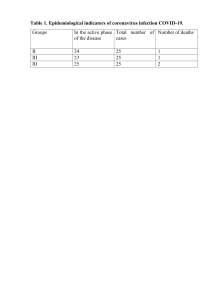
Health risk assessment Lector Associate Professor Ekaterina Shashina According to the WHO, preventive health care is based on collection and analysis information about risk factors Relationship between the environmental factors and health disorders Necessary and sufficient condition The bite of a mad dog rabies (hydrophobia) Necessary but insufficient condition Mycobacteria tuberculosis tuberculosis Unnecessary but sufficient condition benzene leukemia Unnecessary and insufficient condition smoking, fatty and salty foods, physical inactivity, emotional stress myocardial infarction Hygienic diagnostic Environmental monitoring Health surveillance Data analysis, comprehensive assessment, determination of causation. Methods of the hygienic diagnostics: demographic, statistical, clinical, experimental, epidemiological studies, health risk assessment Epidemiological studies Epidemiological studies are aimed, where possible, at revealing unbiased relationships between exposures such as alcohol or smoking, biological agents, stress or chemicals to mortality or morbidity. The identification of causal relationships between these exposures and outcomes is an important aspect of epidemiology. Modern epidemiologists use informatics as a tool. Types of epidemiological studies Experimental studies Observational studies Epidemiological studies • Experimental studies These type of studies consider the effect of different characteristics or exposures that are under the investigator’s control. Investigators can actively influence the exposure conditions and the factors studied as in a toxicological study. Comparable individuals are randomly assigned to a treatment or intervention group and observed for a specific health-related outcome. Experimental epidemiology Three types: • randomized controlled trials (often used for testing new medications), • field trials (carried out on those at a high risk of disease development), • community trials (population studies). Epidemiological studies • Observational studies are designed to further examine known associations or hypothesized relationships. Nature is allowed to “take its course” as epidemiologists observe without interfering in the process. Observational studies Descriptive (ecological, correlation studies) Descriptive observations pertain to the ‘who, what, where and when’ of a healthrelated event. Analytical Analytical observations deal more with the ‘how’ of a health-related event. An ecological study does not link individual outcome events to individual exposure or confounding characteristics, and it does not link individual exposure and confounding characteristics to one another. In an ecological study, information about exposure and disease is available only for groups of people, and critical information can be lost in the process of aggregating these data. The results of ecological studies are difficult to interpret, and serious errors can result when it is assumed that inferences from an ecological analysis pertain either to the individuals within the group or to individuals across the groups. Analytical studies can provide the necessary information to help evaluate the causality of an association and estimate the magnitude of risk. For each person included in the study, information is obtained about their disease status, their exposure to various contaminants characteristics. and confounding Analytical study Cross-sectional study Longitudinal study Cross-sectional study Exposure and disease information relate to the same time period; in these studies, it may not always be correct to presume that exposure preceded disease. These study reflect the state of the groups studied at a given time, so they are often called "sectional studies" or "simultaneous studies." Longitudinal study The time sequence can be inferred between exposure and disease; in other words, exposure precedes disease. The observation of the studied populations is carried out within a certain, sometimes quite a long period of time. Longitudinal (long) study “Case-control” study The investigator identifies individuals having a disease or health outcome of interest and a control or comparison group of individuals without the disease of interest; exposures and risk factors are evaluated in these persons. In a case–control study, a variety of exposures can be studied. Cohort study The cohort study begins with the identification of individuals having an exposure of interest and a nonexposed population for comparison; disease consequences or other healthrelated outcomes are then determined for each group. In a cohort study, a variety of diseases can be studied. Cohort study Prospective study In a prospective study, the case series are followed up over time to evaluate the natural history of disease. The main objective of prospective studies is to reveal the effect of the existing impact with the subsequent analysis of the disease cases. Exposure is now – disease will be in the future. Retrospective study Retrospective studies are aimed at finding the causes of the disease with the