Circulating-microRNAs-as-biomarkers-for-depression-- 2018 Journal-of-Affecti
реклама

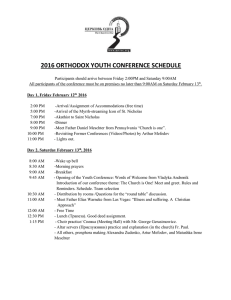
Journal of Affective Disorders 233 (2018) 68–78 Contents lists available at ScienceDirect Journal of Affective Disorders journal homepage: www.elsevier.com/locate/jad Review article Circulating microRNAs as biomarkers for depression: Many candidates, few finalists Heidi Yuana,c, David Mischoulonb, Maurizio Favab, Michael W. Ottoa, a b c T ⁎ Department of Psychological and Brain Sciences, Boston University, United States Depression Clinical and Research Program, Massachusetts General Hospital and Harvard Medical School, United States Pomona College, Claremont, CA, United States A R T I C L E I N F O A B S T R A C T Keywords: MicroRNA Depression Biomarker Plasma Serum Circulating Background: Recent research has highlighted the potential of microRNAs to serve as physiological indicators of disease process among clinically depressed patients. Methods: In a comprehensive literature search through PubMed, we identified 23 articles comparing circulating (blood, plasma, or serum) microRNA expression levels in depressed versus healthy human subjects. Six studies examining circulatory microRNA expression through animal models of depression were also identified through the search and details of each study were outlined. A meta-analytic evaluation of these studies was not considered feasible, given the absence of concordance in the literature to date. Results: A total of 178 specific microRNA candidates were identified in the human studies as significantly expressed among depressed samples. Ninety-seven of these microRNAs were upregulated, 75 were downregulated, and 6 showed mixed expression in depressed samples. Few microRNAs were consistently expressed across studies; the most consistent evidence was for microRNA-132, with replication in 4 different studies. Among animal studies, 2 studies investigated microRNA-16 through distinct stress-induced depression models. Limitations: Structural variations in microRNA sequences, methodological inconsistencies in technology used among studies to measure microRNA expression levels, differences in the clinical severity and forms of depression among subjects, and the overall paucity of studies make it difficult to ascertain any robust, preliminary targets deserving of biomarker potential. Conclusions: Ongoing research needs to address this high rate of non-replication as well as the methodological and reporting challenges of microRNA experimentation in order to determine valid effect sizes for the more proliferative candidates associated with depression. 1. Introduction There is a clear need to understand more about the underlying biology of depressive disorders and how antidepressants exert their biological effects that translate into improvement in mood. Although the treatment of depression has progressed a great deal since the emergence of the first antidepressants in the 1950s, there are still many limitations to current therapies. As it stands, only about half of individuals with depressive disorders respond to FDA-approved antidepressants (Undurraga and Baldessarini, 2012). Among those who respond, many will eventually relapse (Forte et al., 2015). More aggressive therapies such as ECT or ketamine often work faster and better, but their effects tend to be short-lived. Recurrence rates following a course of ECT, even with continuation therapy, are high (almost 40%) within the first 6 months post-treatment, particularly without ⁎ prophylactic antidepressant administration (Jelovac et al., 2013). The beneficial effects of single ketamine administrations can also wear off quickly, sometimes within hours or days, and thus require frequent intravenous or intranasal infusions to sustain the effect (Schwartz et al., 2016), which may be inconvenient for some patients. In addition, these therapies carry particular risks that may make them undesirable for many depressed patients (Andrade et al., 2016; Li and Vlisides, 2016). The treatment of depression is largely a trial-and-error process, with no consistent evidence to suggest that any one treatment is better than another for a specific patient presenting with depression (Kato, 2012). The search for feasible physiological indicators to characterize depression has been a longstanding endeavor. One result of this need has been the search for biomarkers of depression. Stable biomarkers such as genetic variations or polymorphisms may provide information about risk or type of depression. Other biomarkers that emerge or change over Correspondence to: 648 Beacon St., Floor 6., Boston, MA 02215, United States. E-mail address: [email protected] (M.W. Otto). http://dx.doi.org/10.1016/j.jad.2017.06.058 Received 26 December 2016; Received in revised form 14 March 2017; Accepted 26 June 2017 Available online 27 June 2017 0165-0327/ © 2017 Elsevier B.V. All rights reserved. Journal of Affective Disorders 233 (2018) 68–78 H. Yuan et al. such as heart disease, sepsis, and stroke (Ai et al., 2010; Wang et al., 2010; Tan et al., 2009). The goal of using microRNAs to distinguish patients with psychiatric disorders from healthy populations is also becoming more prevalent. A number of animal, human, and bioinformatic studies have demonstrated the potential of microRNA levels to aid in the diagnosis of various psychiatric diseases (Issler and Chen, 2015). Growing evidence continues to highlight the regulatory role of microRNAs in schizophrenia (Schizophrenia Psychiatric Genome-Wide Association Study (GWAS) Consortium, 2011), bipolar disorder, autism, and major depressive disorder (Geaghan and Cairns, 2015). Regulation by microRNAs of CREB/BDNF pathways that affect neural and synaptic plasticity has been suggested as one mechanism by which microRNAs contribute to depressive and suicidal behavior or affect (Serafini et al., 2014). Expression of specific microRNA candidates and their target proteins or signaling pathways has been examined in various brain regions of stress-induced animal models and in post-mortem brain tissue of depressed suicide patients. Indirect mechanisms by which microRNAs modulate depression and suicidal behavior include CREB phosphorylation, BDNF expression, 5-HT cascades, tropomyosin receptor kinase B (TrkB-T1) expression, repressor element-1 silencing transcription factor 4 (REST4) activity, transcription factors such as NOVA1 involved in synaptic plasticity and neurotransmitter release, and glucocorticoid receptor (GR) expression (Serafini et al., 2014). It is evident that microRNAs are fundamentally involved in the intracellular signaling and developmental timing of neurons and other cells associated with depression. In spite of this, little progress has been made to uncover the mechanisms and systems of circulating microRNAs. Consistent with the goal of identifying novel biomarkers of depression, initial research used animal models to identify changes in microRNA levels associated with behavioral paradigms of depression (Smalheiser et al., 2011) or efficacy of antidepressant treatments (Baudry et al., 2010; Smalheiser et al., 2014; O'Connor et al., 2013). An additional body of work has been devoted to elucidating human microRNA expression levels in depressed subjects relative to healthy controls. With the intention to conduct a meta-analysis of the findings in this area, we performed a literature search on studies evaluating microRNA expression levels found exclusively in human blood, serum, or plasma samples, which would render them relatively accessible biomarkers of depression. Examination of the published literature, however, revealed a notable absence of concordance among microRNA candidates. Accordingly, rather than conducting a meta-analysis of promising candidate(s), this report provides a qualitative summary of the current state of knowledge in this new area of study, taking into account both human studies as well as the animal models used to examine depression-related microRNA alterations. time with treatment (e.g. immune markers) may help determine the effectiveness of selected treatment, allowing clinicians to make earlier decisions about whether to continue or alter the treatment plan (Leuchter et al., 2010; Papakostas et al., 2013). Markers that emerge early in