Jet. 199m) Technetiu m (Te) hexam.l.byl· propy~ne·amine-oEime (HMPAO) ;. u~ually ad .
mini.te~ immediately a~r O:l!Jet Or lei~ r• • and thoe lean may be obcaiJled within
"-'Tal hou .....,
WADA TES7'AKA intTliurotid .mytal toeSt. Loca lizea dominant hemisphere (aide of language
fu nction l .nd _ _ ability orhemi. phere witl\out Ie, ion 1.0 mainttin memory when
;aolstad. U. ua lly rHeT'Yed for candidate, for large resectionl'"'.
Start witlla!1fiocr1m (m.)' uH IV digittl . ulXraetion angiotrrt-m (DSA» t.o as_
frOQ now ud to RIO persiltent trige minalartery. Signi licantcTOQ·n .... ia a re!ativeeontraindiuo tion to anelth.tiling ttl. lide or dominan t supply (patient roe' t.o I leep).
Wilda Uat may be r - i y matc:unol4l with hip flow AVM , Alao, poTtiOlll of hippoCampUl may be aupplied by po.tenor circulation (not anestheti1ed by lCA injection ).
EEe monil.orina: it uau.llr perfonned durine the teat wlltn it i. bein, done for Iti.
zure I u.ra:ery , Pat",nl will lllO"N deltt "'''_ duri", deepen I."el or anesthesia.
T echn iq ue
inl truct palient as to what it opectad
tatheteri1e ICA: ul u. lI)" l tart on aide of lei ion
'"
NE.UROSURGERY
have patient hGI':: contralateral ann in air, and instruct them to hGld it there
inject 100·125 mS"sodium amGbarbjtaJ (Amytal®) rapidly into internal carotid ar·
tery (effect start8 almost instantanl!<lusly, begins to subside afl.er_ 8 minutes
(may subside in _ 2 minutes with AVM where now rates are high»
detennine adequacy Gfil\jectiGn by asseasiog mGtor functiGn in elevat.ed arm
(shGuld be _ flaccid)
assess language skills by showing patient picturu Gf Gbjects and ask them to
name each Gne out loud and remember each Gne
assess memGry functiGn by asking patient to name a8 many Gf the pictures as they
can _ 15 mi.nuUll afte r test: if they have difficulty. ask them to pick out pictures
from a grGUp tha t contams additiGnal Gnell nat shown to patient
repeat prac~ure Gn Gther side (use lower Amytal dGses '... lth nch subsequen t in·
jecticm)
INVASIVE TECHNIQUES
EEG OBTAINED WITH INVASIVE ELECTRODES
Risk Gf infectiGa wi ,h depth electrodes'"': 2-10%.
Surface strip electrodes may be placed through a bUrT hGle.
Depth electrodes m:lY be plac~ stereGtactically. Temporal depth electrodes may be
helpful fOlr CPS, usually tG determine the laterali ty Gf the mesintemporal SOUT(:o:' nfseizure , Frontal depth electrodes a re also aometimes used . 2-3% risk Gfintrac~bral
hemorrhage'·'.
Subdural grid electrodes aC<l placed with a craniGtGmy. Thellf' SGmetime$ may allnw
su.mcient mapping to permilsurgery under general anesthesia ..... ithGut need fGr intraGp'
era tive mapping under local anesthesia (helpful in clUldren Gr in the mentally retarded).
SURGICAL CONSIDERATI ONS
Twn basic type8 nfpraceduC<l' ~sectiGns and disconnectiGns":
1. rellf'ctiGns
A. resectiGn of epileptic focuB: higher chance Gf completely CGntrolling seizures.
PerfGrm~ ; 1I nGneloquent brain. Seizures must have focal Gnset (resectioo
nGt encouraged ifmultifocal Olnset) . lnc1udea:
I. IUlterinr temporallobec:tomy: su twtGW
2. amygdalo-hippocampedomy
3. neocortical ~sectiGn8: especially with neurGnal migratiGn abnGrmllli·
ties
B. resectiOln Gf lesiGn in secondary epilepay (e.g. tumCtr, AVM, (8vecoous
malfnrmatiOln'''" .. .). In mOllt cases the seiture focus is in Gr nea:r the leBinn,
but $Gme structuraJ lesiGns aC<l nOlt responsible fOlrthe seizUC<l$. FOlr seizure
foci within me temporaJ IGbe, sei~uC<l control i, better when JesiGnectomy ill
accompanied byamygdalo-hippocampectomy'''"
2. disconoectinns: used when eloquent brain is lnvOllved, nrto sep8:rllte t he electrical
activity nfthe twG «!C<lbral hemispherell
A. ocetion Gf """,,"3 ."lIosu .... (o"ll0e0tomy): when d .... p Pt""O"," pre the ", .... t
disabling seizure type Gr fGr multiple bilateral foci (.«< fwlow)
B. hemispherectomy: fnr unilateral seizure.s with wic.esprelld hemispheric Ie·
siGns and profOlu nd contralateral neurologic deficit. FunctiGnal hemi·
spherectom y isolates the abnGrmallide with _ 80"" seizure control rate
(similar to anatomiC hemispherectomy with pres<>l"Vatinn Gf the baBal glln·
gl ia, but with lower compliClltiGn rate)
C. multiple subpial transectiGn"': fGr partial sei~ure Griginating in elOQuent
CGrtical areaS. ThecGrteK is transacted at 5 mm intervals, thus intelTUpting
tbe hOlrizGntal spread nfthe seizu re while spa ri", the vertically Olriented
functiGnal fibers
ANESTHETIC CONSIDEPATIONS
If intraOlperative electrocorticography is to be perfGrmed:
NEUROSURGERY
13.
Sei~ures
'"
uDder local anesthesia: theoDly anesthetic agents that may be used are narcotics
(usually fen!.anyll and droperidol (the components oflnn(IVBr®)
under genersl anesthesia: ~ benzooioupines and barbiturates
INTRAOPERATIVE ELECmcx;ORTICOGRAPHY (ECoG)
May be pe,;orroed with , urfa"" maw that includes superior temporal gyn>s and
inferior frontal gyn>s. Depth electrode.! in the amygdala (3 cm from temporal tip) and
hippoo:ampus (5 cm (rom temporal tip) may also be used.
Methohexital {Brevitol@)maybegiven:observeforJ fast activity io s uapected focus.
INTRAOPERA nVE CORTICAL SnlofUlATION
For Icx:oting motor strip, sensory cortex, Or speech ""nters intraoperatively. Deter·
mination bas...! On visible ana lomy is unreliab le. For 8J11l"ch center. stimulate cortex
while patient names objects shown on picture cards (automatic verb3.1i~atiOll> such as
counting, is robust and may p<'rsist ). Observe for effect/! ranging from lo!.al speech arnlSt
to paraphuic errors.
Typical settings for a cons!.ant current generator
using 0 bipolar electrode ore shown in TOlI>J~ 13· 16. If Tsble 13-16 Senlngs lor cona voltage based unit is used , start at I vOllt and in ·
. Ienl CUfTenlge n&ralor
crease.
CORPUS CALL OSOTOMY
Psrtialor total section may be most elTective for
gene raljzed mitior moto r seizures. or little benl'fit for
simple or complex seizures. Benefit has been supported for:
L frequent episodes of~.lI..WI ("drop at·
tacu") where loss ofpr;>sturallone - falls and
injuries '" (70% reduction with callosotomy)
2, jlO:Ssibly for generalized seizure disorder with unilate ral hemisphere da mage (e.g,
iD fantile hemiplegia syndrome): hemicortical resection may be better for this
type, whereas callosotomy may promote partial sei zures.
Note: Q "functional hemispherectomy" i8 recommend...! OVl'r "anatomically complete- hem;~ pherectomy to reduce morbidity ond mortali ty'"
S. some patients with geoeralized seizures without identifiable. resectable focu!
Division of the anterior two thirds of the corpus callosum (CC) (minimize. the risk
of disconnection syndrome. su b«low) may be advsntageous over complete collosotomy
(controversial). Some advocate sectioning the CC with intraoperative EEG un t il the typical bisynchronous discharges that are usually ~n become asynchrOIlous "'. No need to
"""tion anterior oom misure. Can u.ually be pe rformed via a bi fronta l craniotomy utiliz_
ing a bicoronal skin incision.
May produce post-op I v.. rbalization or akinet ic mutism that usua lly resolves in
w~u. ~ Contraindication: major behaviora l andlo r language deficits may occur even
with partial division in patients with speech and dominant handedness located in .Qjlj&
W hemispheres ("crossed dominance"l. Thus. Wada test i$ reeonlmended in aU len
handed patients.
MRI sagitta l cuts are superb for assessing extent ofdhtlsion of the CC''',
,,
DISCONNECTION SYNDROME
In a patient with a dominant left hemisphere, conaisl8 orlen tactile anomia , left sid ed dys prax.ia (may resemble hemiparesis). pseudohemianopais, right sided anomia for
smell, impaired spatial synthosis of right hand resulting in difJicultytopyingcomplex lig·
ures. decreased spontaneity of speech, incontinence ,
More COmmon with larger surgical """tions oftbe CC. Risk is le~s if the anterior
commisure is spared. Patients usually adapt af\er2-3 DloDths, with final function normsl
for most daily activities (deficits may show up on neuropsychologicsl testing).
TeMPORAL LOBECTOMV
80% or patients with medically intractable sei~ures with demoTl6trsble (ocus have
foci in anterior temporal lobe. Most patients have neuronal 1088 a nd gliosis of mesial temporal struot ures. Thus, a standard resect io n of temporal ti p (often wi th Bmygdalo- hippoc_
13. Sei1ure$
.VEUROSURGERY
ampectomy) may be performed.
Limi ts of re"ootion (without aia-nificllnt oe urologic deficit)
Not.:! tbat th~e valu" an! generally con.idered .afe, howe'>'e., variat ion. occur from
patient to pIItient and only inll'tloperlltive mapping can reliably determine the location
oflanguas-e «nle .."'. Some ~ot.:! rt .pare the superior tempore.llQ'ruI"·, Tlte following
measure menta aN! made along the m.illlI.lt. temporal gyrol
dQmioan1 temporal lobe: up to 4·6 em may be removed , Ove"'n!OJe(:!ion may injUn!
,peec h ~n t.:!ra. which caOOOI be reHably loc:ali1ed vilually
non.dominant t.:!mpo.el lobe: 6·7 em mey be rue<:ted . Slip! ove r.resection may
- partial eonlralate... 1uppe r !lund ... n! hornonymoua htmienopsia; l'U<!dion of89 cm - complete !luad... ntllnopyia
Alternatively, intraoperelive electrorortico,,"l'aphy may be ulled to guide reaection of
el\lCtricaUy abnorma l areu .
RelICti on .hould b. performed in .ubpial plane ttl prevent il\iuT}' to MCA bTanchM.
AM VGOALD-HIPPQCAMPECTOMV
The amygdala liea in the roof of the ant.:!rior t4!mporal hom of~he lat4!ral ventricle.
two buic approachea:
I . t'8II.cortical: ima~ guidance i. very helpful
A. Niemeyer approach "': 2-3 em longitudinal cortic&1 incision through the
middle temporal gyrus centered . t a point _" em JIOIt4!rior to the tempo.."l
tip
B. approach through the anterior superior tempo.."l cyrus
2. transylvian: approach advocated by V.sargil. More ""'tfictive and great4!r ri. k of
injury to Ml portion of MCA within . yMan fiMure
Complications: va...,ular injury i, the most significant rilk,
RISKS OF SEIZURE SURGERY
Major riil<l; are related to' '':
1. removal of e!lSlmLial areas ofcorteJ:
2 , injury to meduUary core underlying cortieal resection (projection fibera, 855 001 ,
lion fibers. and/or commi8sura! fiber'): the ITI06t common deficit after tempo..,,1
lobectomy il a contralateral (homonymoul) . uperior !luadrantanoplil (1CKII1led
·pit·in·the-9ki'defect, due to an injuT)' to Meyera loop .... herein the fibe .. for the
superior vis ual field of the optic .."d;ation t.akoe a slight rostral "detour" I.owaro.
the tempo..,,1 tip)
3. injury to vtasoels in area of mection - ischemM: damagoo to areu supplied: "p"d ally sylv;8II branches durin( tempo<1lllobectomy or ACA branches with corpus
callosotomy
4 . injuT}' to nearby c.."n'al ""rv,,: especially third ""~ during hippocampectomy
whre it liea medial to tentorium
PERIOPERATIVE MANAGEMENT FOR SEIZURE SURGERY
Mlna,oemoent dun", eva lualion:
During period when A.EDl l n! beingt.lpered, pa!ient . hou!d beobserved 9t.1I times
(for paLitnta not in ICU. a 201 hour·a-day aitter i. required ).
PRE-(JP ORD£RS (EPN.EPrIC SURGEflY)
I . taper antkonvu:... ota. completely ])IC 1 day before surgery
2. 10 ml Decadron® PO h! bero", , uT(lry .•epeat PO or TV On AM of l urgery
3. ilKi&.um drytlpp: phenob.ri;,it.al 130 ml TV (. < 100 IIlwmin)
PosT-QP OROERS (EPfLEPTIC SURGERY)
I . ror ",i1u r" in the immediate po.tt-op period ("honeym«ln tei~UI'ea;·), not n"",·
. ary to treat only one brier genel'tll iled lIilU"'. otherwise load appropriately with
phenytoin or phenobarbital;
2. continue 4 mg dnameth"l0~ ( Decadr0r4) PO !I 6 hfl k ~, then taper over
nut week (eatential to maintain for full ....eek)
NEUROSURGERY
13. Seizu ...
'"
3.
4.
anticanvulsants aTe continued X 1·2 years even ifno po8t-<>p sei zures OCCur
before discharge:
A. neuropsychia tric evaluation
B. serum anticonvulsant level
C. EEG
OUTCOME
(VYrrn A£S;;:CTION OF SEIZUf'lE fOCUS)
The greatest effect of seizure surgery is adJ.ltli9n o(lICi= frt'9uency'''. however.
any surgical procedure way fai l to have a beneficial effect.
Sf.izure con trol is usually assessed at 1.3 & 6 most post ap. and then annually. A
POSt..OP MRI i$ usually obtained at 3 most post..op to assess extent oflurgical resection.
Most patien ts take anti-epileptie dru gs (AEDa) far 2 years post-op, and then may be dis·
con tinu ed in those free ofsazurea.
Recurrent seizures: although late seizures may occur, 90% of sei1u re8 that recu r da
sa within 2 yearll.
2yeano post-ap in patients maintained on AEDs: 5O'Ji> are seizur .... froo, and 80% have
ove r 50% reduction ofiaz"re frequency .
Far temporallobectomies ,n the dom inant hemisphere without intrllaperat;ve mon·
itoring, there is a 6% risk af mild dysphasis. Significant memory deficits occur in ~ 2%.
References
13.6.
c.""...."'" "" CI."if",..... ..., Tcmli .. ",,~ of
II>< I.,."..,,,,,,,", Lel , ,,,, A""o" Ep;k",~ , Prop<><oL
Il .
r", .....;>«Icli nkolond ."",u<><"""p"""",pI<i<
1.
f"'t"""
Com ..." ...... CI ....
and T<rminolon of
IlIc l"",mMl"". , W, .. AI'''''' Epo1c1"7' Ovj,jo·
l.
6.
I....
'nt<,io;:IOI .fMl i<tal ",.Ipo""'"",,,,,,,pbo~.
11,
'""""oJ
""v",ps)'<""Io;;':ol ''''' ",. neoroi"", ,,,,.
rc"" .... "" P"""Iof',
N.~rol l<l· 781 ·1 . 19113.
EOld lJ. S""",, ro.- ,.1,"1'<' . N toll J Mod )}4,
641·)2. '996.
R A. POll')'''"!"",,,", C P. I.""nolo .. y.
""0
On"""••",
S.
9.
10.
II,
OC:IO,,,oep".PSY. A '''''' ... A"'. """"")I/: )90041.
19\13.
!I ...... W A.A .... ,. ... IF. K ~ancllT: I ...... _
01 'fIl"'psy"" ~od ..... "'" •• Iloch<"<f.
Mi • ....,. •• 19)1· 19S4 . EpI"'Pl-b ",. 453·68. '993
Hou""W A.A""....,. V E.Lo< ......... R 8 . <lDI
Se ...... r« ...... _ . fI< •• r. ..., .ni"<'voI.od .. i.. ~
N... [old J ~ t . d J(\1: Sll·'.19n.
11.<,,11 I. Icv;..... n HS. NaJ" .~.m. H."al, Seizv ....
>In>ke: Prodi<toB.nd ~no.". "lO;ro·
;n
""_. Tho: COp<nJI,&< n ~""'. "o<IT.
15;
'S'S·S9.1m.
Landr."' N.O .. ..,..· ~ """." M . W .ib1cyR E. <lol_
Now ",,10' childhood 1<.. "" " Eme,.... ) "'1II"l.
""""'11<';'..0. J Fl. M<d ....... 79: 697·7((1.
"".1<
Sir"".
,m.
12
Ha .... W A. Ro<IIS S, 10«>11, r.t
P. ~"'I. :
Pu"""
po''''.''
oI><;~_""" ....:l""'"rr.-0u4 ••
",ilb ... " Iy d"JnOOO<!'pi I<PSI". Epllq><Io 2a: S ' 6-1,
'"
,.
Ii ... f", .po<Iem.oIo,o< _ .. , "" <p.kps, . ~ pl ltp .
"' lO, J89·9II,19S9.
Mo«.. ,,~ R ~ .So EL- A<I""., _ _ h '011>0:
d.".~ "o. or >e> .. f<, """ <p;kpI:< .,,.,,.,,,,..,
M. ",ctI~ ...... ,1 : ~5·1 •. I9%.
F","""J A. W.III" ...... P D.ThoGao; v 101, <lDI"
a.....:''''''0CI 0( • •• ,1i0/ «mpenllObo: <pikp" . 1.
Ro"l .. oI tH'''''JI_p~,''nl .>omi_, Aon
Ncurol :14: n ..lIO. \993
Willi.m30n P D, F,.."h I A. Thad •• i V M .<la/,
Cban<t<ri" . :< of m«IlOl,ompen llobl: opd<poy. ll.
••
•.
1S. Seilures
>du',
,diopo'"''
• ,.. "r", ..1oo 0( <plkp"" .. i....".. EpUopol. 11;
4S9 ·~1. 19S1 .
1913 (t b"""').
• ... 000",,.,, C. Sehim"""""" R.J. G«IU A T."
"'" V.1v.cf 'h<.I<ct .... "'<pho~m '0
po •
tI.n" "ith .'"reotod
r"" ..." ..... A....
_<Ot4~ : 1ll-7.1m.
Y"",,&O .Row RP.N_ n JA.,,"'.: F,,' ... of
~rb:,i<;al1, o<I""oill.,od p""nY'O.n '"
I... po<I"................... J N...,.... " l
IS.
P"'''''''
~
2J6.
41.1\18).
A_tenJ F.Or.bo.d D co--.:. R V. o,"'.: Se,·
•• '"" . 1Ier _ "'vmo; A
Nn·
<oIof.J XI. 683-'1. I990.
B.lk>: ~ R.a...n" R M.CI;I'\oo(; • .,..,.; (;.ioIe11... 1.. 'ht "'t ".rt""" 01 ....... ~...:IIQj.'l' .
The 0", .. r",um' f ou""",ion(l'/<w YM.,l. Tho:
A...
of 1«"""",ic:0/ S.'r<"'"
IPorI! R",,. . llIinoi,). orIIl The Join, Soc,i,., of 1'1< ••
""..."" oM Oi'o<.'Catc, 19111 .
M<Que<. I K. B100:~_ DH R.Horri, P. <la/ '
Low riol<ol 10.. poII"'u",,,,, "',vm I"U"".. , ...
PDI'I'i""'" ,,0<1,.
nc'. ,,,,,,,,,i..;,,.,
, ... I,..d 'nJUlY. J Ne.,01 Ne.!'$01l:
~y<bl'h" y
06: 3911·9001. l'IIIl .
II.
y""", O. R.pp R P. Non<" 1 A... o/.: F.II ... 01
","""yla:,ic:. lIy od .....
ph<O)'lOin '" "" .. '"
...~~
19.
20.
2 1,
..,.tod
_"....... ,>0: ..,...... J ............... >3: n, ·
'.I98J.
H..... y S.fIoOI>. S, A..---yA M, .,<IIo F.. <O<J;n·
n..."""" """",""",,'0; ..
<h;I<I.... Nn.....
•..,rtcy 1); SM·l. ' 9l!8
W.i.. O H.sa.... A M. V-. SC.""" I'I--.o\i<,.
'" I
<pikp<, io P< ~.I _
i.jo·
'Y. ""h Ncurol 4): ?1 1 ·~. 1986,
T.mI<inN R. D,l.meoSS . Winn H R: I'oo!n. .... 'I<
C~G Non llA..... 1, .lS-J5.
Lt."" ...
poo,,,,,u.,.."