subsequent analysis of the impacts that occurred in the past. Disease is now – exposure was in the past. METHODS OF EPIDEMIOLOGICAL STUDIES Analytical Cross-sectional study Descriptive Longitudinal study Cohort study Prospective Case-control study Retrospective Case-control studies select subjects based on their disease status. It is a retrospective study. A group of individuals that are disease-positive (the "case" group) is compared with a group of disease-negative individuals (the "control" group). The control group should ideally include age-, gender-, and constitution-matched individuals. The case-control study looks back through time at potential exposures that both groups (cases and controls) may have encountered. Analysis of the “case-control” study results Disease Exposure Exposed Non-Exposed Odds Ratio 𝒂𝒅 𝑶𝑹 = 𝒃𝒄 >,<, = 1 Diseased (case) Non-Diseased (control) a c b d • If the OR is significantly greater than 1, then the conclusion is "those who have the disease are more likely to have been exposed to analyzed factor," • if it is close to 1, then the exposure and disease are not likely to be associated. • if the OR is far less than 1, then this suggests that the exposure is a protective factor in the causation of the disease. Cohort studies are based on the subject exposure status. The subjects should be at risk of the outcome under investigation at the beginning of the cohort study; this usually means that they should be disease-free when the cohort study starts. The cohort is followed up through time to assess their later outcome status. A cohort study may be exemplified by the study of the cohorts of smokers and non-smokers over time to estimate the incidence of lung cancer in each cohort. Analysis of the cohort study results Disease Diseased NonDiseased a c b d Exposure Exposed Non-Exposed RR = RR may be > 1, < 1 or = 1 Relative Risk (RR) RR = 𝒂/(𝒂+𝒃) 𝒄/(𝒄+𝒅) RR greater than 1 means "those who are exposed to the factor are more likely to develop analyzed disease" Relative risk (RR) - the ratio between the frequency of disease among people exposed and the least exposed. Relative risk reflects the likelihood of more frequent occurrence of the disease as a result of exposure to environmental factors. Analysis of the cohort study results Attributive Risk (AR) 𝒂 𝒄 𝑨𝑹= − ×𝟏𝟎𝟎 𝒂+𝒃 𝒄+𝒅 RR = • AR is measured as percentage (%) • Example, AR = 80%. This environmental factor contributes 80% to the disease. Other factors account for 20%. • 80% of the diseases is associated with exposure to the environmental factors. Attributive risk (AR) shows the share of ecological risk – how much the environmental factor attributes to the disease development. Prospective studies have many benefits over case-control studies. The RR is a more powerful effect measure than the OR, as the OR is just an estimation of the RR, since true incidence cannot be calculated in a case control study where subjects are selected based on disease status. Temporality can be established in a prospective study, and confounders are more easily controlled for. However, they are more costly, and there is a greater chance of losing subjects to follow-up based on the long time period over which the cohort is observed. Risk is the expected frequency of undesirable effects arising from a given exposure to a pollutant. Risk assessment is the use of the factual database to define the health effects of exposure of individuals or populations to hazardous materials and situations. Steps of risk assessment Hazard Идентификация identification опасности Оценка Exposure зависимости assessment «дозаответ» DoseОценка response зависимости relationship «доза-ответ» Risk Risk characterization characterization Steps of risk assessment: 1. Hazard identification 2. Exposure assessment 3. Dose-response assessment 4. Risk characterization Objectives: • Emission inventory • To identify hazardous pollutants • To identify health effects • To assess the reliability of the exposure level data • To evaluate the reiability of criteria for quantitative risk assessment Goal: to determine the risk assessment area Steps of risk assessment: Soil 1. Hazard identification Air 2. Exposure assessment 3. Dose-response assessment Foods 4. Risk characterization Objectives: • To collect information about the exposure parameters; • To determine the exposure pathway and exposure scenarios Goal: to determine the exposure doses Water Exposure pathway Emission source Input medium Transport medium Exposure medium Routes of exposure Exposure point Exposure pathway Emission source Exposure scenario Environmental medium Exposure routes inhalation oral dermal Atmospheric air + - - Tap water + + Soil + + + Surface water + Ground water Food + +* + + + + + - + - Note: *Fish consumption and/or ingestion of water during swimming Exposure scenarios Industrial Exposed populations Workers Residential Children Recreation Adults Agricultural Exposure scenarios Industrial Exposed populations Adults Residential Children Recreation Workers Agricultural Exposure assessment Direct method Individual monitoring Indirect method