treatment are the most desired ones for this reason (Leuchter et al., 2010). Because biomarkers can potentially identify the underlying mechanism of a particular depressive disorder, they can also guide the selection of a specific treatment to better match the biology of the patient's condition (Bartova et al., 2010). For example, if it were determined that a particular depressive disorder results from increased inflammatory activity, an anti-inflammatory drug could potentially be selected as a first line of treatment, in hopes of obtaining the desired response and bypassing unnecessary and ineffective trials of other medications. A number of biomarker candidates have emerged as promising diagnostic tools for major depressive disorder. These candidates include cytokines and inflammatory markers, HPA-axis hyperactivity (via cortisol levels), neurotrophins, oxidative stress markers, thyroid function, and other genetic or genomic markers (Young et al., 2016). However, given the absence of consistent results and the paucity of replicated studies, it has been difficult to distinguish particularly noteworthy candidates as comprehensive indicators of the disease (Young et al., 2016). Evidence to suggest a genetic basis of depression is growing, and with the advent of proteomic and genomic profiling technologies comes the preference to discover genetic biomarkers involved in the pathology of depression. MicroRNAs are small, endogenously-expressed, non-coding RNA transcripts, approximately 22 nucleotides in length, with unique sequences targeting mRNAs for translational repression or destabilization. By binding to the 3’ untranslated region (UTR) of their target mRNA, microRNAs reduce the overall output of associated proteins, and are thereby crucial to a number of cell signaling, differentiation, and proliferation processes (Bartel, 2004). Circulating microRNAs are of particular interest due to their ease of access and their stability in samples obtained from body fluids (Chen et al., 2008; Mráz et al., 2009). Stability of these molecules is afforded in large part by the packaging through which they exert their functionality. MicroRNAs in circulation exist in high-density lipoproteins (Vickers et al., 2011) and exosomes (Hu et al., 2012) that protect and prevent them from degradation before they are released to target cells (Montecalvo et al., 2012). The machinery of these packaging molecules is important in understanding the functionality of microRNAs - some models have been proposed and investigated to explain the mechanism for microRNA secretion. Among these is a ceramide-dependent exosomal release pathway (Kosaka et al., 2010), plasma microvesicle transfer (Valadi et al., 2007; Hunter et al., 2008), and for immune cells, antigen-driven unidirectional exosomal transfer (Mittelbrunn et al., 2011). Interestingly, the majority of microRNAs found among humans are not exclusively expressed in a single tissue. In fact, a range of highly-abundant microRNAs were found to be ubiquitously expressed in multiple human tissues, demonstrating the low cell-type specificity of these regulatory molecules (Landgraf et al., 2007). This further highlights the power of microRNAs in circulating biofluids as influential moderators of various physiological systems and processes. Circulatory microRNAs have served as useful physiological indicators of disease states (Reid et al., 2011). The first study published linking cancer with circulating microRNAs examined the microRNA expression profile in the serum of patients with large B cell lymphoma, and found a set of microRNAs to be significantly upregulated in cancerous patients (Lawrie et al., 2008). Following this discovery, a number of additional studies emerged that characterized the microRNA expression profile of patients with varying cancers, including prostate, lung, colorectal, ovarian, pancreatic and breast cancer (Mitchell et al., 2008; Hu et al., 2010; Ng et al., 2009; Resnick et al., 2009; Wang et al., 2009; Heneghan et al., 2010). In addition, alterations in microRNA expression profiles were shown to be implicated in other conditions 2. Method For our literature search of the PubMed database through December 17, 2016, we used the Boolean term (((microRNA or miR or miRNA)) AND depress*) AND (blood OR serum OR plasma), to include any articles with the search terms “microRNA,” “miRNA,” or “miR”; “depress,” “depressed,” or “depression”; and “blood,” “serum,” or “plasma.” The term “depress*” was used instead of specifying “major depressive disorder” or any of its derivatives to include all articles examining microRNAs in relation to any form of depression. This search yielded 126 articles. The bibliographies of 7 reviews produced from this search (Dwivedi, 2013, 2014; Dwivedi, 2015; Rucker and McGuffin, 2014; Kichukova et al., 2016; Vijayan and Reddy, 2016; Eyre et al., 2015) were consulted and 26 additional studies perceived as relevant by title or citation context were added to the list of articles. Human studies were included if they met the following inclusion criteria: examined microRNA expression levels, microRNAs obtained from circulating biofluid such as plasma or serum, and included depressed human subjects and control group. Animal studies were included if they met 69 70 PSD 3 18 32 8 63 20 32 40 18 36 30 6 169 34 5 40 3 11 16 32 50 10 16 Depressed patients sample size 3 17 32 9 73 20 30 20 18 30 30 6 52 20 5 40 3 11 14 18 41 10 13 Healthy patients sample size N N N N N N Y Y Y N N N Y N Y N N Y N Y N Y Y Treatment Response Examined Y Y Y Y Y N – – – – Y N SNRI, SSRI, TeCA, ECT, benzodiazepines – – KET, ECT Y Y Y N N N N Y N N N N Y – – SSRI – SSRI – SSRI – – – SSRI – SSRI N N Candidates identified via previous research, bioinformatics or database scan Unspecified (naturalistic) SSRI Antidepressant Class Y N N N N Y N Y N N N Y Y Y Y N Y Y Y Y N Y Y Candidates identified via comprehensive screen (microarray) HDRS−17 MADRS-S HDRS−17 BDI HDRS−17 HDRS−17 HDRS−24 HDRS HDRS−17 HDRS−24 unspecified HDRS−24 MADRS-S BDI HDRS−17 SDS HDRS HDRS−24 HDRS−17 HDRS−21 HDRS, MADRS HDRS HDRS Clinical assessment used to assess depression MDE, major depressive episode; MDD, major depressive disorder; PBMC, peripheral blood mononuclear cells; HDRS, Hamilton Depression Rating Scale; BDI, Beck Depression Inventory; MADRS-S, Montgomery–Åsberg Depression Rating Scale (selfrated); SDS, Self-rating Depression Score; Y, yes; N, no, SSRI, selective serotonin reuptake inhibitor; KET, ketamine; TeCA, tetracyclic antidepressant; ECT, electroconvulsive therapy; SNRI, selective norepinephrine reuptake inhibitors; AAD, atypical antidepressant. Zhang et al. (2016) MDD MDD MDD PBMCs Serum Peripheral blood leukocytes Plasma MDD Blood MDD MDD MDD MDD MDD MDD PTSD & MDD MDD Blood Blood Blood Serum Plasma Blood Plasma Plasma MDD MDD MDD MDD MDD MDD Serum PBMCs Blood Plasma Blood Plasma MDD MDD MDD Blood Blood Blood MDE PBMCs Belzeaux et al. (2012) Bocchio-Chiavetto et al. (2013) Li et al. (2013) Fan et al. (2014) Issler et al. (2014) Liu et al. (2014) Lopez et al. (2014) Camkurt et al. (2015) Li et al. (2015) Song et al. (2015) Su et al. (2015) Wan et al. (2015) Wang et al. (2015) Wingo et al. (2015) Enatescu et al. (2016) Gururajan et al. (2016) He et al. (2016) Liu et al. (2016) Maffioletti et al. (2014) Marques et al. (2016) Roy et al. (2017) Sun et al. (2016) Clinical condition miRNA source Study Table 1 Details of studies comparing circulating microRNA expression data between depressed subjects and healthy controls. H. Yuan et al. Journal of Affective Disorders 233 (2018) 68–78 Journal of Affective Disorders 233 (2018) 68–78 H. Yuan et al. Fig. 1. Venn diagram showing 178 microRNAs that were differentially expressed (significant, with p < 0.05) across the 23 relevant human studies. Ninety-seven miRNAs are upregulated and 75 miRNAs are downregulated in MDD/depression patients compared to controls. Six show mixed results (both upregulation and downregulation) across the studies. All microRNAs in Venn diagram are specific microRNAs. MicroRNAs that appear more than once across studies are indicated. Note on nomenclature: miR-548ai refers to specific microRNA sequence with accession number MI0016813 in miRBase. All microRNAs are specific microRNAs pertaining to human samples; thus, the hsa- prefix is implied. 