.. ....... 1'.",....."
,~,
11 .
Tom~i.N R.Di~""nS
S. W;kn>l<, A 1.<101,: A
m""...I.«I, _ k .bllnd "od)' ofpno:ny,,"" ro.- ....
poi'' '.....1ic ..i....,.. N Er>zI J
M..t 321. 4<n·lOl.199O.
pn: .... ioo of
1)
1'.
O;~ .... S $, T<"",I.1< Il .Millet B... IfI.: I«.tOOoIuo • ...., .rr""" of ph<"J'<oin pmpII,l .. " of pool'
,," ...... ic:"''''k$, JAMA 1M: 1171 ·7.19\1.
HoIri..... A M . N .~I D W. Tcml.l.NIl.<lal, Sid<
;"'EUROSURGERY
">o<",cd ..;u, ... 0( "","y.
1"""'".....'" wi.... propIoyl>,I, J
orr""", """ ......m!I'y
1<1;" f ... mly
".
~6 .
".
"
N.
<.
"
"
".
"
".
".
".
"
"
~.
"
N... reo." 91: n8·91. I'M
Yob"", SA' I'O>'lao.... "' •.,'.... " «h Phy>
Med II."".,;) 70, 91)· 1001, 1991
Nonn) B. J'cl,h. 1I It K. H,.,"" 1< ... uI.' """"ylOi.
jlO>~"" <1'11<,..1: I< _1o·~I,"" >ludy.J
N.u ...... " sa, 61l-l. IWI
Ooorn... M E.S;""",1t P'~'JOA : EliIMIoI
""" " .... "'''''' .y ..... . " Eo\~1 J Mod lll. 44l·~ ••
,""
19~ .
L..oc""n!>cfJ R. Womc,T 101: Sol,.", ""~ .... ,,,,...
• • mnl .1coh<>I oxlO,irlC.. ...., . Arch ..... f"OI 41'
~)s.s. 1990.
C'haboI I, I) R. Krahn I. E. s.o EI, "", . ,,"ydlOl"i< f101"I<~Itp1'" ,,1,",.<, .\1.yo CII. I"r<>< 7" .9J·
~.I9\16
0 .... I It . It......, V. Wh . ~n 5 . .,4L 10111 clu_
.. ,,";.-. of p><u~",,,• •. A«h lII ... roI.2. III)·
7.1985.
Kin. D W.G>II>.Vo: ' II II. M_In AI. ,,"'" 1'><,.
_ " , .... 0" , _ ,,, •• , ''''''' . N''''oIocrll,
18·2).1'182.
1I.."'luT F.T..,l.,OM. F"", I, ,,~I,' MMPI io·
dice< In ,he i<1c .. lf""'...., of PO'''"'' .. ltIc"''"~
p....k,,,,I,,,,,,. Epl!.poIo ~9' I SO·7. ''lS8
Wyll" F.. I.ud<r1 H, M",Millo. I p, "41,: Sorum
pr<>I><"n 10,,1•• flcr <piJe",1c "'ltUm, N,.roIov
).0. 1001 .... 198-< .
DoN·t!acft J. Trimbl< M R. o.l.y l : Prol""' ,n and
,_",,"n.~on v. ro111:"',n'8<""""i-, ~
pulill ..1..,«, J ..... ""' ""' ........ 111 1'» 'chI • .,y
06: lll · S.I 9i ) .
'rid,,,,, P 8. W,._or II a.s"" , J."QI_ So·
"'''' P<Oloc'i' 00'I<I _,001 ...... " ," .,..luu"'" of
.,.._pltp''' "l,ureo. A.... Nturol "'17·9.
~, K D. M.llooly I P.H..-II 6; P>o'.cIln
wnll<' ,~" .. ,"' .... ,!> .. ,fo«! by EE(; mooi' ...•
i",. N• .....,...,.. )S, 11·~. 19S~.
Abbon RJ . 8",""",C MC K, 00 __
Ol W. So·
""" proI>cIl. >till CO!1i .... concrnu .. lo,,, Ir... . ......
mol .. I•• _ . J N,_ N< ....... -,: "'y<lllo,..,. "1,
16)·1, 1980.
J><l<1 R A. MIl .......". O. TnY(ldl R. If <rI.: R<do<·
1"",0(
"IJ>O'I~ ,."h "pc,;,;", " I,.m .
~e p,1o U ' SIS. '931.
T"",,,,"T. I ~_ U.
8 Y.trQI_ SoNM
do';", ",,",.p;Icp1i<u •. J " ... tQI .... y ....
...... Psy,~ ... 'l" 52 . 1 4l~"1 . ' 989.
SpMinl M R, Pru,h¥<!' ,. """I J. " "'" FroIo<.
,io ;. ",n,,1 ,p;I<f'>Y: An ood«" '" <)fl,mtr« 1<,.
......... ". r<... roI :!II: 71(,,21. 1\>36,
M... ~O<d U .~ S.LICbll"'.S . .rQl,oeomI*i_ of "" efl«:1"" lre"101 """ .. _ I lob<
""n .. I .. ; ..... ..,
ic.vel . . ..... b 1'1 ... ,.1.9'
proI""".
,.l._
p<OJ.,,,,,,
JPIOI"""
".
1hN·l1ocIlJ. Trimbl< M k ' """"'". and"....,...
,up;. '100' .... (ull........ "
I" .pik ....po,Otnu,..I'h and owi_ F'Y<hopoIhololl' 8io1
P,y.hI01'l" 19, )Z9-l6. I9&-<.
H,,,,,, AG . _ , n: QIKI ,rodi. , ... rdI ~,01
49. n1 .... 1991 (ed ,torl.l)
V.n'yC M .Cold'",J ' Ri •• of <pll'pol,r.. , f<tnle
_,ol,i..,,, A owionol «>lIOn >lwy. 1I.\1J JOl
1)1l.(,. 1991 ,
r ....... IIJ ~. La Y l.I1"" 00 ... 1>1" F't><oobutial
for ft"b<il ...;'"" •. <II"«" 00 ,",,11;11<_ """ on
.. I,." «<u"""".N F.dJlJ M.d lU- J601·9.1990
R.,."",nN P.CoI, .. T.l..lbO.",J . .. 0), A <Oft..
IJOliod ",.1 old,,,,,,,,," lId"'i";"''''' donn, f<brilo
i"...." '0 i>«vetr1 ... unu<:< of fdonl< .... i..... . N
F.r>;IJ .'1«1 l29' 19·84. '99) .
\\''''',nl G""'P" S,at •• Epil<p"'''' Tre",mcm of
"""" I.i.. """<pil'plco"J" MA no; BSoO·9.
4.
H," .. , W A' SUlu. ,p;ltplicoo: Ep,o\<m,oIoc'" """.
~.
"
~.
~.
"
"
B
"B.
•
"
".
"
W
'ID.
n~·lO.I99~ .
"
".
... ,_ion>.
1""'' '' ........
,W;
NEUROSURGERY
".
•
"
o.
N... """",.'HSoppi 2t. 9-1). 1990.
I'I"I)I,..S A,ShaUIIM R I. EI>oJocyond ...,.,,111)"
of ..... , ,pikpoi<us ;" ,,,IIII,en, "I"<h N... NI~ :
1'-6.I!I89.
It J.'dloc~ I M.T"...", A 1t.... aI" Ep.
Idcmiolo&y or JIr. •• <P'I<j>Ii<., . J Cti. N.......
pII.)"IIoI' I: 112·U. I99S.
FoonW' N 8.
E w, P.. lIOpIIy''''loIy or
""."pilo",;"",.J Clio Ne. n>pby<lolll: )16-. l.
I99S,
O'lpdo-I'.Icuc ..... V, W.... ,I.,.C.T......... OM.
"4/' Man.og"""" of _., cpll<",Ic\l" N t.>gI J
.'>'I«IJ06: 1))1-0.1982
8 . _ E.F ...",..J M: S.-.uupil<p'ic",. F<d, In
R.,I.", • • la ~. 19112.
CU"tOO e 0 , C. ...-.JI'-«I """ ...1...... >I""' 'pd<f'"
'''u •• M.,., CU& Fr0<11: "1117·91. 19\16.
.....y It J. K,.11 It I" T".,m<ftl of " . '" ,p,lcpol""
1O<uo~ , .. ...,h III... , "~! ' 005-11.191)01
\..oW,n,,,,lnl) H.... ",lnoIfMJ.S,mooR P' B. tto, •.
...'" ......,~.".'n:l>< U,,,',,,,OI of" .. ", <plJep1"."
C!i.",.I .. pcn,. ",. ... ,,~ I.
"'''' ''''''11 1':
J95·oI()(I.l'1U.
0....;.,1._ R CO T"""..... of,.r_1OO)'
.h"'" ",no:-<"",,, "',u, .pH<p1i'., ... ,," II<noobor.
b,lIl
fI.,. ~iJlr _ pheJrylOln.
F.pll,poio 1O, 006< ·7 1. 1989 .
01&0,1). M,II,"", M: Lon.!'pam ""., dim"""
for III< '<u""'", of .to'u> 'p1Icp<1c • •. hd ..... III",·
",I 4' ljl·61. 1918
AppIc<orr It, S_"'1 ". 0I0arr .... I, <1.0/,
Lot"'"l"m ....... di.... pom ;" u... ""'" "eatme,,,
of <J>llcp<ie .. i,." • ..., " " ••• piltpicu •. 0 ..
M", C ~1 1d N.. f"OI )7. 68H.lm.
C...... f<Jr<lTO.Mi'chcli We.
5 R.
I.o<' .. ",m ,.<~ IIoJ_ " . '"" <fI'I<p""''''' ",,,.1
.. i...... m«u ................ ""hypl'ly\o.oi•. N...,oIoII1l 7.19Q.5.19f7,
Ub>r 0 R. .-....hm .... R_ J, Hi .... _
,",,,,,,
_.1000 ..1"" roo "" ~,,,••crllor .. f"""'l' ... 'LK
<PI1op11""'.N<wt>IoU.wo '..:)).1.1_.
Brod,. M J. Oi<l,." M A: An",,,,I.poiclirlll,. 1II
l~ J :I'I«I )4' 1M-1$. 19901.
M"""" R H . ~J A.Coll""l
COM'
pori>ot> of C"Mbomo:>q>i"'. pt><_I. phcoy","
In . ...t pri't'"d",,, ;., p"'iol''''' orawbrily
1<",,,11«>1 ",""..,1001< ..1...... III F.... 'I J 101«1
lll' 1.~5'. I'lSS.
M.. _R H.C- I A.CoIIi ... ' F. ..
_ _ of'll_"'''~<_''p1'''' r...,~
........ '" of «)nIpI<. """1. 1...,.,,,. """ _
Iy 11<",,,,1,...,
I" ..s..1 ... 1'1
~ J M.d )17' 7(o}.71. 1991
Oruf. (""pilop'r· M«I 1.<,,« l3, 91 .). 1936
R ._ ~ 8.8o<.i", H E, ~nlop " . .. .0/, """",,,'"l phc")'1Oln_. I< ......... """""""', Tl>t,
~ M""H I: )!S.)). 1919.
SoLI"') I.G" ... R H,SIwp W P.I""""'ionof
,..iI . ....... 1..-di,~.,J r ...... E.,
Null 1(1' In·). 1986.
w""",.J P. WoodC A, W"",,,...,C H' """n)'\WI
.nd _ C'>I,I< foodlnl" NeuJ"Olov}oO: 132. 19S00
0._"""
L<l1",....,
...i,"
po'''.''
1''''''
_"he....
So"""...
f."""
"'""'ooon-
101',""''''''''' "''''''''
•"
".
o.
".
ro
"
"
"
"
".
"........'''''n
(1<,,,,).
8 .... 1.. I! A. 0.,,",,", O. v,n War. M. " aI .. "".
n,..1
of "'~ of "" I.,", hJdloIHOi" . y...
..... 111< N E~JhI«I Jll: 1$(07.72.1990.
1'U~i< H" "1r So"'i«: FIuo> .. ""cphclrytOlll ,.. " .
"","o... . fl)A M~ Bulltrltl 200, 3-<. '990
Winltlo,S R.I_M S' ... ",,,,,,il<p1I<~"" .......
PorI I.
1II...,..,a _9: 449·S2. ,m
Ole! K S. w"'1>t M.I'..,l' J 1\ : C.'O$''''I'"I< ......
kif" ' il"' a", '" d"" I........ '....,: Toyotol ,nd
Oorv .. , So ... N... ,01 31, I"'·! I. 1!I89 ,
CIak ..hou P. H... 0 M: V.I""", •• rId ""., bind•.
II. M«I J 198, 1m-I . 1m.
W,""i<w:ok; B ... C ... in W H: ()r,ce.dal ly rodmlni.·
I'" '''' of pocoob.>rtoi"l I. odul", Clinical <lr"*'1
ptoll"'"'"
s.. ...
SeillJJ'eS
'"
".
•
"
..••
~
".
•
n
• ocI bt""r" . Arcb N<urol .l . /MI· 700. 1981 .
0. ... " Q.Muo:h .. K O. ~""'J II . • "tI.:
On«·(\O,ly oIo<,nl .. ,1Jo ph<"""".".,I • • Mdt<n
.. "h """, .. di_". PtdI "rI.. 68. 12.·). 1981 .
Felhom ... . Mod "',.... )S, 10J ·~ . llI'Jl .
Wiol./<, 5 M.l .. , M $.A!IO,.,iiopo'" w.,. ..........
Pon 2 Su'1i " ..,..., 4<1. X>6-1. 1m,
(lol:>ap<n"n.A_>lIti<on,.,..., Mcd 1.<11<, )6,
~, I 99-l
,m
~""",;" .. 1<lf<pil<f"J, ~'cd
l.ri'" 37. 21.3•
u.-",,,,
C ..""" R. /)Lt ... , C.C • . - p • ., .'.
oI,..j
'i"" ,. ',,,.:rr "')'00""';'; .pilep.
' y. [pu.poI. l~ : ~·Il. 1998.
r opi,..". .. I", <II'lq»y . Mtd 1.<:I .. e )9. SI·l .
'99),
E. W,lda 8 I. R.m .. y R i . .. I>I. Top, ..•
"'... pI_",",,,,,k<I_'''.,;''llnol in ..I .....
IO<y ~.i.1 <1"l<9>y •• i.1 200 •• 4(1). •• nd 6OI).m;
d.ill~ . N ... """,,06' 1/>1:4·90. 1996.
Pr....... M,FiDCh""'It.~')' J. ... MI · Topi .......
pl .. doO-<omrolk4 _·".Ii.,..-Iol in ... f..c,Ot)'
.pik".1 ",inl 0\00., soo..>nd I JXIO."" d.i·
11 -...." . NtUTO!otD "". 167S-13, 1996.
Ti ....i.. l",opil<p>Y. Me.d L<1 .. e40, .S-6. 1991
Sm._, E 1\, Epil.poy i. _ . , M.y.
11 9'11 ·9.1996.
C.II •• ~", ,.,. C.~" A. Cocci. T , W,LM ...... ' ~f
• ",i«>...'"., dru,. ,.
Ir« of
for
J Mod lIS' 9-lH,. ,9$1.
1\-.0. T. 6 ... ,,,..C.I'<,,_A,,,,,'., II ."",.
"..i>oo ..,,_._.001 Ill ...
.~ "'_."i_.".I<".~: A P!O>PK'"''
" ""y. 1I The EEG .. p!<d...."or .."'o.... I",
..."", .....1of ,.....' ...... . ;";1.,.... ll: 22S-J2 .
• 9\17.
Mo4i<.'I1 ...""h C.... ill\.'i.,;l ...... Otul Wi'h·
d, . .... , S''"'1 C,,",p. R _ .... """1 of ..... p;.
10",1< (In., ...;tMo. .. oI"'~"
Lo . .. , Jl7 (I1S1t. 117S-!IO . 1991,
D"'~&O: .. " II. I.,,, D: eoru. ..... I.id.I, ... ,
""" ..... ,. _ _ n.. I' ~'._ ....... or:! ..... oI
oh<
·"h <pil<".,. 1'1", ,,,,,,,,'1
(S.ppl S~ 149-60.1991.
101",..,.. R H.C .. ...,. I A.n.rn.y P D." at · UIe""
1 ............ i'~ <II,lepl1 Jo\MA
m . 1JS.<1O. 19S~ .
Po"", .. E. H<dJeO A.I,UH, K A.
•" .. """1 of 111< ",I." ... en" ... i"'''"in5 proper.
, ... of ",tI<oo .. ~ ... dIU" in 'pile", .. pot.."" . Be
J ClIo I ' I L _ /I' 401·10. '''''.
V,~ M S. F.. ,I P N. McCorm,O! K: 1\""1"1<1""
dlUl d""",,,,,," durinl
"',ur%p" '1
(S.ppi SJ. 11-6. 1m
Di ... M S.5<.." .. L N: 1"_,,..;,) fLo""""",,,
I""" ..."')' .... oI,..j _r"'''''''''' moll....-Ion.
~iO£ "',"""'1'ocI II,. _"",n"", N........
......"" 1l.ljS·66. 1990.
I""", K L. 1.0<", R V.JoILn_ K 11.,,1>1.. P.".""
oJ ,..11.",...,-. in ,flo </.;"",. of _ . "."cd
... ;,h ••"" .....
duno, PfCI'-<I. N "".' J
Mcd )1(10 1661·6. 1919 ,
Rw.o F w · Spin. tor.,. i. ,., ..... .,.....,.... ' ....cd
..,'h<ut.",..... pi .. duLinIP"'I...-.:l N EnJlJ
M«I Jl': 61' .1 . 1991
Han._ J W. Smidt D W: The fetal hydo."';'
d ....... . J PftIO" 17. 28$·90. 19~' .
S<oI.ok D, Nul", •• I, Roo<! J. '"
N.Lll<U1'01op..... 01 <hi"'« ...1">'«1 ,n"""" to""")1Oin .nd
st""'" ."....
F,.""
..
1'0.""
~.
U.
"
...
..
~.
"
"
"
eu.. """,
'''''')'UN. '" .:.."
),<-,1>"""""''' ",
... ", ,."n;"",...
1""'.'" "'''''''...
....,"""''"''''pU.....
..
"
•
•
";"n:'
1"'''''''
.,.1_" __
1"""""'"
,..v:
'Y"
.1.
.>tbam>t<pi"" "''''''''hrnpy. JA.\lA 211 . 167·70 •
•
•
""
'"
101.
,~ .
NIok_ V.Ok.m.r. TilL"'."" M... ~I' M uk,~ ...
"i"H;."w ..O<l, Q/",h< ..... """"rtl and r"., 00';"
joy of 00'''1';101''0: dnol'
0(. <011.1>< ...",<
"udy 1""'1' ,n ,..,..... f.1'i"p5Ia 11, 66)·80. 1980.
W"""C 11.8<1'; V.G><, P$,.,.," OUIOl)fl"l<'l Gf
,.... ..."'1 .._,...., ... iLh "".. p,I<po;,,,,,,,,,I\,,,'
r«oocol II, I»-J. 199-'
K' noo J II: U.. 0( 1)0,,<0</;_1"'" d"'., p"'ln'.·
<y. lobo<. _I..,...;"". ',",Ill 1'>""'"'" ",I'rr«< ,0
pII><m><oI;, ..
D<vp lJ: lSO·IQ ,
11."'_
,L< _,........
,m
S _ " M: r:p,kp>y L< """",n 0( .h,IOI"",,,.,
. : 11 ...,itton •• I,."" ..""", bt . _ •• sc .".
t>am><'p'n<. 8, M.d J 199: S81. 1989.
N.i".,oI ln,uM•• oI!l,.hh C_nlO. 0."'''1'"
.... , Conl.retI«: Su,1C'l' lor .,0101", . J I\MA 260:
129·)).1990.
8orwYI<I<A I. Rowl., H A,I\_""", F' MR in
,..",oJ.",kl"l" V.""of ~"';.", ""', .....
rio: L«~.iqu<' . A./NR 16: 139-4l. I99S.
O&/i./ey I. OJ<LnI •• C A, 0 _... l M, "MI. /drn.
oly,", .";Iopt;'; f""i on :ooon .. _
CI\T
o< •••• l\rd N... ,.06:669·1I . 1~79 .
H..... y AS.H'pl.i .. 'I . Bow< I M. .. MI. F""",I
lob< 'p,lq»),: O,ni .. , .. i.u<echOiX' ..... "".ocI
"'illl "".1 \99mfl"o·HMPI\O SPECT
",.. t%c.J. 1%(,·10 !993.
w..;. I. ~ ........... T'. In"..,,..,,, loJO"'1coo 01
""JU! for"" I... "!i"~",, of .... ~.p«<h 00 .. •
in_•. J N.~, ... " 11: J66·81. 1960
Qtoc< ..... 1 v.c.m..no l 101: IId.""",'.,f>< ........