Calculation of potential doses for exposed population Biological markers Biological marker of exposure The level of the chemical substance or its metabolite in blood (urine, hair, nails, etc.) Biological marker of sensitivity Characteristic of the body ability to react to environmental factors Biological marker of effect Quantitative assessment of the degree of bodily changes determined by health impairment Examples of exposure markers Chemical CO Pb Spirits Biological marker Blood concentration of HbCO Blood concentration of Pb Ethanol concentration in the expired air Volatile organic VOC concentration in the expired chemical (VOC) air Drug The blood concentration of drug or the urine concentration of its metabolite Cigarette smoke Cotinine concentration in the urine Pentachlorophenol PCP concentration in the urine (PCP) Examples of marker of sensitivity Exposure to plant pollen Eosinophil concentration Examples of effect markers Exposure to fluoride Number of mottled teeth (marked with spots or smears of color) Exposure to lead Blue line - change of gum color; lead colic - like abdominal pains; face color becomes iron-grey Exposure to cadmium Spinal pain and leg pain, waddle gait due to bone deformities Estimate of daily contamination dose CDI = [C x IR x ED x EF] / [BW x AT x 365] CDI Chronic daily intake, mg/kg-day C The medium concentration of chemical: water (mg/L), air (mg/m3), soil, food (mg/kg) IR Intake rate of contaminated medium (L/day, m3/day) ED Exposure duration, years EF Exposure frequency, days per year AT Averaging time, years BW Body weight, kg 365 Number of days in a year Chemical concentration at the exposure point Population characteristics (body weight, age, etc.) Environmental monitoring Air dispersion and deposition modeling is the calculation of the chemical concentration in the human respiration zone using emission volumes, emission temperatures, the stack height, wind velocity and direction, etc. Sampling and laboratory analysis Sociological questionnaire data Default values Estimation of chronic daily intake (dose) Exposure Exposure route Inhalation Oral Dermal Σ Ambient air CDIai - - ΣCDIa Soil CDIsi CDIso CDIsd ΣCDIs Tap water CDItwi CDItwo CDItwd ΣCDItw Surface water CDIswi CDIswo CDIswd ΣCDIsw Ground water CDIgwi CDIgwo CDIgwd ΣCDIgw - CDIfo - CDIf ΣCDIi ΣCDIo ΣCDId TCDI medium Food Σ Steps of risk assessment: Response 1. Hazard identification 2. Exposure assessment 3. Dose-response assessment 4. Risk characterization Dose Objective: To determine the relationship between the magnitude of exposure and the likelihood of health effects Goal: to determine the maximum acceptable level Dose-response relationship for non-carcinogens (toxic chemicals) Response Dose Dose-response relationship for carcinogens Response . Dose Dose-response relationship for essential substances Response Optimum zone Dose Fluorides effects Fluorides is ingested predominantly with drinking water Effect on the body caries 0,5 Fluorosis 0,7 1,0 1,5 2,0 6,0 Concentration in water, mg/L Reference dose (RfD) Response RfD is an estimate (with uncertainty) of a daily exposure of the human population (including susceptible subgroups) likely not to be at an appreciable risk of deleterious effects during their lifetime. Acceptable level Dose NOAEL - No Observed Adverse Effect Level LOAEL - Lowest Observed Adverse Effect Level RfD = NOAEL/(UF x MF) Uncertainty factors (UF): • intrahuman variability • experimental animal-to-human extrapolation • subchronic-to-chronic extrapolation • LOAEL-to-NOAEL extrapolation • database completeness Modifying factors (MF) take into account the uncertainty areas not mentioned above. Dose-response curve for carcinogens Response SF Dose . The slope factor (SF) is a slope of the dose-response curve for a certain carcinogen. The more dangerous the carcinogen, the higher the SF value. Sources of the toxicological and dose-response data 1. 2. 3. 4. 5. 6. 7. 8. U.S. EPA IRIS electronic database. HEAST table sheet. ATSDR reports. WHO publications. The results of risk assessment used by the EPA to determine the Federal standards of the atmospheric air quality. The results of epidemiological studies. Toxicological profile of chemicals. The results of Russian toxicological studies. Steps of risk assessment: 1. Hazard identification 2. Exposure assessment 3. Dose-response assessment 4. Risk characterization Objectives: • To calculate the risk (hazard index) for each exposure route risk for each exposure medium risk for the whole scenario of one chemical risks for many chemicals • To compare the risks for many chemicals risks for many sources Goal: which one poses the greatest risk? Risk of non-carcinogenic (toxic) effects Hazard index HQ = CDI/RfD HI = HQ THI = HI • Increased risk is expressed as an increased HI. • If the HI or HQ value is less than 1.0, there is no hazard of toxic effects. HI – Hazard Index, HQ – Hazard Quotient, THI – Total Hazard Index Oral exposure HQо = СDIo/RfDо СDIo – chronic daily oral intake (mg/kg·day) RfDo – reference dose (mg/kg) Inhalation exposure HQi = Ci/RfC Ci –air concentration (mg/m3) RfC – reference concentration (mg/m3) Risk of noncancerogenic effects Exposure Exposure route Inhalation Oral Dermal Σ Ambient air HQai - - HIa Soil HQsi HQso HQsd HIs Tap water HQtwi HQtwo HQtwd HItw Surface water HQswi HQswo HQswd HIsw Ground water HQgwi HQgwo HQgwd HIgw - HQfo - HIf HIi HIo HId THI medium Food Σ Risk of carcinogenic effects ICR = LADD · SF ICR – individual cancer risk LADD - Lifetime Average Daily Dose in mg/kg-day LADD is the dose received over 70 years of lifetime SF – Slope Factor • Risk is the likelihood that an individual with lifetime exposure may develop cancer. “Acceptable” risk is defined as a risk which is no greater than 1·10-6 (1 cancer case per 1 million) Risk of cancerogenic effects Exposure Exposure route Inhalation Oral Dermal Σ Ambient air ICRai - - ΣICRa Soil ICRsi ICRso ICRsd ΣICRs Tap water ICRwi ICRtwo ICRtwd ΣICRtw Surface water ICRswi ICRswo ICRswd ΣICRsw Ground water ICRgwi ICRgwo ICRgwd ΣICRgw - ICRfo - ΣICRf ΣICRi ΣICRo ΣICRd ICRt medium Food Σ Risk analysis Risk assessment Risk management Risk information Bradford Hill criteria to establish a causal relationship between the exposure factor and the effect (disease) ❖ ❖ ❖ ❖ ❖ ❖ ❖ ❖ ❖ Temporal relationship Statictic strength of the relation Dose-Response relationship Reversibility Consistency Plausibility Consideration of Alternate Explanations Specificity of the relation Coherence 1. Temporal Relationship Exposure always precedes the outcome. If factor A is believed to cause a disease, then it is clear that factor A must always precede the occurrence of the disease. This is the only absolutely essential criterion. 2. Strength This is defined by the size of the association as measured by appropriate statistical tests (OR, RR, AR, HI values). The stronger the association, the more likely it is that the relation of "A" to "B" is causal. For example, the more highly correlated hypertension is with a high-sodium diet, the stronger is the relation between sodium and hypertension. 3. Dose-Response Relationship An increasing amount of exposure increases the risk. If a dose-response relationship is present, it is strong evidence for a causal relationship. A threshold may exist above which a relationship may develop. 4. Reversibility (effectiveness of adjusting measures) At the same time, if a specific factor is the cause of a disease, the incidence of the disease will decline when exposure to the factor is reduced or eliminated. The analogy can be applied to global temperatures. If increasing atmospheric CO2 levels cause an increase in global temperatures, then "other things being equal", we should see both a commensurate increase and a commensurate decrease in global temperatures following a respective increase or decrease in CO2 levels in the atmosphere. 5. Consistency The association is consistent when results are replicated in studies in different settings using different methods. In other words, if a relationship is causal, we would expect to find it consistently in different studies and among different populations. For example, it required thousands of highly technical studies of the relationship between cigarette smoking and cancer before a definitive conclusion could be made that cigarette smoking increases the risk of (but does not cause) cancer. 6. Plausibility The association agrees with currently accepted understanding of pathological processes. In other words, there needs to be some theoretical basis for positing an association between a vector and disease, or one social phenomenon and another. 7. Consideration of Alternative Explanations In judging whether a reported association is causal, it is necessary to determine the extent to which researchers have taken other possible explanations into account and have effectively ruled out such alternative explanations. In other words, it is always necessary to consider multiple hypotheses before making conclusions about the causal relationship between any two items under investigation. 8. Specificity This is established when a single putative cause produces a specific effect. This is considered by some to be the weakest of all the criteria. The diseases attributed to cigarette smoking, for example, do not meet this criterion. When specificity of an association is found, it provides additional support for a causal relationship. However, the absence of specificity in no way negates a causal relationship. Because outcomes (be they the spread of a disease, the incidence of a specific human social behavior or changes in global temperature) are likely to have multiple factors influencing them, it is highly unlikely that we will find a one-to-one cause-effect relationship between two phenomena. Causality is most often multiple. Therefore, it is necessary to examine specific causal relationships within a larger systemic perspective. 9. Coherence The association should be compatible with existing theory and knowledge. To put it differently, it is necessary to evaluate claims of causality within the context of the current state of knowledge in a given field and in related fields.