2015; Gururajan et al., 2016) and miRNA-16 was also repeatedly analyzed in 3 studies (Song et al., 2015; Issler et al., 2014; Gururajan et al., 2016), although no significant relation with depression was observed (Table 2). the following criteria: examined expression of one or multiple microRNAs in circulating biofluid (i.e. blood, serum, plasma, or CSF) and induced depression among animal subjects via an established model. Human studies were excluded if they were in review format (13), did not clinically measure depression (51), used bioinformatics but did not provide microRNA expression levels in biofluid samples (5), had no microRNA expression data (33), or did not measure microRNA expression in blood or its derivatives (4). All animal studies identified from title and abstract review were included. This resulted in 22 human studies, 5 animal studies, and 1 human and animal study, all of which met criteria for potential quantitative analysis. Attempts were made to obtain more microRNA expression data from some authors of the selected studies; no information was received. 3.2. MicroRNA expression in animal models of depression The diverse nature of the studies conducted using animal models of depression rendered it difficult to abstract data pertaining to particular microRNAs of interest. Table 3 shows the details of the 6 animal studies that involved the expression of one or multiple circulatory microRNAs in an animal model of stress-induced depression. Three studies extracted microRNA expression from rat blood samples (Song et al., 2015; Ryan et al., 2013; Zhao et al., 2013) and 3 other studies did so from rat serum (Zurawek et al., 2016; Aschrafi et al., 2016; Duan et al., 2016) (Table 3). Among the 6 studies, only examination of microRNA-16 expression was repeated: one study investigated the effect of altering miR-16 levels on antidepressant response whereas the other measured miR-16 levels in stress-induced subjects. Four studies used a stress-inducing method among animal subjects using chronic (unpredictable) mild stress. The source of microRNAs examined varied and included blood (Ryan et al., 2013; Zhao et al., 2013; Song et al., 2015), cerebrospinal fluid (Song et al., 2015), and serum (Zurawek et al., 2016; Aschrafi et al., 2016; Duan et al., 2016). 3. Results 3.1. MicroRNA expression in depressed human subjects Across the 23 studies providing human microRNA data (Table 1), a total of 178 distinct microRNAs were identified as significantly related to depression (Fig. 1). Ninety-seven of these microRNAs were significantly upregulated while 75 of these were downregulated in patients meeting criteria for depression in at least one of the 23 studies. The remaining 6 microRNAs (let-7b, miR-133a, miR-331-5p, miR-335, miR-345, miR-433) showed mixed results, with some studies indicating significant upregulation among depressed patients compared to healthy controls, and others showing significant downregulation (Fig. 1). In addition, we tried to obtain expression data from all experimental microarray screens as well as real-time PCR verification analyses, including those that were not (significantly) differentially expressed between depression patients versus controls. From the readily available data, we found that 1 specific microRNA (miR-132) had consistent expression data in 4 independent studies (Li et al., 2013; Su et al., 2015; Bocchio-Chiavetto et al., 2013; Liu et al., 2016). Comparative expression levels for miRNA-182 was available in 3 studies (Li et al., 2013, 4. Discussion Given this limited concordance among human studies to date, we deemed a meaningful meta-analysis unfeasible. This absence of concordance was evident for both associations to diagnostic group (depressed vs. healthy, n = 20) and treatment response (degree of response, n = 7). For example, the most prevalent microRNA investigated in human studies to date, miR-132, was examined in both studies comparing its expression levels between depressed patients and healthy controls (Li et al., 2013; Su et al., 2015; Liu et al., 2016) and studies 71 Journal of Affective Disorders 233 (2018) 68–78 H. Yuan et al. Table 2 Circulating microRNAs whose expression in blood, plasma, or serum of patients with depression is measured in at least 2 of the 23 human studies. Specific microRNA Relative expression in depressed patients (vs. controls) Author of study in which specific microRNA appears Number of independent studies let-7b Downregulated Upregulated Upregulated Upregulated NS NS NS Upregulated Upregulated Upregulated Upregulated NS Upregulated NS Downregulated Upregulated Downregulated NS NS NS Upregulated NS upregulated NS Upregulated Upregulated Upregulated Upregulated Upregulated Downregulated Upregulated Upregulated Upregulated Upregulated Upregulated NS NS Upregulated downregulated Upregulated downregulated Upregulated downregulated Upregulated NS Downregulated NS Downregulated Upregulated Upregulated Downregulated Upregulated Upregulated Downregulated Upregulated Upregulated Upregulated Upregulated Downregulated Downregulated Upregulated Upregulated Gururajan et al. (2016) Belzeaux et al. (2012) Bocchio-Chiavetto et al. Enatescu et al. (2016) Song et al. (2015) Issler et al. (2014) Gururajan et al. (2016) Bocchio-Chiavetto et al. Enatescu et al. (2016) Fan et al. (2014) Bocchio-Chiavetto et al. Wang et al. (2015) Bocchio-Chiavetto et al. Wan et al. (2015) Wang et al. (2015) Sun et al. (2016) Bocchio-Chiavetto et al. Camkurt et al. (2015) Liu et al. (2014) Wan et al. (2015) Bocchio-Chiavetto et al. Sun et al. (2016) Belzeaux et al. (2012) Wan et al. (2015) Enatescu et al. (2016) Li et al. (2013) Su et al. (2015) Bocchio-Chiavetto et al. Liu et al. (2016) Zhang et al. (2016) Belzeaux et al. (2012) Fan et al. (2014) Enatescu et al. (2016) Li et al. (2013) Li et al. (2015) Gururajan et al. (2016) Gururajan et al. (2016) Enatescu et al. (2016) Belzeaux et al. (2012) Belzeaux et al. (2012) Li et al. (2015) Bocchio-Chiavetto et al. Fan et al. (2014) Belzeaux et al. (2012) Wan et al. (2015) Enatescu et al. (2016) Sun et al. (2016) Belzeaux et al. (2012) Maffioletti et al. (2014) Belzeaux et al. (2012) Enatescu et al. (2016) Belzeaux et al. (2012) Camkurt et al. (2015) Wan et al. (2015) Bocchio-Chiavetto et al. Belzeaux et al. (2012) Bocchio-Chiavetto et al. Belzeaux et al. (2012) Zhang et al. (2016) Belzeaux et al. (2012) Enatescu et al. (2016) Belzeaux et al. (2012) 2 let-7d miR-16 miR-26a miR-26b miR-29b-2–5p miR-30a-5p miR-34c-5p miR-93–5p miR-106b-5p miR-107 miR-125a-5p miR-132 miR-133a miR-146b-5p miR-182 miR-223 miR-331–5p miR-335 miR-345 miR-375 miR-381 miR-425–3p miR-433 miR-451a miR-494 miR-589 miR-636 miR-652 (2013) 2 3 (2013) 2 2 (2013) 2 (2013) 2 2 (2013) 2 2 (2013) 2 2 4 (2013) 2 2 3 2 2 2 (2013) 2 2 2 2 2 2 (2013) 2 (2013) 2 2 2 NS, not significant. for two of its mature products (miR-29a-5p and miR-29b-2-5p), as did Belzeaux et al. (2012) for miR-331 (miR-331-3p and miR-331-5p). These distinctions are clinically important, because establishing one specific microRNA as a biomarker would imply the need to clearly distinguish between individual mature sequences when designing detection probes that bind specifically to the sequence of interest. The current animal literature is also limited and inconsistent, given measuring its alteration levels after a particular intervention (BocchioChiavetto et al., 2013). Variations in the form of specific microRNAs further intensify this absence of concordance. For example, Maffioletti et al. (2014) showed significantly different expression levels between depressed and healthy subjects for three distinct but related let-7 mature sequences: let-7a-5p, let-7d-5p, and let-7f-5p. Similarly, Wang et al. (2015) found significant differential expression in levels of miR-29 72 73 Serum, Edinger–Westphal nucleus (EWcp) Serum Aschrafi et al. (2016) Duan et al. (2016) Wistar rats (m) Albino Wistar-R Amsterdam rats (m) Wistar-Han rats (m) Chronic unpredictable mild stress (CUMS) Chronic variable mild stress (CVMS) Chronic mild stress (CMS) Injection of anti-miR-16 (antagomir) Stroke induced by cerebral artery occlusion, then chronic mild stress (CMS) None Induced depression (stress) model Sex of animal subjects are indicated (m = male, f = female) as described