.u'II<.1..... J<"I<l" 01 _I, <IIikP'Y, Con! ... p
N.u ......... ,~(l6) : 1-6.1991•
Coh<. 0 S. Zulooy C P. Good ..... R R' Soi..,,_·
I<,oonc<<<>"'j fox •• """""" ma'f""",,·
'''''''. J N........"83: 2l1 ..02. 19'15 .
_ R . V.h !l·S.I'I, .... IO"" 0,,,01,:
"""Y ..,,'" .k<'rophy. ,o"'ll<o1ly I UiOod ...... .,.
I", .. """"., lob< ,,,""" ... nil... ,"1 ",i,,, c"'"pk.
N....... '1i13: lll-6. 1m.
Mcrn:1I F.
W W. 6 1«k T P: M.I'iplo,""
pi.1 """...,i",,· 1\ .... ~ 10 ,he ..",<01
off.nl <pile ... ,. J "'...... '1i 70. lJI·~.
1919,
(l .... J R."'pp,~ I E. hpl. "at .. eo.-p •••• Il00010"'1: Cli";';.1o<Ld .Ic<'rn<n«pI>oIoJrl.p/Ii< .fI.....
~piI<,... .I~, 3(l8.16.linI .
M .n",,~ . R"uzo PC In tpil<pty and ,be ......
PI<' .&lIOIum. ~ .."'. 1\ C.'«I.f. Pie •• ", ,.,. ...
Now Vmt. 19S5: pp 181..J()1
80$•• I E•.'kh.l" D H..... oi., P I: Ccmpl ..... Hof
al""""'my ......·• by MRI ""fLo 1ao, ,,,,,, . l\rdL
N........ 5: 11Ol.$. 198t.
0;."'""" C A: ' n SUrp-., ' .... 'm ... ' oI"b< <pI1,,,.
..... F"I<I 1 .'«I.) . R.I'~" p,. ... Ne ... V", ~ . 1981.
..
10l.
,
lOS.
1<>:.';"';,0
,~
'"
,~
"""" .n.,
,~.
11(1,
1..0:.-..
"",,,,,,,,'."'.J
WM",,,
,<UO""'.,
III .
II~,
'"
'"
pp6J5,q .
liS . 0;."'""" C A: S." ... I ""'''py I", mod""" y ",.
..... 111< ''';101''1. J 1'1.."""" 66: .89-911. 1917
116. Ni<nl<y<f p.
wlric.I., ."'Jrd«iQ.hOp.
po<Q"P«'_l iw I<" 'p<;roi _
.pil<!'". I. T.....
por.1obe
8...,.... ILl o<Ld 80iky p.
IM.f. a..,,,,, C Thom», Sprin.r"kl. 19$8, PI'
461·12.
C,andaU P H: C"'......,,,""',,.,..,. I. S. ...... ,
" ..""..., of 110. <pliO,,*,. F.n1'1J. (<<I.). R.... n
Pfe>o. N.... Vort. . 1981. PI' 377-4(>1.
7Jo.,,.,....
qijo,.,.
'"
NEUROSURGERY
14.1.
Low back pain and radiculopathy
TKey points'
law block pain is comm"". and in _ SSilomc:ues, no 'pe<:ific dillgIlOllil can be tnIIde
,niti.I ....nmenl iag•• red \.I) de~tinM"red fl.~~ (indiCliting pnl.entially aeri(>u5
paU\oloi)'l. and in the abHl'K'e oflheM!.lmaging ""diu and further tellin g of pa·
li'nll; i, u..... Ul' not helpful dllrinr lhe f'"'t 4 W"U of low batk .ym ptom.
relieJofdiKorur"rt un be bqlacllieved wilh nonpre&Uiption pain meds and/or
'pinal manipulauOl\
while K tivi tieol .... ay n«d lO he modified, bo!d rel t br.yond 4 de.yl may be more
hlnnful than helpful. and patients .,,*enco\lr8~ \.I) r8\\Ull t(lwork or their nOrmal da ily aclivit.n a • ....m .. ponibl ..
89-~ ofplltientl with low block problems will impl"O'o'iII withi" I month even
without tr.. c.m.nt
wilh Or wilhoutlurgt''Y. ~ ofpe t ief)ta with .cia ti"" ""enLually rem"cr
Low back paIn (LOP) !sexlnmel, preyalent.1U>d ;,lhe_ond mourommon rftSOn
for people to seek medic,,1 att,elltioo' , LaP aa:ounts for . J M~ofaU lick lea ... from work,
and q the ......tcomrnon QUleDf disability fOl' peI'Ons <"45 )'TIl sge". EU.imatu ortifel ime
p~lencenn(l! from EO·~ •• nd the .nn ....1 ;ncid~nce" 5"'" Only l ~ ofpllti~n u will
have nerve·rooI.8ymptoms.~d only J -3'.fJhllvf Lumbar diac: hemiaLion. The progl>OIIis for
n'><llt ~ DfLBP i. load . a nd improvement "s"a Uy IIttUn with Little or no medical in·
lervenlkm.
•
D EFlNITIONs/CLASSIFlCATlONS
,~ rtysbn:lCon rA'!IfI.-.e roaI [~ItId~may iIIc:t.Ior:pM'Il'iiieiii....
l/'itUOIIrA ....1
_
roo:, dem>iI!IwnaI sensory disIurtancH. ~ rA IIIUiSdn n-o.rv.lfo) 171'
Il8MI roo., and ~ III\JSIX ~1dI reII!.- 01 lie umalll.lKlesl
~1
N<A "!Io.I!CIlIoW!",$bae\ ~ (boll ~ 1em'IS) iht
0II!!Wiif.niliiTIDi low
loW ~ ~ bid pa!II. May rftlM IrtJffI $II.., rA !hi . ,. . . ~
igImenIs. ~ ot
!~ joonIi .•• E.td\.des ~~ ~ C&IIi8S te.g. bID. d!l: 1lefTU!1OII... )
""*''"'*
"'I
NoMENCUtTURE FOR DISC PATHOLOGY
Ki.torically. the to>:rminolac h.. been conl.erlt.io". and n"".Ulndardised . Many diagnOllt ic Jabel. a re II.ed inoollli.len\.ly le.l . IpondyLo.i • • • pr.;r.. ' t rain . mUICU)OIkeltW
p.tIl/l. ,"YeNaKial pain .. •). A l ubM:t ofnomenelature proPQlld by a task {orca" i. alIown in
Tobl. 14·1. which il IIHful pri ma rily fDt oonai&lent "'-rrninolOO related to radiocn>phl<:
reports. re.."" h ..
Oejtc ocr al.ed dllle: ..me repDfU indiQle thaI Ih_ ca .. QUM radk\dar "" in poi.iblj by." in!htmmatoty mec:hMi~m·. bill th" ill oot. univ. naLly ~pled.
Du lg:iDg d' ae: taay 01' may not be I ymptom.tic.
Vacuum di e<: ' imarina lind>np orCas In t he d;te 'pKe, \&aulLly i l\Clical,~a nf d llc
deceneulion.
Non-St llDdllrn terme
TI, elM! i<!1"IJ1!" art! inel"dat for QllnpLet.en«4 but are WIJ. rKOOlmended becauie th~
may be co nru .ina or inllccunt.e'
Co ntaIned h e mhtti n n~: dilplaced disc tiuue en l;"'11 I:OnUlined ...,thin an "nin·
tel"T\lpt.;!d ( bu~ po4Iiibly d iotended ) .nul .... or atp"ule (lin' ~301 fo r d.!:finil.lon rump-
Nf.'UROSURGERY
'U/f'). Ilmay be difficu lt t.o distin(Uish thi. on currenuy av.ilabl e imaging . Iudies from
an unconll ined he rn iation wllieh i. undern",alh Ihe pO$lerior longitudinal lig.menl.
Ruptured di..,: coJloquiallerm uaua lly in tended to be equivalent to herniated dille.
Table 14-1
"""'"
Reco mm en ded classifies-
tion
Table 14-2 AHCPR classification
It i, I'fl<'(Immended' that
acule bock problem. be cl sssir~d into OIIe of lhe 3 eatcgon C/i
shown in Tablf' U ·2b!1.ed on the
~ and phui<;al euOl (tee
1";liaJ I,. ..... nunl o{lM palif'nt
wdll bocApain below),
Further evaluation, lrealment, and eveo 1I000e inform a,
tion !'Igarding prognosis esn bo
bated on Ihi •• im pla elull li""
tlon . A m-.ioT 1!NI1 is to delcet -red nap' that may ind icate potantially sen ousspinal Or
nonspinal pathology (1ft P"'8f' 292),
....'''' ..
,
Table 14-J Modic', ciasslUcatlon
NoMENCUoTURE FOR SPINE PATHOI.00 Y OUTSIDE THE DISC
Ve .-u.brai body ma.....,w c hanles:
""-iated with depnentivcor
in na mm"ory changes. Modic'.
c:l aMi fic:a tion' orMRl characteristic.
ilshown in T"bI., l4.J.
lnCeMIty ch.....
~
I
n ..
I
I
2
I
*,Of ,
3
I
I
OeKrip~on
--
DOnt marrow edeflll 8&SOciIled vriIh IMe Of ~
..,...intJa~
'4 , Sp,na and aponar cord
It ...
bent mlrl'l1W by III
fIIt'tNt OSI~
NEUROSURGER Y
DIFFERENnA L DIAGNOSI S
The differential diagnosis arlaw back pain (so,oe Low bee. {XI;", page 907) overlaps
wit h that af myelapalhy . 10 . 85% of ~ases of l.BP no sp""ific diagnru;is Clln be mad"-,
INmAL AS5 E5 SMEtfl' OF THE PATIENT WITH BACK PAIN
Initial assessmeot:onsists ofa history and physical exam focused an identifyingserious underlying renditions such as: fracture, lumnr, in{eelian or cauda equina 8yn.
drome. Seriaull condiliotlS presenting a8 1nw back problems are relatively rare.
HISTORY
The fnllnwing jnfnnnation has been rQund to be helpful in identifying patients with
serious ullderlyingcam!itiaos such 118 cancer and spinal infection'. Tobie 14·4 shows the
sensi t ivity alld specif,ci ty.
I. age
2. history Gf callCer (especially ma lig· Table 14-4
,I
na""ies that are prooe to skeletsl
metas(aSe9: pr()litate, breast, kidlIey, thyroid. hl1lgl
il
3. W'lexplained weight loss
4. immullosuppre.sion: from steroids, organ transplant medica·
lion , orHrv
5, prolanged use af steroids
6. duratiall of symptgms
7. responsiveness to previau s thers ·
,
8.
9.
"
at
"histarythatohk..in infection:
especially
pai n
is wone
"'$1
furuncle
10. history ofrv drug abuse
II. UTI arother infectian
12. pain radiating OOlgw the knee
13. persistent numbness or "'eaweS!;
in the legs
14 . history of significant trauma. In a
young patient: M"VA, a fall from a
height. or a direct blow tothe back.
In an older patient: millOr falls.
heavy lifting or even severe cough.
ing can cause a fracture especially
in the presellCf! ar GS\.e(lporosi s
15. findin~ C(ln. is Umt witb cauda
equina syndrome (see page 305):
A. bladder dysfunctinn (usually
urinary retentinn , or ave rnow inoonlinen.:e)o r fecal in ·
con t inence
B. saddl e anesthe9ia: _ pagt
'"
C. unilateral or bilateral leg
,
estilna'e
weakness or pain
16. psycholGgical and socioeconomic factars may lnnuence the patient's report af
symptoms (also see {XIgt 296), and one should inquire aoout:
A. work. sta tus
B, typiealjob tasks
C. educaliana llevel
D. pending Li~igat ion
1::. worker's compensatian Or disability issues
F. failed previou s treatments
G. s ubstance abuse
Ii . depression
NE:URQSURGERY
14 . Spine and spinal cord
'"
PHYSICAL EXAMINATION
I.~&a helpful tha.n the history i.n identifyillg patients who may be harboring mndi·
tiona such as c'''lcer. but may be more helpful in detecti.ng spinoli.nfections.
I . spinal infection ($fe ~ 240): finding!! that suggest thi a as a possibility (but are
also common in patients without infection)
A. fever: common in epidural abiICe8/! and vertebral osteoml'elitis.lesscommon
in di.~dti5
B. vertebral tenderness
C. very limited range of a pinal motion
2. findings of jXl6Sible oeurologic compromise: the following physical findings will
identify most ca~es ofdinically significant nerve root compromise due to U -5 Or
L5-51 HLD which comprise:> 9O%ofcases ofradicu)opathy due to HLO (limiting
the exam to the following might not detect the much le811 common upper lumbar
dis<: herniations, which TUay be difficult to detect on PE.1tt P'l8" 310)
A. dorsiflexion atren~h of ankle aod great toe: weakness luggests L5 and
some U dysfunction
B. achilles refle~ : d iminished reflu suggests 51 root dysfIJ nction
C. light touch sensation of the foot:
\. diminished ove r medial malleolus and medial fOOl: suggests lA
2. diminished over dorsum of foot: suggesta L5
3. dimini.hed over lateral malleolus and lateral foot: suggest.'l SI
D. straight leg raising (S LR) {also check for crossed 5LRI: Itt fHlIJe 302
"REO FlAGS" IN THE HISTORY AND PHYSICAL EXAM FOR LOW 8 AO< PR08LEMS
Based upon the above history and
physical uam . the findings ia Tobl~ 14·5
would suggest the pos.sibility of s seriOU9
underlying condi t ion as the cause of the low
back problem_
with
FURTHER EVALUATION
For over 95% of patients with acute
low back problems. no further testing wilh·
in the first 4 weeks of symptoms is
required '.
In the absence of any of:he "red flag"
conditions shown in Table 14·5. no further
testing is r«ommended (even for patients
s uspected. of having a HLO) and the treat!Dent is similar for most patients with an
acute episode of low back problems.
Si mple laboratory tests including CSC
and E5R are sufficiently efficaciou s and in·
expensive that they should be obtained
when there isa suspicion of hack relsted tumor Dr infection .
FURTHER EVALU ATION OF PATIENTS WITH LOW BACK PRODLEMS
EKcept for those e><hihiting "red flags" l$fe 000.... ). special diagnostic tests are usu·
slly not needed during the fi rst month of l ymptomB !in~ it is not ptI8lIib!e to predict
which patients will improve las most do) and which will not.
TESTS FOR EVIDENCe OF PHYSIOLOGIC DYSFUNCTION
EMG for lo w bac k proble ma: IfthediagnOl!is ofradicuJopathy seems likely on clinical
grouod s. electrophyaiologic te$ting i8 not r«ommended'. However. these te9ta may be
useful for patients with suspicion ofQlher condi t ions (e.g , neuropat~ y . myopathy. myel.
opathy ... l Or wh en the diagnOlSia of radiculopathy is uncertain (e,g. a HLO on MRI is not
always symptomatid. 'I'esting is highly operator dependent for a'X'u,""cy.
1. needle EMG : can assess acute and chronic nerve root dysfunction. myelopathy
a nd myopathy. Not ind icsted and also Wlrel iab!e when symptoms pre38nt < 34
14. Spine and spinsl coni
Nlf.UROSURGI:.'/lY
WHU. Over.1I accuracy imprQvn w,th knowledge abou t imagin, studies and
clinical intbrmalion'. ,",CCUnlcy in predict;n,]f"!] of involve men I" is _ 84<.10
H-ran ....: me .. u.... HIISOry conduction through nerve I'(l(lUi. U,ed 1II001ly 1.0 u _
_
51 nldlcu iop.lllhy"
3. SEPI. u ..uas .. ntory neU/'ll1\$ in pl'rip~ ...l nel"'U and spinal c:ord. May be .....
ftll in ... aJuptiIlll81.11pe<:te .pinal.tenosi. or .pinal myelopathy
<t. rM!1'Y1 conduction ~t udiu (includill/l NeVa): hell» identify acute and c:hronic tn_
trapmeM neuroplllhiu th'l may mimic radiculop"lhy
6. II ROt reCllmmend<)d fOT uae"' n, A<:UU! low bIIek probl~.'
A. P·wav. relpofl.le: me.Illrel mot.or conduction through nervi roou., u.sed to
~.
...eM proKinUl1 ~W"(lpathiu
8 . ,,,note EMO: " uefiHl,CUU! and chronic reo:",ltment pIIuenad"ringltac.Ie or dynamic task, using ... Tface {i1\lJtt!ad ofnHclla} I!leetrOdea
Bon e ".,. n (or low bAc k proble m a' De.uiption: injection ofradinlabeled oompnunda
(usually technetium-99m) thDt aN uken up by metabolieaJly act ive bon@. A gamma cam _
enl i. then uaed w l(I(:el," region' nfuptllb, Th, tnta! radietinn dGH;' equi"elentto a
aet oflumbDr apin.(! lr-nya' . Contnlindicat<':d during prepancy, and b~nt reedifli mUll
be sUlpended for /I brief interval fnllow;ng ~ bone Ic:aon due to po-eII!lICI! of udiotrater ;1I
the breast milk.
A mGd~ra tely leuit;v, ~t whi(h may he u~ in ...."Iuatlng low be<:k JMlin when
spina l tum or ", infection", or IH:CUIt fr*,!ura;' 'u'J*~ fTOm"r«t nags' 1_ Tobie 14·
5) 011 history oreKDmilla tion . or ruulUi ofJ.b usta or plain .·nlYI, Not....,.., lpecir,e, but
may locat<': occult IH;onl alld help diffu. ntiate thea.. conditioru frQIn def:f!neUl.lve
chllnge" A p<»itive bone IlCan I UggolSting one of theM oondi t lona u5ually mult be confirmed by ot her dil'(tlostie t.e$/4; or procedure. (no Mudi.,. h,vfI eomp.rtd bone tcalUI to
CTII' MRI ).
Low )"leld in patienu with lonpt.anding low beck problema and normal plain . -ray.
and labocatllry I.elIta lespecla lly £SRI".
Thermograpby for 10.... back proble ... ., N!)t r<!COIIIm.nded' . Did not aa;uulely predict absO!nce Or presenceofnerv. root wmp",..ion seen at su rgery", and may be pOIIitive
;n !lsignilicent percentage of 8S)'mptomlltic I>It;ents".
RADIOGRAPHIC EVA LUATION
Diagn()l;ing lumb, apinPl ~tenO/iis or t..miated inurverub.-al dise;' ... ually helpful only in pOl.ential,urrieal o:andidaU$'·. Thi& inc:ludes ~ti~o~ with appropriale. dinj·
cel.yudroroe5 who have not respOnded satisfactorily to adequall non-au.rrieal treatment
over a iufficient pe riod of time. end who have no medical CIHItnlindic:aobon. to IUrger)'.
RIIdiologk confirmation of these diagnoaa uluaUy requi res CT, myelography. MRl. or
$Orne <:Ombination (... bdow l. N8: mye lograpl\y", CT". or MRI" may also show bulginll
or herniated lumbar Wid (HLDl or spinal stenoai, in asymptgmati, patif:f\~ (e.g. 2"'1>
of asymptomatic pati",nta bav" hern;8ted diSCI! on MRland
have ,pinal 5uDO:!li.;
thelM! numbe .... become E6'l1and 21~ ..... pl!Ctivel}' in patienta 60-80 yun old,... Thus,
tMtt- IUt . mull be inr..."reted In lilht ofebnieal findinp. and the anatorok level and
lide shGUld comispOnd to the hIStory . examination, andlor othu pbysiologic data. Diag·
rKNIt;e radioiocy is of limited benriit l1li 1M initial flValu5lion in the majority of spinal
dilOmen" .
In lhe abte(lCe ofud nap fO/' seriou, condllluu, im.ginl.$hJdie$ sr. rIOt recoinmen,u.d in tbe lint month oflymptoma' For patieo,- ... ho have ~ preyioln bad surgery , MRI with c:ontl"ll&l is probably!be besl tat. Myelography (with "' without CT) i.
in~asi~. lUld haslncrealoKl risk of compliatioru, and i. ther..LOre ind icated only in !lilu.tio.... where MNl cannot be donee or il inadequatt. and I Urpry II anticip.a~ .
4'
•
NEUROSURGERY
14. Spine and spinal corti
PlAIN WMBO.SACRAL X-RA YS
UnOl!xpeoted findina:S(H:t ur-red in only I in 2500 IIdultt < l\O yea ... ,,"", DilfTlOti. of
l urgiuol conditions ofdisc herniation aod apinal stenosis cannot be made from plain
f, lma. Va rioul cOR£ilnitalabnormalitiea of uncertain silr"ific,nce rn a, be Identifi ed (a .l _
'pi na hiM. occ1,l)ta). a nd evidence of dea;eneraUve chanle. (including oeteophyt.esJ are
a. frequent in sy mptomatic a. in asymptomatic patients. Gonadal r.diation il , ign;fi·
canL Seldom indict. U!d durinr prtlr'lsncy.
