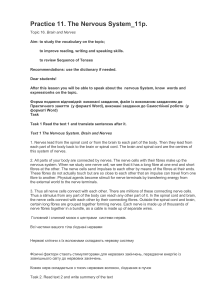
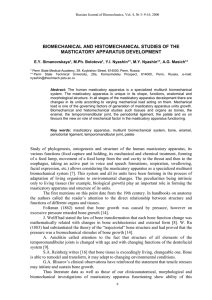
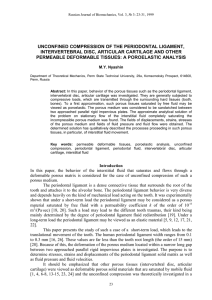
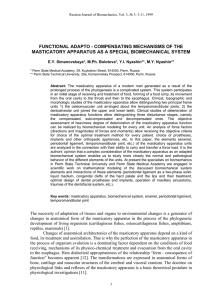
Diaphragm • • • • • • • Double-domed (right and left) Musculo-tendinous partition Convex superiorly Chief muscle of inspiration Central portion descends during inspiration Normally, right dome is higher (b/c of liver) During expiration, right Dome rises up to 5th rib and left dome up to 5th ICS • Level varies acc to: – Phase of respiration – Posture – (lowest when sitting) – Size and degree of distension of abdominal viscera Structure Origin • Muscular part peripherally • Fibres converge on the trifoliate shaped Central Tendon (aponeurotic part) – lies beneath pericardium and is fused with it • Muscular part is divided into: – Sternal part • 2 slips • posterior aspect of xiphoid process – Costal part • Wide slips • Internal surfaces of inferior 6 costal cartilages and their adjoining ribs, interdigitating with transversus abdominis muscle – Lumbar part • Arises from 2 aponeurotic arches ie Medial and Lateral Arcuate Ligaments; and L1,L2,L3 • This part forms the right and left crura (singular crus) • • • • • Crura: Musculotendinous bands Right one is larger and longer (L1-L3/4) Left crus (L1-L2/3) The tendinous arch between the medial aspects of the two crura is called: Median Arcuate Ligament • • • • • • Medial arcuate ligament/ Medial Lumbocostal Arch Thickening of fascia covering psoas major From side of body of L1 to tips of transverse process of L1 Lateral arcuate ligament/ Lateral Lumbocostal Arch From tip of transverse process of L1 to lower border 12th rib Covers Quadratus Lumborum muscles Openings in diaphragm • Aortic hiatus(lower border T12): (Osseoaponeurotic) b/w crura, posterior to the median arcuate lig. – Aorta – Thoracic duct – Azygous vein • Esophageal (T10): I 8 = IVC at T8. 10 EGGs = EsophaGus and vaGus at T10. AAT 12 = Aorta, Azygos, and Thoracic duct at T12 I ate, 10 Eggs, At 12 (in right crus) – esophagus – Vagus nerves – esophageal branches of Left Gastric artery+ accompanying veins • Caval opening (T8): (Central tendon – to the right of midline) – IVC – Branches of Rt. Phrenic Nerve Small openings Opening in Structure that passes R+L crura Greater and Lesser Splanchnic Nerves L crus Hemiazygous vein Behind medial arcuate ligament Sympathetic chain +least splanchnic nerves Behind Lateral arcuate ligament Subcostal nerves & vessels Gap b/w xyphoid & costal origin of diaphragm Larry’s space/foramen of Morgagni Superior epigastric vessels and lymphatics from diaphragmatic surface of liver At level of 9th Costal cartilage Musculophrenic vessels pierce Central tendon pierced by small veins • Lymphatics – on superior surface: anterior and posterior diaphragmatic nodes parasternal, posterior mediastinal and phrenic nodes • Inferior surface: lymphatics anterior diaphragmatic, phrenic and superior lumbar nodes Actions • Role in Respiration: On contraction vertical dia of thorax ↑ volume of thorax↑, intrathoracic pressure↓ Air pulled into lungs • Role in Circulation: ↑intraabdominal pressure and ↓intrathoracic pressure venous return to the heart via IVC↑ • Fibres of Rt. Crus decussate, forming a sphincter for the esophagus that constricts it when the diaphragm contracts Clinicals • Hiccups – involuntary, spasmodic, contractions of diaphragm • Irritation of afferent or efferent nerve endings, or medullary centre in brain. • Other causes: alcoholism, diaphragm irritation, indigestion, cerebral lesion, thoracic or abdominal lesions clinicals • Section of Phrenic nerve in the neck: • Complete paralysis and later atrophy of the corresponding half • Paradoxical movement seen. Permanent elevation, even during inspiration Clinicals • Referred pain • To shoulder region (the skin in that area is supplied by C3-C5) –supraclavicular nerves • Irritation of peripheral region more localized (intercostal nerves) Clinicals • Rupture of diaphragm after trauma. Sudden pressure changes (95% of the time on left side, as liver provides barrier on right side) • Herniation of abdominal organs into the thoracic cavity HERNIA CONGENITAL RETROSTERNAL POSTEROLATERAL* POSTERIOR ACQUIRED CENTRAL TRAUMATIC HIATAL Clinicals • Lumbocostal traingle is a nonmuscular area. • When traumatic hernia occurs, the stomach, small intestine, transverse colon and spleen may herniate through this into thorax • Congenital Diaphragmatic Hernia (CDH) • Large posterolateral defect (foramen of Bochdalek) • Almost always on the left • Cavity occupied by abdominal viscera, one lung does not have room to develop normally pulmonary hypoplasia • Hiatal hernia – protrusion of part of stomach into thorax. The other structures passing through it can get injured when surgical correction is being done. 2 TYPES : ROLLING AND SLIDING A: Sliding commonest B: Rolling- junction intact