in the study. Serum, ventral tegmental area (VTA), nucleus accumbens septi (NAcc), hippocampus, medial prefrontal cortex CSF, blood Song et al. (2015) Zurawek et al. (2016) Sprague-Dawley rats (m) Peripheral blood, brain Zhao et al. (2014) Sprague-Dawley rats (f) Sprague-Dawley rats (m) Blood, dentate gyrus, hippocampus, frontal cortex, cerebellum Ryan et al. (2013) Animal type miRNA source Study Table 3 Details of animal studies examining circulating microRNA expression through a depression model. miR-383–5p, miR764–5p miR−326 miR−16 miR-16 miR-137 miR-212 Main miRNAs manipulated or discovered miR-212 and BDNF levels in whole blood and in dentate gyrus significantly increased following chronic administration of electroconvulsive shock therapy (ECS) Significantly lower miR-137 levels in the brain and peripheral blood of post-stroke depression rats, miR-137 overexpression in the brain improves behavioral deficits in post-stroke depression rats Rats injected with anti-miR-16 antagomir after 2-week period showed increased anhedonic behaviors, lower miR-16 levels in CSF, and increased expression of SERT (major target for the selective serotonin reuptake inhibitor) protein in rat raphe Significant increase in serum levels of miR−16 expression after 7 weeks of CMS, significant alterations in miR−16 levels in VTA, NAcc, and hippocampus after 7 weeks of CMS Reduced miR-326 levels in the EWcp of CVMS rats; in fully-recovered CVMS rats, miR-326 levels in both serum and EWcp recovered to non-stressed levels 6 significantly altered miRNAs in serum of CUMS rats compared to controls, 16 significantly altered miRNAs in serum of CUMS rats with electro-acupuncture (EA) treatment; expression of miR-383–5p and miR-764–5p were upregulated after CUMS and then downregulated by EA intervention Main microRNA-related finding (s) Investigation of EA on miRNA expression No antidepressants No antidepressants Investigation of miRNA on antidepressant response No antidepressants; investigation of miRNA on depression behavioral response Investigation of ECS therapy on miRNA expression Involvement of antidepressants/ treatment intervention H. Yuan et al. Journal of Affective Disorders 233 (2018) 68–78 Journal of Affective Disorders 233 (2018) 68–78 H. Yuan et al. 2015; He et al., 2016; Sun et al., 2016; Camkurt et al., 2015; Su et al., 2015; Issler et al., 2014; Liu et al., 2016; Roy et al., 2017; Marques et al., 2016; Lopez et al., 2014; Li et al., 2013). Maffioletti et al. (2016) employed both methods to select their set of microRNAs (Table 1). These considerations are relevant because they underpin the fundamental technical discrepancies that may emerge from experimental analyses of microRNA expression. Of the currently available technology for microRNA expression profiling, the most common approaches include bioinformatics and high-throughput screens via microarrays, RNA sequencing, or real-time quantitative PCR (Issler and Chen, 2015). The inherent biological variability of microRNA expression patterns among participants can further complicate results obtained from a qPCR analysis. One important step that must be taken in order for microRNA expression profiling to be valid across a number of independent studies is to establish the natural variance of circulating microRNA levels in a healthy population of individuals (Issler and Chen, 2015). For studies employing PCR to quantify expression levels among patients in comparison to healthy controls, identifying adequate reference genes is essential. In fact, the normalization of microRNA expression data requires reference genes that demonstrate considerably stable expression and abundance levels similar to the full amount of microRNA in the original sample (Bustin et al., 2009). Most studies have used statistical methods or database-identified RNAs or microRNAs as normalization controls (Mestdagh et al., 2009). Only one study thus far (Liu et al., 2014) has attempted to systematically and experimentally identify suitable plasma-based reference genes for microRNA expression analysis, a clear indication that this critical methodological measure has been underutilized in current research. Repeated experiments are necessary in order to confirm the validity of the selected reference genes and assert that they demonstrate consistently stable expression across blood, serum, and plasma). the diversity of depression models, type and sex of animals used, and the source of the microRNA (Table 3). Although evidence is scarce, the data highlight miR-16 involvement in depression models as well as its potential function in the regulatory mechanisms of antidepressants such as fluoxetine. Early evidence showed that the antidepressant effect of fluoxetine involves miR-16-mediated hippocampal neurogenesis that is propagated by raphe-secreted S100ß neurotrophic factor in the locus corueleus (Launay et al., 2011). A more recent study (Song et al., 2015) reveals a significant reduction in cerebrospinal fluid serotonin in antimiR-16 treated rats, suggesting that this circulating microRNA participates in the serotonergic transmission system involved in antidepressant treatment mechanisms. Zurawek et al. (2016) further identified stress-resiliency as a conditional phenotype for increased rat serum levels of miR-16 in response to induced chronic stress. Despite these intriguing findings from animal models, none of the four human studies investigating miR-16 found differences between healthy and depressed subjects (Camkurt et al., 2015; Gururajan et al., 2016; Issler et al., 2014; Song et al., 2015), raising questions about the meaning of these findings in animal models, at least in relation to the circulating microRNA assays used in the human studies. 4.1. Methodological caveats The state of the literature is further complicated by the variable decision to analyze samples of whole blood (Song et al., 2015; BocchioChiavetto et al., 2013; Maffioletti et al., 2014; Wingo et al., 2015; Li et al., 2015), serum (Wan et al., 2015), plasma (Camkurt et al., 2015; Liu et al., 2014; Wang et al., 2015; Zhang et al., 2016), peripheral blood leukocytes (Sun et al., 2016), or peripheral blood mononuclear cells (He et al., 2016; Fan et al., 2014). These variations in sample collection, coupled with the range of clinical scales used to determine depression among patients (i.e. Hamilton Depression Rating Scale [HAMD; Hamilton, 1960], Beck Depression Inventory [BDI; Beck et al., 1961], or Montgomery-Asberg Depression Rating Scale [MADRS; Montgomery and Asberg, 1979] scores) and the marked heterogeneity of this clinical condition (Cassano and Fava, 2002), make it difficult to determine an overall effect size across a limited number of studies. Furthermore, to be as inclusive as possible, two of the studies selected for review assessed patients with comorbid disorders such as PTSD (Wingo et al., 2015) or specific forms of depression such as post-stroke depression (Zhang et al., 2016). It is possible that data for such specific clinical populations would lower the generalizability of any findings to all depressed patients. It is also important to note that the therapies used in the studies covered in this review have diverse mechanisms of action. Some are primarily serotonergic (selective serotonin reuptake inhibitors, SSRIs), noradrenergic (tricyclic and tetracyclic antidepressants), combined serotonergic and noradrenergic (serotonin-norepinephrine reuptake inhibitors-SNRIs), GABAergic (benzodiazepines), glutamatergic (ketamine), or work via seizure induction followed by yet unclear physiologic effects (ECT). This diversity of psychotropic mechanisms of action could explain the lack of replication across studies in humans. Further verification of the mechanisms of microRNAs has the potential to clarify the variable results in the depression literature for these microRNAs, helping to identify those factors and conditions that may have a tighter relationship to microRNA expression than diagnostic status or treatment response. Concerns surrounding the methodology in quantifying microRNA levels in human subjects merit additional attention. Whereas some studies conducted a microarray expression profile prior to verifying a set of experimental microRNA candidates via quantitative RT-PCR (Wingo et al., 2015; Fan et