Recorumeoda tio n
Not. recommended for rouline avaluatioo ofJn.tieou with acute low back problem.
during the fI ... t monUi oraymj)tomt unleM II "red nag" i, pree.ent(Itt' kll)W). ~rve LS
x-rays for plltienta with II Ilkehllood orbavillll' apioal malignancy, infection, innamm_tory 'pondylit;', orcl ini",Uy significant frllCture . ln the" calel, plain x-ray. are o1l.enjust
II .tartiJlt point, a nd further study (CT, MRl ,.,) ruay be indicated e ven if the plain x·rlly.
I n normal. "Red nags" for thBe conditiolll includ .. the following:
I . ~:>70yea ...,or <20y ...
2 •. Iy.wruically ill patienta
3. wmp:> 10000F (or :> 38' C )
4. hii toryofmaJignlncy
.5. reoent infectioo
6. patienta with neurologic def,cita IUResting possible cauda equinasyndrome
( ... eldl .. a nesthesia, urioary iocootioelKe or ~ntion, LE wewess, 6« paNe 30$)
7. I\Hvy alcohol or rv drug a bulen
8. diabet ;'"
9. inunllJ"lo.upp'lIIIIIed patientll( ilKluding prolongd lteat.rnent with corticoste.oids)
10. reoent urinary tract or Ipi nal l urgery
11 . ~1I1 traUIllll : any ...e with significant trauma. 0':>.50 yrs old with mild t.aurua
12. unrek!oling pa in at ~
13. persisteot pain for more than - 4 weelul
U. unexplained weight 10M
.....'hen s pine x-rays a re ind icated, AP and lalellll views are usuaOy adequa~. Obl;qua and coned-down L5-$1 .iews more than double the rsdilltion eKpoIIure. and add
infon.... t:on in only 4-h of c.llses", a nd can be obtained in specific int tancu where WaT'
ranted (<!-!C". to diagnor;e spondylolysis when lpondylolisthesis ill found on the lateral
film).
MRI
MRl hill! supplanted cr and myelography for diagnosing moetdiac herniations and
also in most cases of apinalatenoai • . n.e test of choice for patienta who have had previoul
badliUrpry. Specificity and ~.iti";ty ror HLO are on the allme order ... CTlruyelOjlTa·
phy, which is better than myelography alone,· .. • .
Advaotages:
I. provides inf(N"mation in ..gittal plane lea n easily eva luate ca uda equina)
2. provides information re,an:iing tissue o utaide ofth•• pinal ca"al (e.g. extreme
late..al disc herniation (Me paiJf 311), turno ...... )
3. non·invasive alld does not in""lve ionizing ."diation
Dildyan la,.*,
I. plltienu io.evue pIIin or with claustrophobia may have difficul~ holding It,ll
'2. d .... not vi.ualiu bone w~1I
3. poor for etudying blood early (e.g . • pm..lepidu,al hematoma)
4 . eJ:J)@IlI'ye(nOl.l:maybemoreCOlte ffl!divethanmyelographyi f pon·myelogram
overnipt hospitatiution i. avoided. and especially if a rln complic. tion from
myelographyoccun)
5. difficult to inlt'llre t in ct._ ofltQliosi • . Myel~ may be luperior
6. a numberofcontraindi:atiooa: 1M COII lraiiVlieoliOlll to MRI, ~ge 135
Findiogs:
In addition todemonltnti", herniated lumber dise 1l{lJ)) outaidaofth, dill<' inta.·
Bplleeeompruaing ne ..... root Or thecal J.K. MR.l can demoo'U"IIte .ignal ch'''geI within
Ibe inte ...pace Iuggeetlve ofd.ilul.tftllm!.ilw" (Iou of.lgnal intenlity on 1'2WI, lou of
dille , pace he ight).
LUMBOSACRAL CT
Not co",idered i tate ofth. art.lrtac:hnical1y adequate ,marescan beobtained {e.g.
'"
14 . Spi". and .pina l cord
NEUROSURGERY
good quality scanner, images not ob$cured by artifact from patient moveloent Or obesity),
CT can demonstrate most spine pathology. For HU l, sensitivity is 8O·95%,!lJld specific·
ity is 68·88%"· '". Howe_er. even some large disc herniations will be missed with plain
CT. CT studies for HLD tend to be less satisfactory in the elderly. More utility ... ith frac·
tures.
Disc maUlrial haa density (Hounslield UJ1iu) ~ twice thatorthe thecal eac. AS!IOCiated findings with hern.iaUld disc include:
I. loss of epidural fat (normally seen as low density in the snterolateral canal)
2. 10$5 ofnonoal "convexity" of thecal $ac (indentation by herni;lted disc)
Advantages:
l. images 80ft tissu~ to a d<.'gl"(!e th$t may bI! adequate
2. excellent bony detail
3. non·invasive
4. outpatient evaluation
5. evalustes for extreme lateral disc herniation to SOme degree
6. evaluates paraspinal soft tiuue (e.g. to rule out tumor, paraspinal abscess .. )
7. advantages over M"RI: fasterscanning(significant in patienu who have difficulty
laying still for loog time), less expensive, less claustrophobic, fewer contrllindica·
tions (see Contra;ndiallion$ U) /WRl, page 135)
Dissdvant.ages:
1. does not evaluate &agittal plane (may be partially ameliorllted by eliminating
skip regions and then utilizing computerized sagittal reconstruction.)
2. ev. luates only those levels thals", .scanned:
A. higher cuts must be taken through the COnUS medulla ris to avoid missing
occasionsl pathology there
B. performing cuu only through the disc spaces (a COmmOn practice) may miss
pathology t.etween tbe disc $pa(e$
.s. sensitivity is sigqilicantly lower than MRI or myelogramJGT
MYELOGRAPHY
With water soluble contrast, sensitivity (62·100'Jt,) and specificity (83·94%>-" are
similsr toCT for detection ofHLD. When combined with polIt-myelographic CT ~can (my.
elogrsmJCT), the sensitivity and ""peelally specificity increase>'. A herniated disk in the
large spate between thecal $BC and posterior border of vertebral bodi"" at U·SI (insen·
s itive apace) may DOt be seen on myelography (CT Or MRI are usually better at detectingthis).
Advantages:
I. provides information;o sagittal plaoe (unlike plain CT)
2 evaluaUls cauda equina (unlike routine CT)
3. provides "functiooaJ " ioformation about degree ofswnosis (a high-degree block
will allow now of dye only aller certain position changes)
Disadvant.ages:
I , occuionally requires overnight hospitaliution
2. may mies pathology outside of the dura (including far laterally herniated disc).
~n$i~ivity i$ improved with pOSt·myelogr"phi~ (,'T
3. lIlVaslVe
A. dru!1:S e_f(. wanarin must be stopped, and sometin:.es converted to heparin
B. with occasional side effects (pOSt LP HlA, NN, raN! seituru)
4 . iodine allergic patients
A. requires iodine allergy prep
B. may still be risky (especially in severely iodine allergic patients)
Findings:
HLD produces extradurallilling defect at the level of the inUJrvertebral disc_ Mas·
sive disc herniation or severe lumba r stenosis may produce a total or near tot.al block. In
some c8Ses ofHLD, the finding may be very subtle and may consist ofa cut-<:>ff of the fill.
ing (with controst) of the nerve root sleeve (compared to nOrma I nerve(s) on contralaUJrIIl
side or st other levels). Another subtle finding may be a ' dual shadow· on lateral view.
BONE SCAN
Seepage 293
NEUROSURGERY
14. Spine and spinal cord
'"
DISCOGRAPHY
Injection of water· soluble contrallt agent directly into the nucleus pulposua of the in·
tervertebral disc being atudied. Re~ults of the test depend on volume of dye accepted into
the disc. tile pressure needed to iQject.the dye. tile configuration of the dye (i ncluding
leakage from tile confines of t he disc space) on radiographic imaging (plain x·rays produce the so·called "discOf(ram" , CT scan may also be utilized), a nd reproduction of the pa·
tient', pain on injection. Someoft he basis for performing a discogTam is to identify levels
that may produce -discogenic pa in" or-painful disc ~yndrome", II CQntro~ersial point (see
PRACTICf; PARAMf;Tf;R 14·5. page 300).
Critique:
Invltsive. Interpretation is equi'·ocal. and complications mayoccur (dillC8pace infection. disc Ilemiation , and significant radiation expo.ure with CT-disCQgr8phy ). May be
ahnonnal in asymptomlllic patients""'· (as any of the above tests may be) IIlthougll tile
false poaitive rllte may not beq uite this Iligh"'. SeePRACTICf; PARAMETf;R 14·9. page
301 for recommendations.
P SYCHOSOCIAL FACTORS
Although SOme patienta with chronic LPB (> 3 montha durlltio n) may h9ve started
offwith a di agn0$8ble condition. PlIychological and socioeconomic factolll (su~h a8 depression. secondary gain ... ) may come to playa lignificant role in perpetua ting Or amplifying
pain. Psychological factolli. especially elevated Ilyateria or hypodiondriasis seal.... on the
Minnesota Mult iphasic Personality Inventory (MMPI) were found to be a better predictor ofouk:ome than finding-s on radiographic imaging in one study'. A .creening lICIlle of
5 factors has been proposed'" (positive findings in any 3 suggests psyehological distress):
I . pain on simulated axiltllOllding: press on top of head
2. inconsistent performance: e.g. difficulty tole rating $traight leg ra ising (SLR)
while supine, hut no diffi culty when silting
3. ove~action during th e physical exam
4. inappropriate tenderness tbat is superficial Or widespread
these two items may not be rf!liable.
5. motor o.r sensory abnormaliti"" not
the others an potentially reliable'"
co~sponding 1.0 anatomic confines
However. the usefulness o.fthis info.nnation is limited. and no effective interven·
tions have been identified \.0 address tllese factors, Therefore the AHC PR panel was un·
able to recommend specific as:senment tool . or intervention.' .
I
T REATMENT
An initial period of nonsurgical management ("conservative" treatment. /IU b<!lowl
is indicated except in tile followingd rcumst.smes where urgent surgery is indicated:
symptolT\l ofa cauda equina syndrome (urinary retention. saddle anesthesia .... see Cauda equino, S)'ndn:m... page 305). progre5Sive neurologic deficit. or profound motor weak·
ness . A relative indication for proceeding to urgery witllout conservative management
is seve'" pain that (/Ul not be . ufficiently eontrolled with adequate pain medication
(ra",).
If specific diagnoses such as Ilemiated intervertebral lumbor disc Or symptomalic
lumbar ~ ten05 i e are made. euo'gical tfeMme"t fOj' theoe- conditione Play boo considered if
the potient fails to improve satisfactorily. In cases wllere no specific diagnosis can be
made. managementconsisUi o.f conservative treatment and following the patient to rule
out tile possible develo.pment of symptoms suggestive o.f a mol"(! serious diagnosis that
may not have in itially been evidenL
"CONSERVA TlVE~ TREATMENT
This term has regrett.ably come to be u.sed for non·surgical management. With
slightmodilication. simila r spproaches can be used for mechanicsllo ... back pain. as well
as for acute radiculepathy from disc herniation .
Recommendations (based on AHCPR findings' in the sheen"", of "red Oag-s-A):
II . OOm. kty liten"u", <iUl io .... tt it .." h.",. prim.rily lhooo rrom Ih.
. heAnn<y forll •• llh C. ... Pol .<), and Re...... h lAHCPRI po...,1
r.r to 8i"", .. aI. ' for MI an.Jj'I;' and li.t ~ref.~n <H
".
14. SpiJle and spinal CQrd
bt",,, , tu<!i.. lho• • uppan
~m",.nd •• iona.
H.,.....or. re-
NEUROSURG~'RY
1. activity modirkationa; nn studies were found thal met the panels review criteria
for adequate evidence. However. tbe foUowing information WaS felt to be useful ;
A. bed rest;
1. the theoretkal objective is to reduce symptoms by reducing pressure
on the nerve roots and/or intradiscal pressu1"l!$ which is lowest in the
s upine seOli·Fowler position" , and also 10 reduce movements which
are e,,~ienced 88 painful by the patient
2. deactivation from prolonged bed rest (> 4 days) appe8.1""8 to be worse ror
patien,", (producing weakneS8, stiffness, and increased pain ) than a
gradusl return to O(lnnalactivities"
3. recororoenda tio",,: the majority of patients with low back problems
will [lot require bed rest. Bed reat ror 2-4 days may be an option ror
thOSl' with severe initial rodU;warsymptoms, however, this may be nO
bett.,.. than watchful ....·aiti ng<' and may be hannful"
B. adivity modification
1. the goal is to ath.ieve a tolerable level of diM:Omfort while continu ing
sufficient physical adivity to minimi~ disruption of daily activities
2. risk factors: although there is rtOt agTffmenton their uact role. the
following were identified as having an increLsed incidence oflow back
problems. Jobt requiring heavy or repetitive lifting, l<ltal body v;bra.
tinn (from vehides or industrial machinery), asymmetric postures, Or
JX>Stures sustained for long periods (jndudiog prolonged si tting)
3. n!<XI':IIMndationa; temporarily limit beavy lifting, prolonged sitting,
and bending or twisting of the back. E6tabli~h activity goals to h.. lp focus lItU!ntion Oll expected return to full rumtiona1 status
C. exercise (may be part of (I pb ysical therapy program),
1. during the 1st month of Sympl<lU18, low-stress aerobic eJ<erdlle can
minimize debility due to ina~tivity. In the rorsl2 weeks, utilize exer·
cises thal minimally stress the back: walking, bicycling, or .wimming
2. condjtioning ""ercises fOT trunk muscles (especially back extensors,
and po88ibly abdominal muscles ) are helpful irsymptoms persist (during the first 2 weeki<, these exercises may aggravate symptoms)
3. the,"", is no evidence to support s!retcbing of ba~k muscles, Or to rec·
ommend back·specific exercise machines over traditional exe....,;se
4. recommended e~ercise quotas thal are gradually e5(:8lat.ed resulta in
betU!r outcome than having patients simply stop when ptlin QCeur!"
2. analgesiea;
A. for the initial short-term perin<!. a~taminophen lAPAP) or NSAJDs (ft"e
page 28) may be used
stronger analgesiC!! (mnsUyopioids , see page 30) may be requi~ for """ere
pain , usuBlly severe radicular pain. For non-specific back pain. there was
nOearlier ~etum to rulL activity th8ll with NSAJDs or APAP'. Opioids
.hould not be used,. 2·3 weeks , at whi~h time NSAJDs should be instituU!d
3. muscle reluants (set page 34)
A. muscle spasms have not been proven to cause pain, and the most commonly
used musde retaxants have no peripheral effect en muscle spasm
B. probably more effective tban placebo, but heve not been shown 1<1 be more
effective than NSAJDs
C. potential ror side effeeLl: drowsiness (in UP to 30%). Moat manufacture ...
r«(lmmend U$e ror < 2-3 weeks. Agents su~h as ~hlorzoxazone Warafon
For1.e® and oth era) may be associated with risk or~erious and potentially
fatal hepatotoxicitY"
4. educAtinn; (may be provided aa part ofa pbysical therapy program)
A. explana tion of the condition to lhe patient" in understandable terms, and
positive rea 88 ur8nCE! that the condition will almost certainly subside" have
been show.., to be more effective than many other rnrms of treatment
B. proper posture. sleeping positions. lifting teehniqe>e •... should be conveyed
to the patient. Formal "back school " seems 1<1 be marginally effective"
5. spinal manipulation therapy (SMT); defined as manual therapy ill which loads
are applied to the .pine using long Or short lever methods with the sel«tedjoint
beillgtaken 1<1 its end range of voluntary motion, rntlowed by applica~ion of an im·
pulse loading (may be part or a pbnica l lberaQY progrnm )
A. may be helpful ror patients with Reule low haek problems wilhout radieulopathy when used in the firat month ofsympl<lrns (efficatY al"l.er 1 month i.
unproven ) for a period not to extee<l 1 month
a.
NEUROSURGERY
14. Spine and .pinal cord
8 . illluffidfn~ .... i.t.ne« to Il'IlOmmend 8 MT in th., p~flCt! oInodi~u\(lp'lh)'
C 8MT .hould not be u:M!d in 1111. face ofuvere or progresSM! neuroLogiedef;CII until "!.iou. CQllditionl hllve b<!en , uled Ilut
D. • reporta or.~rilll d,ulI'Clion {"lfI'lt;~ Il)' veneb",1 arl.fcry) (let pagt 883)
and e VA. myeloplthy" 5ubd"ral hematoma wit h cervical 8MT lind cauda
.quina l}'TIdrome wltll lumlmr S MT"'"" a nd t he uncertainty ofbenelita h .....,
led to the que,t ionlng oftl\e ulle ofSM'J'II (npecially eervica1)
6. epidural inJeetiona:
A epiduul lcortlcoJ.teroid iujtctionl (t';SI); there is no evidence thlt Uti. i.ef·
feet iveln treating .eute r.diculop.th,.... ProI~ti". Iwdie. yield ... aried
retul ta" , S<.>me improvement It 3 &. 6 w~ may O«:u r (but no function,1
benen t. lind no chunge In lhe need for ,ulVery). with DO bMeli"t 3
month .... The . e."onlf in chronic bock JIIIin iI poor in COlllpllrison t.o aool.e
PIIio, ESt ro8y ~ In option ror~ reii,fol'rodi<ulor .,.in ... h~ncon ,
Iml on 0.. 1 mtdkltioh, i. ina del'tuale or for patlent. wh. are not lurpe.1
alndidalel
8 . there i. no evidenl:e to . upport the ut, of epidur.1 ,.uec:tignl olltel'll,d.,I.,.
cal IInnt he tk.. and/or gplo.id . for Lap wilhout ..diC\llopoolhy
C. efficacy ... ilh comn lignillueh I . lumbar _pinal
~ tOnnietin,"
_tcnos,. ...
PRAC TICE PA R AMETER 14 1 INJtC"ON
' H ~~AP'
.0" ,OW'PACK PAl"
OplI0n5" : lumba r epidural ifl,ie.:tionl or t n@r point in,j.etionilrelllll.-n·
I!,lend ed for long·tenn relido(chronkL8P. These techniqu.. o. fa~1 il\ject,olUl
may be ,,1\I!d to provid e ItIOJIONII)' relief in sel""t pl tientlo
DiiiftoiUO
DptiDII5 "~
lu",ba r faeel lojecllons
may pndict the respllnf;e to ndiDfrequency facet ablltion
• nm rewmmende:i
ba r (usion
11&
a diagn*tic tool to predJtI the n-s,onte to lum·
~Ql. recommended by lhe AHCPR pan .. I' for trealmenl of aeu\.e low back pl'llblems
In the a~ of"red nap" (."" TaMs 14·5, page 2921:
L medieationl
A. or.1 lte roids: 110 dIfference was found alone Wefl: and 1 year Biter .andom·
iUtiOn to receive I WNk therapy "'lUI oral den.nwthuone or plMebol"
B, wlc:hicln,; <:onflicting evidence. show. el1M. IIOme" or rod" mer.peutic bell'
er;~ Side effect. offill\' and diarrh'"
C /ln l idepre,na lll medications; UlDSt I t ud;H 0(01_ m4!dicatioru; were for
dron;" back pain. S _ meUlodolo(inlly f1a_d studlH fai led to .h",,,, benefit. when compared to placebo for thronit fn~ acute) LBP"
2. ph,..ic.llnaUn~nl.$
A. TENS (u 'Inec:utar.O!OUI eleclncai nerve alimuiation); lll!lo slatiltk:ally aigtill'.
icanlb' belter than plaoebo. and . dded no bene!;t toexercise al~
B. tnoc:tion u ncludinJ' po!lvic t raction): not d.llnonllrated to be I!ffectiv~
C phy.kalarenuand mod.lititt inctuding hut (i ntllldin, diathumy), ice,
ultrasound. Bendt ill ilUlu(ficienlly pl'O"en , however, ..If·otdmuUste....!
home prognlnl for application ofhea~or cold may be COf>Iid~""!. Ulln.
lound and dialhenny Ihould nOl be uled in pl'1!gJlanty
o IUUl b.r COrMt. In~ IUPport belta: nol pI'O'Itn beneflCi/l1 f(or atut.e bIItk pmb·
Ie"",. f>TlIphylldit UM hal been advot't.ed, hut thil l.wn lrovfniwa'
E, biofeedback; hOI not beftliludieci for
hatk problema, Prim.rily ad".,.
fUeci I'or c:hronk LBP, wbere ,ffKlJventSl b mntTOV .....i.Ifo>
3 in,jKl>On ttlenpy
A. InAer poin t and Il,amentous lnjKtionr thO! then')' Ih.t l riUt' points
c:lUH or perpetu.:e LaP bcontrove,..ialand disputed by "'11I}'1!JIp.ertll, [II'
jeetiOl.lI 01 local allHlheue an! of eqwvOC81 emeaty
8 , ranlt jolnl injectiON: theo.-et k.l ba,il i, thai thtl'i! Wit. I "fll<:«1 sy n·
dro m.e " pTOCiUClnC LBP ... hlth i, ",grev,ted by _pine ute!Ui ion, willi no
ne"" root ten ... on _ignI i _ PGII"302~ No I ludi" hive Idequ,tely i.wel ll·
"ted U'\)«'tiooe fOT pain < 3 monr.ha4ur'tiQn. For du'onic LBP, neilher Ih e
.,.,nl nor the locat ion ( intrar~oet or p.erieapllulad m~de , S'IIlif.aonl differ.