al., 2014; Wang et al., 2015; Liu et al., 2014; Zhang et al., 2016; Wan et al., 2015; Gururajan et al., 2016; Belzeaux et al., 2012; Bocchio-Chiavetto et al., 2013; Enatescu et al., 2016), others sought to determine these candidates based on prior studies, bioinformatics, or microRNA databases (Song et al., 2015; Li et al., 4.2. Mechanistic explanations for the role of miRNA-132 in MDD Little is known about the ways in which circulating microRNAs are shuttled and delivered to their target mRNA transcripts, or the putative mechanisms of action by which miRNAs regulate or are regulated by depression. The paucity of these mechanistic explanations calls for continued comprehensive screening for viable circulating miRNA candidates followed by targeted verification of prominent ones. Although the data presented in this study cannot confer a target, it is worth acknowledging miR-132 as the most replicated candidate among studies, with a consistent expression pattern across four independent studies (Table 2). miR-132 is known to target the 3′ untranslated region (3’ UTR) of the methyl CpG-binding protein 2 (MeCP2) gene that influences the in vivo expression of BDNF (Klein et al., 2007). Numerous studies have acknowledged the involvement of BDNF in modulating antidepressant response in conjunction with its signaling receptor TrkB, although unclear associations prevail with regards to the role of BDNF in the pathophysiology of major depression (Castrén and Rantamäki, 2010; Lee and Kim, 2010; Martinowich et al., 2007). As Li et al. (2013) have pointed out, the dysregulation of BDNF in other neurodegenerative and neuropsychiatric diseases (Yasutake et al., 2006; Harrisberger et al., 2015; Ikeda et al., 2008; Cunha et al., 2006) marks it a nonspecific indicator of disease, thereby requiring additional depressionspecific biomarkers in order to serve as a clinically useful diagnostic. Proposed mechanisms for the link between circulating miR-132 and BDNF levels are scarce or incomplete. Evidence suggests feedback regulation of of miRNA-132 expression by BDNF via a MAPK/ERK1/2 signaling pathway, which alters the concentration of postsynaptic glutamate receptors (Kawashima et al., 2010) and neuronal proliferation in the hippocampus (Yi et al., 2014). A recent study also reported that blood levels of miR-132 were associated with visual memory deficits among depressed patients (Liu et al., 2016). This recognizes that miR132 targets proteins of signaling pathways that regulate the formation of dendritic spines, whose density and functionality are known to be 74 Journal of Affective Disorders 233 (2018) 68–78 H. Yuan et al. Ayerst Laboratories. involved in visual memory (Liu et al., 2016). However, these models do not relate the mechanism of circulating microRNA-132 to its activity in the brain, a crucial step in determining whether it can effectively diagnose depression. Taken together, these findings imply that it may be advantageous to identify additional circulatory microRNA candidates that indirectly or directly regulate BDNF among depressed patients, such as miR-182 (Li et al., 2013). These microRNAs may be not only indicative of MDD, but also predictive of the BDNF-dependent antidepressant mechanisms associated with treatment response. However, it must be noted that these proposed mechanisms fall short in elucidating the mode by which circulatory miRNAs participate in the aforementioned processes, further underscoring a critical gap in the studies to date. More effort must be made to confirm a correlation between circulatory and brain-localized microRNAs, in addition to clarifying the transport systems through which microRNAs access their targets. Advisory Board/ consultant Maurizio Fava Abbott Laboratories; Acadia; Affectis Pharmaceuticals AG; Alkermes, Inc.; Amarin Pharma Inc.; Aspect Medical Systems; AstraZeneca; Auspex Pharmaceuticals; Avanir Pharmaceuticals; AXSOME Therapeutics; Bayer AG; Best Practice Project Management, Inc.; Biogen; BioMarin Pharmaceuticals, Inc.; Biovail Corporation; BrainCells Inc; Bristol-Myers Squibb; CeNeRx BioPharma; Cephalon, Inc.; Cerecor; CNS Response, Inc.; Compellis Pharmaceuticals; Cypress Pharmaceutical, Inc.; DiagnoSearch Life Sciences (P) Ltd.; Dinippon Sumitomo Pharma Co. Inc.; Dov Pharmaceuticals, Inc.; Edgemont Pharmaceuticals, Inc.; Eisai Inc.; Eli Lilly and Company; EnVivo Pharmaceuticals, Inc.; ePharmaSolutions; EPIX Pharmaceuticals, Inc.; Euthymics Bioscience, Inc.; Fabre-Kramer Pharmaceuticals, Inc.; Forest Pharmaceuticals, Inc.; Forum Pharmaceuticals; GenOmind, LLC; GlaxoSmithKline; Grunenthal GmbH; Indivior; i3 Innovus/Ingenis; Intracellular; Janssen Pharmaceutica; Jazz Pharmaceuticals, Inc.; Johnson & Johnson Pharmaceutical Research & Development, LLC; Knoll Pharmaceuticals Corp.; Labopharm Inc.; Lorex Pharmaceuticals; Lundbeck Inc.; MedAvante, Inc.; Merck & Co., Inc.; MSI Methylation Sciences, Inc.; Naurex, Inc.; Nestle Health Sciences; Neuralstem, Inc.; Neuronetics, Inc.; NextWave Pharmaceuticals; Novartis AG;Nutrition 21; Orexigen Therapeutics, Inc.; Organon Pharmaceuticals; Osmotica; Otsuka Pharmaceuticals; Pamlab, LLC.; Pfizer Inc.; PharmaStar; Pharmavite® LLC.; PharmoRx Therapeutics; Precision Human Biolaboratory; Prexa Pharmaceuticals, Inc.; PPD; Puretech Ventures; PsychoGenics; Psylin Neurosciences, Inc.; RCT Logic, LLC (formerly Clinical Trials Solutions, LLC); Rexahn Pharmaceuticals, Inc.; Ridge Diagnostics, Inc.; Roche; Sanofi-Aventis US LLC.; Sepracor Inc.; Servier Laboratories; Schering-Plough Corporation; Shenox Pharmaceuticals; Solvay Pharmaceuticals, Inc.; Somaxon Pharmaceuticals, Inc.; Somerset Pharmaceuticals, Inc.; Sunovion Pharmaceuticals; Supernus Pharmaceuticals, Inc.; Synthelabo; Taisho Pharmaceutical; Takeda Pharmaceutical Company Limited; Tal Medical, Inc.; Tetragenex Pharmaceuticals, Inc.; TransForm Pharmaceuticals, Inc.; Transcept Pharmaceuticals, Inc.; Vanda Pharmaceuticals, Inc.; VistaGen. Research support Speaking/Publishing Abbott Laboratories; Acadia Pharmaceuticals (pending as of 8-1116); Alkermes, Inc.; American Cyanamid;Aspect Medical Systems; AstraZeneca; Avanir Pharmaceuticals; AXSOME Therapeutics; BioResearch; BrainCells Inc.; Bristol-Myers Squibb; CeNeRx BioPharma; Cephalon; Cerecor; Clintara, LLC; Covance; Covidien; Eli Lilly and Company;EnVivo Pharmaceuticals, Inc.; Euthymics Bioscience, Inc.; Forest Pharmaceuticals, Inc.; FORUM Pharmaceuticals; Ganeden Biotech, Inc.; GlaxoSmithKline; Harvard Clinical Research Institute; Hoffman-LaRoche; Icon Clinical Research; i3 Innovus/Ingenix; Janssen R & D, LLC; Jed Foundation; Johnson & Johnson Pharmaceutical Research & Development; Lichtwer Pharma GmbH; Lorex Pharmaceuticals; Lundbeck Inc.; MedAvante; Methylation Sciences Inc; National Alliance for Research on Schizophrenia & Depression (NARSAD); National Center for Complementary and Alternative Medicine (NCCAM);National Coordinating Center for Integrated Medicine (NiiCM); National Institute of Drug Abuse (NIDA); National Institute of Mental Health (NIMH); Neuralstem, Inc.; NeuroRx; Novartis AG; Organon Pharmaceuticals; PamLab, LLC.; Pfizer Inc.; PharmaciaUpjohn; Pharmaceutical Research Associates., Inc.; Pharmavite® LLC;PharmoRx Therapeutics; Photothera; Reckitt Benckiser; Roche Pharmaceuticals; RCT Logic, LLC (formerly Clinical Trials Solutions, LLC); Sanofi-Aventis US LLC; Shire; Solvay Pharmaceuticals, Inc.; Stanley Medical Research Institute (SMRI); Synthelabo; Takeda Pharmaceuticals;Tal Medical; VistaGen (pending as of 8-11-16); Wyeth- Adamed, Co; Advanced Meeting Partners; American Psychiatric Association; American Society of Clinical Psychopharmacology; AstraZeneca; Belvoir Media Group; Boehringer Ingelheim GmbH; Bristol-Myers Squibb; Cephalon, Inc.; CME Institute/Physicians Postgraduate Press, Inc.; Eli Lilly and Company; Forest Pharmaceuticals, Inc.; GlaxoSmithKline; Imedex, LLC; MGH Psychiatry Academy/Primedia; MGH Psychiatry Academy/Reed Elsevier; Novartis AG; Organon Pharmaceuticals; Pfizer Inc.; PharmaStar; United BioSource,Corp.; Wyeth-Ayerst Laboratories. 5. Conclusions In summary, across 23 human studies, a total of 178 distinct microRNAs were identified as significantly related to depression, with little replication across studies. The most consistent findings were for upregulated expression of microRNA-132 among depressed patients. Animal studies fail to align with data from human studies with regards to microRNA-16. Given the high rates of non-replication to date, it will be important for future studies examining microRNA correlates of depression to address both the methodological and reporting challenges for this area of study. Knowing which candidates fail to replicate may be as important as positive findings during this time of rapid proliferation of targets. Author disclosures Role of funding source This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Stock/Other financial options None. Equity holdings Compellis; PsyBrain, Inc. Royalty/patent, other income Patents for Sequential Parallel Comparison Design (SPCD), licensed by MGH to Pharmaceutical Product Development, LLC (PPD); and patent application for a combination of Ketamine plus Scopolamine in Major Depressive Disorder (MDD), licensed by MGH to Biohaven. 75 Journal of Affective Disorders 233 (2018) 68–78 H. Yuan et al. Ment. Health 1 (1), 1003. Dwivedi, Y., 2014. Emerging role of microRNAs in major depressive disorder: diagnosis and therapeutic implications. Dialog-. Clin. Neurosci. 16 (1), 43–61. Dwivedi, Y., Roy, B., Lugli, G., Rizavi, H., Zhang, H., Smalheiser, N.R., 2015. Chronic corticosterone-mediated dysregulation of microRNA network in prefrontal cortex of rats: relevance to depression pathophysiology. Transl. Psychiatry 5 (11), e682. Enatescu, V.R., Papava, I., Enatescu, I., Antonescu, M., Anghel, A., Seclaman, E., Marian, C., 2016. Circulating plasma micro RNAs in patients with major depressive disorder treated with antidepressants: a pilot study. Psychiatry Investig. 13 (5), 549–557. Eyre, H.A., Papps, E., Baune, B.T., 2015. Treating depression and depression-like behavior with physical activity: an immune perspective. Progress in Physical Activity and Exercise and Affective and Anxiety Disorders: Translational Studies, Perspectives and Future Directions, 11. Fan, H.M., Sun, X.Y., Guo, W., Zhong, A.F., Niu, W., Zhao, L., Dai, Y.H., Guo, Z.M., Zhang, L.Y., Lu, J., 2014. Differential expression of microRNA in peripheral blood mononuclear cells as specific biomarker for major depressive disorder patients. J. Psychiatr. Res. 59, 45–52. Forte, A., Baldessarini, R.J., Tondo, L., Vázquez, G., Pompili, M., Girardi, P., 2015. Longterm morbidity in bipolar-I, bipolar-II, and major depressive disorders. J. Affect Disord. 178, 71–78. Geaghan, M., Cairns, M.J., 2015. MicroRNA and posttranscriptional dysregulation in psychiatry. Biol. Psychiatry 78 (4), 231–239. Gururajan, A., Naughton, M.E., Scott, K.A., O'connor, R.M., Moloney, G., Clarke, G., Scott, L., 2016. MicroRNAs as biomarkers for major depression: a role for let-7b and let-7c. Transl. Psychiatry 6 (8), e862. Hamilton, M., 1960. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 23, 56–62. Harrisberger, F., Smieskova, R., Schmidt, A., Lenz, C., Walter, A., Wittfeld, K., Borgwardt, S., 2015. BDNF Val66Met polymorphism and hippocampal volume in neuropsychiatric disorders: a systematic review and meta-analysis. Neurosci. Biobehav. Rev. 55, 107–118. He, S., Liu, X., Jiang, K., Peng, D., Hong, W., Fang, Y., Qian, Y., Yu, S., Li, H., 2016. Alterations of microRNA-124 expression in peripheral blood mononuclear cells in pre-and post-treatment patients with major depressive disorder. J. Psychiatr. Res. 78, 65–71. Heneghan, H.M., Miller, N., Lowery, A.J., Sweeney, K.J., Newell, J., Kerin, M.J., 2010. Circulating microRNAs as novel minimally invasive biomarkers for breast cancer. Ann. Surg. 251, 499–505. Hu, G., Drescher, K.M., Chen, X., 2012. Exosomal miRNAs: biological properties and therapeutic potential. Front. Genet. 3, 56. Hu, Z., Chen, X., Zhao, Y., et al., 2010. Serum microRNA signatures identified in a genome-wide serum microRNA expression profiling predict survival of non-small-cell lung cancer. J. Clin. Oncol. 28, 1721–1726. Hunter, M.P., Ismail, N., Zhang, X., Aguda, B.D., Lee, E.J., Yu, L., Nana-Sinkam, S.P., 2008. Detection of microRNA expression in human peripheral blood microvesicles. PloS One 3 (11), e3694. Ikeda, Y., Yahata, N., Ito, I., Nagano, M., Toyota, T., et al., 2008. Low serum levels of brain-derived neurotrophic factor and epidermal growth factor in patients with chronic schizophrenia. Schizophr. Res. 101, 58–66. Issler, O., Chen, A., 2015. Determining the role of microRNAs in psychiatric disorders. Nat. Rev. Neurosci. 16, 201–212. Issler, O., Haramati, S., Paul, E.D., Maeno, H., Navon, I., Zwang, R., Awatramani, R., 2014. MicroRNA 135 is essential for chronic stress resiliency, antidepressant efficacy, and intact serotonergic activity. Neuron 83 (2), 344–360. Jelovac, A., Kolshus, E., McLoughlin, D.M., 2013. Relapse following successful electroconvulsive therapy for major depression: a meta-analysis. Neuropsychopharmacology 38 (12), 2467–2474. Kato, M., 2012. [Choosing the adequate antidepressant focusing on efficacy, tolerability and its predictors]. Seishin Shinkeigaku Zasshi. 114 (5), 589–600. Kawashima, H., Numakawa, T., Kumamaru, E., Adachi, N., Mizuno, H., Ninomiya, M., Hashido, K., 2010. Glucocorticoid attenuates brain-derived neurotrophic factor-dependent upregulation of glutamate receptors via the suppression of microRNA-132 expression. Neuroscience 165 (4), 1301–1311. Kichukova, T.M., Popov, N.T., Ivanov, H.Y., Vachev, T.I., 2016. Circulating microRNAs as a novel class of potential diagnostic biomarkers in Neuropsychiatric disorders. Folia Med. 57 (3–4), 159–172. Klein, M.E., Lioy, D.T., Ma, L., Impey, S., Mandel, G., Goodman, R.H., 2007. Homeostatic regulation of MeCP2 expression by a CREB-induced microRNA. Nat. Neurosci. 10 (12), 1513. Kosaka, N., Iguchi, H., Yoshioka, Y., Takeshita, F., Matsuki, Y., Ochiya, T., 2010. Secretory mechanisms and intercellular transfer of microRNAs in living cells. J. Biol. Chem. 285 (23), 17442–17452. Landgraf, P., Rusu, M., Sheridan, R., Sewer, A., Iovino, N., Aravin, A., Lin, C., 2007. A mammalian microRNA expression atlas based on small RNA library sequencing. Cell 129 (7), 1401–1414. Launay, J.M., Mouillet-Richard, S., Baudry, A., Pietri, M., Kellermann, O., 2011. Raphemediated signals control the hippocampal response to SRI antidepressants via miR16. Transl. Psychiatry 1 (11), e56. Lawrie, C.H., Gal, S., Dunlop, H.M., Pushkaran, B., Liggins, A.P., Pulford, K., Hatton, C.S., 2008. Detection of elevated levels of tumour‐associated microRNAs in serum of patients with diffuse large B‐cell lymphoma. Br. J. Haematol. 141 (5), 672–675. Lee, B.H., Kim, Y.K., 2010. The roles of BDNF in the pathophysiology of major depression and in antidepressant treatment. Psychiatry Investig. 7 (4), 231–235. Leuchter, A.F., Cook, I.A., Hamilton, S.P., Narr, K.L., Toga, A., Hunter, A.M., Faull, K., Whitelegge, J., Andrews, A.M., Loo, J., Way, B., Nelson, S.F., Horvath, S., Lebowitz, B.D., 2010. Biomarkers to predict antidepressant response. Curr. Psychiatry Rep. 12 Copyright For the MGH Cognitive & Physical Functioning Questionnaire (CPFQ), Sexual Functioning Inventory (SFI), Antidepressant Treatment Response Questionnaire (ATRQ), Discontinuation-Emergent Signs & Symptoms (DESS), Symptoms of Depression Questionnaire (SDQ), and SAFER; Lippincott, Williams & Wilkins; Wolkers Kluwer; World Scientific Publishing Co. Pte. Ltd. David Mischoulon Research Support Dr. Mischoulon has received research support from the FisherWallace, Nordic Naturals, Methylation Sciences, Inc. (MSI), and PharmoRx Therapeutics. He has received honoraria for speaking from the Massachusetts General Hospital Psychiatry Academy. He has received royalties from Lippincott Williams & Wilkins for published book “Natural Medications for Psychiatric Disorders: Considering the Alternatives.” Acknowledgements The first author would like to thank Dr. Otto for his mentorship and guidance in the literature search and review process, and Dr. Mischoulon and Dr. Fava for devoting their collective time and effort to editing and improving the draft of this paper. References Ai, J., Zhang, R., Li, Y., et al., 2010. Circulating microRNA-1 as a potential novel biomarker for acute myocardial infarction. Biochem. Biophys. Res. Commun. 