~ce in outcomes" ..
C. epi4un l il1,ifttiml in thl!abaenCO! of ... dltulopoothy: _ a~
.all'
'"
L4 ,
Spi ne and ,pilla! cord
,..'EUkOSURGEm'
D.
.ctlpunclu~.
no . t udlu were. f"und thnt evlllUII I~ the. u.. in pcu~ b.ck
problema. )JJ nmdomi'ted clin ical lrla l. fOUM we~ for pat ienu w,th chron·
k LBP, and ewln th' besl /l.tud'uwert! f'lt to be. mediO(:N!.nd con trndictory ,
Indl c. t; onto for , urllcry ror bOlnlhlted Jumbar dbe:
In p~litl/lt.l with c 4·8 w~bd"rllt;on of symptoms:
A tllou wilh "l'I!d nap" thol wMlld II'IIIke.lh~m Mndid.lel flIT urgent tT@al·
IDfn t (e .i . c:IIl.lda equina s )'l1drome. proi"UoIIiwe nel.lroioric IN!flcit.. .. )
B. ;",II;Ii lil), \.0 conltol l'/l.in wllh adequate p.ooin medication (uneommun) mill)'
..qui t e. e. t ller rldiographlc eVllWltlon IOMI'On.llderation for I Urce.ry
InItie.n ta with ~ 4·8 weeu of.ymptoma of sanies that Irl both .."ere and di.
Bblinl: Ind ~rll not ImPTowinli "";th lime, with a I"lIdlogr.phkaU)' identll'il!<labnoromalit.JI thaLc:o.rt!IBtu with lindinp on thl hietOry Il1Id ph),lic.l fun,
I.
2.
PRACTICE PARAMETER 14 2 MRI & Q,<,.COGIIM'I1'
'O~ PA"tt"
S[l re'",,,' 0"
LU"B~A ~USIO'"
Guidelines"":
MRI i. ncoa,mendlld u the mitiel di lgnO&tic te'l
norma\lIppearing dillCe on MRI , hollid not be c(msidltel.l for d~­
ph)' ortrntm»:nt
lumbltr diKOgTaphy should not be ulld es. tland ·a lOQe telt
if dilCOfl'aphy .. ~ : to c_ider • dlec level for l rtatmlnl Ih, ... ahl)Uld
be .. concordant paoln raponsllt A a!illOciatad MR I .bnormalitiHl
Opt ion s"; diKOlP'l,ph.y I hotJld be rese,.."ed for e.quivoo:al NRJ liodinK*."pedally lit Illvel, adjllC1Hlt to I,Int!qUTYOeIIU)' abnormal 1_"
101, _ _ ""
_oI_~._PRA.Cr.cEP~/oAEr£R
""""""a8tII PIIoIn _
.
'*"
IClenlicai O! ..,., ........ ... 1!1I.1IMieN·'
oogIa;>ht""'PI'~_.L8P""_
_I'MIOO$(:~"" "'-R I :~'"
' • . I. jIOIQII2M
_1*11 ~ INS
_
.......... """'~
r2'WI""""'intet>MY. _ _ ~._CNIn\JM..
_~.......,.ItaeIlr'odlrQl_"~oo::ur.,~~
I"dic llli o" a for fUIIloD for chronic LaP without lItl'nMia Or -.>Ondyl olil theal.:
PRACTICE PARAME. TER 14·3
LI,I'AB . ~
'us<or, ~O~ lBP "'<TOmu'
SH~OSIS O~
SPO><O'"O,-,~ "'ESIS
S l ~nda r ds'": lumt.a.r fusion is rtODmmended for CIIN!rull), Hlected patienu'
WI th d,ublin, Lap due to 01111- or lwo-Ie.ve.i dtgenuat;"e d ~ without sleno01' spondylohathQis
I i.
Options ......: Inlel1l"'e Pl'and cognitIve lh~repy I!I reoommended lUI. option
ft:r pllUenla wjth LBP in whom con.-entiooal mediUlI mon.ment h .. failed
;"1M~~~po6.ulwl_L8Pkr~:l-"_I'II1d~~oI
<boo~"""""U-u"lS-S I , ,,,-._r..<I"""_INdicIoI~
PRACT CE PARAMETE R 14 4 CHOICE o. <1,15'0" T~CH"'OUE
liuldellnU" , ror Ai.I P or AU f'. innrummllltion. the addition ofa posleroI"\.eral r... ion il not recommended"
Options" ;
either a potr...mlat.l!raJ f ...ion Or In loterbody fUl! in... (PUP', 'fU r 0<
AUr) are OptiOfT. lOr pa!.le1llll with LBP dIM to DO D I~ I or 2 J"y~bo
an interbod), graft lI.n option to U1Ipl"O\tf! fulion ratn and functionll
DII\.COmet
III
lh~
ua. or multiplJ: approaehfl (anter>Or" pl»t.I!riorl il nOI recommend-
ed ... I'OIIt",.oplion ror LBP without deformIty
"_"
__
.".1T>""o> ..,..
_
~_""'_. ' III--""IIIme_bk>oa_~
~
.. ...,...., .... _ _
"'' '' .. IrQ..IId~''''' " ...
NEUROSURGBRY
~
~~. _
__
...
.. lINDOiIO,..,
(• .11 a64j' 1IIHTn1
~fuI5on
.~
101_ Spme Ind .pinal cord
'"
TYPE OF SURGICAL TREATMENT
Th. type of surgical proc.
.peeir.c condition ;dentir.ed. Ex·
.mplea.re shown in Tobit 14·6.
DilCullion
options
i•
dura
chosenofi.lOme
tailored
to the
• 1'0 provided below.
f~'~b~"~'''''~i~~~~:;;':O~W~b;';':k;;~1
Lum ba r s pi na l fusion
Although thtre is no conleWlUSOO the indication."', lwnblr , pinal f"lion (LSF) i,
I~pted treatmeot for fracture/di,location or instabili ty
relulting from tumor or inre<:_
tion.
For degenera t ive apine di5'
eUf, practic"" plnunewra IuIve
been developed and are indud·
ed herein .
Options":
lumbar fusion i3 DIl1 routinely re-r:omroended following dilC exci.ion in
patientl with HLD Or recunent HI.D c....inlj" ... dicu lop'-:hy
lumbar fUllion ;. a potenti,ladjund to di lC excision in aolel of a H I.D
or Tee"lTent HLD:
• with ",idence of preoperative lumbar spinal deformity or inlubil ity
• in patients with chronic IUi.1 LBP usadlted with rad.iculoplthy
Ins trum e ntation 1111 an IIIdjunct to fu s ion
Opllo ns" : pedicle oc,...... !lxllinn i. recommended a. I t.r ntllwm t option for petientl with I.BP ~ated with po!!terolateraJ fusion who Ire It high risk for fu·
sian railure~
- . . ...... 0I1*11c1o SC1ews II diSOOU<8ged bK:aoM 01 conIIiaing _
_ ""'_.-.c.oI.......-a>sI .....
01 -.1IDgeI'* _
~
Th e u.. ofin.tNmenlilion increa_ the fusion ratel">. Hardwlre used in the It;..
een« affusion will eventually fatigue, especially in the region of the lumbar IordOlis.
Therefore , iMlTumenlalion mU$t be viewed ala temporary internalltlbili1inl" mellure
while ,waitinl" tha ruaion prooeu to complete.
S urgica l fu lion option !
Eerly experien« with midline f .... ion. rel"lted in luroNr ' pinal ltel108il as 8 late
complication. Then.foT1!, CUlTftDt fUlion t.echniquel ..... pamro-llteral rusiQI<, Or enteri(ll"
or poIten« lumba. inurbody lUlion.
POltenor lumbar interbociy hilio n (PUY): Biliterillaminectomy and aggre&Sive
di&cectomy followed by the place ..... nt ofbane grsf\a into the decorticated dillc .pace. It
h.. been adYOCIIted to redUOl the movement in In abnonna l "motion "gment" (defined
.. lhe lrel between twO vertei:>ra). Relatively contreindicated with well PT1!urved dille_
' pI« height.
Mlny PI.I Fa when atudied ~ 1 ,.."Ialolr Ihow re-<:OUlPH of the dis<: apaCl:', which
raiu. the qUlllion II to .... hether the PUF has I ny benefit over 'i m~le di8CeCtomy.
Sund... lnM PUF. may be _ilted with P'08""!"IIIive lpolldylol i,thesi l ll that leveland Ire usually .... pple ..... nted with pedicle laewtlrodl. PUF i . ..lltively contraindicated when the di,k ' PIOI ia very Iall.
An t enor lUJ'lli>ar In t erbody tulioD: Re ll tively contraindicated in male. beclUse of
ri,k Qrretro..... dt ~"ulltoon in 1-2iio.
JOO
14. Spi .. e and Ipin.' cord
NEUROSURCER Y
PRACTICE PARAMETER 14·, 801<[ G"MT
HI~"UH'S
& SUBsr'HlHS
St an d a rd s ": auto:ogoul boml or ~mbi nallt humin bone mOrph~Mt ie
protein t rhBMP-2) bone grin I ubatitutl iI recommended in Ih, setting of I n
AUF in <'OIljunction wilh I th~aded liUlnium clge
OpHons":
rhBMP·2 i.o conJu.nction with hydn>)(yapa tite and lrio:l!ci wn phOlphate
may be lubLtitut.ed fot lutorran;n lOme callet of ~Olterol~ter~1 fU l ion
n!cium ph.. phate il recom.men ded AI I bona vanaxtendar, upacia lly
when comhined with autoiogoul bone
Aase5Ioi n, auryic:&i lumbar fI.Il lo D: See PRACTICE PARAMETER 14·8.
PRACTICE :>ARAMETER 14·8 R.. O!()(.R"~M'C ASSfSS"'HH Of fUS'O"
StandardS" : It.lIlit ". rays
~lone
a ..
rua r_mended
Guidelines "":
in t he illwln£f or riJid inl tn.oml1\tation.lack o/'mOlion between verU·
brae on laten' n"".o.vuleo.ion x-raya i. high ly au.ggeltive Or,uCff$$_
rul fu.ion
• tedlnetium·99 bone Ka nnin, il DIll recommended
Options", radiOfTaphlc techniquel, onen in «Imbination, mlY be used when
failed lumbar fuaio:l il IUl pected. including: atalic and nel<ionlexte nsion x·
raYI, CTscan
NB:
t~
il welk «Irrelal ion belween fusion and dinic:a.l ou l«lme.
Op tio n s " , tha «I.,...,la l ion belween fu.ion and clinical ou tcome il not s trong,
and in given ,it uaLon fusion sLa tus may be .. n,.d(Jf~ to QUtcome
CHRONIC LOW BACK PAIN
Rarely can an anatomic diagn..il be made in patien ta with chronic: LBP" 3 monthsduralioo" . Abo, lee
P~iol r~IOI'" pace 296. Pat ients wi t h chronic
pain Iyndn>mel ICPS) ",fer to their problems with af_
fecl iveOl"emotional terma with a higher frequency than
th .... with acute pain". The amQUnt of time that a pa·
tient hal bHn out of work due to low back problams i,
related Ul the ch llncea of the patient getting back to
work II.i Bhown in Table 14·7.
14.2.
Table 14-7 Chances ot pao
lien1a going back to work
TlIM out Chancel at gettilT9
at -..:oB
bitt to-..:oB
< 6 mol
50'4
"
""
Intervertebral disc herniation
INTERVERTEBRAL DISC
The funttion of tile intervertebral dill; is to pennit stable motion of the spine while
l upporli.ng an d di stribu t ing loadl under movement.
ANATOMY
Aoul ua fibl'Otlua (IInulu l may alte rnatively be lpelled ann ulUl, but r,b rotul it the
only correct "pe ll ing and II distinct /'rom!ib,.,,'-,'!': the mu ltit.. minsted I.,a"",nl that en·
rom pa .."" the periphert of the di$e apace. AtLach"" \.0 the end·plate ca rtas"" and ring
opophYllul bone, Bland s ce ntrally .... itb th e nueleul pulJlOlU.l.
Nu c:le ull pu lpo.u l : the centra l portion of the disc. A remnant ofUlI! notocord.
C ap. w e': combined fibers ofthe anulul fibror;Ullllld the po5terior longitudina l li(.
ament \th is term i, useful b«au~ th ese 2 stn.oetur"" may not be diltlnguilhable on im'
ft,; ng st ud'''''l.
NEUROSURGERY
14 . Spine lind I pinal «Ird
'"
14.2.1.
Lumbar disc herniation
C LlN!CAL ASPECTS
The posterior longitudinal ligament is atro~at in the midline, and the posterolateral annulus may bear II disproportionate portion of the load . The .... rore , most hemi.
at.ed lumbar disca (HLD) OCCur posterior ly. slightly "ffto one aide, compressing a nerve
root, characteri~tically c81l3ing .""".e radicula r poin . (j.{,<lt of rrea fragmentll that miI!T8te
move superiorly.
Characteristie fmdings on the history often indude:
\ . symptoms may start ofT with back pain, which aft.er days or weeks gradually Or
sometimes suddenly yields to radicula r pain oneil with reduction of the bac k poin
2. precipitating f/lctors: varioWl factors are ollen bl amed, but an! rarely identi fied"
with «,rtainty
S. pain retiefupon nuing the knee and tlligh
4. patients generally 8void e~C<:!$I!i"e movements, however , remaining in anyone po.
sit ion (sitting •• t.anding, or lying) t.oo long may also exaceroot.e the pain, some·
times necessitating position changes at interval. that range from every few
minutes to 10.20 minutes. This i. di.tinct from constant writhing in pa in e.g. with
ureteral obstruction
5. eXlIoerbation with ooughing, ~noezing, or straining at the 5t.ool : t hi, positive
' cough etfeet" OCCUCT~ in 87% in one eeries"
6. bl adder sym ptoms: the incidence of voiding dyafunction is 1·18<J&13'.-. Most
oonsist ofdi fficulty VOIding, s training , or urinary retention . Reduced bladder $/.'n·
satinn may be the earliest finding. Later itis not unusual to !lee "irritat ive" symptoms including urinary urgency, frequency (i ncluding nocturia). increased po8tvoid residual . Less oommonly enuresis, and dribbling incontinence is reported in
radkulopath~ (note: frank urinary retention may be see n in cauda equina syn·
drome, ut be/ow). Occasiona lly a HLD may present only with bladde r symptoms
which may improve after surgery"". Laminectomy may improve bladder function.
but thi, cannnt be allSU red
PHYSICAL FINDINGS IN RADiCULOPA THY
Back pain per se i8 usually a minor component (only 1% nf potientB with scute low
buck pain have $Ciatica' ), and when it is the only presenting symptom, othe r cause..
should be sought (see £,ow bod. poin, page 907 ), Sciatica has such a high sensitivity for
disc herniation , thst the likelihood of a clinically significant disc heroiatio,," in the absence of sciatica is 1 in 1000. ExceptioIl8 include a central disc hemilltion which may
cause sym ptoms of lumbar ~ tenosi8 (i.e. neurogenic daudication)or a cauda eq uina syn·
drome .
Nerve root impi ngement giVO'fl riM to a set or signs and symptoma present to "ari·
able degrees. Cha racteristic $yndromes Bre described rnr the mO$t cornmnn nerve rootll
invnlved (~Nerw mol synd.-omes below).
[n a aeries ofpatientll referred to neurosurgical outpatient clinics for radisting leg
pain, 28% had motor loss (yet only 12% listed motor weakness as a presenting oom·
ph.int), 45% hRd ..,n~"ry di_I>I<Mn,..,. Rnd 51% h~d rene~ ~h~n~ .
N
Findings suggestive of nerve root impingement indude the following. Toble 14·8 shows
the sensitivity a nd «pecHkityofsome findings on the exam among patientll with sciatica.
1. signs/symptoms of ndiculopathy (Il00 Tabu 14·9, page 304)
A. pain radiating down LE
B. motor weakness
C. dennatomru sensory cha~
D. renex cbanges: mental factors may innu .. nce l ymmetryM
2. posi t ive n.. rv.. root teasion sign(s): including LQ~gue's sign (_ below )
3. tenderness over the sciatic notch
Nerve root tension s igns
Includes'":
1. Lasell\1e's sign: AKA straight leg railling (SLR) test. Helps differentiate Sciatica
from pain due to hip pathology. Test: with pstient supi ne , raise amicted limb by
the snkle until pain ia elicited'" (should occur at < 60'. tension in nerve increases
little above this angle).
'"
14. Spme and spinal cord
NEUROSURGERY
A pIlaltiv., tell con,;al.l of leg
pain or
2.
3.
4.
5.
6.
~rilthfSin
in the dia·
Table 14·8
II I
tribution o(pain :back pIIin
lea l
I
II
, Ion., doel not qualify). The pa·
t;e!'lt mBy a llO utend the hip
(by liftina: ito/flabl,,) to reduce
the anile . AlthoUlfh not part of
LaHg'ue', aign. aMI. dOrline.ion with SLR U$ij . lly lUI'
menu pain due ~ nerve root
com preulo n. SLR primarily
tenMI L5 and 51, tA lellllO.
and m"~ pronmal rool.l "ery
little. Nerve·root compreuion
produca. poeiti~ La.Mgue',
aif'l in _ 83" of cases- ( mo~
likely to be poeit;v. in patien""
'" 30ynage wil.l\ HLD" ). May
be po$ilive in lumbosacral
ple~opatb)' (_ PClI{C ~).
r-;'nt.e: n.xi", both thilh. witll
the kf\<!ft .xu...ded (0 ong ... ;(ling" or .itHn,Me.! htenlion)
may be Loleraud furthe r than
nUlD, the .ingle Iy rnptomatie
. ide alone
l'
Cram luI: with patient Illpine, rlise the aymptomBtic leg
with the klM!e alightly n."ed.
Then, ."tend the kneoe. Reaui"" aimilar to SLR
"roued atr algh t leg· r aiaiD' test AKA F llie rszt llin'. alga: SLR On the pain'
len leg ca ......seontralaterallimb pain la greater degree of elevation is usu ally required than tlw painfu l . ide). More specific but less sens itive than SLR (97% of
patients undergoingluTi...., with thia sign haveeonfirmed HI...O*"), May correlate
with a mil"' I:!:DJJ:Dl disc herniation
fe mo r al stretch test'"', AKA ",verse I tra ig ht I"g rai aing: patient prone, ex·
aminer's palm at popliteal fossa, knee il maximally doraiflexed . Often ~itive
with L2. L3. or 1,1 nerve root COO'lprn.aion (e., . in upper lumbar di, c herniation).
or with ntreme lateral lumbar disc herniation (mly a\$o be positive in diabetic
femoral neuropathy or psoas hematoma l; in thelle . ituations SLR (Las~gue·•• ign)
it frequently negative (.ino. L5 &. SI not involved)
"bowatring , i p"; Onte pain oocura with SLR. lower the foot to the bed by fl e";ng
koee, keepiog the hip flued. !kiatic paio eeal ... with thil maneuver. but hip plin
pl:'r:lisu
litting knee""I" nalo n tat: with patientM!ated and both hipa.nd knee! flexed
90' , llowlyextend one knee. Strttch.... nerve roots al much a.I a tnoderatedegree
ofSLR
Otbe r s ips uae.flIl in eva luat ion fo r hun ba r rad iclllopathy
FABER: ao acronym for Flexion ABduction Extern al· Rotation , AKA FABERE
test (the t,ailina:"e" it for ..x """'ion), AKA Patrick·t-tt\$l . A tat of hip O'IOlion.
Method: the hip and knee are flned and the lateral mal leolus il pla<*l on til.,
<:ontral.ter, 1 knfl!. The ipSilate ral knee " ge ntly ditpla:ed downwlrd towarda
!he eum table . Th il al._a the hipjoiM and d_ not ul uilly ..acerbate tru e
nerve-root eompreasion, often ml.k«lly pOti t i"" in the prtsellOe of hip joint disease (e.a: . trochanteric: burlitis.&ft ~ 326), »e roi liiti, or me<:hanical low·back
pain
2. Tren de lenburg .ir'" examin.. obMrv.. pelvis from behind while patient raise,
one lea: while .tanding. Normally t he pelv is rtlIlllin.l horhon tal. A plNitiv. lip
occu.. .... hen the pelvis tllt.l down toward theaideofthl lifted tegindicatina: weak.
neas of the <:ont"lal.etllt thigh add udora (primarily U 1I'lnervated)
3. CToued . d d uct(l ...: in elicitinr kntoejerk (KJJ , the contra llteral thia:h addu~.
tors contract. In the presence of I hmlraet.ive ipeilateral KJ it may indicate an
u~per motor neu ron letion, in the pretence ofl hxgQactive ipAil.terl] KJ it may
be a rorm of patholoa:ical . pre.d, indieatina: nerve root i:"titability
I.