391, 73–77. Andrade, C., Arumugham, S.S., Thirthalli, J., 2016. Adverse Effects of Electroconvulsive Therapy. Psychiatr. Clin. North Am. 39 (3), 513–530. Aschrafi, A., Verheijen, J.M., Gordebeke, P.M., Loohuis, N.F.O., Menting, K., Jager, A., Glennon, J.C., 2016. MicroRNA-326 acts as a molecular switch in the regulation of midbrain urocortin 1 expression. J. Psychiatry Neurosci. 1, 8872147. Bartel, D.P., 2004. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell 116, 281–297. Bartova, L., Berger, A., Pezawas, L., 2010. Is there a personalized medicine for mood disorders? Eur. Arch. Psychiatry Clin. Neurosci. 260 (Suppl 2), S121–S126. Baudry, A., Mouillet-Richard, S., Schneider, B., Launay, J.-M., Kellermann, O., 2010. miR16 targets the serotonin transporter: a new facet for adaptive responses to antidepressants. Science 329, 1537–1541. Beck, A.T., Ward, C.H., Mendelson, M., Mock, J., Erbaugh, J., 1961. An inventory for measuring depression. Arch. Gen. Psychiatry 4 (6), 561–571. Belzeaux, R., Bergon, A., Jeanjean, V., Loriod, B., Formisano-Treziny, C., Verrier, L., Loundou, A., Baumstarck-Barrau, K., Boyer, L., Gall, V., 2012. Responder and nonresponder patients exhibit different peripheral transcriptional signatures during major depressive episode. Transl. Psychiatry 2, e185. Bocchio-Chiavetto, L., Maffioletti, E., Bettinsoli, P., Giovannini, C., Bignotti, S., Tardito, D., Corrada, D., Milanesi, L., Gennarelli, M., 2013. Blood microRNA changes in depressed patients during antidepressant treatment. Eur. Neuropsychopharmacol. 23, 602–611. Bustin, S.A., Benes, V., Garson, J.A., Hellemans, J., Huggett, J., Kubista, M., Mueller, R., Nolan, T., Pfaffl, M.W., Shipley, G.L., 2009. The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 55, 611–622. Camkurt, M.A., Acar, Ş., Coşkun, S., Güneş, M., Güneş, S., Yılmaz, M.F., Görürg, A., Tamer, L., 2015. Comparison of plasma MicroRNA levels in drug naive, first episode depressed patients and healthy controls. J. Psychiatr. Res. 69, 67–71. Cassano, P., Fava, M., 2002. Depression and public health: an overview. J. Psychosom. Res. 53, 849–857. Castrén, E., Rantamäki, T., 2010. The role of BDNF and its receptors in depression and antidepressant drug action: reactivation of developmental plasticity. Dev. Neurobiol. 70 (5), 289–297. Chen, X., Ba, Y., Ma, L., Cai, X., Yin, Y., Wang, K., Li, Q., 2008. Characterization of microRNAs in serum: a novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 18 (10), 997–1006. Cunha, A.B., Frey, B.N., Andreazza, A.C., Goi, J.D., Rosa, A.R., Gonçalves, C.A., Kapczinski, F., 2006. Serum brain-derived neurotrophic factor is decreased in bipolar disorder during depressive and manic episodes. Neurosci. Lett. 398 (3), 215–219. Duan, D., Dong, X., Tu, Y., Liu, P., 2016. A microarray study of chronic unpredictable mild stress rat blood serum with electro-acupuncture intervention. Neurosci. Lett. Dwivedi, Y., 2013. microRNAs as biomarker in depression pathogenesis. Ann. Psychiatry 76 Journal of Affective Disorders 233 (2018) 68–78 H. Yuan et al. derived neurotrophic factor expression via homeostatic interactions with microRNA132 in rats with depression. Mol. Med. Rep. 12 (4), 5399–5406. Sun, N., Lei, L., Wang, Y., Yang, C., Liu, Z., Li, X., Zhang, K., 2016. Preliminary comparison of plasma notch-associated microRNA-34b and-34c levels in drug naive, first episode depressed patients and healthy controls. J. Affect. Disord. 194, 109–114. Tan, K.S., Armugam, A., Sepramaniam, S., et al., 2009. Expression profile of MicroRNAs in young stroke patients. PLoS One 4, e7689. Undurraga, J., Baldessarini, R.J., 2012. Randomized, placebo-controlled trials of antidepressants for acute major depression: thirty-year meta-analytic review. Neuropsychopharmacology 37 (4), 851–864. Valadi, H., Ekström, K., Bossios, A., Sjöstrand, M., Lee, J.J., Lötvall, J.O., 2007. Exosomemediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat. Cell Biol. 9 (6), 654–659. Vickers, K.C., Palmisano, B.T., Shoucri, B.M., Shamburek, R.D., Remaley, A.T., 2011. MicroRNAs are transported in plasma and delivered to recipient cells by high-density lipoproteins. Nat. Cell Biol. 13 (4), 423–433. Vijayan, M., Reddy, P.H., 2016. Peripheral biomarkers of stroke: focus on circulatory microRNAs. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 1862 (10), 1984–1993. Wan, Y., Liu, Y., Wang, X., Wu, J., Liu, K., Zhou, J., Liu, L., Zhang, C., 2015. Identification of differential microRNAs in cerebrospinal fluid and serum of patients with major depressive disorder. PloS One 10, e0121975. Wang, J., Chen, J., Chang, P., et al., 2009. MicroRNAs in plasma of pancreatic ductal adenocarcinoma patients as novel blood-based biomarkers of disease. Cancer Prev. Res. 2, 807–813. Wang, J.F., Yu, M.L., Yu, G., et al., 2010. Serum miR-146a and miR-223 as potential new biomarkers for sepsis. Biochem Biophys. Res. Commun. 394, 184–188. Wang, X., Sundquist, K., Hedelius, A., Palmér, K., Memon, A.A., Sundquist, J., 2015. Circulating microRNA-144-5p is associated with depressive disorders. Clin. Epigenetics 7, 1. Wingo, A.P., Almli, L.M., Stevens, J.J., Klengel, T., Uddin, M., Li, Y., Bustamante, A.C., Lori, A., Koen, N., Stein, D.J., 2015. DICER1 and microRNA regulation in posttraumatic stress disorder with comorbid depression. Nat. Commun. 6. Yasutake, C., Kuroda, K., Yanagawa, T., Okamura, T., Yoneda, H., 2006. Serum BDNF, TNF-alpha and IL-1beta levels in dementia patients: comparison between Alzheimer's disease and vascular dementia. Eur. Arch. Psychiatry Clin. Neurosci. 256, 402–406. Yi, L.T., Li, J., Liu, B.B., Luo, L., Liu, Q., Geng, D., 2014. BDNF–ERK–CREB signaling mediates the role of miR-132 in the regulation of the effects of oleanolic acid in male mice. J. Psychiatry Neurosci. 39 (5), 348. Young, J.J., Silber, T., Bruno, D., Galatzer-Levy, I.R., Pomara, N., Marmar, C.R., 2016. Is there progress? An overview of selecting biomarker candidates for major depressive disorder. Front. Psychiatry 7. Zhang, Y., Cheng, L., Chen, Y., Yang, G.-Y., Liu, J., Zeng, L., 2016. Clinical predictor and circulating microRNA profile expression in patients with early onset post-stroke depression. J. Affect. Disord. 193, 51–58. Zhao, L., Li, H., Guo, R., Ma, T., Hou, R., Ma, X., Du, Y., 2013. miR-137, a new target for post-stroke depression? Neural Regen. Res. 8 (26), 2441. Zurawek, D., Kusmider, M., Faron-Gorecka, A., Gruca, P., Pabian, P., Kolasa, M., Dziedzicka-Wasylewska, M., 2016. Time-dependent miR-16 serum fluctuations together with reciprocal changes in the expression level of miR-16 in mesocortical circuit contribute to stress resilient phenotype in chronic mild stress–An animal model of depression. Eur. Neuropsychopharmacol. 26 (1), 23–36. (6), 553–562. Li, J., Meng, H., Cao, W., Qiu, T., 2015. MiR-335 is involved in major depression disorder and antidepressant treatment through targeting GRM4. Neurosci. Lett. 606, 167–172. Li, L., Vlisides, P.E., 2016. Ketamine: 50 Years of Modulating the Mind. Front Hum. Neurosci. 10, 612. Li, Y.J., Xu, M., Gao, Z.H., Wang, Y.Q., Yue, Z., Zhang, Y.X., Wang, P.Y., 2013. Alterations of serum levels of BDNF-related miRNAs in patients with depression. PLoS One 8 (5), e63648. Liu, X., Zhang, L., Cheng, K., Wang, X., Ren, G., Xie, P., 2014. Identification of suitable plasma-based reference genes for miRNAome analysis of major depressive disorder. J. Affect. Disord. 163, 133–139. Liu, Y., Yang, X., Zhao, L., Zhang, J., Li, T., Ma, X., 2016. increased mir-132 level is associated with visual memory dysfunction in patients with depression. Neuropsychiatr. Dis. Treat. 12, 2905. Lopez, J.P., Lim, R., Cruceanu, C., Crapper, L., Fasano, C., Labonte, B., et al., 2014b. miR1202 is a primate- specific and brain-enriched microRNA involved in major depression and antidepres- sant treatment. Nat. Med 20 (764Ð8). Maffioletti, E., Cattaneo, A., Rosso, G., Maina, G., Maj, C., Gennarelli, M., Tardito, D., Bocchio-Chiavetto, L., 2014. Peripheral whole blood microRNA alterations in major depression and bipolar disorder. J. Affect. Disord. 200, 250–258. Marques, F.Z., Eikelis, N., Bayles, R.G., Lambert, E.A., Straznicky, N.E., Hering, D., … & Lambert, G.W., 2016. A polymorphism in the norepinephrine transporter gene is associated with affective and cardiovascular disease through a microRNA mechanism. Mol. Psychiatry. Martinowich, K., Manji, H., Lu, B., 2007. New insights into BDNF function in depression and anxiety. Nat. Neurosci. 10 (9), 1089–1093. Mestdagh, P., Van Vlierberghe, P., De Weer, A., Muth, D., Westermann, F., Speleman, F., Vandesompele, J., 2009. A novel and universal method for microRNA RT-qPCR data normalization. Genome Biol. 10, 1. Mitchell, P.S., Parkin, R.K., Kroh, E.M., et al., 2008. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 105, 10513–10518. Mittelbrunn, M., Gutiérrez-Vázquez, C., Villarroya-Beltri, C., González, S., Sánchez-Cabo, F., González, M.Á., Sánchez-Madrid, F., 2011. Unidirectional transfer of microRNAloaded exosomes from T cells to antigen-presenting cells. Nat. Commun. 2, 282. Montecalvo, A., Larregina, A.T., Shufesky, W.J., Stolz, D.B., Sullivan, M.L., Karlsson, J.M., Milosevic, J., 2012. Mechanism of transfer of functional microRNAs between mouse dendritic cells via exosomes. Blood 119 (3), 756–766. Montgomery, S.A., Asberg, M., 1979. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 134, 382–389. Mráz, M., Malinova, K., Mayer, J., Pospisilova, S., 2009. MicroRNA isolation and stability in stored RNA samples. Biochem. Biophys. Res. Commun. 390 (1), 1–4. Ng, E.K., Chong, W.W., Jin, H., et al., 2009. Differential expression of microRNAs in plasma of patients with colorectal cancer: a potential marker for colorectal cancer screening. Gut 58, 1375–1381. O'Connor, R.M., Grenham, S., Dinan, T.G., Cryan, J.F., 2013. microRNAs as novel antidepressant targets: converging effects of ketamine and electroconvulsive shock therapy in the rat hippocampus. Int. J. Neuropsychopharmacol. 16, 1885–1892. Papakostas, G.I., Shelton, R.C., Kinrys, G., Henry, M.E., Bakow, B.R., Lipkin, S.H., Pi, B., Thurmond, L., Bilello, J.A., 2013. Assessment of a multi-assay, serum-based biological diagnostic test for major depressive disorder: a pilot and replication study. Mol. Psychiatry 18 (3), 332–339. Reid, G., Kirschner, M.B., van Zandwijk, N., 2011. Circulating microRNAs: association with disease and potential use as biomarkers. Crit. Rev. Oncol./Hematol. 80 (2), 193–208. Resnick, K.E., Alder, H., Hagan, J.P., Richardson, D.L., Croce, C.M., Cohn, D.E., 2009. The detection of differentially expressed microRNAs from the serum of ovarian cancer patients using a novel real-time PCR platform. Gynecol. Oncol. 112, 55–59. Roy, B., Dunbar, M., Shelton, R.C., Dwivedi, Y., 2017. Identification of MicroRNA-124-3p as a putative epigenetic signature of major depressive disorder. Neuropsychopharmacology 42 (4), 864–875. Rucker, J.J., McGuffin, P., 2014. Chipping away at major depressive disorder. Genome Biol. 15 (7), 1. Ryan, K.M., O’Donovan, S.M., McLoughlin, D.M., 2013. Electroconvulsive stimulation alters levels of BDNF-associated microRNAs. Neurosci. Lett. 549, 125–129. Schizophrenia Psychiatric Genome-Wide Association Study (GWAS) Consortium, 2011. Genome-wide association study identifies five new schizophrenia loci. Nat. Genet. 43 (10), 969–976. Schwartz, J., Murrough, J.W., Iosifescu, D.V., 2016. Ketamine for treatment-resistant depression: recent developments and clinical applications. Evid. Based Ment. Health 19 (2), 35–38. Serafini, G., Pompili, M., Hansen, K.F., Obrietan, K., Dwivedi, Y., Shomron, N., Girardi, P., 2014. The involvement of microRNAs in major depression, suicidal behavior, and related disorders: a focus on miR-185 and miR-491-3p. Cell. Mol. Neurobiol. 34 (1), 17–30. Smalheiser, N.R., Lugli, G., Rizavi, H.S., Zhang, H., Torvik, V.I., Pandey, G.N., Davis, J.M., Dwivedi, Y., 2011. MicroRNA expression in rat brain exposed to repeated inescapable shock: differential alterations in learned helplessness vs. non-learned helplessness. Int. J. Neuropsychopharmacol. 14, 1315–1325. Smalheiser, N.R., Zhang, H., Dwivedi, Y., 2014. Enoxacin elevates microRNA levels in rat frontal cortex and prevents learned helplessness. Front. Psychiatry 5, 6. Song, M.F., Dong, J.Z., Wang, Y.W., He, J., Ju, X., Zhang, L., Zhang, Y.H., Shi, J.F., Lv, Y.Y., 2015. CSF miR-16 is decreased in major depression patients and its neutralization in rats induces depression-like behaviors via a serotonin transmitter system. J. Affect. Disord. 178, 25–31. Su, M., Hong, J., Zhao, Y., Liu, S., Xue, X., 2015. MeCP2 controls hippocampal brain- Heidi Yuan is currently pursuing her bachelor’s degree in Molecular Biology at Pomona College in Claremont, California. She worked in the lab of Dr. Michael Otto during the summer of 2016, where her research centered on exploring and evaluating potential and current clinical interventions for a variety of psychiatric disorders. David Mischoulon is the Director of the Depression Clinical and Research Program (DCRP) at the Massachusetts General Hospital, and an Associate Professor of Psychiatry at Harvard Medical School. His research interests have focused on the role of complementary and alternative medicine in psychiatry, as well as the role of biomarkers as moderators and mediators of treatment response with antidepressant therapies. His research has been funded by NARSAD, by the National Institutes of Health, and by the National Center for Complementary and Integrative Health. He has published more than 230 articles and a textbook on the use of natural medications for the treatment of psychiatric disorders. Maurizio Fava is Director, Division of Clinical Research of the Massachusetts General Hospital (MGH) Research Institute, Executive Vice Chair of the MGH Department of Psychiatry, and Associate Dean in Clinical and Translation Science at Harvard Medical School. He has had over 30 years of experience as a clinical investigator. Under his direction from 1990 until 2014, the MGH Depression Clinical and Research Program (DCRP) became one of the most highly regarded depression programs in the world, conducting research projects in a variety of areas including pharmacotherapy of treatment-resistant depression, alternative medicine, neuroimaging, genetics, neurophysiology, neuroendocrinology, novel pharmacotherapies, and psychotherapy. He has authored or co-authored more than 800 original articles published in medical journals with international circulation, and which have been cited more than 50,000 times in the literature articles published in medical journals with international circulation, and which have been cited more than 50,000 times in the literature (h factor > 115). In 2007, he founded and is now the Executive Director of the MGH Psychiatry Clinical Trials Network and Institute (CTNI), the first academic Contract Research Organization specialized in the coordination of multi-center clinical trials in the CNS area. He has successfully obtained funding, as principal or co-principal investigator, from the National Institute of Health and industry for a total of more than $95,000,000 in the past 30 years. He has also trained 77 Journal of Affective Disorders 233 (2018) 68–78 H. Yuan et al. promotion of the emotional and cognitive benefits of exercise. Dr. Otto has been identified as a “top producer” in the clinical empirical literature; he is author of Exercise for Mood and Anxiety: Proven Strategies for Overcoming Depression and Enhancing Well Being, with Oxford University Press, as well as over 300 other articles, chapters, and books spanning his clinical and research interests. Dr. Otto is a past President of the Association for Behavioral and Cognitive Therapies (formerly AABT), a fellow of the American Psychological Association, and a member of the Scientific Advisory Board for the Anxiety Disorders Association of America. Dr. Otto is a regular provider of continuing education and continuing medical education workshops across the United States. and mentored over 50 research fellows. Michael Otto is Professor of Psychology at Boston University. He specializes in the cognitive-behavioral treatment (CBT) of anxiety, mood, and substance use disorders. An enduring theme across these disorders is the role of exposure-based emotional tolerance/ acceptance strategies in improving mental health. Current research includes investigations of potential moderators of CBT efficacy, including several translational-research agendas such as the application of putative memory enhancers (e.g., d-cycloserine) to facilitate exposure-based treatments. Dr. Otto also focuses on health behavior promotion ranging from medication adherence and smoking cessation to documentation and 78