NEUROSURGERY
14. Spine and spinal COld
""
N ERVE ROOT SYNDROMES
Due to the fact.8listed below, a herniated lumbar disc
(HLD) usually Spa",8 the
nerve root exili ng at that interspa~, and impinges on the
nerve exiting from the neural
fora men one level ~ le.g. a
lb-51 HLD usually causes 51
radiculopathy). Thi. gives rise
to the cha racteristic lumbar
nerve root syndromes shown
in Table /4.9
Ta bl e 14·9 Lumbar disc I yndromes
"'
Importan t fatUI in lumbardis:
diaease:
!. in the lumbar region,
the Mrve root exiUl ~
~ a nd in dose pm,,_
imity to the pedicle or
iUllike_numberll(! verJen<lr,,"I ~ """""' . ... moy reln/oree (pa,"'" p ..... t>ana. _"
tebra
againSieach OIh .. wMe ,..tie. is e'ia''''')
2. the in tervertebral disc
medial I>.1msl' .... rene. is unr .. latlle IfoOl a/Wavs PI". 1.51, ma1
space is located well
. '00 S1imulare eadUClGrS when . ' ia~ng
below the pedicle
I _WE.AKNESSIn TaOle tH/. P"!Ie303lot br/la~CIOWIl
3. in t he modal (most
~
MMOrYOnpeir~"I1IO$I_inlloedlSlal."' r_oIlh.
common ) human spine,
.,.,malo.......
the", are 24 prtS9cral
vertebme, however
some individuals have 23 and others have 25"'. Thus, a HLOat the ultima te disc
space(usu ally L5-SlJrnnstn!ten impin.ges on t he 25th nerve rootlhowever, in the
varia nt cases, it may actuaJly impinge on the 24th or 26th rootJ"'
R ADIOGRAPHIC EVALUATION
See Radiographj,c f uoluolion On page 293 under Low back poi" .
N ONSURGICAL TREATMENT
For nonsurgical trea tment, se.e "Conurooli",,·In!lIlmerll. p88e 296.
SURGICAL TREATMENT
INOICA TlONS
In s pite of multiple attempts, nO One has been able to detennine which patients are
likely to improve on their own and which wouJd be better served with $Urgery.
1 r~ il" .... of non_.".gic81 m''''~geme'' t' <W<>r 85% of pr>ti .. nt.!l with 9~l"e diS<" hemia_
tion will imp rove !d.t.kQJI.Is"rgical intervention in an average or6 weeks" (70%
within 4 weeks'"'). Most clinicians advocate waiting somewhere between 5·8
weeks from the onset of rad i(ul<>pathy befort considering surgery (assuming none
of the items listed belnw applies)
2. MEMERGENT SURGERY": (i.e. before:;,.8 w eek.. have lapsed ). Indications!
A. cauda equina syndrome (CES): b<1f bElow)
B. "roartsajye motor deficit (e.g. foot drop): pa resill ofWlknown duration is a
doubtful indica t ion for surgery 01 . . . . . (no study has doc:ument.ed t hM there
is less motor deficit in BurgicaJly lreated pa t ients with this finding) . How·
ever , the acutecevelOpllleolor progre&!lion of motor weakness isconsidered
an indication for rapid surgical decompreS8ion
C. 'u r~nt' surgery may be indica ted ror patients whose pain .... maios intole r·
able in spite of adequate nan:otic pain medication
..... _""li.ono iBdud.: II 0, 13";b t....rinr;: ...... b.... ora l~mboN<r.l tnm. it ion.I . . .... .....: <he te,·
minology of. -l~rnb .. li:ted S t ·'..... br... • 01"' -... ,. li«<ll.5 ....... brae- i. irn~l"ffi .. and <OrIN.inll'
14. Spine and spinal cord
NEUROSURGERY
3. :t pat.ien~ who do not want to invest the time in a trial of non·surgical treatment
if it is possible thllt they will still require ~urgery lit the end of the trial
Cauda equina lIyndrome
Syndrome usually due to C()mpreSllion of the cauda equina. See Tllbl~ 17.70, page
517 fllr featUr1l8 to h~lp differentiate CES from a eonus lesion.
Possible findings in CES:
I . sphinCU: r disturbance:
A. urinary re\.eotioo: the most consistent liDding. Sensitivity _ 90% (at 8I)me
point in time during (ourse l '''''·'. Have patient empty bladder and (hed:
post-vo id residual. In a patient without retention, only 1 in 1000 will have
a CBS. Cystometrogram (when done) shows a hypotonic bladder with de ·
creased sensation and inCr1lased capacity
B. uri.o.Pry and/or f<!'Cal incontinence'" (some patienlJl with urinary retention
will present with overllow incontinence)
C. anal spbinct<!r tone: diminished in 60·80%
2. "uddle IIneslhu)a ": the most COmmon sen8l)ry deficit. Distribution: region of
the anus, lower genitals, perineum , OVer the buttocks, posterior-superior thighs.
Sensitivity -75%. Onoe total perineal anelltheaia develops, patJenl$ tend to have
permanent bladder paralysis'"
3. significant motor weakness: usually involves mOre than a aingle nerve root (if un·
trooted , may progress to paraplegia)
4 . low back pain a •.d/or sciatica (sciatica is usually bilateral. but may be unilateral
or entir1l1y absent, prognosi, may be worse when absent or bilateral'·')
5. bilateral absence of Achilles reflex has been no~'oo
6. "J<ual dysfunction (usually not detected until a later time)
Etio logies ofCES includes:
I . massive herniated lumbar disc: ue below
2. tumor
A. from compression: e_g. with metastatic disease to the spine with epidural
extension
B. Intra vascwllrlympho mlltos ls (B.celllymphoma): a circulating lym·
phoma without solid mass(s""pagt463l. Often presents with CNS findings:
CES, dementia, enhancing meninges on MRI , lymphoma cells in CS F
3. trauma
4 . spinal epidural hematoma
5. free fat gran following discectomy'·
6. ankyl08ing spondyliti $: etiology is often obscure (Ut page 344)
CES rrom HLD: May be due to mllJJsive ruptured disc, usually midlioe, most COmmOn
at U ·5. often $uperimp:!aed On a p~J<isting condition (spinal stenosis, tethered
cord ... )'''.
Prevalence ofCES:
I. 0.0004 in all patient$ with L.BPOO
2 . only _ 1-2% ofHLD that come to $W"gery""
Time course CES tends to develop either acutely, or (less typically) slowly (prognosis
is wOrse in the acute onset group, especially for return of bladder function, which ocC\l~~Gd in only _ 50<1.)'110. 3 l>atw~M'OO:
Croup I . sudden onset ofCES symptoms with no previous symptoms related to
the low back
Croup II • previou, history ofr<!'Current backache and sciatica, the latest episode
resulting in CES
Group III • preflentation with backache and bilateral sciatica that later develop
CBS
S urgical in ue" A bUaterallaminectomy i. advised'''. O<:casionally, when it i. difficult
to remove a very teose midline disc, lransduTal removal will be n<!'Cusary'"'.
Timing or di_etomy in CES: controversial, and the pJint of contention in nu·
meroWllaw suils , In ~pite of early repor15 emphasiling rapid <:k><:ompreS!lion'''', other reo
porta found nO correlation between the time to surgery aller presentation and th e return
of function'''' "'. Some evidence supporta the gool of performing surgery withln 48
hou rs (although performing surgery within 24 hours is desira!>le if possible, there is no
statistically significant proof that delaying up to 48 hrs is detrimental)'''' '·.
NEUROSURGERY
14. Spine and spinal co rd
J"
SURGICAL OPTIONS FOR LUMBAR RAOICULOPATHY
OI'lC<! it i. decided to trut . urgicaU,. options include:
L
lral\l~llnal
appl'Olllchu
It andard open lumbar laminec:l<Imy lind dikeclomy: 65·8S~ ~ported no
. dlltka one yell' PGlt-<>p ((lmp.a.~ to 3&10 for con.ervative t .... lment' ...
Long-term fUlIl", (> I ~ar) were . imilar. 10'11> ofpatienLi underwent further back s urge ry during the fi r. t ,u,'"
B. "microdi$Ce<:t(lmy·"""': " mila r to , t. l'ldard procedun!, however am. Her in_
ci' ion il utiliud . Advantage. m.y boI rosmetie, . hortened hoepitalltay.lowat blood 10". May be more difficult to retriev • .orne fngmenu"'"'''''' '''.
Overall efficacy is ,;ma.r to sta ndard discecl.Omy'H
2 . int.,d iscAI procedure. (SIt /)flow)
A. ehemonuclwly.i,: using chymopaJ)1lln (_ btlow)
a . automated perc utaneoul lumbar dise«tomy: utilizes. nudeotome
C. perc ut.BneouI endGiCOpic di.~t()my: ' " /)flow
D. ;n(radi"".. ] endothermal the rapy UDET or IDTN : IN bdow
E. 18ser diS/: deoompreli$ion
1\.
C h e mo Duc\eoiYlli 9
Ac<:eplllb~ trea t ment, but Ie.. efficacious than routine 0' rnicro-d itoeetomy'. Ut ili,es chymo pa pll;n (Chymodi l.eti~) iojected ;ntr.dilca lly. Proven nlore etreelive Ihl n
placebo injection "" II •. Typical.u<:ce.M nlt.eI: at I yur 85... ofpalienU undel'iOin.r di.$·
<:edomy had good or excellent resulU compared to ••,..,,, to
forroemonueieoly. ..
(CNL). Aithough S/:iatica improvu in botb group', only lbedi.eceetomy group had . ipjf.
ic.nt improvemenl in back pain' ''. In one . tudy, a t 6 month. ~ of patienu ioili.ily
h8ving CNL hlld undergone surgery for unrelieved . ymptoms'''.
RiskB'·''':
Ri$k of th e significant complication of lUlaphylaxi. (~timel fatal) may be reduced by sk.in·teats for .1Iergic Hnsitivity to thl 'lIent. Other complicalions reported indude: diS/:; t i.,H. neurologic injury. vascular injury, thrombophlebitia, PE. tr.nsvene
myelitis'" (very uncommon ).
63,..'"
Intradisea l surgical procedures (lSP)
[SP. (.ft below for specific procedures).re among the IOOIt controversial proceduret
for lumbar spine surgery. '!'be theoretical advantage is that epidunolsearring i. avoided,
IlIId that a smaller incision Or ""enju,t a pt.lIIdure site is u$e<!. Thill i. also purported to
redue<:! po6topenotive pain and hospital stay (o!\en performed all 8n outpatient procedure). The collCflptu.1 problem with ISPa is tha t tbey are di rect...d a1: removing disc mao
terial from the centerohhe disc space (which is notprod""ingsymptonw)8nd rely on the
reduced intradiseal pressure to decompress the herniated portion oft.he-disc from the
ne .....e root. Only _ 10. 15... ofpatienu eoosidered for .qal treatment ofdisc di.eaae
artcandi d8tea for.n iSP. ISP. are ... uallydoneurnier local Me5ti>etlC;n order topenni t
t he patient to ~port ne ..... e root paio to identify impin~~nt on a ""rve root by th<! Sur·
rical in, trument or needl". Overall. ISPI are not I'KOmroend~ until controlled trials
prove the efficacy '.
Ind ication. util il~ by proponeot.ll ofintradisce l procedures:
I. type of disc herniation: I ppmpriate only for "contained" disc hern iation (i.e. outer
ma "-;n of anu lul r.brosu. ;nUld)
2. appropriate ]evel: best for U·S HLD . May allo be uJIed II L3-4. Difficult butonen
worbble (utilililllll.nlled inatroment.a or other technique,) at 1..5-51 beeauge of
the angle required and interrer~1"ICOI by iliac crest
3, not recommended in presence of"HVere I'\eurologic defICit '"
Re.ul u:
"SU«eII" rate (_ pain f~ and retum to work when appropria.te) reported ranges
from 37.7511.'.'''.
Au tom a ted pereu taaeoualumba . d i..::ectomy, Utiliztt . n ... deotome'" to remove
dilC material from the untet ofth. intervembral dilC apace. Sil"iticalltly leu efficacio... than cbymopapain ''', ...,th l}'Nr ' UCHM nlltof37'40 (c:ompaml t.o 66,.. for CNL),
ComplicalionJ include cauda equina , yndrom<:t from improper n""leotome placement'·.
[.alter d ilC d ecamp",.. ;on: IIIJertion of a needle into the di lC, and Introduction ofala·
Hr fiberoptic cable throulh the need le to allow al.ate r to b... rn a hole in the center of the
disc .... 'J! (with or without ndoseopic vitualitation),
14. Spine alld ' pina l cord
NEUROSURGERY
Percutaneoull e ndosco pi c lumbar dil",ectQmy (PELD): Thi$ ~nn refers to a n essentially intradi5"81 procedure indicated primarily for contained disc hemiations, although some small "nooconwined" fragroenUl may be treatabl~'>I. No large randomiud
study has been done to compare the technique to the accepted s tandard, open discectomy
(wilh or without microsco~). [n One report ...... of326 patients ",ith LA·S HLD. only 8 ap·
propriate candidates for PELD (i.e. 2.4% ofHLD at L3-4) W~re found. Of these 8 , only 3
were reported as havinga good result. This study is not adequate forevaluating the technique.
Intradi scal endotbermal therapy (lDt.'T): AKA intradiscal electrothennalanuloplasty (lDTA). Efficacy: 23·60% at I yea r for treating"internal discdisroption"'" (radial
fissures in th e nucleus j:>ulposus extending into the anulus fibrosus) which is purported
to account for 40% ofpatienUl with chronic low back pain of unknown etiology'·.
A DJUNCTIVe TREATMEIflIN LUMBAR LAMINECTOMY
Epi dural steroids following di scecto my
In a single-blinded non-randomized study oflhe u~ or fJ).i.!1luaI steroids (methylprednisolone acetale (Depo- Medrol®). dor;e not specified) irriga t ion of the thecal sac and
nerve root following discectomy prior to wound closure found no statist ically s ignifi<:ant
evidence of benefit in t",ms of amount of post-op analgesic medication needed, du ration
of hospital stay , or time to retum to work'''. However. the combination of sysftmic steroids at the start of the use (Depo-Med rol® 160 mg 1M and methylpredn isolone sodium
su«inate (Solu ·Medrol®) 250 mg [V) combined with infi!tration of30 ml of 0.25% bi puvicain,, (Marcaine®) into the paraspina! muscles at incision and closure, may reduce hos·
pital stay and post·op narcotic requirements'"'.
Method s to reduce IIcar ronnatioo
Epidural r..... e rat gr-aft' The use of an autogenous fl"fll fat graft in the epidural space is
a fa irly common practice, that i.!I employed in an attempt to reduce post-op epidural scar
format ion. Opinion vari" widely as to the effectiveness, some fe.:,l it is helpful , other$ fe.!l
it actually ex ace rbales seamng '''. 1n some patienUl, no evidence of the graft. will be found
on reoperstion years later. The rat graft can very rarely be a cause of nerve root
compression'" Or cauda equina syndrome'" within the first few days post-op. and there
i. a case report Qfcompr~nion 6 years following surgery '''.
Otber meaau ..... s: Other measures include the placement of barrier films or gels"'.
RISKS OF WMBAA LAMINEcrOMY
Overall risk of morta lity in large serie8"~ ,<3: 6 per 10,000 (i.e. 0.06%), most ollen
due to septicemia. MI . or PE. Complication rates are very di lli cult \.0 determine
accurately''', but the following is included as a guideline.
Co mmon complications
(consider discussing these as part ofinforllled consent)
I.
2.
3.
4.
infection:
A. superficial wound in fection: 0.9·5%'''' (risk is increased with age,long tenn
steroids, obesity. ? DM): most are caused by S. IJUP"('U5 (oee Laminu/cmy
wo"nd ill{tCfWII. page 216 for managemenl)
B. d .... p infection: "" 1<Jl,( .... 1Hk>w undor U".,.""""." , ""mplicalio,..)
increased motor deficit: 1·8%(some transient)
unintended ' incidental'durotom~ (S'-'" bit/ow) incidenoe i.!I 0.3·13% (risk increases to _ IS% in re-do operations)"'. Possible sequelae incl ude those listed in Tobie
14·10
A. CSF fistula (extemal CSF lea k): the risk of a CSF fistula ~uiring operative repair is _ 10 per 10,000'"
B. pseudomeningocele: 0.7.2%'" ( may appear sim ilar radiographically to spinal epidural abscess (SEA), but post-op SEA o!\.en enhances, is mOre irreg'
ular. aAd is associated with muscle edema)
recurrent herniated lumba r disc (&a rne level either side): 4% (with 10 year rollowup)'" C.... e page 317)
Uncommoo comp licat ions
1.
direc~
i!\j ury to
NEUROSURGERY
~u ral
strocturea. For large disc hernialions, <:(Insider a bilalera!
14. Spine and spinal coro
2.
3.
4.
5
6.
7.
8.
9.
exposure to reduce ri~k
injury to structu"", anterior to the vertebral bodiu (VB): injured by breaching
t he anterior longitudinal ligament (ALL) through t he disc space, e.g. with pitu·
itary rongeur. Tho> depth of disc space penetration with inlltruments should be
kept ~ 3 em , since 5%of lumba r disca had diameteTlu small as3.3 em'''. Asymptomatic perforations cfthe ALL occu r in up to 12$ ofdiscectomi..... Breach of the
ALL riaks potential injuri .... to:
A. great veliSels"': risks include poteotial1y fatal hemorr~.age, and arteriovenous fist ula which may present YMnllate r. Moat aueb injuriea OCCur with
U·S discectomies. Only - 50% bleed into th e diae space intraopentively.
the rest bleed into the retroperitoneum. Emergent laparotomy is indicate<i,
preferably by a surgeo;>n with vascular surgical experience, [f available. Mor_
t.ality rate is 37·67%
I. aorta: the aortic bifurcation is on the left .ide ofilie lower part of the
lA VB, and so the aorta may be injured above this level
2. below lA , t he a:)mmon iliac arteries may be injur..d
3. veina (mOle common than arterial injuries)
a. vena cava at and above 1.4
b. common iliac veins below lA
B. ureters
c. bowel: at LS·SI the ileum is the most likely viscus to be injured
D. sympathetic trunk
ran! infections:
A me ningiti,
B. deep infect ion: « l'itt. Including;
I . d i,..,;tis: 0.5% (sfe ptJ//f 245).
2. spinal epidural absceu (SEA>: 0.67% (ree po.ge 240)
cauda equi na syndrome: may becaused by post-(lpapinai epidural hematomll(su
bdow). Incidence wao 0.21'11 in one series of 2342 lumba r dd.te<:tomiu'" and
0.14 % in a aeriea of 12,000 spine opera t ions'''. Red flags: urinary n!l.ention, Dnesthes ia that may be I18ddl~ or b.i.la.tJ:m.l LE
complicationBofpoaitioniog:
A. compression neuropathies: ulnar , peroneal nerves. Use padding over elbowa
and avoid pressure on posterior popliteal r<><lsa
B. anterior t ibial compartment syndrome: due tQ preaaur~ on anterior com·
partment of leg {reported with Andrew'. frame). An orthopedic emergency
that may require emergent fasciotomy
C. preaaure On the eye: corneal abrasioos, damage to the anUlrior chambe r
D. cervicalapin e ;rouries during )XI'!itioning due w relaxed muscles under an·
esthesia
post op arachnoiditis: risk factors include epidural bematoma, patients who tend
to develo\l hypertrophic s<:a r . post op disci tis, and intrathec:al if\jection of Pant<>paqul4l, anesthetic agents or steroids. Surgical treatment is dia.appointing. In·
tmthetsl depo-medrol may provide ahort-te rm r.,lieflin 'pili! of the fact that
steroids are a risk faewr for the development of arachnoiditis). Nsoset ptJ//e 315
th rombophlebitis and deep-vein thrombosis with risk of pulmonary embolism
(PE)"': 0.1% (see Thrornboembo/um in rt.t"roa"rgt ry. pllge 25)
reflex sympathetic dyatrophy (RSDl : IuuI been reported in up to 1.2'11 of CS$e$,
usually after J>(lllteriordec:0Illpre8lJion with fusion. often follow ini: reoperlltions'"
with onset 4 days to 20 weeka post-op. See pogt 396 for a critiqUl! ofRSD. Treatmentincludea some or alJ of: PT, sympatheticbloc:ks, oral methylpredniwlone, reo
moval of ha rdware ifany
very rare: Ogilvie's ayndrome(paeudo·obatruction of the colon) hall been reported
as a a:)mplication of spinal surgeryftrauma , spinal or epidural anesthesia, spinal
metastal!e6. and myelography''l
Uni nte nded dur o tomy
Unintentional opening of the dura during spinal surgery has an incidence of 014%'''".
T e rm ino logy: The terms · u:!intended durotoroy·, "incidental durotomy"''', or even just
"dural opening", have been recommended in preference to ·dural war" wbich may imply
careles.sneu'''when none wu present. Dural openingll have been auoc;ated with One or
more aUl'ged complicationa o. sequelae in medical malpractice suits mvolving s urgery on
tht lumbar spin e.
14. Spine and spinal a:)rd
NEUROSURGERY
The injury: By itself, opening the dura inten tionally or otherwise is not e~pected to have a
Table 14·10 Possible sequelae
deleterious effed on the patient '#. .... In fact,
of dural opening
dural opening i. ofU!n a standard part of the
op" .... tion for intradural disc he,..,,;ation' '', tu·
mors, etc .. Although not frequent, unintended
durotomy is not an unusual oe<;urrence, and
alone, is not con sidered an act of malpractice.
However, itmay result froman eventor events
that produce more serious injuries. Thest!
events and if\iuries should be dealt with on
their own meri ts.
Possible sequelae indude those listed in
Tobie 14·10. A CSF leak may produce 'spinal
headache" with its a!lSOciated symptolTUl (S«
past 46), snd if it bresches th e s!tin it may be
a risk factor for developing meningitis. Pain or
sensory/motor deficits may be associated with
injuriea to nerve roots ar herniation of nerve
roots through the dural opening.
Etiologies: For incidence. S« oboue . Potential causes are many, and include"' : Wlanticipated anatomic variations. adhesion of the dura to romoved bone. slippage of an instrument. an obscured fold of dura caught in a rongeur Or curette. thinning of the dura in
cases oflong!!ta.uding SWnosis. and the pos.sibility of a delayed CS~'leak caused by p"r·
foration ofthe dura when it expands onto a surgically croated spicule of bone'''. The risk
may be increased with anterior decompression for OPLL. wit h revision surgery, and with
the use of high .speed drills ''''.
Tn:atmeot: [fthe opening is recognized at the time of surgery, watertight primary clo·
sure (with or without ps tch graft) should be attempled with nan absorbable s uture if at
all possible to prevent pseudomeningocele andlorCSF fistula . Fibrin glue may be used to
supplement primary c!C5Ure lU.
Although bed rest.o: 4--7 days is often advocated to reduce symptoms and facilitate
healing. when watertight c1o~ u re has been achieved . normal post·op mobiEtation is not
a.ssociated with a high failure rate (bed reat i! recommended if symptoms develop)'''.
In one report ofS patienta with leaks that appeared post·op, re-Op"rat;on wa~ avoided when treated by resuturing the s!tin under locsl anesthesia, followed by bed rest in
slight Trendelenburg position (to reduce pre\lsure on the leakage site). broad spectrum
antibiotics and antibiotic ointlllent Over the s!tin incision. and daily puncture and drain·
age of the subcutaneous collection"'.
Also, set! po.ge 46 for other treatment measu res for HlA associated with CSF leak.
PosT-QP CARE
P ost-op orders
The following are guidelines for post-operative orders for II lumbar lam.inectomy
without intra-opera tive complications: variations between surgeons and ill$titutions
muat be taken into coru.ideration:
1. admit post·anesthesia recovery (PAR) unit
2. vital SlgoS On the nursing unit: q 2" II: 4 hNl , q 4" II: 24 ' , t hen q S"
3. activity: up with ass ist. advance as tolerated
4 . nu !"!!ing care
A. 1'5&0'$
B. iDteno;ttent catheteri .... tion q 4·6' PRN 00 void
C. optional : TEO hose (may reduce risk of OVT) or PCB
D. optional (if drain usedJ: empty drsin q 8" and PR.'I
5. diet: clear liquidll. advance u tolerated
6. IV: 05 112 NS +- 20 mEq KCIII @75 mllhr.OICwhen tolerating PO well (after an ·
tibiotics D/C'd if prophylactic antibiotics are U$oo )
7. meda
A. laxative of choice (LOC) PRN
B. sodium dOC\ln ate (e.g. Colace®) 100 mg PO BIO when tolerating PO (stool
softener, does not Bubstitute for LOC )
C. oplwnal: prophylactic antibiotics if used at you r institution
O. acetaminophen (TylenoJ®) 650 mg PO Or PR q 3" PRN
NEUROSURGeRY
14. Spin e and spinal cord
."
£.
8.
fCOrcot.ic lJnlJlgf,h;
F. lJplilJnlJl: .teroidlll!"e ulled by some I U rgelJns tel reduce nerve·root irritlltilJn
from . urgical manipuilition
labs
A. lJplilJfUJl fif l ignj{lCtJrll blood 1~1 during 'ur~ry): CDC
POlt-Op c bec k
In additioo 100 routine, tile foIlO""ng . lIou ld be cheeked:
o t . 'lr'enith ofl_er tlltrem'tiH, Mpedlilly muteles relevllnt 100 nt-rve root. e.g. gill'
trocnemiul for L,5·S1 surgery, EHL flJr lA·S .urgery ..
a 2. appeart.r>c. of dressing: look for l ign. of nreSlive bleeding. CSF leak ...
a s . • ign. of Clludll equilu. syndrome (1ft /KIIJc 305). e.,. by post-op .pin.1 epiduTlI
hematelm.:
A. loti of peri nul "nution (' •• ddle .neslhtli.· )
8 . inability to void : may not be not unulu.1 .f\.er lumbar laminectomy. more
C(Once ming ifa(:((l:npanied by ION ofperiM/l I "filiation
C. pain out of the ordi nlry ror the post-()p period
D. wealmesl of multiple m....,l. graup$
Any new Murologi( deficit should prompT. rapid euluation for . pin.l epidural
hemotoma' " (EDH) . ~Iayed defi";uo may be due to EOH or epidural
Post.-op
films in the recovery room can rul e out graft or hlrdwan! malpotitioo for fuaio ... or in.
slrumentlltion procedures, orchangM in sUgrunent. The dilgno.tic!at oI'ehoice i. MR1.
Ifcontraindicated or oot available. CTlmyelography may be indic:llt.ed. An extradural defect immediately post.-op .uggesta ECH .
.hKa,.
OUTCOME OF SURGICAL TREATMENT
In a stries of 100 patientB undergoing diseectomy, at I year post-op 73.. hid com·
plete relief oneil' pain and 63% had complete relief of back pain;.t S-10 yea .. the numbef1!l were62% for each ~ategory". At 5-10 yeart post-op. o nly 14% felt that the ~in will
the seme Or worse than pre-op (i.e. 86% felt improved), and S" qualified .. h.vinll' a
fai led back aynd r .. me (not returned I.() w"Tk , requiring analge\lio:., receiving w.. rlter'1
compenaation, see Fu.ilt!d bac.\ ~"dromt!. page 314).
In the only random ized atudy comparing standard diMJect.omy with COIlSe ... Bt.Ve
treatment, two groups of. SO patienta with a document.ed hemi.ted d isc that failed tel
improve afl.er 14 d.y. of rut (without strong indicstions for SU~I)', e.g. csud. equin.
syndrome, unbearable pain ... } were randomized to surgeI)' or cootinl>l.'<i CI;InSl' ... ative
t restment (h_ever, . 2S'I(, ofpatienuo {roll) Ihe <XHl1e...ative treatment group were referred to surgery for prolonged or worsening pain). There will a .ignificantly bett<>r outcome at 1 year follow-up in tho! aurgkal grouP. this was not signifi(.8.1lt at4 years, Ind at
10 yurs neith<!r gnrup reported lCistictl or ba(k pain". provided lb.t pat>enta who did
not improve sati.f.cloOrily .n.:r conservative lTe8trnent underwO!nt s l1lllery.
In patient.l wilh. dimiru.hed knee-jerk or ankle.jen. pr1!-<Ip. 35<J,and 43<1(, ( re!lpec'
tively ) 'ti ll had reduted renexu I year post-op"; rtnens wuO! lost post-op in 3'1(, snd
10'l& rffpeetively. ThO! ..me study found Ihlt mol.()r loa was improved in~, Iggravlted in 3",.nd w" newly PreHnt in 5* post.-op; and that lel1lOry loa was improved in
69'lo and was worsened in 15" post-op.
Recurrent diK hemistion (m' pu.gt 317)
HERNIATED UPPER LUMBAR DISCS
(UV£lS LI-2, L2-3. & L3-4)
lA-S &. 1.5-S1 herniated lumbar disc. (RW) account for most C8SC$ of HLD (up 100
24'111 ofPl"tienta wilh HL.D at L3-4 frequently have a PlSt history of. HLD It lAo
S or L,5·SI. IU"estinll' a reneraliztc! tendency taward, dill( hern •• tion . ln. te ri« of
1.395 HLDt, there W.'I 4.t L I·2 (O. ~ incidence), 18 It L2-3 (I .3'iIlo). Ind SI at LS-4
98~);
(3 .6")101.
PRESENfATION
Typiully presenU; wilh LBP,onselfoIlQWingll'tiumt.or at .. in in SI". With prove.·
.ion. paresthesia.,nd pain in 1.he anuriorthillh occur. with complain:.. oriel .... alme..
(Clpecially 0<1 atoending , tai ..).
'"
14. Spine .nd lpinal eord
NEUROSURGERY
SIGNS
Quodriceps femonl wos !.he mOfit oommOo'l muscle involvt'd, demon~tra\i ng weak·
nesa and sometim e&. atrophy.
S trai~htJeg r~ising was positive in only '10%, P&(l8S st ret.<;h Le$Lwas pooi tin in 27'Jl>.
Femoral strclI:h (en may be positive (.., />Ott' 303).
50'\ hod reduced Or eh/;o>:M knee jerk; 18% had ankJejerk abnormalities: nlfiex
wangel! were more common witl! WI·4 HLO (SI,..,) lhan L j .\! (no"e) or L2.3 (44%).
EXTREME LATERAL LUMBAR DISC HERNIATIONS
De fin ition: hern iat ion
of i!I disc at (foramina '
di$C herni lltioo ) Ot dis!IIl
to (u trafo ramin a l lurabar disc he rnial lon ) t.... e
facet (lome authors do r,o t
consider foraminal di6C
herniation 1.0 be ""Klreme
lateral"). See Fisu.~ 14 -1.
I ndden~.. (_ T"bJ~
14· //) , 3- 1 ~ of hern iated
lumbar discs (HLD ) (""lies
with highe r numbers'" in·
dude some HLD thot aN
not truly exl~ttU laLera!),
Di fTefll from Ihe more eommon (man!. medially loc;atell) HLO in that:
the nerve root in·
vol,,~d Is u~uaJ1y the one eKi tlnl~ that levol (c. r. the
Table 14-11 Incirvot eKitinl a t the level below)
dence 01 eX lreme lalstraigh t leg raising (SLR ) is negative in 85-90% OfC8&eS
eral HLD by ]eveJ'
., I w"""k 8~r uR!;eL(udud mg double henJ;lItions:
DIse Ihel No.
- 65% will be negllt.iv~ ifdouhle hern illtions are indud4
edl; m ay have posit ivI'. femoral strekh teu{.ap<!Jf,3f)3t Lt·2
pa in i~ reproduoed by laural bending to the lIide of her· ~.
niation in 75<K.
3S
~.
myelography a lone rartly di~g"O!Itic (u~uatJy ""luifllfl
l ..
~
CT''''''' or MRl)
higher incidenu of ntrud~ fragment.!! (60% )
"'51
higher incidenu of double herni~tions on t ha IIIIme side
at the .a.me lev..1 ( IS'JO)
pai n tend. to he more !leVere than with rou tine HLD
(may be due to r.ct t.h~! the dor8al TOOtgang1ion may be co mpressed dirK !lyl
Occurs most common ly at..kl.:li pnd next a t La,"" (..-f '("ble II-II), thu~ lA il the
most COmmon nerve invDlv~d and I...'l is ne><L With a clinical pietu~or~n upper lumbar
' '', ........ ·l'OOt <»"'p ...... . ion ! i.~ . ""diculop.tI,l' ...-ith no>ij~tiv. SLR). "h"""" ~'" _ g to I tha I
it i, an ext remel,. late ... 1 HLD rather than an upper lumbn disc he rniation ,
..
•
"
"
.,.
'"
• '
,
.
PRESENTATION
Quadric'!ps ",·ea kn eBl. reduction ofpa te Uar reflex. and d,minisht'd sen8 Dlion in the
L3 or U der(091.Onle are tbe most comnlon ('ndings.
DifJ~ rent , al d;agn~i. ind udes:
1 late ral reces.'~nosi$ or superior artic ular face! hl'per1TGphy
2. relropj!ritoneal heOlatomft or tumor
3. diabf!tlc neuropath,. ( .m,.orTDph,.~ Uf p<JIJ;e fjij6
'I. spin all.uWOT
A. benign (schwannoma or neurofibromal
8 . malignant (umOI'1l
C. lymphoma
S. i,,(<<tiou
A. localized (. pinMI epidur1Il ablicess)
NF.UROSURGF.RY
14. Spin!! and Ipina l co,'d
a. plSmIS mWlde ab3<:e!lll
C. granulomatouadisease
6. spondylolisthesis (witn pa rs defett)
7. compress ion of conjoined nerve root
8. on MRI. enlarged foraminal veins may mimic extreme late ral disc herniation
RADIOGRAPHIC DIAGNOSIS
Radiographic diagnosis may be elusive. and up to one third are initially misaed'~.
However. ifactively sought, many asyroptomatit far·lateral disc herniations may be
demonstrated on CT or MRJ.
Mye logl"aphy : fails to disdose the pathology even with wa ler ooluble contrast in
87 % of rases due to the fact that the nerve root compression Dl'<'U1"8 distal to the nerve
root sleeve (and therefore beyond the reach I)fthe dye)'''.
CT $Can"': reveals s roaM displacing epidu ral fat and encroaching on the intervertebral foramen or late ral re<:us. compromising the emefJing TOOt. Or. may be Illto:ral to
foramen. Sensitivity is - 50% and i8 similar with poll-myelographic CT..•. P09t-diseography CT'" may be the most sMaitive test (9 4%)" '.
MRI: similar sensitiv ity to post-myelographic CT. Sagittal views th rough the neura l foramen may help demonnrate the di.., herniation'''. M RJ may have _ 8% false positive rate due to presenceofeolarged foraminal vei ns that mimieex~me lateral HLO'~.
SURGICAL TREATMENT
Fo ramin a l d is c s
Usually requires mesial facetectomy to gain acress to the region lateral to the dural
sac without undue retraction On n~rve root or cauda equina. Caution: total facetectomy
combi ned with di$Ct!Ctomy may resu lt in a high incidence ofinstabiHty (tota l racetectomy
alone eau.ses _ 10% rateofslippage). although ot he r aeries found this risk to be lower{~ 1
in 33'" "'). An alternative technique is to removejus~ the lateTaI portion of the superior
a rticular fa"'!t below ..•. Endoscopic techniques may be well suited for hero.ia~ discs in
this loeation'''.
Disc s herniated heyo nd (lateral to) t b e fo rame n
Numerous approaches are used. including:
l. traditional lDidline bemilllminect.omy: the ipsilftteral facet must be partially
Or completely removed. The safest way to fiod the e¥.iting nerve root is take t he
laminectomy of the in ferior portion of the upper verteb ralle.el (e.g. lA for a lA5 HLDl high enough to expose the nerve root axilla, and then follow the nerve la t.
erally through the neural foramen by removing facet until the HLD is identifIed
2. late r a l ap pro ... ch (i. e. eJ(tra-<anall through a paramedian indaioo''". Advantages: the facet joint is preserved (facet remov al combined with di5cectomy may lead
to instability). muscle retraction is easier. DisadVantage" unfamiliar approach
for most surgeons an': the nerve ca nnot be followed medial to lateral
DI SC HERNIATIONS IN PEDIATRICS
Less than one pero::ent of su rgery for hemiated lumbardiS(: is perfol"Tlre<l on patients
age . of 10 and 20 yr8 (ono &eri"" a~ Mayo found O. ~ 'lo of operated HLD in
patientll ., 17 yra age"'). These patients often bave rew neurologic findings ex"'!pt for a
consisten t ly posi t ive straight leg raising test"'. Hemia~ disc materisl in youths tends
to be firm , fibrous and strongly attaehed to the ca rtilaginous end_pla te unlike the degen_
erated material usually extruded in adult disc herniation . Plain radicgraphs disclosed an
unusually high frequen9 I)f <ongenital spine aJlQma.lies (t ransitional vertebra. hyper lordosi s. spondylolisthesis. spina bifida .. .). 78% did well alter thei r finlt operation"'.
bc~wcen ~he
INTRA DURAL DISC HERNIATION
Herniation ofa fragment of disc into the tbecal sac,or into the nerve rootsleeve{the
latte r so metimes referred to as "jntraradicular'" disc herniatio n) has been reoogni~
wi t h a reported ind<i<ll>Ce of 0.04-1.1% of disc herniations'''' "'_ Although it may be ,u,_
pected on the basis of pre-op myelography or MRI. the diagTlO.'lis is rarely made
preoperativelym. l nttsoperstively. it may be suggested by the impreasion ofa tense firm
14. Spine and spinal cord
NEUROSURGERY
ma.. w,thin the nerve f'1;IOt sleeve or by th negative e~ ploration of a level with obvious
clinical 'tgnl lind dear Cut radiographic abnonnalitiell (aJ\.er veri fying t ha t t he correct
level is fllIposed ).
S\lrlJical ~atment:
A..Ithough a l urgical dural opening mllY be
nec:esury in a minorit)' of cateS"'.
u tili~"".
othoers have found this to be
INTRAVERTE8RAL DISC HERN1AnON
AKA Schmorl's Mde or nodule. AKA &hmor'. (no ' I") nocule AKA Gf!ipel hoemill' lS.
Disc hernia t ion th!"(lugh t ill! cartilaginoua end plate into the cancellous bone of the ver·
tebral body (VB) (AKA int ral pOnlJiO\lS disc herniation). Ol\en an incidenta l finding on x·
ray or MR I. Cli nical aigDificn nce i. controveraiBI. May prodUCtl low back pain inilially
that laua ~ 3-4 montha al\eronHt . Di ff\la.edi.lplactroent(u may be seen in osteopOrosis l
i. IOmet,mes Nlferred I<:> Bla blillooD d i~·.
Clinic al findinga
Ou ring the acu te (_ymptoma t id phase, patient.l may exhibit LBP that i. aqt1lvated
by weight bea ring and movement. There may be tendem"l to pereu.-Ion or manual
compTenion over t he involved a.egment.
Radiographic flndin lf'
Plain x·ray: ,,33% may be lun on plain x·rayl''" .
They may not bedetectable acutely unlilscleroticOl1eOl.LS
bone casting developl.
MRI : the I)I t l"\lli(ll) of diK material into the VB i.
easily appNlciated on IBgit181 images . It hal been
suggested ,n that acute (symptomatk) lesion. may .ppur
d ifferentieted from chronic (uymptomatic) Ielion. by the
presence of MRI f,"ding. of inflammation in the bone
I1)IIr!"(lW immedi.tely lI,fTounding the Mde .. outlined in
Toble 14·12.
Treatment
Tlbl,1 4· 12 MRI ,lg NlIInlenllty In Schmorl '. nod" '
...""
-
"WI "WI
..-.."
I- I
'"....1 ....
..,
(dllO'IIcl
... _
.......... _
Conserv.tive trNlment i. indicated, Ulu.lly con·
listing of non·ste roida l anti.inflamnuotory drop
(NSA IDsJ. Ooca.ionally Itl"Onger pain med ication and/or lurn"r bncing may be ....•
quired. Surg~ is rarely indicated.
Outcome
With cooservative treatment, symptoms generally rellOl ... within 3 .... month. of on·
set {as "'ith m.o. t ,·e.l"tebral body fractural.
JUJ(1"AFACET CYSTS OF THE LUM8AR SPINE
The 1.ennjuxtafaoetcy.t (JFC) "'as originated by Kao et al."" and includes both
aynovia l cy.~ (th ... having a .ynoviallioing membr.ne)and gaoglio o ey st e (thole
lacking Iynoviallining) adjaunt to • • pin.1 facet joint Or .rising from the ligamentum
fllvum. Oi.tinction between these two types of C)'It.I may be difficult {.su bflow l and ;.
cl iniell\y unimportant It.
JYC Ottu r primarily ill the lumbe r lpine (although cyIt.1 in the cemea!''''''' and
thoracic'" Ipine have beeo t\e.uibed). They w.. re firat reported in 1880 by von Cruker
durin,.n autopsy''', and were lirat di.gDOHd clinically in 1968". The et;olo(O' is un·
known { po. .ibilitie. include: .ynovi.1 fluid .... tl"\ll ion from the joint capsule. latent
fTOwth of. developme:lt.al nit, myxoid degeneration and CY'~ formation in collagenous
connective ti..ue ... ), lncreaaed motion seem. to have a role in ma ny c)'IIta, and the role
of t.nums in the pat.ho!lenesis il debated'" ,. but probably piaYI a !"(lIe ill a .mall n um·
ba, (. 14'ii1o) .... JYC are .... I.tively rare , only 3 t.ses were iden:ified in a ... riel of 1,500
s pina l CT U&II\II'., but the frequency ordi'gROIis may be on th .. rioe d ue to the wide·
.pn.d ute of MRI ."d.n lnc ...... in' aw.nne .. (If the condition.
C linica l
The average .~ .... 6:1 yeara In one .erie. '" and 58 yura in a I"Ilview of54 casl!; n
the Iite,.ture" (range: 33·87) with. sUght fem.le pnponderllnce in both .., rin. Mo.r;t
NEUROSURGERY
14. Spine and Ipi091 cord
oocur in pati~nta with severe spondylGtil lind fllcetjointdegeneTlltion 1to, 25" had degen.
erat ive spondyloll. Lhe.ia' .... 1A-5 i. the mooIt coml11on Ihe]'''' ''', Th ey mol' be bilattra l.
Pain;' the roost COmmOn Iymptom , a nd i, ... ually radicular. Some ,IFe may contribute
I.ocanal l tenOli.and can produce neurogenic d.udiclltion'" (Ju p~326)or on
oca~io n
.cauda equi.oa .ymirome. S)'Jll pl.olTUl may be man interm itte nt in natu l'iO than with firm
Inion •• ",ell .. HLO. A , ,,dden exace rbation In p8in mllY be due to !lemo ...
Th. within the cyst. Some J FC m'1 be • • ympl4matie'''.
Differen tial dia(f1lo.il (llllOlIM Difftrfnlia/ dilllll1o,i•• Sda,;eQ on page 905). Oif.
ferentilltingJFC frolll other m..... rt lie. Ill1Ielyon the IIppell TanC<l lnd loca ti on. Other
diatinguialling futu ... include:
L neurolibroro.: unlikely 1.0 be ulcili.d
2 . fTH fragment of HLD: nol CYltiC in ' .. pe'TIIOte
3. e pidW"1lI or nerve root metllitalel: not cYltic
• . d ... Nl I .... bIor..clu>oid r"OI>t . 1..... dilatation : """ Sp,nlJ/ mfn'tIjJf"ll/ cy.If, page 3.8
b. I ..chnoid cyit (from 8llchnoid he rniation through. d ... NlI defect); notauoci.ted
with feat joint. ma!"(inl thinner th an JFC'"
6. perineurill cysta (Tl rlov'l cflt): .rite in l pace between perineurium and endane ... ri ... m....,ulllyon ucrll roou' •. a«al;onllly &how delayed filling on myelog·
ra phy
comp~ssive
PatbololY
Cyst walla are compased Gf fibfO\.l' cono~tiva ti.,ue of varying thiekn..... and ceHu·
lari ty. There is \l5ulHy no aigtll ori nCection or inflammation. There lIIay be a synovial
lining'. (sync,...al (flt) 0 . it (I"IIY be Iblent'" (ganglion cflt). The distinction between the
two me.y be dil'rlC:,,]t ''", pouiblyowingin part to the flct thst fibmblllJltJ in ganglion cYIU
mly fonn In incomplete ')'1IO"ill.like lining'·. Prol,ferltion of .maU .. en ... les is lee n in
!.he eonneclive liMue. He~iderin Itl ining may be p ~e llt. and lJIay Or may not be as·
toci.ted with a history oft •• " ml'''.
Evaluation
Id enlifyingl J FC pN>oOp helps the . ...rreon, I' the approach differs slightly from
that for HLD, end !.he qat mi~t otherwise be missed 0 ' ... n kn .... ingly deflated and un·
nKelaery time wuted afterwards t.r)'iDg to find I oompreuive lesion. 0,.. the unwitting
may mi sinterpret the cyst as a "tran5(\" ••1 disc extrusion" Il"d needll!tily open
the d ...... ~pdi"",_ were ;nrolTe<:t in 3(W. of operated cases ofJFC'"'.
Myelogrlpby: po$temla teral filJ;ngdef""t (whereu (IIOIIt d~ are , it ... ate<! an te·
riorly, an ooeasion.1 fragment may mignlte poetemlaterally, where8ll a JFC will always
be ~terolate..1), often with a ro ... nd ext ..du.alapP"arante.
cr .can.: I hows a low denlity epidu ral cys~ lesion typiClUy with a posterolate ral
jUlltaarticullr locat ion. SnIDe have calcifoed riUl '"'. I nd lOme m.y have gas within'''. Erosion of bony l.mina is ~asiona lly ~n '"'. ,-.
MRI: variable findings (l":UIy be d"e todiffering compnsition ofcyu fluid: serous vs.
proteinaceous'''"). Unenh. nced sipal ch.racterist ics of non·hemorrhaglc JFC.re very
I;mi llr toCSF. H\!Ulorrhagic: JFC are hyperintense. May be missed ( n aa,gittal imaging
without contrlL!lll Axial images may bette r d~mOllltrlteJFC. Gtdoli " l ... m enh811Ol!ment
in<nases the seMitiv'ty'"". MRI usua lly mi ..... bony erosiDo.
."'f"K1!OlI
Treatment
OptiUl. 1 treatment i, not known. The.. it one ClK report ofa cyJl. thtt "'lOlved
spontaneou.aly' •• lf . ympl.ol1ll persist with conserv.tive trn tment. _
promote CYlt
IL!lIpiration or facet irUection w jth lteroid ....., "'!We mol t Idvocal.e . ... !"(ic.] excision ofth
cYlt
Sw-gical t reatmen t conaideratiOll" The cyst may be .dherent 1.0 !.he dura. The cyst
mBy also coliapH d ... ring the n>~cal appl"Pllch and may be miaaed. A J FC mBy serv, II
B Ula rker for po..ible inl tabil ity and ,hou ld prompt In eulultiDo for the ... ma. Sorne ar·
gue for performi.nl' fu.ion .inee JFC UI.y ar; .. from inltability, however, it 'PPNrs
th.t fUlion i. not required for I cood retult in many ClMI-. ",. ...1( . , it il IU"" ted
that consideralioo for fUlion be mad e on the bIo,i. ofany instability.nd not marely on
the ba.is of the pretence of a JFC .
Sy mptomslic JFC may loter develop contr.loteral to a . u!'(iall,. treated cy.t"'.
F AllED SACK SYNDROME
Th is il ' con diti on where the ... II f.ilure to improve u ti.factorily followilll btoc:k
'"
tA . Spin. and spinal cord
NEUROSURGERY
1Urvery (ror hemiatoed in~rvertebral disc. iarninect.omy for atenOllil .•. ). Thea" pat;en'"
often require analgHiallnd • .., unable toNltum to work . The fai lure rate for lumbar di ....
c;ectomy to provide M tidsctory long_term pain ",Iieri, ~ 8·251b" ' . Pending legal or work·
er'. eompen98tioa claim. we.. the mO$t frequeM dete rrents to a good out.rome"',
r a(ton thllt may CBuM or wntribut4: to th e fa iled back syndrom e:
I. iTlC'O~ initial diagnOlii.
A. inadequate pre-op imagil'l¥
B. dinic.J findi ngs not correlet.ed with abnormaHty demon. t. atoed (In imagi o,
C. othe r ao utea oflymptorlll (Iometim e. in the prelM!:nce orwhat was coDsid·
ered to be an appropriate Inion on imaging . tud i" wh ic h may h.~ been
..ymptomatic): e.g. trochanteric bursitis, diabetic amyotrophy ...
2. continued nerve root or cauda equ ina com p ~ion caused by:
A. f'Midual disc material
B. Teeu,",,,! d isc hemlation at th.tame level: u l ual :)' ha"e pain-free interval
:>
6 ..... post-op (I« ~ 317)
C. disc herniation at another levtl
D. oompreMion or nerve root by perid uralllCar (il'"", lation)tlnue (lfe belowl
E. pseuoorwningooele
F. e pidural hematomll
3.
4.
5.
6.
1.
8.
9.
G. aegmenta l instability: 3 pattem.e-, ) ) latera) >"OU tional in,tability, 2) poIIt.
op . pOndylolil the, il , 3} poIt-<lp twliolil
II. lumb.r .pi""l . ~is
1. in patienr.. operal<!d for ltenoail. recurrenee orstenOllis at the ope ra~
eo:! I...ltl (over mIIny yeara)M
2. devtlopment of ,teno.i. at ao\jaceM level.'"
3. devel09mentof . te ..... i. at levell fu$('(\ in themidline(the hillh rate of
this h• • result.ed in .urgeons,witching to I.teral f\l.llion)
pennanent ~rve root injury from the o riginal disc herniation or from surgery. includes de.fferentation pain "'hkh iI usually con$tant and burning or ice mid
adheaive .... chnoldltl.: responsible for 6·16'JbofpersutentsympCOrn.os in post-op
p8 l ienta" (au below,
disciti.: usu. lly produce8 exquisite back pain 2-4 weeks po!!t-op (1ft page 245)
spondylosis
othe r QuSH of b.a. pain unrelated to the original cond ition; p8rnpin.1 mUlde
'palm, myofawlsyndrome ... Look for trigger points, evidence ofapasm
polIt.-op rena $)VIpathet ic dystrophy (RSD1: I« page 308
- non·an.tomic facton": poor patient motivation, aeoondary gainll, drug addiction.
P5ychologiQI pr¥bleons ... (I n ~luwJdoJ ftu:.IOI"I, page 296)
ARACHNOIDITIS (AKA ADHESIVE ARACHNOIOmS)
InnamlO8tof)' cond ition of the lumbar nerve roots. Mtu.l1y. misnomer, l inee tid·
hesi"e araclmoiditi, is re.l1y an innamm.tory process 01' fibrosis that invol,,".n three
meningea l layers (pill, arachnoid, lind dura). M.ny putat ive "risk f.cton- have been described for the development of arachnoid it;', including>-:
1. spin.l anesthesi$ : eithe r due to the .nathetic agen", to <feUrgent contami·
nanta on the syringes used for same
2. $pinal meningiti " pyogenic, ,yphil itic, t ub...culow
3. neopl asms
4. rtlyelOiTaphic contrast agenr..: less common with currently .v.ilable ",.Ur solu·
ble contr.st .genta
S. tr.um .
A. poIl-s urgic.l ; espeo;i.lly . ner multiple operatioN:
B. utemal tr.uma
6. hemorrhage
7 . id iopathic
,r
Radiographic findings in .rachnoiditi.
NB: RadiOjl'aphic evidence ofa rlchnolditis m.y ,lao be foww:! in umptDm ltk
patitnta-. A.. chnoiditis must be diffel't'nti. ttd from tumor: the oentrtl . dhet.ive type
(.,.., bel/)W ) may rll$f!mbie CSF Heding oftumor, and myelOfnlphic block may mimic in_
tr.th eca l tumor.
Mye logl'IIOl' May demonltrlte completa block, Ol'clu mpi ogofnel'V' roou. On. of m.ny
myel0jl'8phic cI.Mif,cation ' ystam, - for arachnoid ili. i. Jho,!; n in Tabk 14· 13.
MRI, 3 pfItUrllt On Mltl ...· ..:
NEUROSURCERY
14. Spine.n d l pin.lcord
lOS
central adhesion of the nerve roots into
lor 2 central ~C(lrds·
"empty thecal aoc"pattern: roots adhere
to meninges a round periphery, only
CSP . ignal i. visible intl'llthecally
3. thecal sac filled with innammatory tissue, nO CSP signal. Correspond. with
myelographic block end tlndlt·dripping
appearance
Arachnoiditis will usually not enhance
with gadolinium WI much as tumor (In MRL
1.
2.
PERIDURAL SCAR
Table 14-13 Myelographic claasillcalio n 01 anlchnoidil is
-
, Iunilaleral focalDesctl ",Hm
defecl
Typo
,
h~ng
centeled on
lheoeM! root~ a~I\o ~
cncumf&/enlial consIriction aroond !hi.,~
3
•
oompIeIe obstrJCIion with · stalaCI~es·
01 'candle goJn.ring", 'cancle-dripping',
01 "painl-brush' liling cleJeelS
Wllu'ldoboJlaf MOO·sac with loss oJ
A1thougb peridural scar i8 frequently
radicular strialicr1s
blamed for causing recurrent 8ymptoms.... "·,
there hou bee n no proofof corre lation"'. Peri·
dUTIII fibrosis is an inevitable sequelae to lumbar disc Bu rgery. Even pat ients who are reo
lieved of their pain following di$Cectomy develop some sca r tissue post·op'''. Although it
has been shown that if a patient has recurrent redieul ar pain following a lumbar discec·
tomy there is a 70% chance that extensive peridural sca r willllf! found on MRltl'. this
Bt udy also Bhowed !haton post-op MR ls nt6 months, 43% of patients will have extensive
star. but 84% of the time this willllf!~"·. Th us, One must U5e clinicsl
grounds to detennlne if a patient with extensive scar on MR I ia in t..'e 16% mioori ty of
patients with radicula r symptoms a ttributable to sea""".
For a discuuion of mea&urflS to reduce peridu ral scarring, see polJe 307.
RADIOLOGIC EVALUATION
Patien14 with ollly persistent low back or hip pain withou t a strOllg radicu lar com·
ponent, with a neurologic exa m that is Ilor mal Or unchanged from pre-op,should llf! treated symptomatica lly. Patielli.!l with ~ igns or symptoms of recurrent rndiculopathy
(positive SLR is a sensitive test for nerve root compreeaion), especially if these follow a
period of apparent recovery, should undergo fu rther evnluation.
It is critical to d ilTerentiate UlIiduallreclll"re nt disc herniation from scor tissue and
adhesive arachnoidi t iB as surgical t reatment has gellerally poor results with the hitter
t wo (..,.. T~olmel1l o{{ailw back syndrome llf! lowl.
MRI wmlOur AND WITH IV r;ADO/.lNlUM
DiagnostiC ~1".d.tl!kl:. The llf!st exam for detecting residual 01" recurrent dis<: he r·
niation, and to rflliably differentiate dis<: from scar tisaue. P re· contrast studies with
Tl WI and 'l'2WI yields 8J1 accuracy of ~ 83%, comparable to IV enhanced CT'''·tlO. With
the addition of gadolinium, using the protocolllf!low yields 100% sensit ivity. 71% speci·
fidty. e nd 89% accu racy.. •. May also detect adhesive arachnoiditis ~ al><w<!). As scar
becomes rnorfl f,brotic en d ca lcified wi th time, the differential enhan...-ement with respect
to disc material attenuates and lIlay bec:ome undetectableet lOme p<Jint. ~ 1·2 yean post01"" (some scar con tinues to en hance for" 20 ytlIl.
Recomme nded protoco l'"
Get pre..:ootrast Tl WI and T2WI. Give 0.1 mmollkg gadolinium IV . Obtain TIW]
images within 10 minutes (early post..:ontrastl. No benefit from post-<:onlrast T2WI.
Findings On Wl..~ MRI
Signal from a HLD becomes more intense as the sequence is varied from Tl WI T2WI , wbereas !!Car tissue bocomesless intense with this tra nsition. Indirect aigna (also
applicable to CT),
1. mass efTect: a nerve root i8 displaced away fro m disc materi al , whereas it may llf!
ret racted towaroscar tiS-llue by ad here nce to it
2. location: discmateria:l lenda to llf! in contiguity with the disc io lenpace (best8een
on sagittal MRI)
Findings On enhanced, MRI
On tculy ( .. 10 millS pos:.-contrast) TlWI images: scar enhallces iohomogeneously.
wherfl8S dis<: does not enhance at all. A nonen hancing central Drea surrou nded by i~g·
ul ar enhancing material probably represents disc wrapped ill scar. Vellou s plexu s also
'"
14. Spine and spinal cord
NEUROSURGERY
enhWlee.s, and may be mOre pronounced when it is distorted by disc material, but the
mO'l'hology i~ easily differ ential.ed from 3C8r tinue in the8e U!IU,
On /(;.tt (> 30 mi n9 post-contrast) T I W1: scar enhllll<'u homogeneou sly , disc had
variable Or no enhancement. Nonnal nerve roota do not enha nce even on late images.
C T SCAN WITHOUT AND WfTH IV (IODINA TED) CONTRAST
Unenhanced CT scan densi ty measurements are unreliable in the poatoperative
back'''. Enhanced C'T is only fairly good in di fferentiatiogscadenhancingl from disc (unenhancing with po&Sible rim enhancement). -'«uracy is about equal to unenhancd MR J.
MYELOGRAPHY, WITH POST-MYELOGRAPHIC CT
POlItoperatiV<! myelogrnphiccriteria aloneare unreUable for distinguishing disc material fro m 5"a.....·Il• • With t he addition ofCT 3C8n. neural compression is clearly demo
onst rated, but SCar sti ll cannot be reliably diatinguished from disc.
Myelogra phy (especia lly witb post_myelographic CT) is very ca pableofdemonstrating srachnoiditis'" (..... above).
PlAIN LS X-RAYS
Gene rally helpful only iu eases ofi'Ultability, malaHgnm~nt, or sp•.mdyIOllis:" . Flexion/extension views sre most helpful when trying to demonstrate instability.
T REATMENT OF FAILED BACK SYNOROME
For treatment ofinte,..,·ert.ebral disc-a pace infectil)fl, oee Discitis, page 245.
S y mptomatic trea tme nt
Recommended for patients who do not havII radicular $igns and symptoms. or for
m06t patients demonst~ated to have scar tissue or adhesive anochnoiditis on imol,:ing. As
in other case. of non ·~pecific LBP treatment includes: short-term bed rest, analgesics
(non-narcotic in most cases), anti ·inflammatory medication (n(ln-steroidal, and occasion·
ally a short course of steroids), and ph)'!lieal therapy.
S urge ry
Reserved for thOK with recttrrentor re sidua l disc herniation, segmental instability,
or patients with a pseudoroeniogoeele. Patiente with post-op spinal in~tability should be
"<,,,sidered for spinal fusion"" (;we pa.ge 300).
In roostseriM wltb 8uffocient follow·up, $ueress rlttes after reopeTlltion are lower in
patients with only epidural scar (as low as 1%) compared to those patients with disc and
..,af (.till only _ 37%»,'. An overall suec"". rate (> 5~ pain relief for ,,2 y,.,.) of - 34%
was ~Ilfln in one series"', with better results in patients that .... ere young, female, with
good results following previous surgery, a small number of previous operstions. employ·
ment prior to surgery, predominantly radicular (cfaxial) pain , and ab.en"" of sea, reo
quiring lysis.
In addition to the absence ofdi.., mltterial, facto". associated with poor ouw;.mA
were: sensory loss involving more than one dermatome, and patients with past Or pending compensation claims"'· ' ''.
Arachnoiditi s: Surgery forcarefuUy selected patienta with 9T1lehlloiditis {those with
mild .adi<>gra.,hie involvQm ..nl ('T'ypoo~ 1 & 2 in Tobl~ IJ.13 ). and ",-:I previou, back 0p" ' alions)"" haa met with moderate SUC""., (althoud! in t his slIries, nO patient retu rned to
work). Approximate succe$S rate in other Mries''''''': 50% failure, 20% able to wo-rk but
with sy mptoms, 10·19% with no symptomll. Surgery e<:>nsists of removal of ex tradural
scar eoveloping the thecal sac, removi ng any herniated disc fragments, and performing
(oramino1omie. when indkated. Intradural lysis of adhesion. is Jl2l indicated .ince nO
means for preventing reformation of scar h88 bllfln identified"'.
R ECURRENT HERNIATED LUMBAR OISC
RllteS quoted in the literature ra nge from 3-19% with the higher rates usually in sotries with longer follow-u p"'. I" an individual series with 10 year mean FlU, the rate of
rE~current disc herniation was 4% (same level, either side), OM third ofwhkh occu rred
during the 1$t year poat-op (mean' 4.3 yrs)'''. A ~ recurrence a t the same site oc·
curred in 1% in another series'" with mean FlU of 4.5 yrs. In this series"', patients preseoting for a second time with disc herniation had a recurnnoe at the same level in 74%.
NEUROSURGERY
14. S pine and spinsl cord
but 26\110 had a HLD at anothe. level. Recurrent HLO oc:eurred at lA·S more thon twice
as o~n as 1.5·S1....
It i. often poMible for a 1/Illller omount of "",urrent herniated di.~ to UuIN .ymptoms thao in a 'virgin ba<:k". due to the f.el that the nerve root is o~n (juted by K a r
tisaue and ha.liltle ability to deviate . w.y from the fragmeot"".
TREATMENT
Initi.l recommended Ire.Lment;8 at with a first t ime HLO. Nooaurgknl trutment
abould be utilized in the ab$en:e ofprogn..ive neurologic denci t, clude equina Iyn·
dronM (CES) or intractable J)l.in.
Surgical treatment
Disagreement oc:eu rs raprding optimal UlIalment. For re~WTen : HLO without
demonatrsted I pinallnatabiUI}', a 1992 l urvey . howed opinion divided primarily between simple repeat diacectotlly (57\110) v• . rapellt diKectomy with fu.lI;Qn 1 ~ 0\II0) (when in·
l tabllity ia preMnt, m